
Abstract
The field of endovascular surgery continues to evolve rapidly with the introduction of novel techniques and devices. Among the most significant advances in recent decades is the development of branched and fenestrated endografts, which have become the cornerstone of treatment for complex aortic pathologies, including thoracoabdominal aortic aneurysms. These devices enable the preservation of visceral vessel perfusion while allowing for effective aneurysm exclusion. However, their use introduces technical challenges that demand a high level of expertise, particularly during the catheterization of target vessels. Target vessel cannulation is widely recognized as one of the most technically demanding and time-consuming steps in fenestrated and branched endovascular aneurysm repair (FEVAR and BEVAR, respectively). This difficulty is often exacerbated in patients with hostile anatomy – such as extreme aortic angulation, severe vessel tortuosity, small-caliber, or heavily calcified arteries. In such settings, prolonged attempts at vessel catheterization may increase the risk of complications, including ischemic injury to abdominal organs, dissection, perforation, or embolization due to plaque disruption. To address these procedural challenges, several bailout strategies have been introduced. These techniques are generally reserved for non-standard cases and are not employed in routine or straightforward anatomies. One such strategy is the snare-ride technique, which has gained recognition as a practical and reproducible approach using widely available endovascular tools. It involves the snaring of a guidewire from the aortic component and advancing the wire and the snare assembly into the target vessel, using femoral access. While effective, this technique has raised concerns about its potential to cause endothelial trauma, particularly when the snare is advanced into a diseased vessel. To mitigate these risks, we propose modifying the traditional snare-ride technique. In this article, we introduce the Modified Snare-Ride Technique, a bailout approach designed to enhance the safety and effectiveness of target vessel cannulation in anatomically complex settings. After obtaining access to the intended target vessel with a stiff supporting wire, large sheath, and a deflecting sheath for control, through-and-through access is obtained from the portal to the contralateral stiff sheath. Once established, the lower stiff sheath is advanced to the origin of the target vessel, thereby pinning the through-and-through wire in position near the target vessel orifice. In doing so, the portal sheath can then be advanced along the through-and-through wire to the vessel origin for easy cannulation and delivery of the bridging stent. The modification avoids advancing the entire snare system into the vessel and instead uses a through-and-through access to improve pushability, control, and deliverability. This adjustment minimizes mechanical damage to the vessel wall and reduces the risk of vascular injury. However, its usability is dependent upon device and sheath size compatibility. By enhancing wire support and control with deflectable sheaths, this modified strategy provides an alternative that can be selectively employed when traditional techniques fail or are unsafe.
Clinical Impact
Target vessel catheterization remains one of the most challenging steps in fenestrated and branched endovascular aneurysm repair, particularly in patients with complex anatomy and unfavorable branch orientation. The modified Snare-Ride technique provides a reproducible bailout strategy that stabilizes sheath positioning at the target vessel origin while potentially reducing the risk of visceral artery injury associated with the original technique. By facilitating target vessel incorporation in difficult anatomical scenarios, this approach may expand endovascular treatment options, improve technical success rates, and reduce the need for more invasive alternative catheterization strategies.
Keywords
Key Findings
A modified Snare-Ride technique is used to achieve through-and-through access and stabilize the delivery sheath at the target vessel origin in cases of hostile anatomy. By avoiding advancement of the stiff snare into the target vessel, the modification may reduce the risk of intimal injury and vessel dissection compared with the classic technique.
Take Home Message
The modified Snare-Ride technique is a practical bailout option when standard target vessel catheterization fails during FB-EVAR.
Table of Contents Summary
This report describes a step-by-step modification of the Snare-Ride technique to allow stable target vessel sheath positioning and safe stent delivery during FB-EVAR in difficult anatomy.
