
Abstract
Objective:
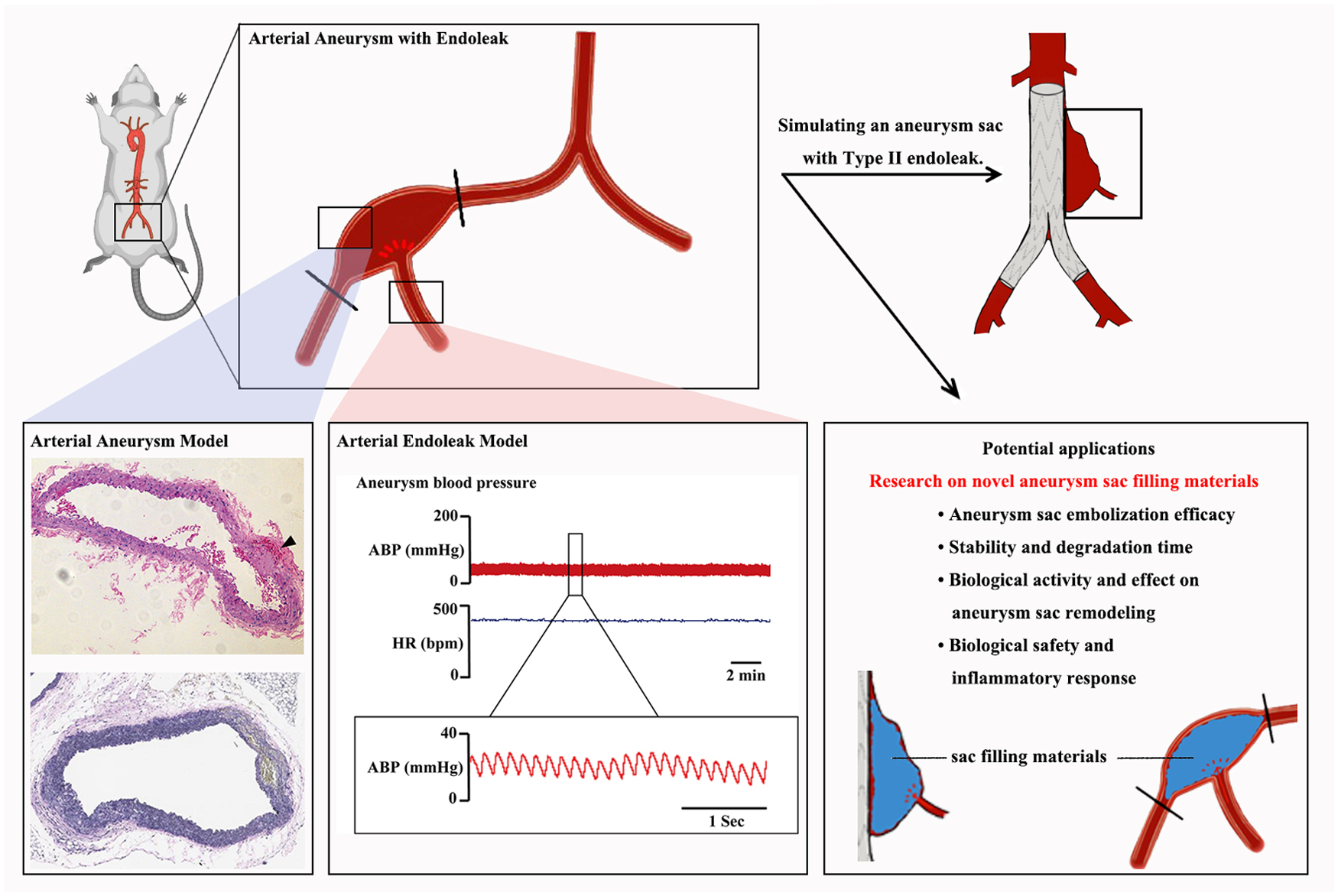
To develop a novel arterial aneurysm model that replicates sustained endoleak flow while also preserving a biologically active environment within the aneurysm sac. This model serves as a platform for assessing and refining aneurysm sac-filling materials aimed at improving the prevention and management of endoleaks following endovascular aneurysm repair.
Methods:
To create an aneurysm model, this study involved the surgical induction of vessel wall dilation and damage in the common iliac artery and external iliac artery of rats. Subsequently, the internal iliac artery was retained as a single collateral vessel of the aneurysm sac. Retrograde branch flow from the internal iliac artery contributed to the pressurization of the aortic aneurysm sac and continued expansion of the aneurysm. This approach established type II endoleak models. Aneurysm sac diameter was measured regularly to monitor model progression dynamically. Histological analysis was employed to assess the structural integrity of the aneurysm walls. Furthermore, both systemic and intra-aneurysmal blood pressure and heart rate in rats were monitored to ascertain the presence of endoleaks.
Results:
Twenty rats were allocated into four groups, with 15 model rats surviving to 1, 2, and 4 weeks. Aneurysm diameter in the model groups significantly increased compared to that in the sham group (P < .05) and remained stable over time. Histological analysis showed greater elastic fiber fragmentation at 4 weeks (3.600 ± 0.547 vs. 1.200 ± 0.447; P < .001). Endoleaks were confirmed through arterial blood aspiration and arterial waveform detection. Intra-sac pressure averaged 28.2 ± 5.4 mm Hg (28.7 ± 4.9% of systemic mean arterial pressure), with pulse pressure recorded at 15.4 ± 6.9 mm Hg. No pressure decline was observed over 4 weeks, indicating persistent, stable endoleaks.
Conclusions:
This research successfully developed a novel type IIa endoleak aneurysm model, providing a robust experimental platform for the advancement of EVAR studies and the development of sac-filling materials.
