
Abstract
Background:
Endovascular aortic repair (EVAR) has been the standard treatment for abdominal aortic aneurysms (AAAs) for about 20 years, offering advantages in morbidity and mortality in the short- and mid-term. However, long-term complications, such as endoleaks (ELs) and aneurysm sac rupture, can arise due to mechanical issues with the EVAR technique, including material fatigue.
Patients and Methods:
We report the cases of 3 patients with partial or total separation of the bare metal suprarenal stent-struts separation in the bifurcated Medtronic Endurant II EVAR stent-graft, treated with various methods. Here, the BMS-SSS occurred 2.5, 6.8, and 6.7 years, respectively, after the initial EVAR procedure. All 3 patients were treated using different (conservative, endovascular, and open surgical) therapy methods.
Discussion:
Since the introduction of the EVAR technique, advancements in prosthesis design have significantly reduced complications resulting from different types of ELs. Bare metal suprarenal stent-strut separation (BMS-SSS) remains as a rare issue, being associated with EL type I, graft migration and late aneurysm sac growth and rupture. Treatment options include conservative management for stable cases, endovascular interventions like stent realignment or cuff implantation, and, as a last resort, open surgery with late open conversion. Strict surveillance after EVAR is essential to detect BMS-SSS in time and to prevent serious, potentially-life-threatening complications.
Clinical Impact
This study highlights the critical necessity of lifelong, strict surveillance after EVAR to detect rare but life-threatening mechanical failures like bare metal suprarenal stent-strut separation (BMS-SSS). It provides a comparative clinical insight into managing this specific complication using conservative, endovascular, and open surgery approaches. For clinicians, these findings mean that treatment must be highly individualized based on anatomical conditions, graft condition and patient stability, rather than relying on a standardized protocol. Ultimately, this shifts clinical practice toward heightened vigilance regarding long-term material fatigue and expands the decision-making framework for late EVAR complications.
Keywords
Introduction
For about 20 years, endovascular aortic repair (EVAR) has become the standard treatment for simple and complex abdominal aortic aneurysms (AAAs). While short- and mid-term results for EVAR show significant advantages in morbidity and mortality rates over open repair, these advantages recede after longer observation periods.1-5 The main reason for this late rise in mortality and morbidity after EVAR are complications resulting from the EVAR technique and containing mechanical issues. 6 These may lead to, e.g., endoleaks (ELs), resulting in (late) aneurysm sac enlargement ((L)ASE), which implies the risk for, sometimes lethal, late aneurysm sac rupture.7-10 One rare condition is material fatigue, described as EL III, where a loosening of the connection between the modular components of the EVAR stent-grafts (EL IIIa) or material breaches or holes (EL IIIb) appear.6,11 According to the literature, the incidence of EL III varies between approximately 2% and 5%, with a higher frequency observed in older-generation endografts compared with newer-generation endografts, also with varying manifestations across different models.12-16 Moreover, a strongly-angulated and calcified aneurysm neck could be shown to be risk factors for EL III.12-14 Distinctively, the (partial) separation of the bare metal stent-struts, designed for the suprarenal fixation of the main body of the EVAR stent-graft, has been described as a rare occurrence of material-fatigue.6,17-20 The consequences of this material-fatigue can range from asymptomatic incidental findings during follow-up examinations after EVAR to clinically highly symptomatic and potentially life-threatening secondary complications. For example, a partial bare metal suprarenal stent-strut separation (BMS-SSS) may only lead to slight migration of the stent-graft prosthesis without relevant secondary complications such as an EL Ia or (L)ASE. On the contrary, a total BMS-SSS is often more likely to result in significant migration of the stent-graft which can subsequently lead to EL Ia, (L)ASE and life-threatening rupture of the not actually excluded AAA.17,19,21,22 A recent review by Krogt et al 6 describes 12 BMS-SSS in different devices. A search of the Manufacturer and User Facility Device Experience (MAUDE) database (provided by the US Food and Drug Administration) 23 using the keywords “endurant’” and “bifurcated” as well as “zenith” from January 2010 to December 2025 yielded 496 and 500 results, respectively. The detailed information in the results was searched for the keywords “bare metal” (endurant 9 results, zenith 42), “demolition” (endurant 0, zenith 0), “detachment” (endurant 21, zenith 2), “separation” (endurant 30, zenith 103), “strut” (endurant 2, zenith 7), “suprarenal” (endurant 47, zenith 39), and “tear” (endurant 26, zenith 84), resulting in the identification of 11 cases of BMS-SSS in Medtronic Endurant and 5 in Cook Zenith stent-grafts, respectively.
We here report 3 consecutive patients with partial and total BMS-SSS and consecutive demolition of the suprarenal fixation of the bifurcated Medtronic Endurant II EVAR stent-graft, which were treated using different, i.e., conservative, endovascular, and open surgical methods.
Patients and Methods
A retrospective review of a prospectively-maintained EVAR database was performed to identify BMS-SSS cases. All consecutive patients with detection of BMS-SSS, regardless of which EVAR prosthesis was used to treat the AAA, were included. A total of 3 consecutive patients has been diagnosed with BMS-SSS (all Medtronic Endurant II), while 991 EVAR prostheses were implanted in a 10-year period (January 2010–December 2019), corresponding to a share of 0.3%. Of the implanted grafts, 876 (88.4%) were from Medtronic, 56 (5.7%) from Cook, 32 (3.2%) from Gore, 18 (1.8%) from Terumo/Vascutek, and 9 (0.9%) from other brands. Regarding the period in which the affected EVAR prostheses were implanted, the incidence of BMS-SSS corresponds to a share of 0.7% (447 EVAR procedures in 2016–2019).
