
Abstract
Objectives:
Intramural hematoma (IMH) is characterized by an unpredictable natural history. Thoracic endovascular aortic repair (TEVAR) has increasingly been employed as treatment with limited midterm outcomes reported.
Methods:
To better characterize the natural history of type B IMH and TEVAR outcomes, we reviewed our institutional experience. Data were collected prospectively, and patients followed in a dedicated aortic clinic.
Results:
Since 2001, 40 patients were treated for type B IMH without focal intimal disruption (FID) on initial computed tomography (CT). All patients were initially treated with optimal blood pressure management, pain control, and control CT within 5 to 7 days. Fourteen patients had TEVAR during the index hospitalization due to the presence of a new FID with progression of the IMH thickness or persistent symptoms. Of the remaining 26 patients, 16 required late TEVAR at a mean of 41.3 ± 112.2 months for type B dissection, new FID, or pseudoaneurysm formation. The remaining 10 patients had complete resolution of the IMH on optimal medical therapy (OMT) alone. Patients in the early TEVAR group developed a significantly higher rate of complication than patients treated in the chronic TEVAR phase (78% vs 38%; P = .003). Patients treated with early and late TEVAR had a 5-year survival of 100% and 64.9%, respectively.
Clinical Impact
Favorable outcomes can be achieved with OMT and TEVAR for patients with type B IMH. The TEVAR performed in the acute setting carries a substantial risk of complications, emphasizing the need to optimize the timing of TEVAR and adapt stent-graft design to the pathophysiology of IMH.
Introduction
Acute aortic syndrome (AAS) includes aortic dissection (AD), intramural hematoma (IMH), and penetrating aortic ulcer (PAU). These 3 entities share similar clinical features and may progress from one to another or coexist.1,2 While AD remains the most frequently encountered form of AAS, IMH accounts for approximately 5% to 15% of patients presenting with AAS. 3
Intramural hematoma is characterized by bleeding within the medial layer of the aortic wall. Its physiopathology remains debated. While initially the etiology of IMH was reported to result from vasa vasorum disruption, more and more evidence supports the presence of focal intimal disruption (FID) leading to hematoma within the aortic wall. The hematoma within the media weakens the mechanical properties of the trilaminar structure and may contribute to the unpredictable natural course of IMH. Intramural hematoma behavior goes from total resolution to aortic aneurysm/penetrating ulcer, dissection, or even rupture. 4
The current standard of care for uncomplicated type B IMH is optimal medical therapy (OMT) through strict blood pressure and pain control with early serial imaging to monitor potential progression. Indications for intervention may include persistent chest pain, increasing hematoma thickness, FID/ulcer-like projections, rapid aortic expansion, new onset of dissection, or hemodynamic instability. 3
Thoracic endovascular aortic repair (TEVAR) has increasingly been employed as a therapeutic option for type B IMH patients. Data suggest that TEVAR improves aortic remodeling and reduces aortic-related death compared to medical therapy alone.3,5 Despite promising early results, mid- to long-term outcomes remain variably reported. Although TEVAR may reduce aortic-related complications, patients remain at risk of late TEVAR adverse events and aortic reinterventions. Thoracic endovascular aortic repair–related complications include retrograde AD, endoleaks, or proximal/distal stent-induced entry tear. The risk of these events reflects the fragility of the intima and media in the setting of IMH.
Hence, selecting patients for TEVAR vs continued optimal medical management remains a subject of ongoing investigation. To better characterize the natural history of type B IMH in patients without FID on initial presentation and TEVAR outcomes, we performed a retrospective review of our institutional experience.
Methods
Patient Selection
A retrospective review was conducted through our prospectively maintained database, from January 2001 to December 2024. A total of 40 patients with acute uncomplicated type B IMH were identified. Acute uncomplicated type B IMH was defined as an AAS with hematoma within the aortic wall, without an FID on initial CT. To ensure a homogeneous study population, patients with IMH and FID on initial presentation were excluded. Per institution protocol, OMT with strict blood pressure control with intravenous hypotensive drugs was achieved, as well as pain control. In all patients, CT was controlled within the first week or earlier in case of new onset or persistence of symptoms. Patients demonstrating a new FID on CT in the presence of ongoing chest pain or an increase in hematoma thickness (> 10 mm in hematoma thickness) were considered as ‘complicated IMH’ and planned for a semi-urgent TEVAR procedure (early TEVAR group). Thoracic endovascular aortic repair sizing was based on the proximal landing site diameter without oversizing. The length of the device was measured to include the FID. Overall stent length was 187.1 ± 47.7. Eighteen COOK (Bloomington, Indiana) and 12 Medtronic (Santa Rosa, California) grafts were implanted including 9 tapered grafts. Patients with good response to OMT were discharged and followed in a dedicated aortic clinic with a CT scan at 3 to 5 weeks, 3 months, 6 months, and yearly thereafter. The follow-up rate was 100%. Patients with late aortic complications were treated with TEVAR when anatomical prerequisites were favorable (late TEVAR group).