Clinical Impact
This study presents an innovative aneurysm model that effectively simulates a bioactive environment within the aneurysm sac and exhibits the characteristics of Type II endoleaks, responding to the pressing demand for appropriate models aimed at evaluating aneurysm sac-filling methodologies. By employing in situ arterial mechanical injury along with dilation techniques, this model facilitates a straightforward, swift, and highly reproducible method for creating an active aneurysm wall. Furthermore, it reproduces a persistent Type II endoleak through the internal iliac artery, thereby authentically mirroring the hemodynamic conditions seen in patients. In this way, this advancement equips clinicians with an essential resource for exploring novel materials and techniques, which could enhance patient outcomes in endovascular aneurysm repair interventions.
Introduction
Endovascular aneurysm repair (EVAR) is a critical treatment for abdominal aortic aneurysms (AAAs), with benefits over open surgery due to its minimally invasive nature. 1 However, endoleaks, caused by incomplete aneurysm sac exclusion and persistent blood flow, can reduce EVAR’s effectiveness and increase the need for re-interventions.2,3 Type II endoleak (T2EL) is the most common complication following EVAR, with the highest incidence among all endoleak subtypes. While some cases resolve spontaneously, a subset of T2ELs persists, characterized by a progressive increase in intra-sac pressure and continued aneurysm expansion. Persistent endoleaks significantly raise the risk of rupture, necessitating secondary intervention. Follow-up observations suggest that, in patients with persistent T2EL after EVAR, aneurysm sac enlargement (≥5 mm) occurred in 27.4% of cases—a proportion notably greater than the 2.7% reported in those without such endoleaks. In addition, about 14.9% of T2EL patients ultimately underwent reintervention as a result of sac expansion, which again contrasts sharply with the much lower rate of 0.7% seen in patients free of T2EL. T2ELs are significantly associated with late adverse events, including aneurysm sac enlargement, reintervention, rupture, and AAA-related mortality. 4 These findings underscore the urgent need to deepen our understanding of T2EL pathophysiology and to develop more effective therapeutic strategies.
To address the persistent sac expansion and rupture risk associated with persistent T2ELs, researchers propose the technique of embolization and sac-filling, which uses diverse embolic agents to fill and seal the aneurysm sac, aiming to eliminate the residual sac and the risk of endoleak. 5 As exploration of this technique and research on embolic agents advance, the lack of an endoleak aneurysm model becomes a significant obstacle to research progress.
On the one hand, there is a dearth of aneurysm models. Although existing patch-based aneurysm models in large animals morphologically resemble human aneurysms, the graft materials lack local blood supply and biological activity, limiting their application in studies of the body’s natural biological responses.6,7 Conversely, while pharmacologically induced aneurysm models in small animals demonstrate better biological relevance, the induction agents are expensive, the modeling process is time-consuming, and there is significant individual variation in aneurysm location, morphology, and severity, 8 making them difficult to apply in large animals and unsuitable for evaluating surgical materials and embolic agents.9,10 However, these factors are pivotal in ascertaining the long-term stability and efficacy of the sac-filling materials. On the other hand, and more importantly, T2EL models are scarce. Existing endoleak models simulate type III endoleaks through stent-graft puncture, 11 but there have been no reports of animal models for T2ELs to date. However, T2ELs are the most common clinically and represent the primary research target for aneurysm sac embolization techniques.
This study therefore seeks to establish a biologically active T2EL aneurysm model that can serve as a platform for investigating novel sac-filling materials. The model must capture the essential biological processes that characterize endoleaks—hemodynamic patterns, interactions between tissue and materials, and the biological responses triggered by embolic agents. Beyond these fundamental aspects, it should also mirror the intricate biological dynamics within the aneurysm sac itself, encompassing phenomena such as thrombus formation and subsequent tissue remodeling. Such a model would provide a solid foundation for evaluating how effectively embolic materials can prevent endoleak recurrence while maintaining stability over extended periods.
Materials and Methods
Animals and General Procedures
Sixteen-week-old male Sprague Dawley (SD) rats (weight: 260-300 g) were supplied by Beijing Vital River Laboratory Animal Technology Co., Ltd. Rats were housed in a temperature-controlled room and kept on a 12:12 hour light-dark cycle with free access to food and water. During the course of the study, the aneurysm model exhibited consistent and stable characteristics. In comparable model-based studies, the inclusion of a minimum of 3 rats per experimental group is typically suggested. However, taking into account potential experimental losses and procedural uncertainties, the final group size was set at 5 rats per group, based on discussions with a statistical expert. A total of 20 rats were randomly assigned to 4 groups: a sham surgery group and 3 surgical groups. The sham surgery group underwent vascular exposure without any ligation or mechanical dilation. Rats in the 3 surgical groups were euthanized at 1, 2, and 4 weeks after the surgery for tissue collection. All animal experiments were conducted in accordance with the ARRIVE guidelines (Supplemental File 1) and the Guide for the Care and Use of Laboratory Animals (NIH) 12 and were approved by the institutional animal care and use committee of hospital.
Establishment of an Aneurysm Model With Endoleak
Rats were fixed in the stereotaxic apparatus (Alcott Biotech) with continual 3% inhaled isoflurane for gaseous anesthesia. The common iliac artery, external iliac, and internal iliac artery were surgically exposed. The distal end of the external iliac artery and the proximal end of the common iliac artery were ligated, the internal iliac artery became the only branch of the target area, and the internal iliac artery was transiently occluded using a vascular clamp. A minor incision was created at the common iliac artery. A 1-ml syringe needle (0.45 mm × 16 mm, WEGO) is inserted into the common iliac artery through the incision, a 4-0 suture (MERSILK, Johnson & Johnson) is used to close the gap between the syringe needle and the vascular intima at the distal end of the rupture with a slip knot, and normal saline (NS) was infused while maintaining constant pressure. This induced mechanical trauma to the arterial wall, causing the artery to expand to 1.5-2 times its original diameter, thus establishing an aneurysm model. Then, the clamp was removed, and the slip knot was cut into a square knot to completely close the proximal end of the aneurysm sac, allowing reverse perfusion of blood flow from the internal iliac artery to the aneurysm sac to create a type IIa endoleak model (Figure 1).