The postoperative follow-up protocol after EVAR included examinations immediately postoperatively, as well as at 3, 6, and 12 months, followed by annual examinations. The follow-up examinations involved contrast-enhanced ultrasound (CEUS) as well as a native X-ray of the abdomen in 2 planes to initially evaluate the condition and configuration of the EVAR stent-graft prosthesis. In the case of an ambiguous or pathological finding, a computed tomography angiography (CTA) of the aorta was performed to evaluate the condition of the EVAR prosthesis and to identify underlying pathologies. Here, a BMS-SSS was defined as a partial or total disconnection between the uncovered suprarenal bare metal stent-struts and the covered part of the EVAR stent-graft prosthesis, visible in the X-ray and/or CTA images.
The institutional review board’s approval was not required for this study, as no experiments involving humans or animals were conducted. Written informed consent for publication of their clinical details and any accompanying images was obtained from patients included in the manuscript.
Results
Details regarding the patients’ and EVAR stent-graft characteristics, the initial treatment, and the actual presentation are provided in Table 1.
Characteristics of the Patients, Anatomy, and Implanted EVAR Stent-Grafts at the Time of Initial Implantation and at the Time of Current Presentation With the BMS-SSS.
Abbreviations: AAA, abdominal aortic aneurysm; AHT, arterial hypertension; BMS-SSS, bare metal suprarenal stent-strut separation; CAD, coronary artery disease; chEVAR, chimney endovascular aortic repair; COPD, chronic obstructive pulmonary disease; EVAR, endovascular aortic repair; IBE, iliac branch endoprosthesis.