Introduction
In the past 2 decades, the endovascular approach has become the cornerstone in the management of complex anatomy aortic aneurysms, and currently, fenestrated/branched repair (FB-BEVAR) 1 has been widely indicated due to its positive outcomes in terms of early and 5-year morbidity and mortality2,3 even in elderly patients with multiple comorbidities. 4
Despite technological advances, target vessel (TV) catheterization remains one of the most challenging steps of the procedure, especially in cases involving anatomical hostilities such as extreme vessel angulation, tortuosity, ostial stenosis, large gap between the device and TV take-off, or misalignment between branch or fenestration portals and the target ostium. 5 The presence of an aortic dissection further complicates the procedure. Straightforward vessel cannulation is often not feasible due to the presence of the septum, which typically increases the gap distance. In such cases, bailout techniques may be required to achieve successful catheterization. 6
Standard catheterization approaches may be ineffective in these scenarios. As a result, bailout strategies have been developed to ensure technical procedural success. Among these, the “Snare-Ride” technique6,7 has emerged as a valuable maneuver, enabling transfemoral delivery of wires into visceral arteries via snaring.
Although extremely useful and suitable for challenging TV catheterization, especially considering downward branched endografts8,9 used in upward TVs, the main concern about the snare-ride technique is the potential intima layer injury and risk of visceral artery dissection, particularly in patients with diseased and calcified small vessels. This article describes a modification of the classic snare-ride technique to reduce the likelihood of intimal damage and TV injury.
Technique
A 62-year-old male with extensive prior medical history, including hypertension, hyperlipidemia, cerebral vascular disease, thalassemia-associated anemia, asthma, chronic kidney disease, hepatitis B, was referred to our institution with a diagnosis of postdissection aneurysmal degeneration from a type B aortic dissection (TBAD) 6 years prior.
Upon presentation, the computed tomography (CT) scan demonstrated aneurysmal degeneration distal to his prior thoracic endovascular aortic repair (TEVAR), measuring up to 10 cm, which represented a significant increase compared with prior scans.
It was recommended a 4-vessel branched endovascular aneurysm repair (BEVAR) with a patient-specific company-manufactured device, incorporating the celiac trunk, superior mesenteric artery, and bilateral renal arteries.