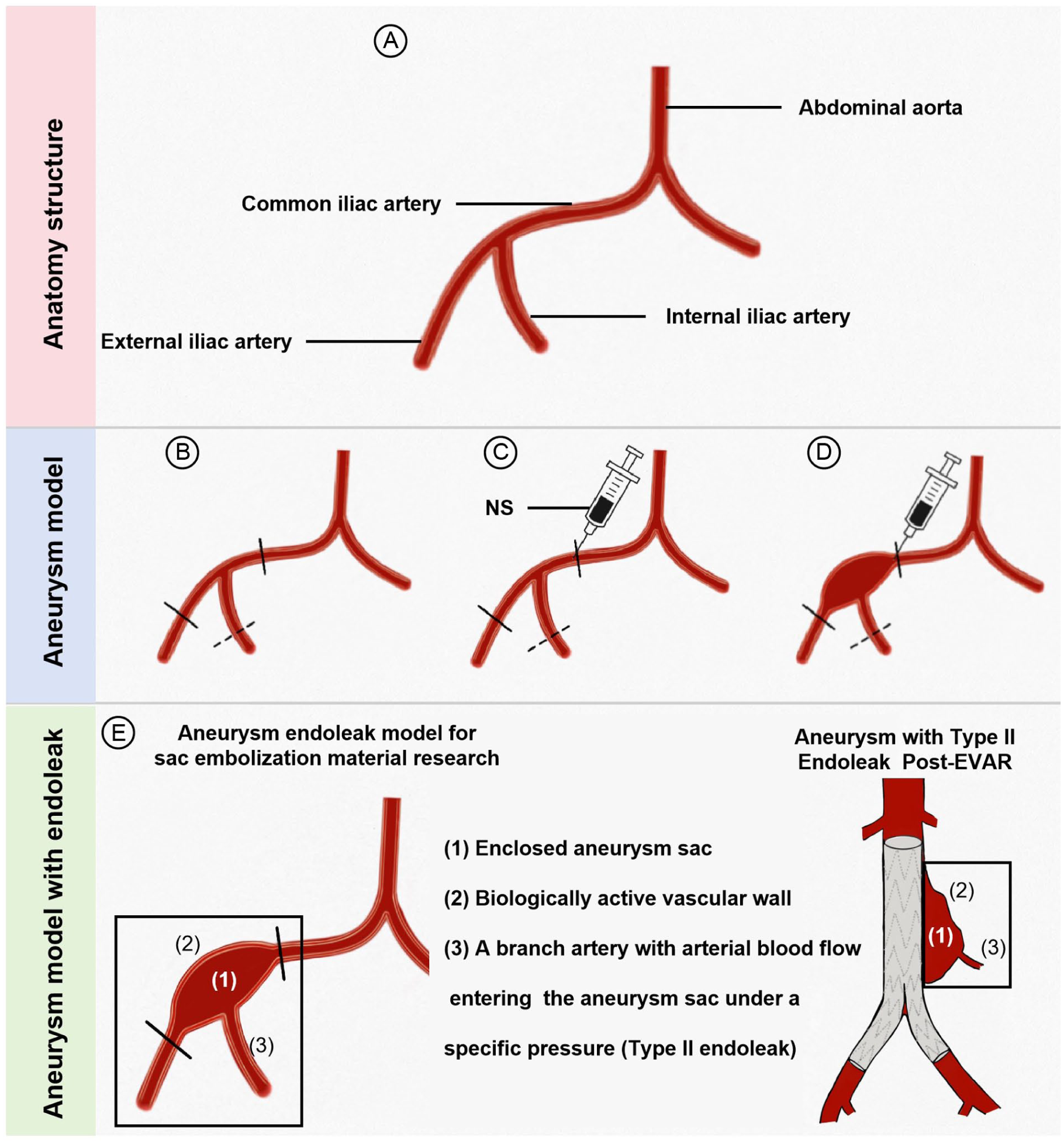
Establishment of an aneurysm model with endoleak. (A) The common iliac artery, external iliac artery, and internal iliac artery were surgically exposed; (B) the distal end of the external iliac artery and the proximal end of the common iliac artery were ligated, and the internal iliac artery was transiently occluded; (C) a syringe was introduced into the common iliac artery; (D) normal saline (NS) was infused while maintaining constant pressure; (E) the clamp was removed, allowing reperfusion from the internal iliac artery to create an endoleak model.
After surgery, each rat received intra-muscular injections of penicillin G at a dosage of 50 mg/kg/day for 1 week to prevent infection.
Measurements of Blood Pressure and Heart Rate
To identify the existence of endoleak, the levels of systemic and intra-aneurysm blood pressure (BP) and heart rate (HR) in rats were recorded. Briefly, before surgery, the left femoral artery was cannulated to monitor the BP of systemic circulation in all rats of model groups. After the clamp was removed in the modeling surgery, aneurysm BP was measured for all rats of model groups, with the arterial aneurysm cannulated. Then, before tissue harvest at 1 week, 2 weeks, and 4 weeks after surgery, the arterial aneurysm was cannulated again to detect the BP, which proved that the blood flow continued to flow back to the aneurysm sac through the internal iliac artery, and the endoleak persisted.