After initial shrinkage to 45 mm.
Patient 1
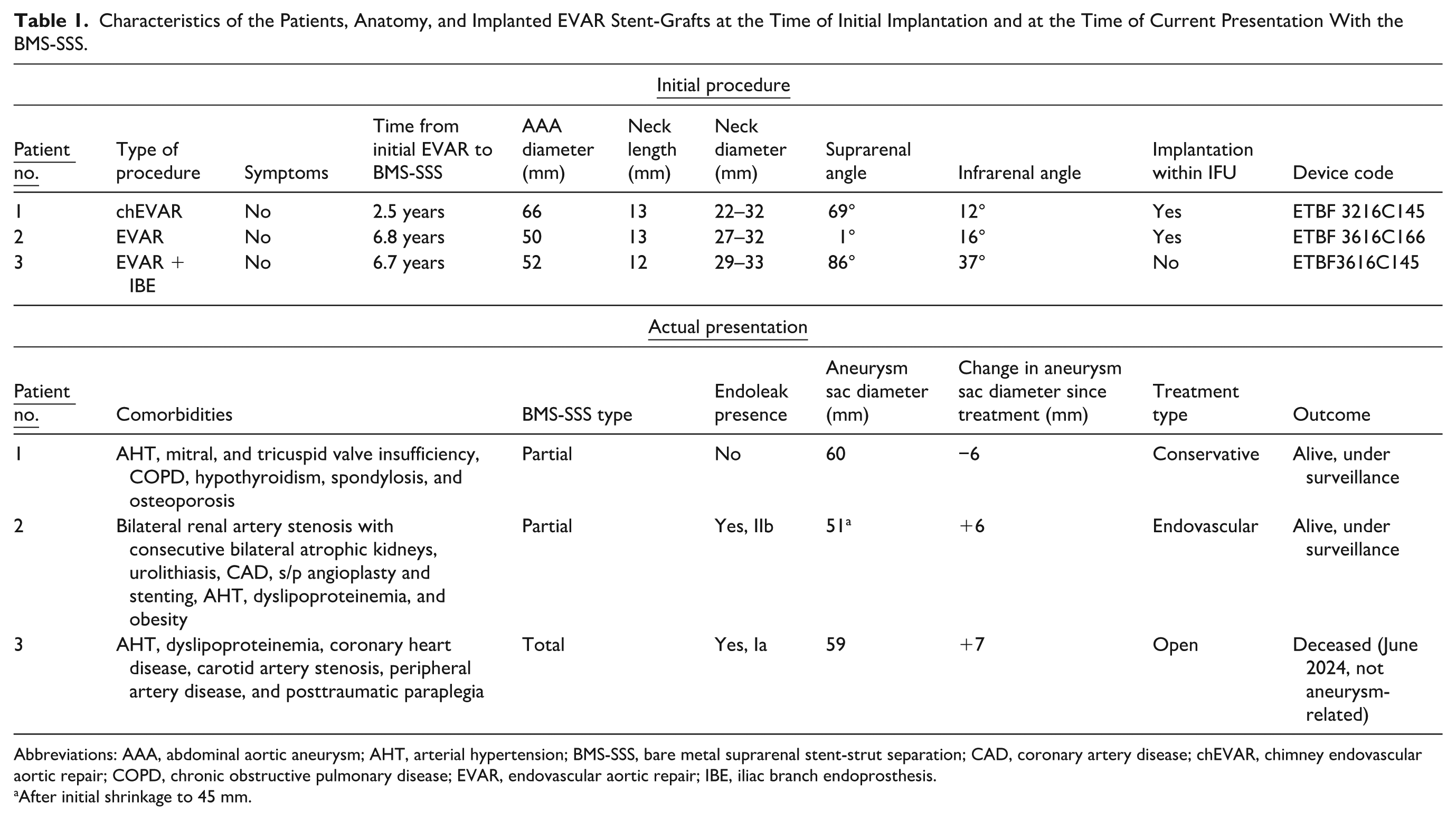
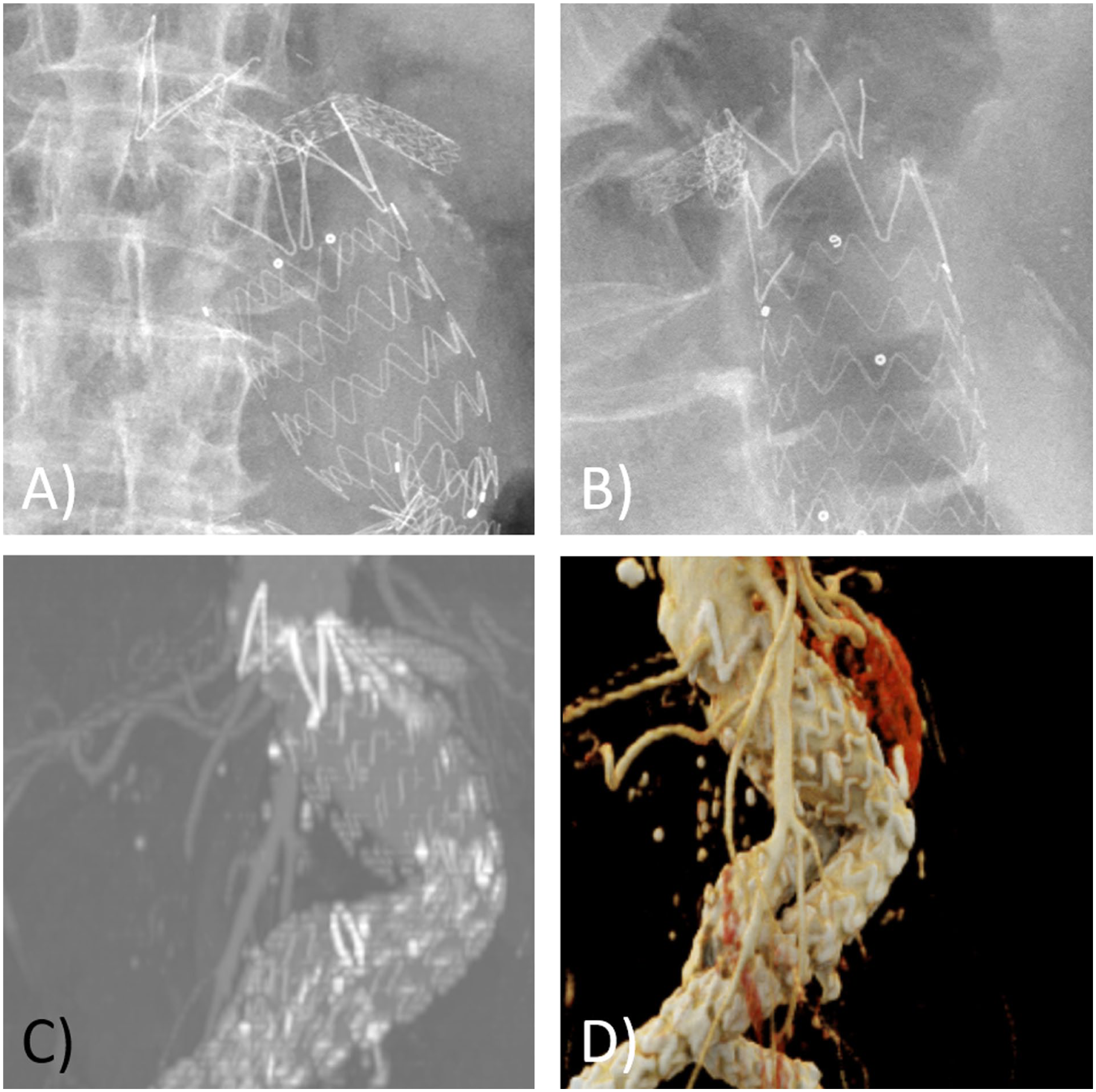
An 82-year-old female patient presented in an elective setting in November 2021 as a part of the regular follow-up after chimney EVAR (chEVAR), performed in May 2019, with a partial BMS-SSS without evidence for an EL, diagnosed by CEUS and subsequent X-ray and CTA (Figure 1). The primary chEVAR was performed for an asymptomatic AAA using an aorto-bi-iliac Medtronic Endurant II main body stent-graft (Medtronic, Inc., Minneapolis, Minnesota) with bilateral limb extensions and chimney stent-graft for the left renal artery (Advanta V12, 6 × 59 mm) (Getinge, Goteborg, Sweden). Regarding the AAA characteristics (Table 1), the procedure was performed in accordance with the instructions for use (IFU). In the semi-annual follow-up visits, the aneurysm sac shrank and since the diameter of the aneurysmal sac was constant and the patient remained asymptomatic, a conservative treatment was performed due to the chEVAR configuration and the poor general condition of the patient. The latest follow-up CTA in November 2024 showed no evidence for an EL while showing a slightly progressing distal dislocation of the chEVAR stent-graft (Figure 2).
Conventional abdominal X-ray in anteroposterior view (A) and lateral view (B) and computed tomography (CT) angiography in anterolateral view multilayer CT reconstruction (C) and anterolateral view 3D CT reconstruction (D) of an 82-year-old female patient, showing a partial dorsolateral detachment of the suprarenal stent-strut fixation of the implanted chEVAR prosthesis (Medtronic, Endurant II) without late aneurysm sac enlargement, 2.5 years after the initial chEVAR procedure.