The repair was performed through bilateral percutaneous femoral access and right brachial artery cutdown.
The celiac trunk, superior mesenteric artery, and right renal artery were successfully catheterized via brachial access without incident. However, due to the large diameter of the aneurysm sac by the left renal artery (LRA; Figure 1), multiple attempts of catheterization from either the brachial or ipsilateral groin were not successful at establishing a stable system for TV stent delivery.
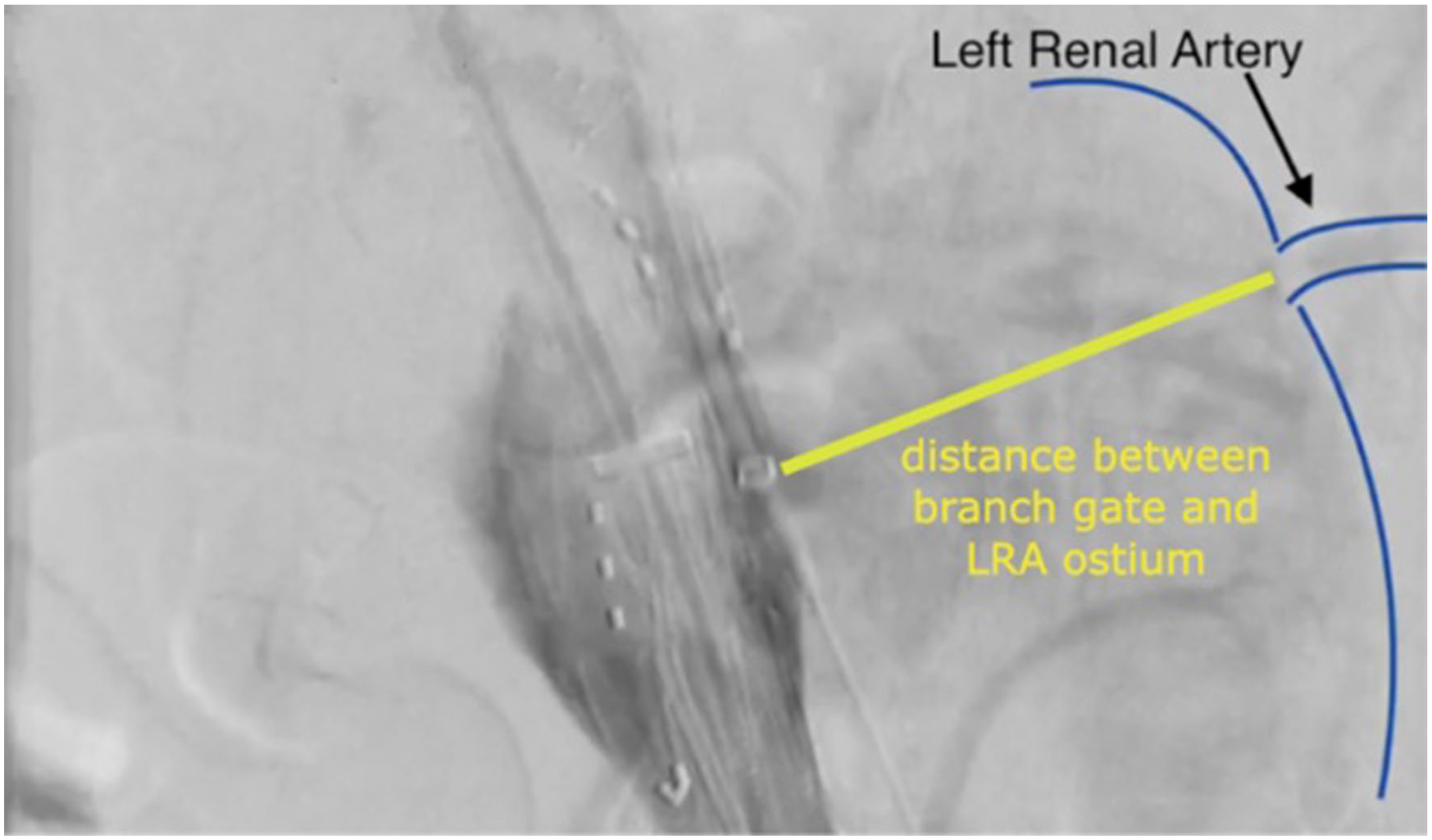
Large distance between the LRA branch gate and the LRA ostium.
A decision was made to perform a modification of the snare ride technique for TV stent delivery. This was accomplished by accessing the LRA from the contralateral groin using a large bore access sheath (Figure 2).
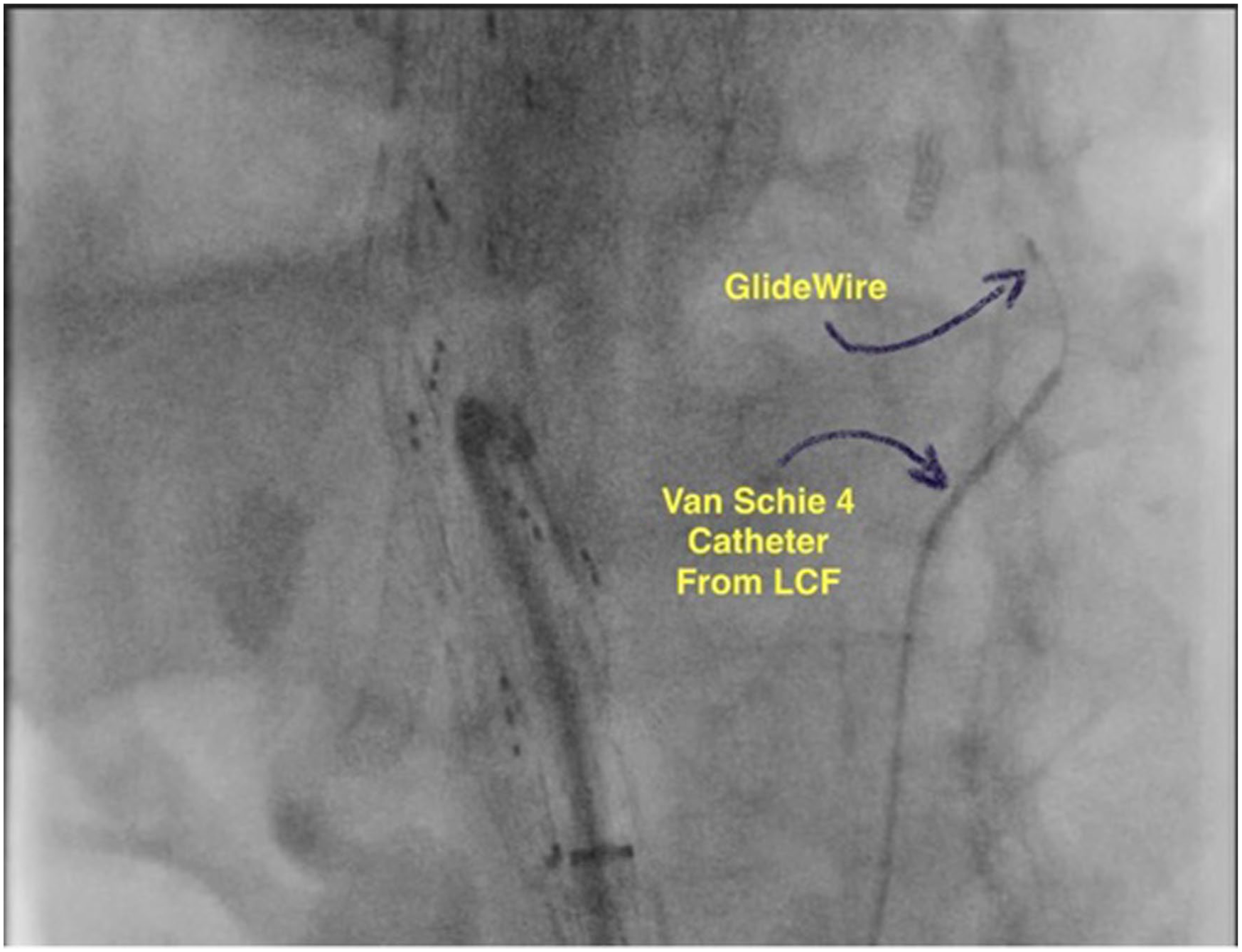
Van Schie 4 and glidewire gained access to the LRA through the false lumen.
The glidewire was then exchanged by a Rosen wire, which was placed into the LRA to provide support, allowing advancement of an 8F sheath (coaxially inside the 12Fr) to the level of the LRA origin (Figure 3).
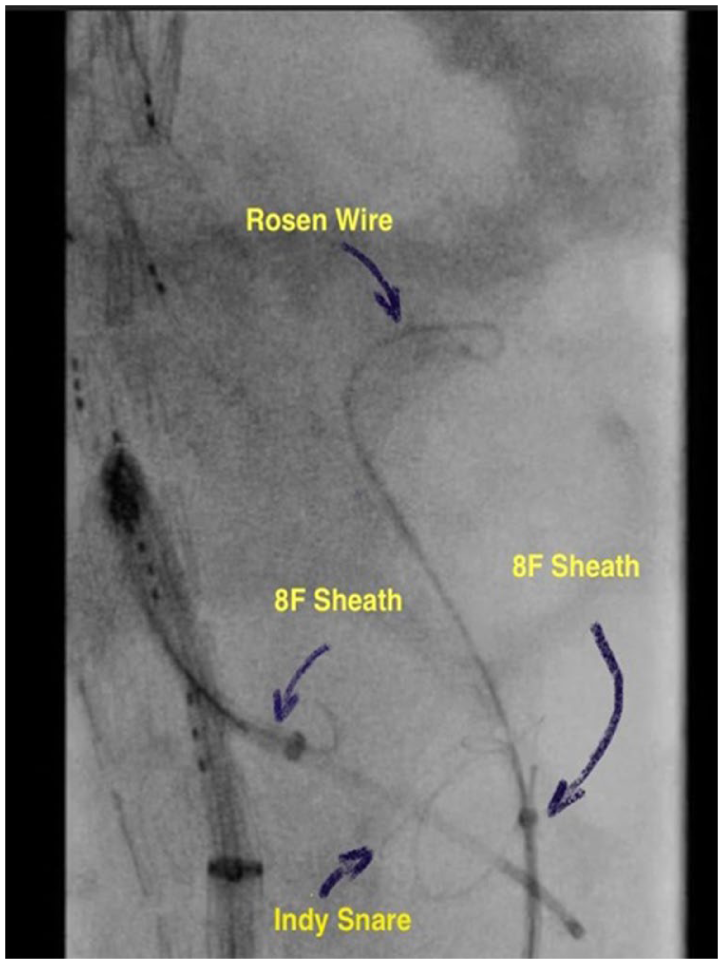
Rosen wire parked into the LRA from the LCFA access. Indy snare opened by the tip of the 8Fr Sheath from the LCFA.