HR was derived from the BP pulse. Signals were recorded by the PowerLab system (AD Instruments) for at least 10 minutes.
Histological Analysis
Arterial tissue was harvested in the modeling location, which was then fixed in 4% paraformaldehyde, dehydrated, and embedded in paraffin to make a tissue chip. Hematoxylin and eosin (H&E) staining, Masson’s trichrome staining, and elastic Verhoeff-Van Gieson (EVG) staining were performed on 5-μm sections as previously described. H&E staining was used to assess tissue morphology, cell arrangement, and overall tissue architecture. Masson’s trichrome staining is used to identify connective tissue in tissues, such as collagen fibers, as well as to evaluate extracellular matrix (ECM) fibrosis and tissue remodeling in vascular tissues. EVG staining was used to highlight elastic fibers in tissues to assess the integrity and structure of elastic fibers in arteries. Elastic fibers are an important component of the vascular wall, providing vessel flexibility and strength. Briefly, the sections were stained using the HE Staining Kit (Solarbio) and Masson’s Trichrome Stain Kit (Solarbio). For EVG staining, the sections were immersed in EVG solution for 30 minutes, followed by incubation with ferric chloride differentiation solution until the background was gray-white. Then, the sections were re-stained with Van Gieson’s solution. After dehydration using 100% ethanol, the sections were photographed under a light microscope. The histological results were observed and photographed using a microscope of Nikon (ECLIPSE CI).
Statistical Analysis
The experimental data were analyzed with GraphPad Prism software, which was presented as mean ± standard deviation. Differences in the sham and model groups were analyzed by unpaired t-test. Differences among multiple groups were analyzed by one-way analysis of variance (ANOVA). Changes in BP at 0, 1, 2, and 4 weeks after the surgery were measured by one-way repeated measures ANOVA. Differences in systemic and aneurysm HR at 0, 1, 2, and 4 weeks after surgery were measured by two-way ANOVA.
Results
Twenty rats were randomly allocated across 4 groups. The sham group was subjected to surgical exposure of the vessels without ligation or mechanical dilation. The surgically manipulated groups were euthanized at postoperative time points of 1 week, 2 weeks, and 4 weeks for tissue collection, corresponding to the 1-week, 2-week, and 4-week groups, respectively. Fifteen rats in the surgical group successfully underwent the surgical procedure and survived until the endpoint of euthanasia. Four weeks after modeling, the mortality rate among the animals was 0%.