The primary outcome was overall survival across the 3 treatment groups (OMT, early TEVAR, and late TEVAR). Secondary outcomes included freedom from reintervention, TEVAR-related complications, and imaging resolution of IMH. Thoracic endovascular aortic repair–induced complications included new intimal tear/dissection or endoleak. Thoracic endovascular aortic repair–induced intimal tear was defined as the occurrence of a new intimal tear at the proximal or distal graft edges in the presence of residual hematoma. Type 1 endoleak was defined as the presence of blood flow (contrast) between the aortic wall and the graft at the proximal (1a) or distal (1b) edge.
Patient consent was waived, and the Institutional Review Board committee approved the study (#22476).
Statistical Analysis
Descriptive statistics were used to summarize baseline patient characteristics. Continuous variables are presented as a mean with standard deviation or median (IQR). Survival and freedom from reintervention in the early TEVAR and late TEVAR were estimated using the Kaplan-Meier curve, and comparisons between groups were performed using the log-rank test. Statistical significance was defined as P < .05.
Results
Baseline characteristics of the 40 patients are summarized in Table 1. The mean follow-up was 6.0 ± 5.1 years. Fourteen patients underwent early TEVAR intervention during their initial hospital course. Twenty-six patients were discharged from the hospital with OMT. Of these 26 patients, 16 patients required a late TEVAR intervention, while 10 patients continued with OMT alone. Patients treated with early TEVAR tended to be younger (63.6 ± 12.1 years) compared to late TEVAR (71.4 ± 7.5 years) and OMT patients (73.5 ± 10.1 years). Women represented 57.5% of the entire cohort with the highest proportion in OMT (70%). Hypertension was common among all groups, while other cardiovascular comorbidities such as CAD, MI, or diabetes were frequent. Mean aortic diameter at the proximal and distal necks was, respectively, 32.6 ± 4.6 mm and 32.1 ± 5.3 mm; mean maximal hematoma thickness was 9.8 ± 3.1 mm.
Patient Characteristics.
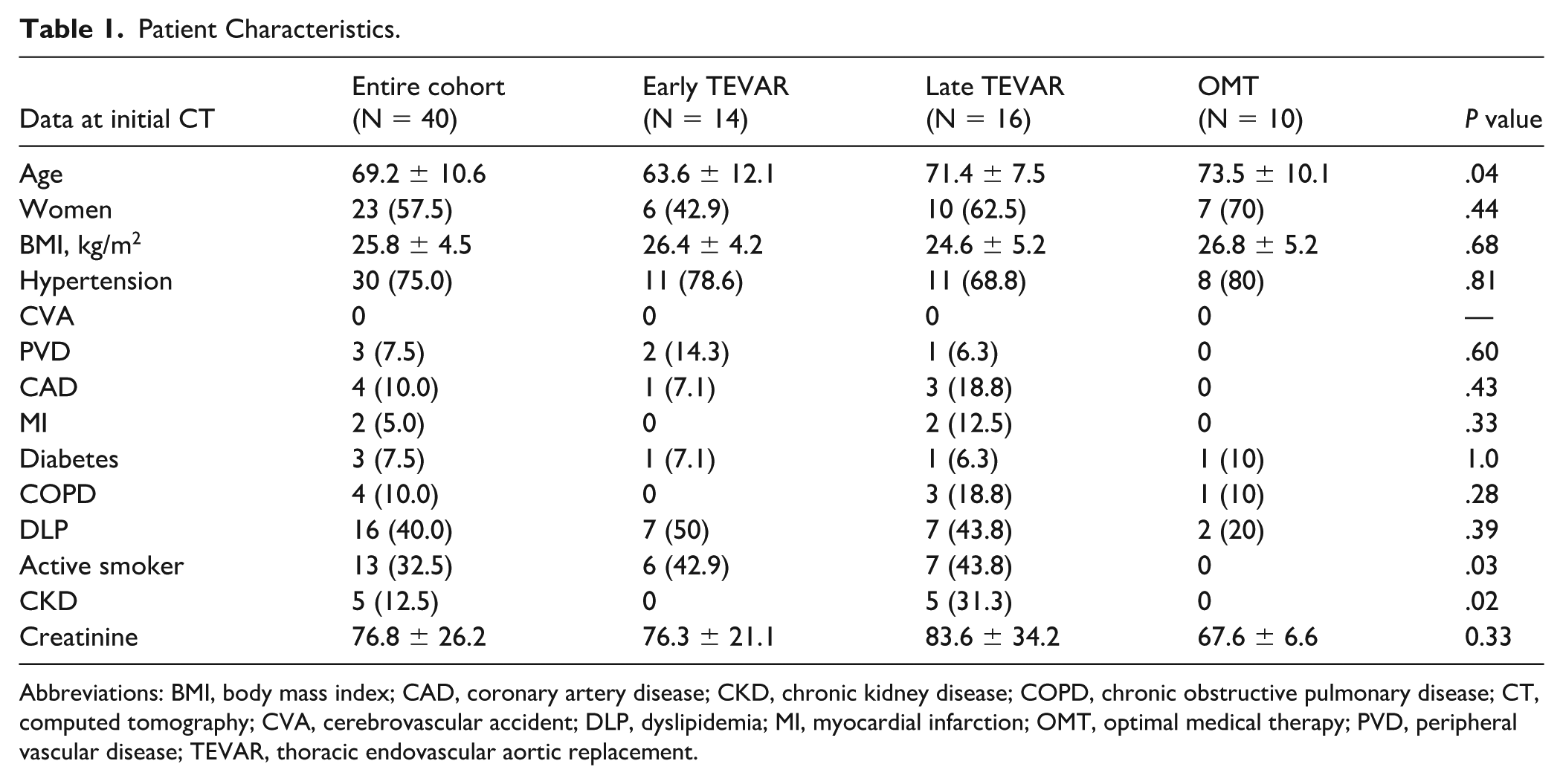
Abbreviations: BMI, body mass index; CAD, coronary artery disease; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CT, computed tomography; CVA, cerebrovascular accident; DLP, dyslipidemia; MI, myocardial infarction; OMT, optimal medical therapy; PVD, peripheral vascular disease; TEVAR, thoracic endovascular aortic replacement.