Computed tomography angiography (CTA, transversal view) of an 82-year-old female patient with a partial dorsolateral detachment of the suprarenal stent-strut fixation of the implanted chEVAR prosthesis. (A) Transversal plane of the initial CTA revealing the partial dorso-lateral detachment of the suprarenal stent-strut fixation of the implanted EVAR prosthesis (shown in Figure 1), here showing the aneurysm sac without evidence for an endoleak and with no aneurysm sac growth since the last follow-up visit. (B) Transversal plane of the follow-up CTA 3 years after the initial CTA (A), still showing the aneurysm sac without evidence for an endoleak and with no aneurysm sac growth since the last follow-up visit (A). Note the caudal dislocation of the chEVAR prosthesis in (B) compared with (A).
Patient 2
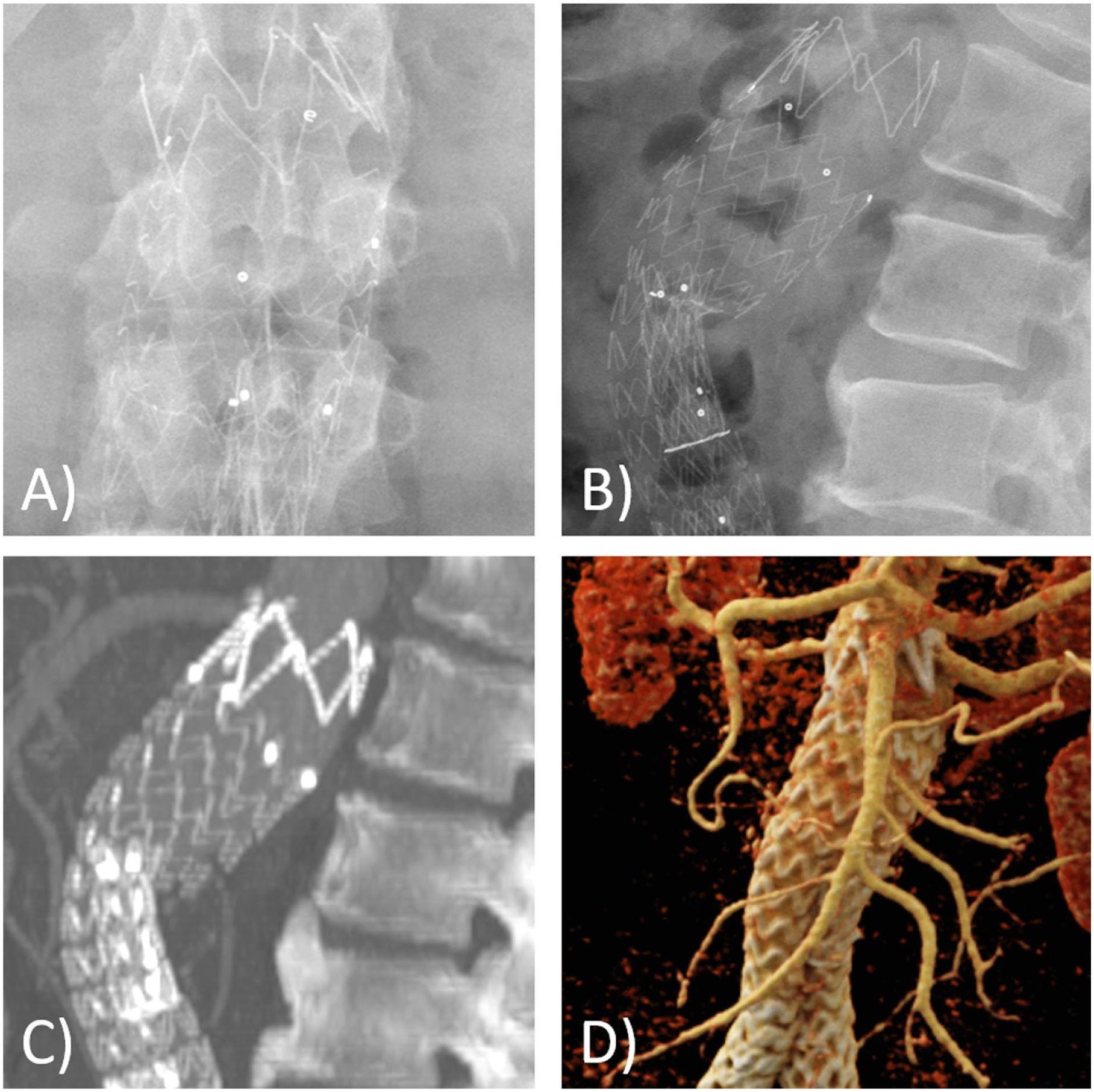
A 60-year-old male patient presented in an elective setting in December 2022 and was diagnosed with a partial BMS-SSS after EVAR (performed in February 2016) by means of conventional abdominal X-ray and subsequent CTA (Figure 3). The primary elective EVAR was performed using an aorto-bi-iliac Medtronic Endurant II main body stent-graft (Medtronic, Inc., Minneapolis, Minnesota) with right iliac and left limb extensions, the procedure was performed in accordance with the IFU (Table 1). In the early postoperative follow-up visits, despite a small EL II, the aneurysm sac showed a shrinkage to 45 mm, followed by a rapid LASE up to 51 mm at the actual presentation. The patient was treated by a proximal aortic cuff extension (ETCF 3636C49EE) (Medtronic, Inc., Minneapolis, Minnesota), which was additionally fixated with the Heli-FX EndoAnchor System (Medtronic, Inc., Minneapolis, Minnesota) in February 2023 (Figure 4). Postoperatively, the patient developed an acute renal failure due to the renal artery stenosis in addition to the use of contrast agent and required dialysis, from which he recovered 6 weeks postoperatively. In the latest follow-up visit with CEUS and conventional abdominal X-ray in November 2024, the aneurysm measured 49 mm (stable) with no evidence for an EL, stent-graft dislocation, or fracture (Figure 4).