Aneurysm Modeling Efficacy Assessment
Before the harvest of aneurysmal tissue, we initially assessed the maximum diameter of the aneurysms in vivo. The results demonstrated a significant increase in aneurysm diameter in the Model group (1-week, 2-week, and 4-week groups) compared to the sham group. No significant differences in aneurysm diameter were observed at 1, 2, and 4 weeks after modeling (Figure 2A). The structural characteristics of aneurysm walls were analyzed by the H&E and EVG staining of the aneurysm cross-sections, as depicted in Figure 2B and C. The Model group exhibited a significantly increased diameter compared to the sham group (Figure 2D, P < .05). After surgery, the structural characteristics of the arterial wall did not show a significant change with time. The assessment of aortic wall structural damage was based on the analysis of elastic fiber breakage (Figure 2C). The 4W group displayed a significantly higher degree of elastic fragmentation compared to the sham group (3.600 ± 0.547 vs. 1.200 ± 0.447; P < .001) (Figure 2E).
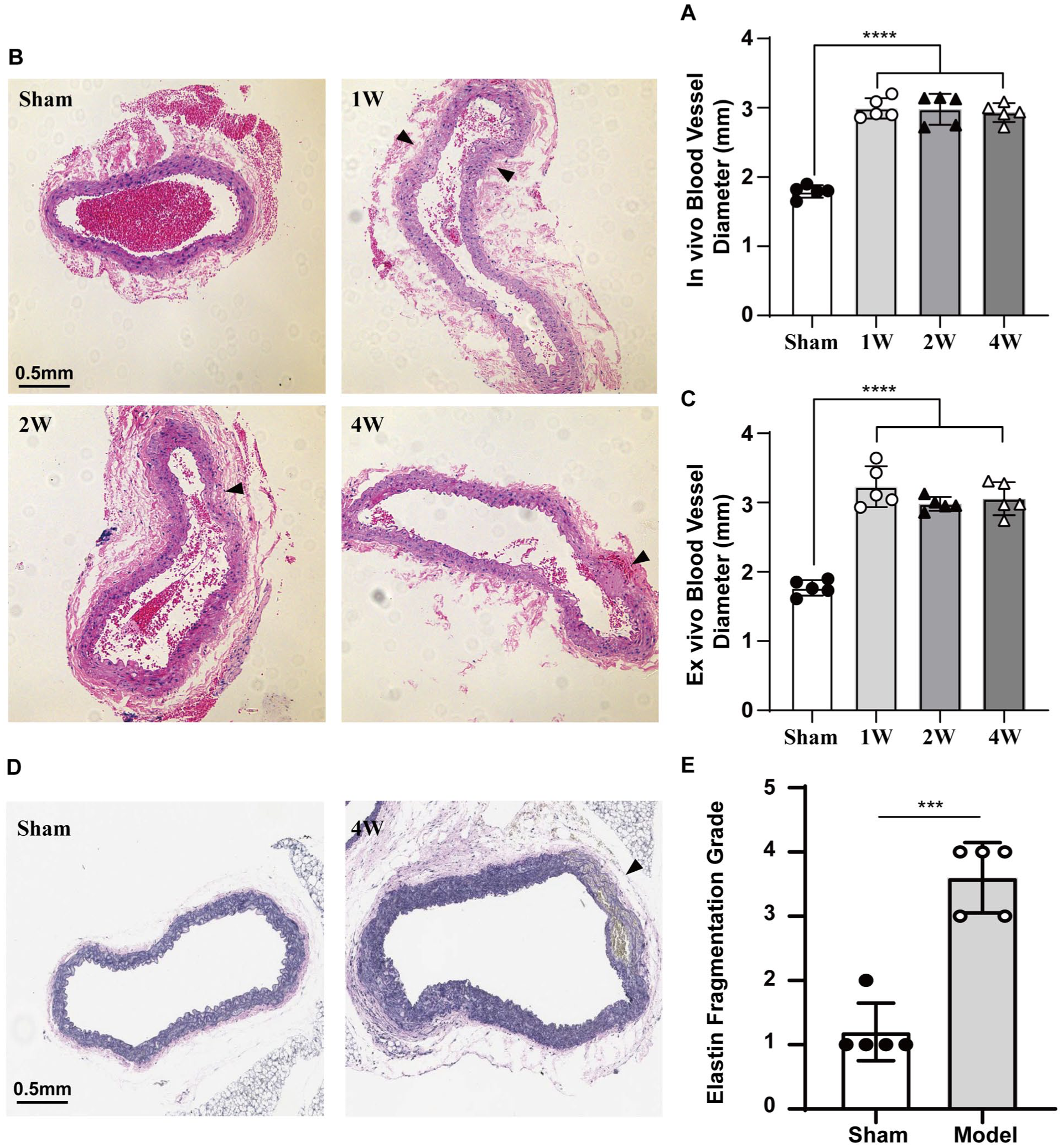
Validation of the aneurysm characteristics in the model. (A) In vivo vessel diameter in model group (1 week, 2 weeks, and 4 weeks after modeling) and sham group; (B) representative hematoxylin and eosin staining of the vessel cross-sections in model group (1 week, 2 weeks, and 4 weeks after modeling) and sham group (arrows: elastin fragmentation); (C) the blood vessel diameter in model group (1 week, 2 weeks, and 4 weeks after modeling) and sham group; (D) representative elastic Verhoeff-Van Gieson staining of the vessel cross-sections in model group (4W after modeling) and sham group, (arrows: elastin fragmentation); (E) the elastin fragmentation grade in model group and sham group. Values are mean ± SE; n = 5 in each group. ***P < .001, ****P < .0001.
Endoleak Modeling Efficacy Assessment
Regurgitant arterial blood is a key factor in the occurrence of endoleaks. After completing the model construction, we found that arterial blood could be continuously aspirated within the aneurysm using a syringe, confirming the presence of blood reflux in the internal iliac artery and endoleak formation (Figure 3A).
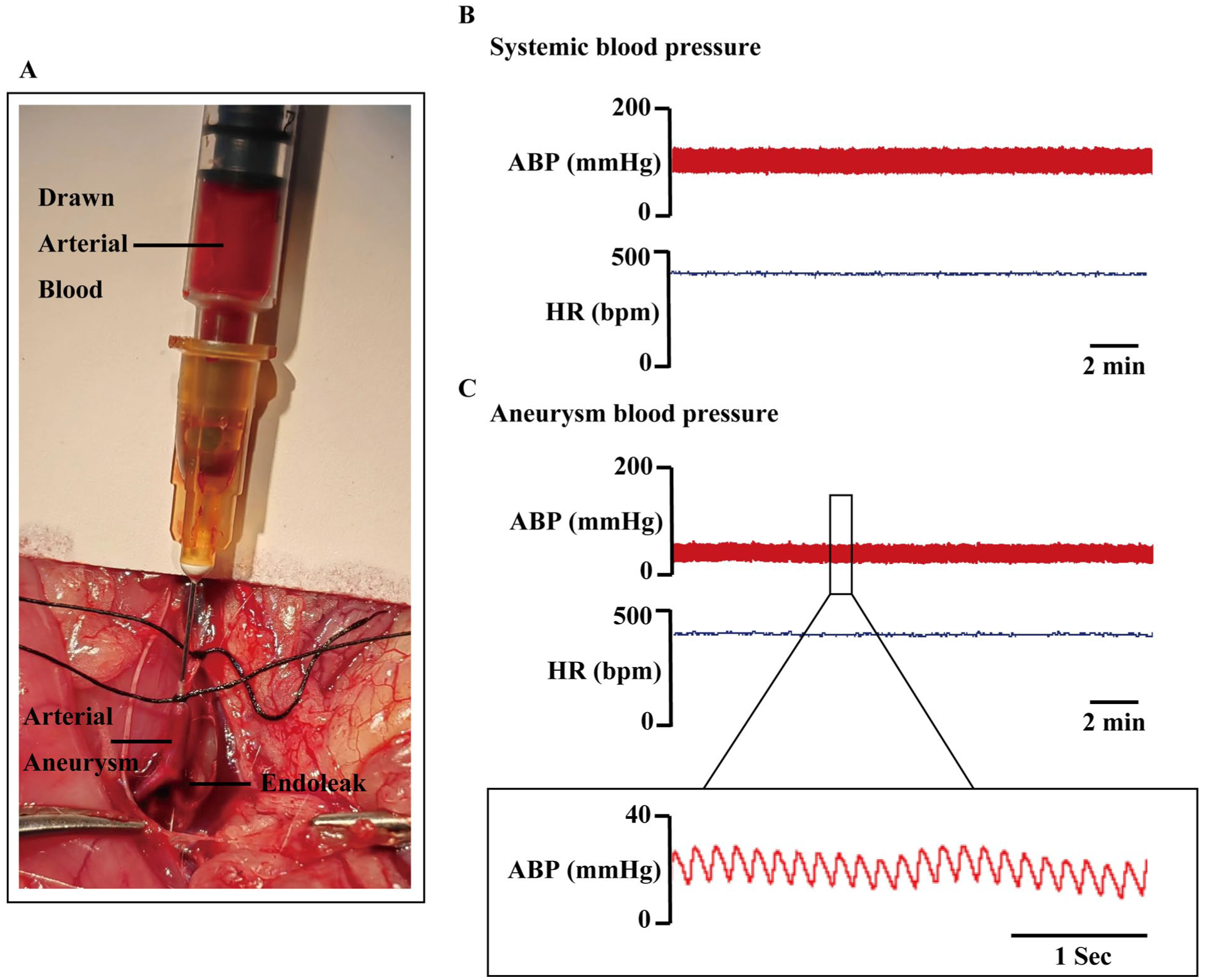
Validation of the endoleak characteristics in the model. (A) Drawn arterial blood from the aneurysm after modeling demonstrated the presence of blood reflux from the internal iliac artery; (B) representative original recordings of arterial blood pressure (ABP) and heart rate (HR) of systemic circulation; (C) representative original recordings of arterial blood pressure (ABP) and heart rate (HR) of aneurysm sac.