Early Thoracic Endovascular Aortic Repair Group
Early TEVAR was performed at a mean of 5.1 ± 3.8 days from diagnosis and all within 14 days from diagnosis. Maximal hematoma thickness at presentation was 11.4 ± 3.1 mm (IQR = 10-13 mm). Preoperative hematoma reached the distal arch in 3 patients (21%) and below the aortic hiatus in 13 patients (92%). The cause for early intervention was visualization of new FID within the IMH with an increase in hematoma thickness or persistent chest pain. There was no early dissection or rupture. The median proximal TEVAR graft size was 30 mm (IQR = 28-34). Proximal landing zone was evaluated to be IMH-free in 8 cases (61%), with proximal TEVAR landing site in zone 1 for 1 patient with carotid-carotid and carotid subclavian bypass, zone 3 for 9 patients, and zone 4 for 4 patients. Mean graft length was 188 mm ± 50 mm. The median distal graft size was 29 (range = 28-32) mm with a mean of 23.2% oversizing compared to the maximal aortic lumen diameter at the distal landing site, which incorporated aortic wall hematoma in all cases. The distal landing zone was zone 4 in 5 patients, zone 5 in 9 patients, and zone 6 in 1 patient. At the last follow-up, all patients had complete resolution of IMH.
Late Thoracic Endovascular Aortic Repair Group
Late TEVAR was performed in 16 patients at a mean of 41.3 ± 112.2 months, following the IMH diagnosis. Maximal hematoma thickness on initial CT was 9.4 ± 2.6 mm. No patients had hematoma reaching the arch, and 7 (43%) extended below the hiatus. The most common indication for intervention was pseudoaneurysmal evolution of the IMH (50%). Two patients were found with a type B dissection on late follow-up scan, 5 had new FID, and 1 had progression of the IMH. The median proximal graft size was 35 mm (IQR = 32-36); significantly larger than the early TEVAR group (P = .04). The TEVAR landed proximally in IMH-free aorta in 7 patients (43.8%). Proximal landing zone varied from zone 1 (1 patient), zone 2 (2 patients), zone 3 (7 patients), and zone 4 (6 patients). The median distal graft size was 34 (range = 32-38), with a mean of 20.2% oversizing compared to the maximal aortic lumen diameter and 94% landed in zone 5. At the last follow-up, all patients had positive aortic remodeling and complete resolution of IMH.