Conventional abdominal X-ray in anteroposterior view (A) and lateral view (B) and computed tomography (CT) angiography in lateral view multilayer CT reconstruction (C) and anterolateral view 3D CT reconstruction (D) of a 60-year-old male patient, showing a partial dorsal detachment of the suprarenal stent-strut fixation of the implanted EVAR prosthesis (Medtronic, Endurant II), 6.8 years after the initial standard EVAR procedure.
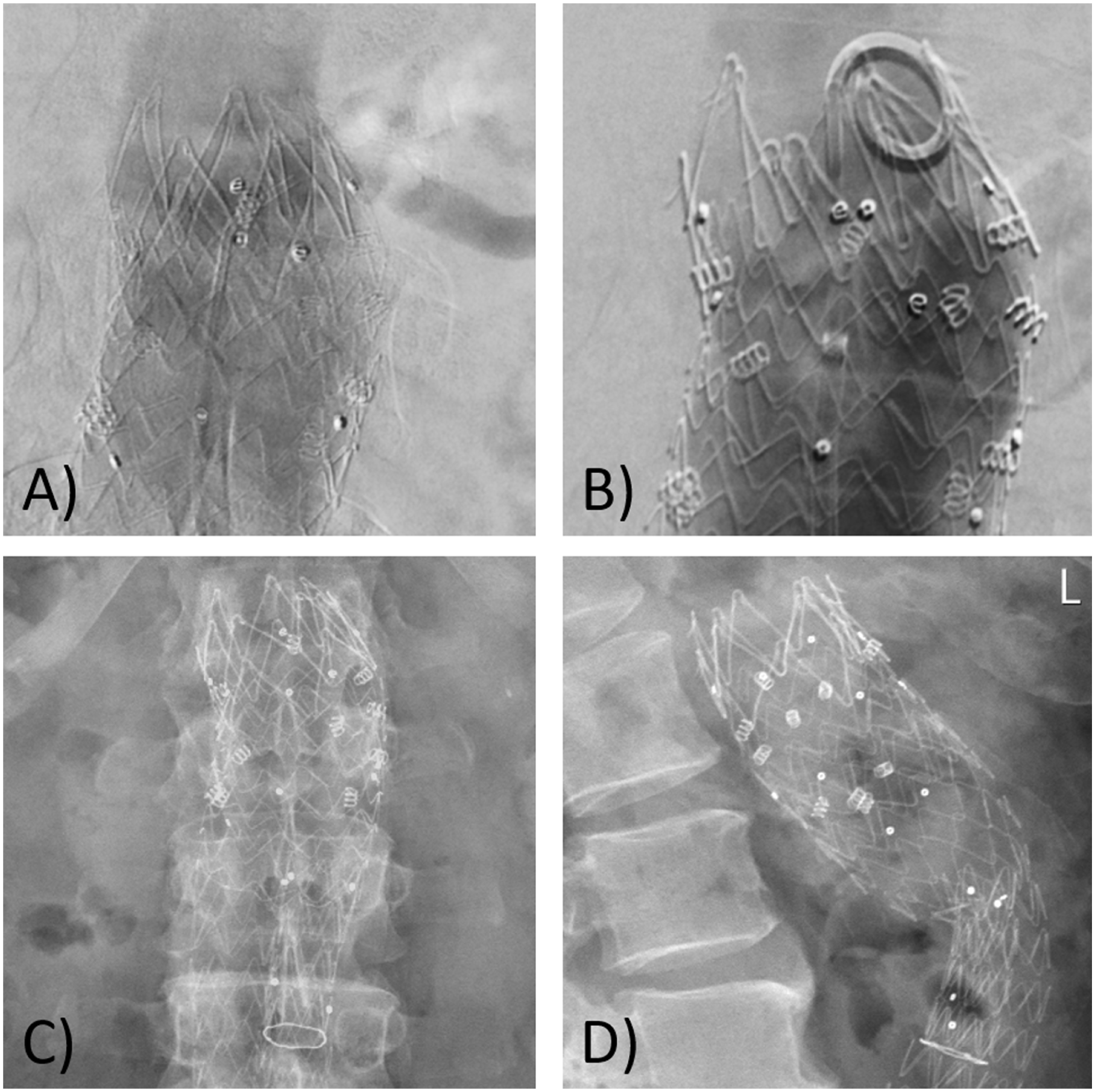
Intraoperative angiography (A, B) during the proximal aortic cuff extension and fixation using endo anchors and postoperative conventional abdominal X-ray images in anteroposterior (C) and lateral view (D) for a 60-year-old male patient with a partial detachment of the suprarenal stent-strut fixation of the implanted EVAR prosthesis (Medtronic, Endurant II).