We further assessed the severity of the endoleak by measuring the intra-aneurysmal pressure. The results indicated that the mean arterial pressure (MAP) in rats was 98.0 ± 5.1 mm Hg, whereas the intra-aneurysm MAP measured 28.2 ± 5.4 mm Hg (Figure 3B and C), representing approximately 28.7 ± 4.9% of the systemic MAP. As illustrated in Figure 3, the BP within the aneurysm sac displayed a characteristic arterial waveform. The pulse pressure (PP) reached 15.4 ± 6.9 mm Hg in the aneurysm. These findings substantiate the presence of internal leakage in the aneurysm model. More importantly, 1, 2, and 4 weeks after the modeling surgery, there was no significant reduction in the intra-aneurysmal BP, while the BP fluctuation rate within the aneurysm sac shows no significant difference from the systemic HR (Figure 4, Table 1). These results suggested that the endoleak persists, and its intensity remains stable.
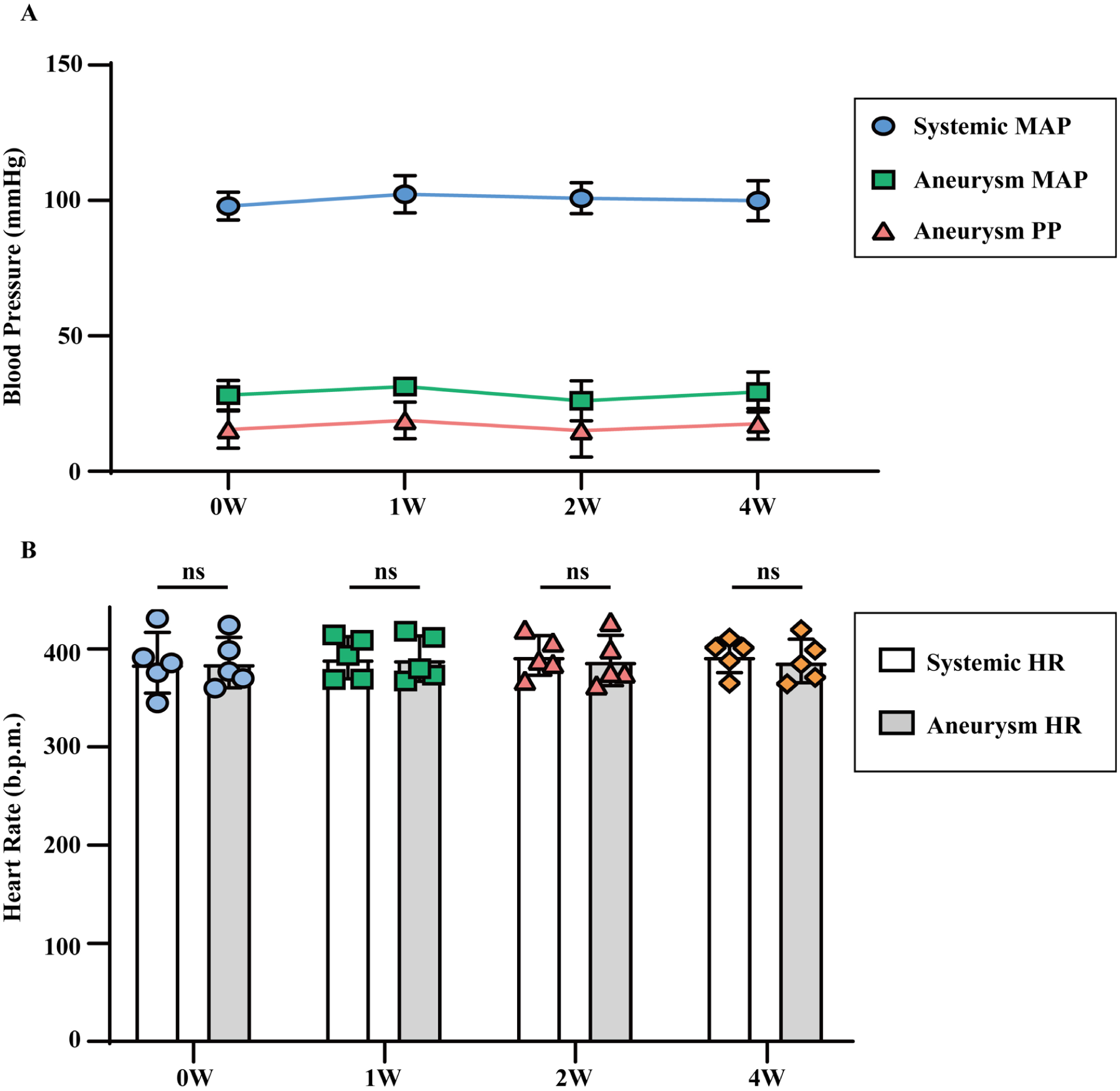
Validation of the endoleak characteristics in the model. (A) Systemic mean blood pressure (MAP), aneurysm MAP, and aneurysm pulse pressure (PP) in the model, 0, 1, 2, and 4 weeks after modeling; (B) systemic heart rate (HR) and aneurysm HR in the model, 0, 1, 2, and 4 weeks after modeling. Values are mean ± SE; n = 5 in each group.