Optimal Medical Therapy Group
Ten patients were treated medically and followed for 6.3 ± 4.0 years. The maximal diameter of the IMH was 8.1 ± 0.8 mm at presentation and was significantly lower than groups 1 and 2 (P = .01). Hematoma involved the distal arch in 1 patient, and 4 patients had hematoma extending below the hiatus. All patients showed complete regression of the IMH at 6.2 ± 7.7 months, following the initial diagnosis with no late complication.
Reintervention and Thoracic Endovascular Aortic Repair Complications
A total of 30 patients required TEVAR, early or late, during the study period (Figure 1). Patients undergoing TEVAR in the early phase demonstrated a significantly higher rate of reintervention compared with those treated in the chronic phase following a period of OMT (P = .003). Within the early TEVAR group, 11 patients had TEVAR-associated complications at a mean of 1.9 ± 4.6 years post-TEVAR implantation. One patient sustained an intraoperative retrograde type A extension during manipulation of the guidewires; emergent ascending/arch repair was performed. One patient with type IA endoleak was treated conservatively owing to significant comorbidities. Four patients presented a type IB endoleak, of whom 3 were treated with TEVAR extension and 1 with ongoing medical surveillance. All endoleaks were linked to the TEVAR landing in segments with IMH. Regarding other aortic-related complications, 3 patients showed the presence of new ulceration/pseudoaneurysm in the distal non-stented aorta, requiring TEVAR extension in 2 cases and an open aortobiliac graft in 1 patient. Another patient presented a dissection distal to the TEVAR 4 months following the TEVAR implant. Rapid expansion required an open type IV thoracoabdominal replacement 9 months later.