Patient 3
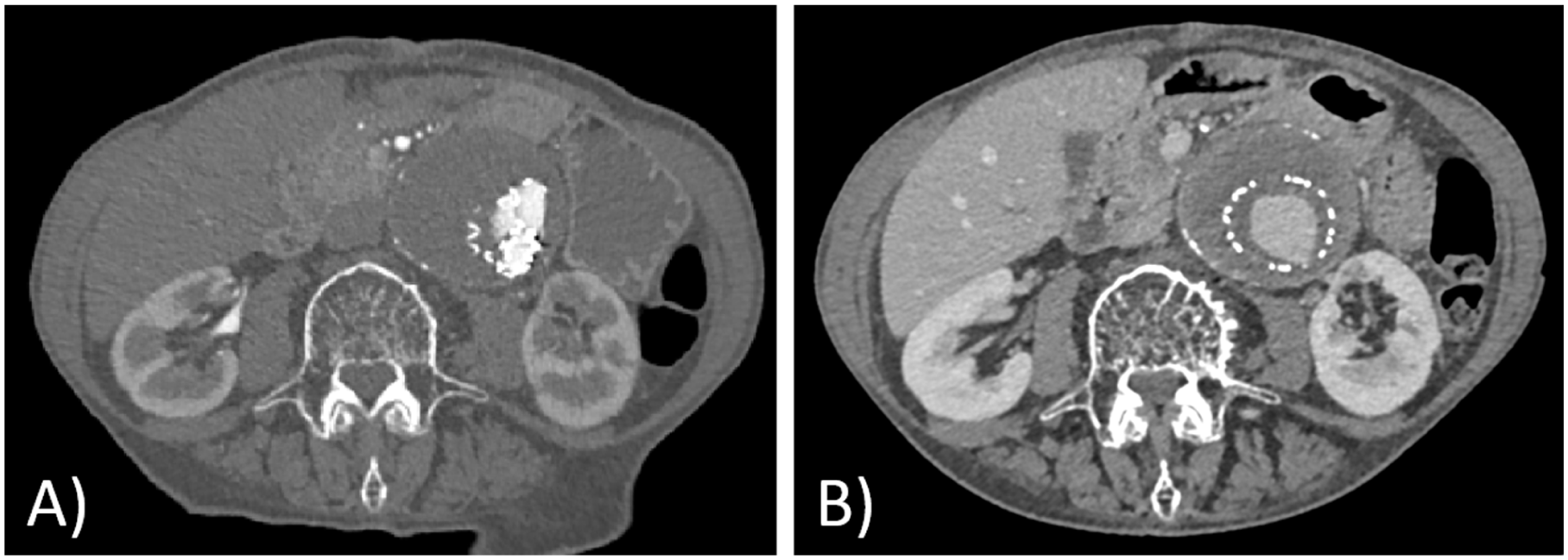
A 69-year-old male patient presented in February 2024 electively as a part of the regular follow-up after EVAR, performed in June 2017, and was diagnosed with an asymptomatic EL Ia and LASE by CEUS and, subsequently, complete BMS-SSS was detected using X-ray and CTA (Figure 5). The primary elective EVAR was performed using an aorto-bi-iliac Medtronic Endurant II main body stent-graft (ETBF3616C145) (Medtronic, Inc., Minneapolis, Minnesota) with bilateral iliac extensions and a Gore Excluder iliac side branch endoprosthesis (W.L. Gore & Associates, Inc., Flagstaff, Arizona) on the left side. As the renal artery was doubled on both sides, fenestrated EVAR was not an option. Due to the distinct angulation (Table 1), the procedure was performed outside the IFU. In the subsequent follow-up examinations, the aneurysm sac showed a constant size until the actual presentation with a rapid LASE, while the left iliac aneurysm had shrunk from 30 to 25 mm. Due to the risk of rupture, the indication for late open full conversion was made (Figure 6). The EVAR prosthesis has been entirely explanted and an aorto-bi-iliac Y-prosthesis (Gel-Soft- Plus, 20 × 10 mm) (Terumo Corporation, Sunrise, Florida) was implanted. On the first postoperative day, the patient developed a stroke due to a thrombotic occlusion of the left vertebral artery, most likely due to a hypotensive episode during the reperfusion phase, and was transferred to a neuroradiological department for interventional treatment, where thrombectomy and stenting were performed successfully. Hereafter, the patient was readmitted to our vascular surgery clinic for further treatment, where he had to undergo a series of angioplasties due to symptomatic coronary heart disease. Finally, the patient was discharged to a geriatric rehabilitation hospital. He deceased in June 2024 due to a cause unrelated to the AAA.