The Systemic Blood Pressure and Intra-Aneurysm Blood Pressure of Rats.

Discussion
The objective of this study is to develop an aneurysm model that closely mimics the disease state associated with a T2EL. The model consists of an aneurysm sac that is expanded in situ from a structurally compromised rat vessel wall. This aneurysm endoleak model exhibits 2 significant characteristics: First, it incorporates a bioactive aneurysm sac, and second, it is characterized by a persistent T2EL. Thus, this model serves as a suitable animal model for investigating materials used to fill the aneurysm sac.
Initially, we compared the similarities and differences between this model and existing aneurysm models. Current animal models of aneurysms are mainly divided into 2 categories: one constructed by artificially suturing arterial patches, and the other induced by local or systemic pharmacological agents causing vascular injury.13,14 The patch aneurysm model, commonly used in large experimental animals, such as swines and dogs, is morphologically similar to human thoracoabdominal aortic aneurysms, thus widely used in the study of endovascular stents and other intra-luminal implants.13,15 However, the transplanted patches, often made of artificial vessels, decellularized bovine jugular veins, or autologous femoral veins, lack local blood supply and biological activity. This hinders its application in studies considering the body’s innate biological responses. 16 On the other hand, pharmacologically induced aneurysms in small laboratory animals, like mice, closely resemble the biological characteristics of human aortic aneurysms and are frequently used in research on aneurysm pathogenesis and pharmacological intervention. However, the drugs, such as β-aminopropionitrile and angiotensin II, are costly, and the modeling process is lengthy. 17 In addition, there is significant individual variation in the location, morphology, and severity of the aneurysms. These make it challenging to use pharmacologically induced aneurysms in larger animals and the study of surgical materials.18,19 Therefore, a biologically active and consistently available aneurysm model is currently lacking but is in urgent need for embolic agents studying. The aneurysm model developed in this study can meet these requirements effectively. First, since the aneurysm sac originates from the in situ, dilated, and structurally damaged arterial wall, it retains biological activity similar to that of human aortic aneurysm sacs. Moreover, the location and severity of the aneurysm are highly controllable by fixing the infusion pressure and monitoring the vessel wall diameter. Notably, the design of this modeling approach does not rely heavily on the size of the experimental animals, suggesting potential adaptability to larger animal models. However, further validation is required to confirm its feasibility in such contexts.
For endoleak models, existing models puncture covered stents during EVAR surgery in pigs or dogs to create type III endoleaks. However, there is a lack of models that simulate T2ELs, which are the most common type of endoleak in clinical practice and the primary target for aneurysm sac-filling techniques. 20 T2ELs originate from branch arteries within the aneurysm sac, with a reflow pressure lower than the main systemic circulation pressure and a similar rhythm. 21 In our model, we have preserved the open internal iliac artery as a branch vessel within the aneurysm sac, and arterial blood reflux into the aneurysm sac continuously through the internal iliac artery to simulate the clinical scenario of T2ELs. This allows for the assessment of not only the biological activity of sac-filling materials but also their resistance to blood flow.
We evaluated the efficacy of the arterial aneurysm model with type IIa endoleak from 2 aspects: the morphology and structure of the aneurysmal vessel, as well as the presence and extent of endoleak. 14 Regarding the aneurysmal vessel, luminal dilation and vascular wall damage are the primary indicators. We measured the maximum diameter of the in vivo aneurysm and the vascular diameter in tissue sections, finding that the vascular diameter in the model group increased by more than 50% compared to the sham group, with minimal intra-group variation and no significant progression or contraction over time. Further examination of the vascular wall’s elastic fibers through EVG staining revealed disorganized alignment, increased spacing, and instances of rupture in the model group. In addition, elastin fragmentation grade results indicated that the degree of structural damage in the model group was significantly greater than that in the sham group. These findings suggest that the model meets the diagnostic criteria for aneurysms and is ready for use immediately after modeling, exhibiting high consistency. In terms of endoleak, in this model, the open internal iliac artery serves as the primary source of endoleak, which is consistent with the principle of T2EL following EVAR (Figure 1). T2EL is the most common type of endoleak after EVAR and is the main target for aneurysm sac filling. The aspiration of arterial blood from the aneurysmal sac and the arterial waveform detected within the sac confirmed the presence of an endoleak. The intra-aneurysmal pressure reached 25%-30% of the MAP, similar to that observed in patients with endoleaks in thoracoabdominal aortic aneurysms. Importantly, from 0 to 4 weeks after modeling, there were no significant changes in intra-aneurysmal pressure or PP, indicating the persistent presence of the endoleak. Thus, our study successfully validated the endoleak aneurysm model through both aneurysm modeling and endoleak assessment.