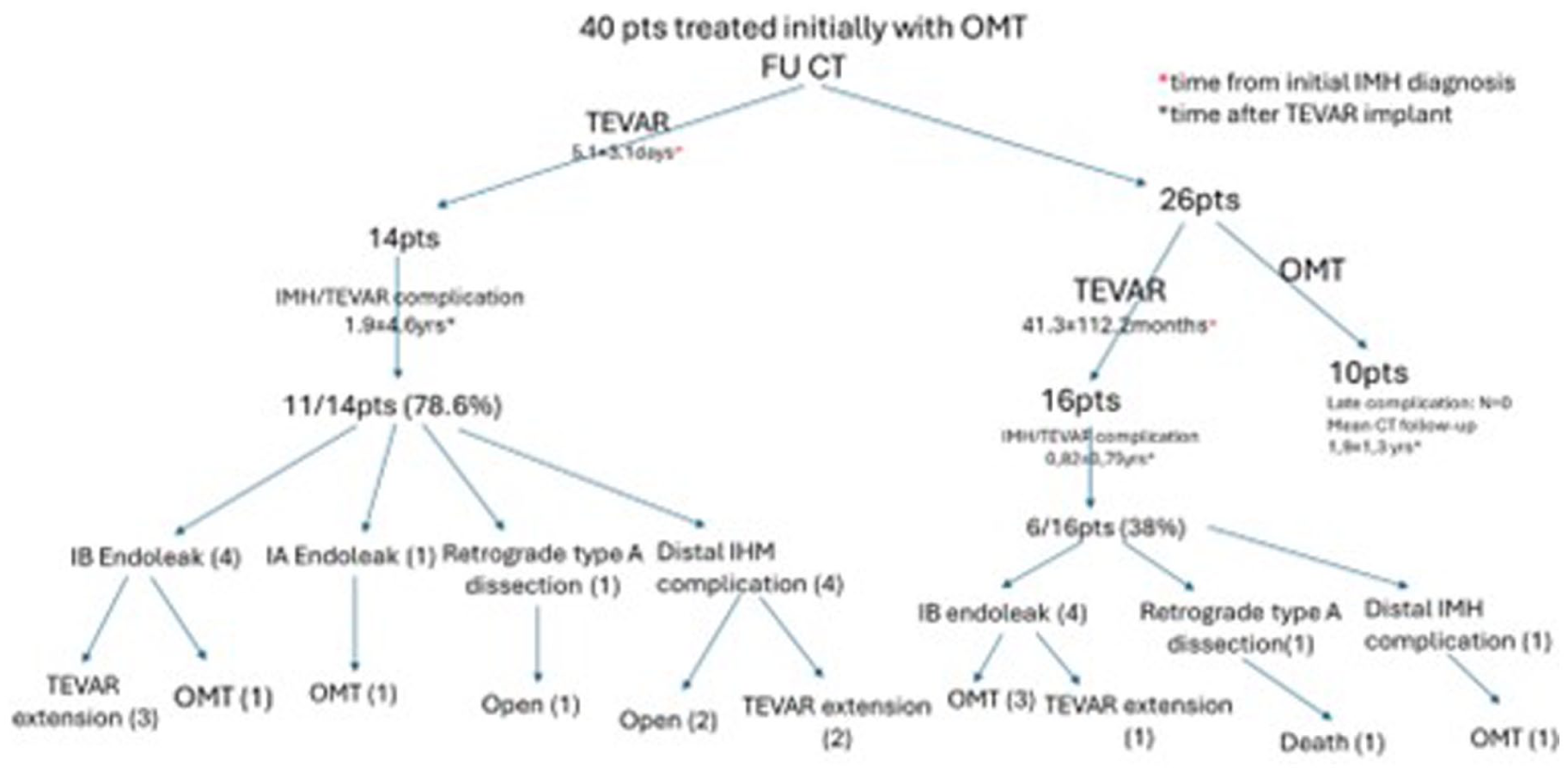
Flow diagram representing patient evolution after initial type B IMH diagnosis. IMH, intramura hematoma.
In the late TEVAR group, 6 patients (38%) developed complications at a median time of 14 months (IQR = 9-47). Four patients developed a type IB endoleak with 1 patient treated by TEVAR extension and OMT among the 3 other patients. One patient presented a new ulcer at the thoracoabdominal junction, followed by imaging surveillance. An 83-year-old patient treated at 1 month post IMH with a Captivia TEVAR device (Medtronic Inc) experienced a retrograde type A dissection 2 months thereafter to which he succumbed and died of this condition.
Survival
Early survival following type B IMH was 100%, meaning the entire cohort left the hospital following initial hospitalization regardless of their treatment group.
Patients treated with early TEVAR had a survival of 100% at 5 years. Patients treated within the late TEVAR group had 1-, 3-, and 5-year survival of 93.8%, 77.9%, and 64.9%, respectively, while patients treated with OMT alone had 1-, 3-, and 5-year survival of 100%, 88.9%, and 88.9%, respectively. Deaths were related to respiratory failure (n = 3), cardiac (n = 2), cancer (n = 1), and retrograde type A owing to TEVAR in the TEVAR cohort and 1 death of unknown etiology in the medical treated group.
There was no survival difference between early and late TEVAR groups (Figure 2). Furthermore, no significant difference in survival was observed between IMH patients treated with TEVAR or OMT (Figure 3).
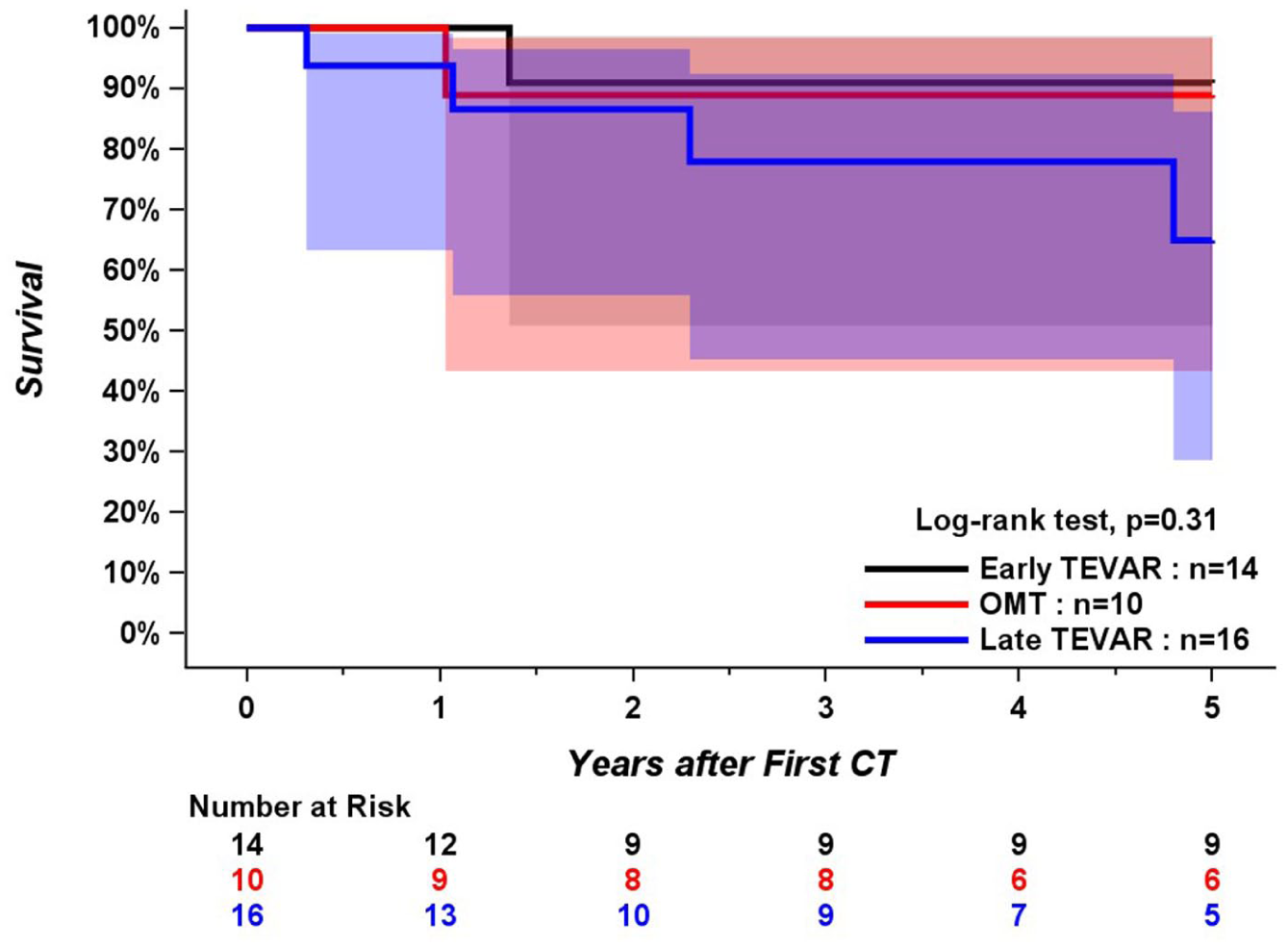