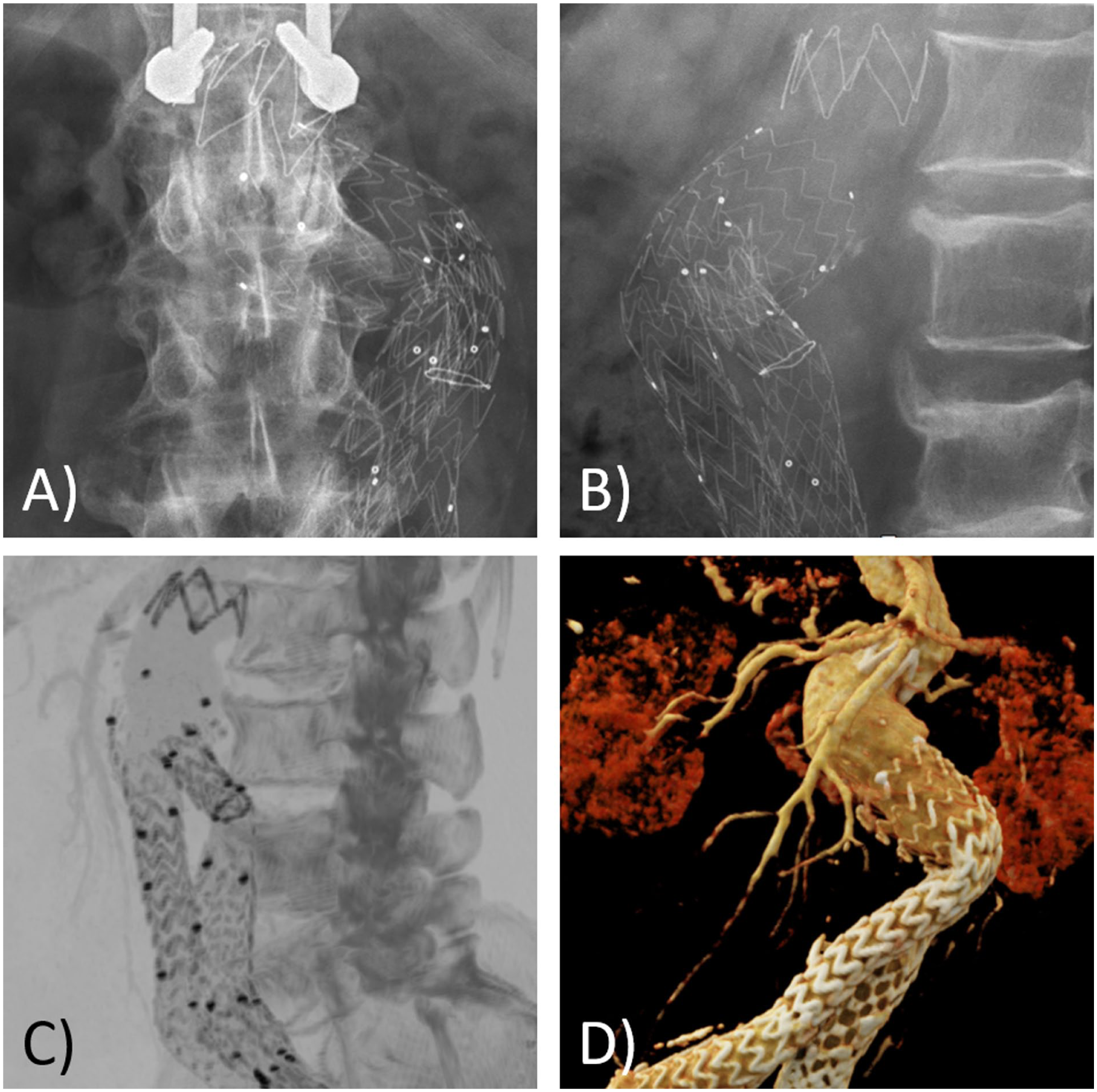
Conventional abdominal X-ray in anteroposterior view (A) and lateral view (B) and computed tomography (CT) angiography in lateral view multilayer CT reconstruction (C) and anterolateral view 3D CT reconstruction (D) of a 69-year-old male patient, showing a complete detachment of the suprarenal stent-strut fixation of the implanted EVAR prosthesis, 6.7 years after the initial standard EVAR procedure. Note the complete separation of the uncovered stent-struts from the covered part of the EVAR stent-graft.
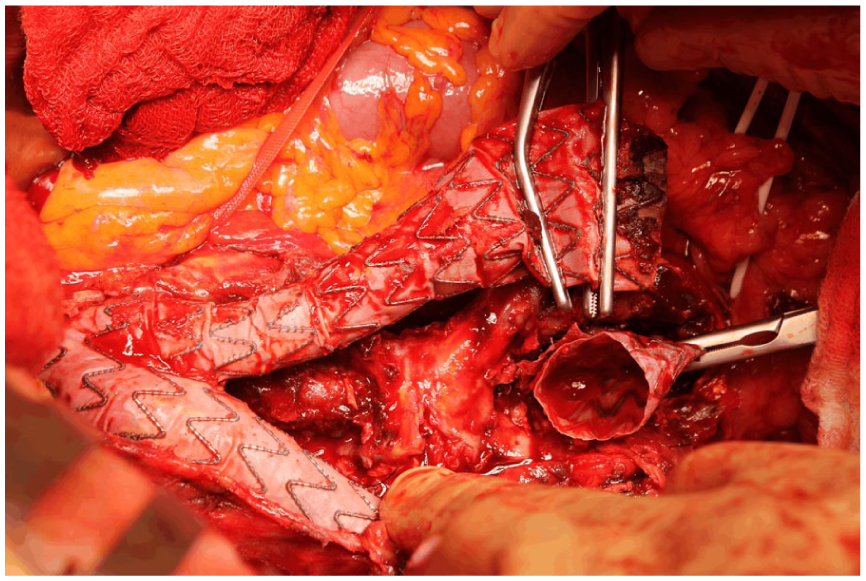
Intraoperative view of an 82-year-old male patient, undergoing an open surgery revision of a Medtronic Endurant II stent-graft prosthesis, 9.9 years after the initial EVAR procedure.