This study also has certain limitations. A significant limitation of this model pertains to the relative size ratios of the aneurysm and branch vessels when compared to those found in human pathology. Specifically, the diameter ratio between the aneurysmal sac and the abdominal aorta in rats is smaller than the ratio typically encountered in humans, where the sac can expand to more than double the original vessel diameter. In addition, the preserved internal iliac artery, used as the branch vessel to simulate a T2EL, has a comparatively larger diameter. This situation diverges from clinical scenarios, where endoleak sources—such as lumbar or inferior mesenteric arteries—are considerably smaller in caliber. These anatomical differences may have implications for hemodynamic parameters within the sac, including reflow pressure and flow patterns, which could, in turn, impact the translational relevance of embolic material performance. Future research should aim to enhance the model by more accurately replicating the size ratios observed in clinical cases, especially during the transition to larger animal models.
While the arterial aneurysm model presented here offers a useful experimental system for studying sac-filling materials, it is essential to recognize its considerable constraints in mimicking the pathology observed in human disease. One key limitation stems from the model’s anatomical basis in the rat iliac artery, a site that naturally differs from the human abdominal aorta in dimensions, location, and hemodynamic forces. Consequently, the pathological responses captured may not fully reflect the clinical spectrum. For instance, although cellular behaviors such as smooth muscle cell apoptosis and immune infiltration are observed in rats, these responses may not fully align with those in humans, where fibroblast activity and smooth muscle cell phenotypic shifts tend to be more complex. Likewise, while animal models generally exhibit acute, localized inflammation, human aneurysms are characterized by chronic and persistent inflammation. Structurally, animals tend to show thinner vascular walls and simpler alterations in the ECM, whereas human aneurysms involve more intricate changes, including collagen deposition and matrix remodeling. Notably, features like calcification and thrombus formation are less common in animals but are more prevalent in human aneurysms. In conclusion, although animal models offer valuable insights into basic mechanisms, they do not fully capture the complexity of human aneurysm progression, and caution should be exercised when extrapolating findings from animal studies to human aneurysm pathology. These discrepancies do not undermine the model’s primary objectives. The model aims to establish a biologically active aneurysmal sac, facilitating the study of immune cell infiltration, surrounding tissue inflammation, the implantation of tissue cells within the sac, angiogenesis, fibrosis, and other related processes that occur after the introduction of a sac-filling material.
Stent grafts or small cannulas were not used for revascularization during model establishment, as this study primarily focused on the bioactive effects within the residual lumen. While stent placement may partially reduce retrograde flow from the internal iliac artery, its absence is unlikely to significantly affect the observed responses. This simplified model is intended for early-stage evaluation of sac-filling materials. For future studies, particularly in large animals, stent implantation may be required to better mimic clinical conditions.
Although our current model is established in rats, we recognize the potential advantages of extending it to larger animals, such as pigs or dogs. These larger models, with anatomical and physiological similarities to humans, offer more accurate biological responses and pathological features, including vascular wall strength, structural changes, and inflammatory responses, thereby enhancing the translational potential of our findings. However, such studies face technical, ethical, and resource-related challenges, and we intend to explore the feasibility of applying our aneurysm model to larger animals in future studies. This aneurysm model, defined by persistent T2ELs and a biologically active sac, offers significant potential for the preclinical evaluation of sac-filling embolic materials, particularly those intended to address endoleaks following EVAR. Due to its structural similarity to clinical aneurysm sacs and its reproducibility, it provides a reliable platform for assessing the biocompatibility, long-term sealing performance, and degradability of novel embolic agents. In addition, the stable endoleak environment enables controlled studies on pressure modulation, thrombus formation, and the interactions between embolic materials and vessel walls over prolonged periods. With further validation in larger animal models, this approach has the potential to effectively bridge the translational gap in aneurysm treatment strategies.
Based on our current results, we have constructed an aneurysm model featured by a biologically active arterial wall, an expanded and structurally compromised vessel, and a consistent endoleak. This model demonstrates potential applicability in the study of aneurysm sac-filling materials.
Supplemental Material
sj-docx-1-jet-10.1177_15266028261454345 – Supplemental material for Development of a Rat Arterial Aneurysm-Endoleak Model for EVAR Sac Filling Material Research
Supplemental material, sj-docx-1-jet-10.1177_15266028261454345 for Development of a Rat Arterial Aneurysm-Endoleak Model for EVAR Sac Filling Material Research by Jie-Fu Fan, Kang-Jie Chai, Hao Zhang, Xiao-Nan Wang, Yang-Kai Wang, Zhi-Yong Li and Lei Zhang in Journal of Endovascular Therapy
Footnotes
Ethical Considerations
All animal housing and experiments were conducted in strict accordance with the institutional Guidelines for Care and Use of Laboratory Animals at Changhai Hospital, Navy (Second) Military Medical University. All animals were cared for in strict accordance with the Guide for the Care and Use of Laboratory Animals (NIH Publication No. 85-23, revised 1996).
Author Contributions
Jie-Fu Fan: Conceptualization, Methodology, Formal analysis, Writing–original draft, Writing–review and editing, Project administration.
Kang-Jie Chai: Conceptualization, Investigation, Data curation, Writing–original draft, Writing–review and editing, Supervision.
Hao Zhang: Conceptualization, Formal analysis, Investigation, Visualization, Writing–original draft, Writing–review and editing.
Xiao-Nan Wang: Resources, Validation, Formal analysis.
Yang-Kai Wang: Data curation, Validation, Formal analysis.
Zhi-Yong Li: Conceptualization, Supervision, Project administration, Funding acquisition.
Lei Zhang: Conceptualization, Supervision, Project administration, Funding acquisition.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the funding of Shanghai Science and Technology Innovation Action Plan 2021 (21Y11909200), Hospital 234 Discipline Peak Plan Funding (2020YXK050), Biomedical Technology Support Special Project of Shanghai Science and Technology Innovation Action Plan 2020 (20S11901900), and Medical Special Project of Shanghai (202240388).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.