Survival among different treatment groups: early TEVAR, late TEVAR, and medical therapy alone (OMT). CT, computed tomography; OMT, optimal medical therapy; TEVAR, thoracic endovascular aortic replacement.
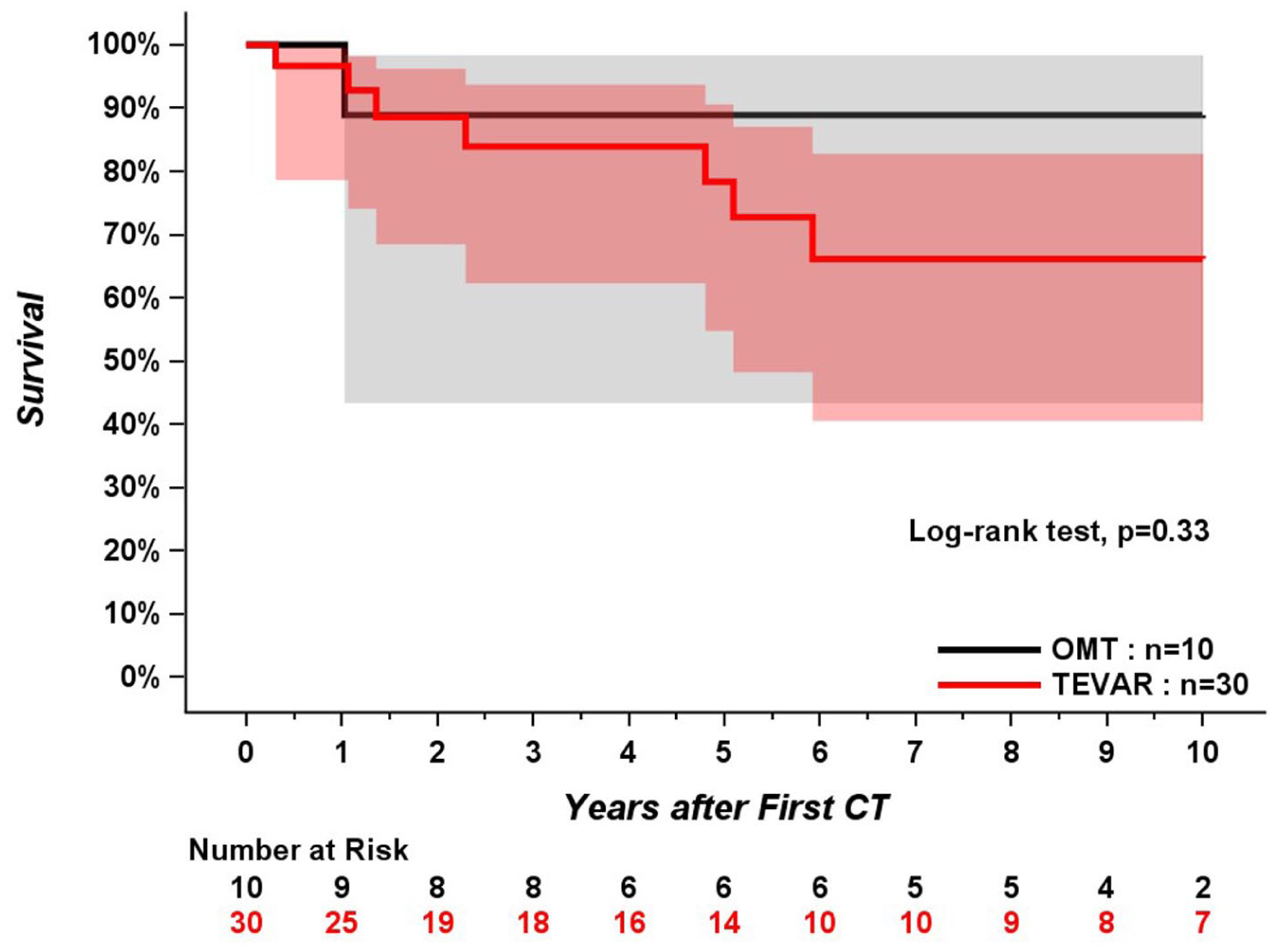
Survival analysis comparing patients treated with TEVAR and patients treated with medical therapy alone (OMT). CT, computed tomography; OMT, optimal medical therapy; TEVAR, thoracic endovascular aortic replacement.
Discussion
This study analyzed a specific cohort of patients presenting with type B IMH without an identifiable intimal tear on initial CT, all managed according to a single-institution protocol. The results underscore 3 key findings: (1) the unpredictable natural history of type B IMH, requiring strict clinical and imaging follow-up; (2) the high rate of TEVAR-related complications and reinterventions, particularly when the procedure is performed early after diagnosis; and (3) the excellent aortic remodeling and midterm survival observed among both TEVAR and medically treated patients.
Intramural hematoma represents approximately 5% to 15% of all AAS. 6 Whereas most cases of type A IMH require urgent surgical intervention due to their unfavorable natural history, type B IMH is usually considered a more benign entity. In the absence of rupture or impending rupture, OMT, including strict blood pressure and pain control, combined with serial imaging, remains the cornerstone of management. Nevertheless, a subset of patients will progress to dissection or rupture within the first month after presentation. 7 While aortic diameter >45 mm and hematoma thickness >10 mm are recognized risk factors for type A IMH complications,8,9 specific predictors for type B IMH outcomes remain less clearly defined. Within the present study, patient demographics were comparable among different treatment groups, although patients responding positively to OMT had significantly less maximal thickness of IMH.