Subsequently, A Metro wire (0.021) was advanced from the right common femoral artery through a 16Fr Aptus sheath and 8F by 90cm sheath from inside of the branched device through the LRA branch gate. An Indy snare system was passed over the LRA Rosen wire from the left femoral. The Metro wire is then successfully snared into the left femoral artery coaxial system, establishing through-and-through access. The contralateral renal access sheath was then advanced to the LRA origin, securing the through-and-through wire at the LRA orifice. The TV delivery sheath (8Fr) was then advanced over the through-and-through wire bringing it into position at the LRA origin. A Kumpe catheter and a glidewire were then advanced into the LRA from the sheath positioned through the device branch portal. After angiographic confirmation of correct positioning, the glidewire was exchanged for a stiffer wire to facilitate delivery of the LRA stent (Figure 4).
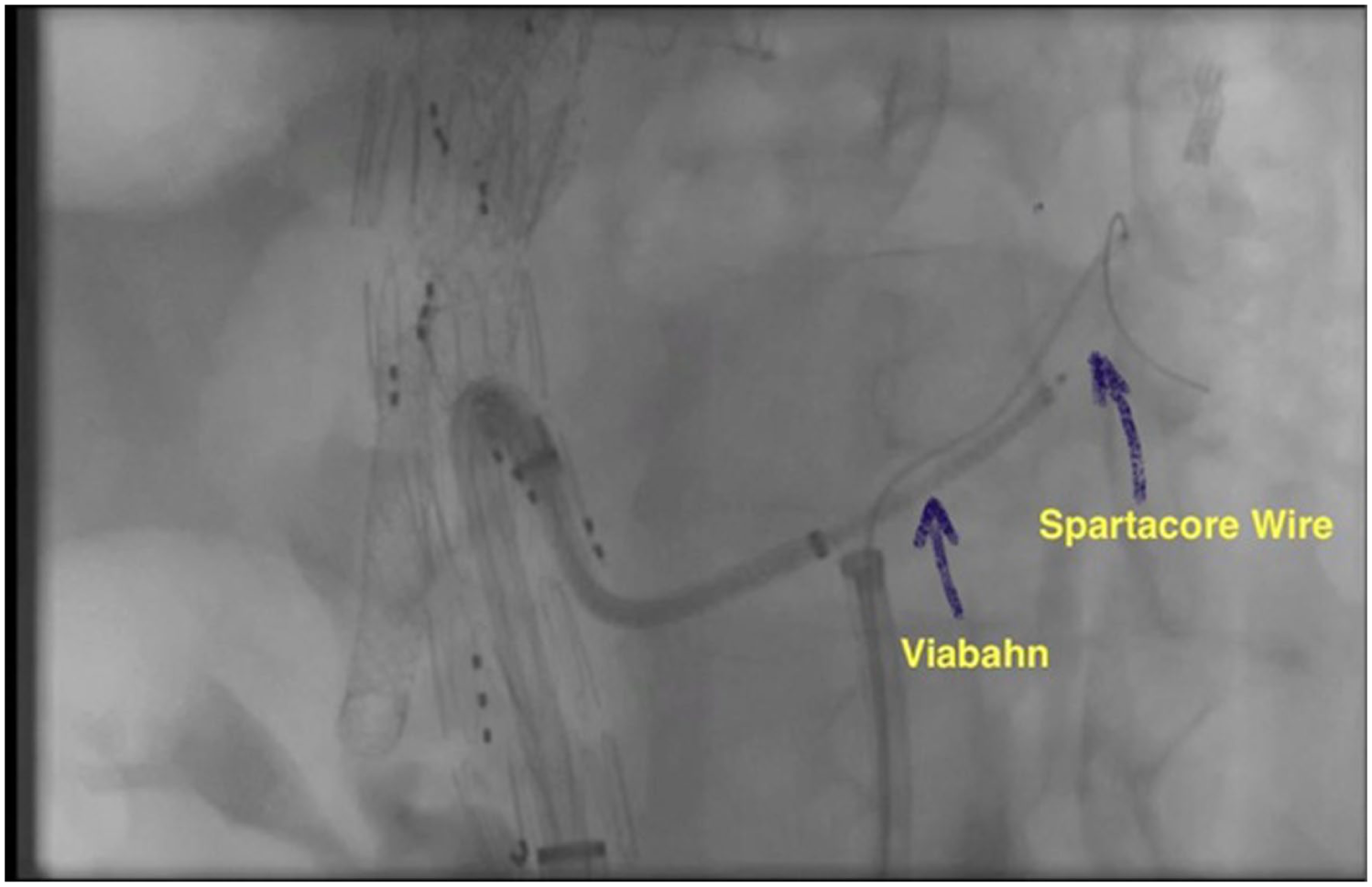
Viabahn stent advanced into the LRA over Spartcore wire.
The complete step-by-step sequence of the modified technique is shown in Figure 5, with a corresponding step-by-step procedural video (Video 1).
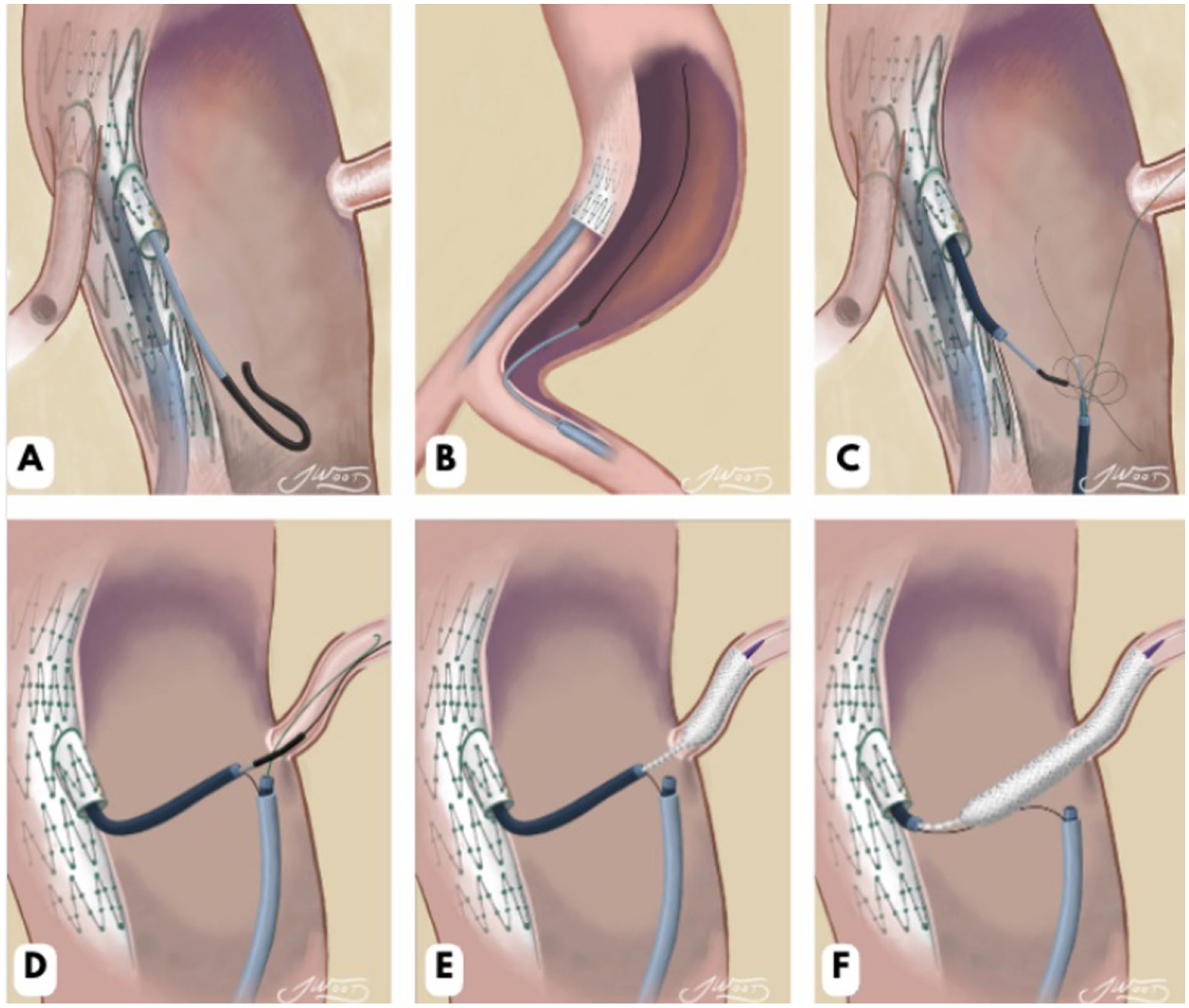
Step-by-step illustration of the modified snare-ride technique. (A-B) Establishment of access and wire positioning across the true and false lumens. (C) Advancement of the Indy snare system over the Rosen wire from the left common femoral artery, with successful snaring of the Metro wire. (D) Creation of through-and-through access with stabilization of 2 coaxial systems at the target vessel origin. (E-F) After parking the Spartacore wire within the left renal artery, the self-expanding stent is advanced and deployed. Illustrations by Dr Jacob C Wood, MD.