The presence of an FID has been identified as a potential prognostic marker in patients with type B IMH. Ishizu et al 10 reported in a cohort of 76 patients that those with large FIDs (length > 10 mm and depth > 5 mm) experienced significantly more aortic-related events than patients with smaller or absent FIDs. In their study, 66% of patients had an FID on initial CT; among the remaining 26 patients, 9 (34.6%) developed an FID during follow-up. Similarly, in our cohort of 40 patients without FID on initial CT, 14 (35%) developed a new FID on in-hospital control CT. In addition, 5 patients developed new FID or IMH-related complications distal to the stent-graft after discharge, emphasizing the need for complete thoracoabdominal aortic imaging at follow-up.
The timing and indications for endovascular intervention in type B IMH remain controversial. Management decisions must balance the risk of adverse aortic events related to the type B IMH against the procedural risks of TEVAR. In our institutional algorithm, the appearance of a new FID on follow-up CT—particularly when associated with increasing hematoma thickness or persistent pain—was considered a high-risk feature and considered as a complicated IMH warranting early intervention. Similar findings have been reported by Li et al, 11 who identified new ulcer-like projections, increasing hematoma thickness, and large baseline aortic diameter as predictors of adverse outcomes. Other authors have supported FID presence as a key risk factor,12,13 while Moral et al 14 emphasized that FID <3 mm may not confer significant risk.