Discussion
During FB-EVAR cases with unfavorable anatomy, the standard antegrade catheterization of visceral arteries may not be feasible due to issues such as vessel tortuosity, angulation, heavy calcification, or stenosis. In this scenario, the use of bailout techniques becomes essential to ensure procedural success. 10 In the original snare-ride technique, first published by Ferreira et al, 6 the wire from the device portal is snared and advanced into the TV along with the snare. Although effective, this method has raised concerns because the Indy snare is stiff and not flexible resulting in potential intima layer injury and TV dissection. In this case report, the large aneurysm sac diameter made the LRA catheterization difficult, which was effectively managed by creating through-and-through access and stabilizing the TV delivery sheath at the TV origin.
Many alternatives to manage unfavorable anatomy in TV catheterization have been proposed in the literature. Lérisson et al 10 introduced the elevator technique, which involves pre-cannulation of the TV prior to endograft deployment. A balloon-expandable stent is deployed with its proximal segment extending into the aortic lumen. Subsequently, the sheath is advanced into the stent to flare and elevate its proximal portion inside the branch, therefore facilitating successful catheterization through the gate.
Heideman et al 11 described the balloon-anchoring technique, designed primarily to stabilize catheter position inside the TVs and facilitate safe exchange to a stiff guidewire in complex aortic interventions. Although not initially intended to assist with vessel catheterization, it may serve as a bailout in certain scenarios. A potential limitation of this technique is the theoretical risk of TV injury due to balloon inflation within fragile or diseased arteries.
Another innovative approach was described by Heartault et al, 12 describing translumbar puncture for retrograde catheterization of a kinked left renal stent following fenestrated endovascular aneurysm repair (FEVAR). In this case, standard antegrade and hybrid approaches failed due to stent configuration and patient comorbidities, prompting the use of a translumbar retrograde access route to achieve successful revascularization.
The modified snare-ride technique described in this report offers an additional bailout option for challenging visceral arteries, especially when associated with a large distance between the device and the TV ostium.
Although the need for this adjuvant technique could have been avoided by designing an upward oriented renal branch, waiting for a patient-specific custom manufactured device is not always possible. The technique described does provide a reproducible approach that stabilizes both sheaths at the TV origin, facilitating catheterization and mitigating the risk of TV injury, especially when stenotic and calcified visceral arteries need to be incorporated into the endovascular repair.
Conclusion
The modified Snare-Ride technique represents a feasible and reproducible approach for catheterization of challenging visceral vessels in patients with complex anatomy aortic aneurysms FB-EVAR. This bailout technique provides an additional option in unfavorable anatomy cases and might increase technical success when conventional methods are not feasible.
Footnotes
Authors’ Note
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.A.F., MD: Consulting and clinical trial support from W. L. Gore; consulting from Getinge; research support and clinical trial support from Cook Medical; consulting and clinical trial support from ViTTA; stock options and clinical trial support from Centerline Biomedical. F.E.P., MD: Consultant for Centerline Biomedical with stock options; research support from Cook Medical. V.A.N., MD; V.C.G., MD; and J.C.W.: The authors have no competing interests.
Type of Research
Technical report describing a modified bailout technique for target vessel stenting during fenestrated and branched endovascular repair.