From a technical perspective, the presence of a hematoma at the intended proximal landing zone may predispose to retrograde type A AD, and excessive distal oversizing due to lumen compression may lead to distal graft-induced intimal injury. Our results corroborate these concerns: among early TEVAR cases, 6 of 14 (42.9%) experienced device-related complications, predominantly at the distal landing zone, among whom 5 required additional procedures. Among the late TEVAR patients, 5 of 16 (31.3%) developed late complications, including 1 retrograde type A dissection and 4 type IB endoleaks, among whom 1 required graft extension. Patients who underwent TEVAR earlier after IMH diagnosis were significantly more likely to experience device-related complications, supporting prior findings by Wang et al. 15 Multiple factors may contribute to the high rate of device-related complication, especially in the acute setting. Landing proximally or distally in an aortic segment with fresh hematoma increases the risk of intimal tear. Landing proximally in normal non-diseased aorta secures a stable platform for proximal sealing and should be planned whenever possible. However, in most IMH cases, aortic lumen at the distal landing zone is significantly narrowed by the hematoma and leads to excessive oversizing with current graft technology available off the shelf. Such oversizing in a fragile aorta without a doubt contributes to the high rate of distal device-related complication in an acute setting. Optimizing stent-graft design may improve procedural safety. In our series, both cases of retrograde type A dissections occurred with devices featuring proximal bare stents, suggesting potential trauma to the fragile intima. Use of 8-mm tapered grafts may mitigate distal oversizing, while low-radial-force distal stent designs could reduce wall stress. Ideally, stent-grafts should be tailored to disease morphology; in selected chronic cases, custom-manufactured devices with tapered configurations and a distal unstented soft polyester segment may possibly improve outcomes.
At midterm follow-up, complete resolution of IMH was observed in both the TEVAR and OMT groups, with comparable survival outcomes. Meta-analyses by Chakos et al 3 and Sá et al 16 have reported similar findings, demonstrating excellent outcomes under combined TEVAR + OMT algorithms. However, most comparative studies fail to account for variations in clinical presentation and risk profile. A systematic review by Li et al 5 focusing on high-risk type B IMH found improved aortic remodeling and reduced aortic-related mortality with TEVAR.
Study Limitations
Due to the rarity of type B IMH, most available studies are observational and heterogeneous. This study specifically analyzed a homogeneous population of 40 patients without initial FID, emphasizing the variable course of this condition. While the emergence of a new FID is recognized as a major risk factor, our analysis did not stratify based on ulcer size; smaller ulcers may have been safely managed medically, avoiding early stent-induced complications. Furthermore, our results may have been biased by our institutional algorithm and limited sample size. Better characterization of IMH disease is required to optimize the timing of intervention to prevent aortic complications and also to avoid unnecessary TEVAR implants with secondary complications. Future work integrating machine learning–based predictive modeling 17 and PET-FDG metabolic imaging 18 (IMH15) is currently being investigated and may enhance individualized risk stratification. Despite the inclusion of various stent-graft models, our findings reinforce that early TEVAR is associated with higher procedural risk. Further refinement of device design and timing criteria may improve safety and durability.
Conclusion
In patients with type B IMH without FID at presentation, the unpredictable natural course mandates close clinical and imaging surveillance during the initial medical management phase. Thoracic endovascular aortic repair performed in the acute setting carries a substantial risk of complications, emphasizing the need to better stratify the IMH risk of aortic-related complication, optimize timing of TEVAR, and adapt stent-graft design to the pathophysiology of IMH. Using our institutional treatment algorithm, favorable midterm outcomes can be achieved with either OMT or selective TEVAR intervention.
Footnotes
Acknowledgements
The author acknowledges Mrs Stéphanie Dionne.
Ethical Considerations
This study was approved by the Research Ethics Board of the Quebec Heart and Lung Institute (approval number: 2025-4207).
Informed Consent
The study was conducted in accordance with institutional and national research ethics guidelines and the Declaration of Helsinki.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: FD is a consultant and proctor for COOK Medical and has received honorarium from Abbott Medical and Edwards Lifesciences.
Data Availability Statement
All data were collected, reviewed, and analyzed in accordance with strict confidentiality standards. De-identified data may be made available upon reasonable request and with approval from the institutional ethics committee.