Discussion
Factors like neck motion, neck angulation, calcification, and oversizing can critically influence the stability of the suprarenal aortic endograft fixation to the aortic neck after EVAR.6,24 For example, significant neck movement over the years following implantation of the endograft, along with continuous anatomical changes in the sealing zone, may result in increased stress and material fatigue, leading to a partial or total BMS-SSS. Also, EL IIb with consecutive (rapid) (L)ASE as observed in patient 2 or sharp angulation and a wider neck as observed in patient 3 may compromise the proximal seal, while heavy calcification or inappropriate oversizing may increase the risk of suprarenal fixation failure.12-14 Especially, the severe neck angulation seems to play an important role in the development of BMS-SSS, as it is mentioned notably more frequently in the MAUDE database, referenced in the literature,12-14 and, not least, was observed as the most likely cause in one of our patients. Since the first implementation of the EVAR technique by Volodos 25 and Parodi, 26 different models of EVAR stent-graft prostheses, consisting of different materials and configurations, have been designed and widely established. Here, e.g., the occurrence of EL III could be reduced from 12.7% in early first and second EVAR generations to 1.2% in third-generation endografts due to improved material and design.27,28 Among several special features, the suprarenal fixation using uncovered bare metal stent-struts, which are attached with barbs or hooks to the aortic wall, 17 has been designed to fixate the main body of the EVAR stent-graft to the aortic wall and, thereby, to prevent distal migration of the prosthesis and, consecutively, EL I and (L)ASE.17,27,29,30 EVAR prostheses with this feature have become increasingly common, especially for the treatment of AAAs with hostile necks and challenging anatomy.17,27,31 While defects of the main body of the EVAR stent-graft have been widely described and may be categorized as EL IIIa and IIIb,11,20,28,32 the separation (also called detachment, disintegration, or fracture) of the suprarenal bare metal stent-struts has been described as a rare complication of EVAR stent-grafts without clear assignment to an EL type.18,33 Pathophysiological, the proximal part of the EVAR stent-graft, representing the proximal sealing zone, appears to be a weak point, susceptible to the separation of these two stent-graft components. Here, the hemodynamics in the aorta and the aneurysm sac, as well as the force of the downward blood flow exerts force on the seams of the junction between the uncovered bare metal stent-struts and the covered scaffold of the rest of the EVAR stent-graft prosthesis, entailing the risk for fracture of the seams with consecutive BMS-SSS18,19,21 Another discussed reason for BMS-SSS is the overdilatation of the proximal part of the EVAR stent-graft prosthesis during the implantation procedure, leading to a distortion of the metallic struts, fabric tear and consecutive rupture of the seams.28,30 This could be a possible explanation for the BMS-SSS in our case 3, since the proximal main body of the EVAR prosthesis was dilated several times and significantly to adapt the prosthesis to the aortic wall.
Particularly noteworthy is the fact that this specific defect has not yet been categorized as any of the known EL types. While a fabric tear and/or fracture of the metal scaffold is by definition to be assessed as EL IIIb,11,28,30 the BMS-SSS itself may lead to EVAR stent-graft migration and/or an EL Ia with (L)ASE and therefore imply the risk for, sometimes lethal, aneurysm sac rupture and a more frequent need for late open conversion.21,27,29 Moreover, the renal ostia are crossed in approximately one-third of EVAR cases by the bare metal stent-struts, 33 so that their separation and a demolition of the suprarenal fixation might result in renal artery injury as suprarenal fixation has been reported to cause renal infarction, renal artery occlusion and visceral compromise.17,20,31 Depending on the consideration of whether the uncovered bare metal suprarenal stent-struts and the covered part of the stent-graft prosthesis are regarded as 1 component or constitute 2 components, Massara et al 34 propose to define the defect as EL IIIa or EL IIIb. Following up on this argument, we recommend to consider both parts of the EVAR prosthesis as one component as they are not assembled in a modular manner intraoperatively (defect resulting in an EL IIIa), and since the intention is that the components do not come loose at all (defect resulting in an EL IIIb). Thus, for this rare occurring defect coming along with an EL Ia, the designation as an EL Ia/IIIb may be proposed.
Up to now, only 12 cases of BMS-SSS have been reported in the literature and a systematic review has recently been published by van der Krogt et al 6 in 2023, adding the latest 2 cases. Here, 10 cases with Cook and 2 cases with Medtronic prostheses were described. In 2016, several cases of BMS-SSS have been reported for recent EVAR stent-graft generations, e.g., 2 for the Cook Zenith and 1 for the Medtronic Endurant prosthesis.21,34 While BMS-SSS has already been described for older-generation Cook Zenith stent-grafts,19,24,35 Lindström et al. and Torres-Blanco et al. describe the first partial BMS-SSS for a Cook Zenith endoprosthesis after the industrial modification of the graft by use of double suturing between the uncovered bare metal stent-struts and the covered segment of the stent-graft, reinforcing the junction between these 2 parts. Here, the initial EVAR procedures were performed in 2006, 2011, and 2012 and the partial BMS-SSS occurred 2, 4, and 8 years, respectively, hereafter.18,21 The case reports indicating a higher occurrence of BMS-SSS in Cook Zenith endografts are consistent with, e.g., findings from the prospective Enzen trial conducted by De Athayde et al. 36 This trial revealed a significantly higher rate of late EL, specifically EL I and EL III, as well as increased rates of reintervention and aneurysm-related mortality in the Cook Zenith group compared with the Medtronic Endurant group.
According to van der Krogt et al, 6 up to now BMS-SSS has only been described in one Medtronic Endurant EVAR stent-graft (while our search of the MAUDE database yielded 11 results) 23 by Massara et al 34 in 2016. Here, a complete BMS-SSS was observed 4 years after the initial EVAR procedure. 34 Compared with Medtronic’s Talent stent-graft, the Endurant stent-graft has a reinforcement of the bare metal suprarenal stent-strut fixation where the woven polyester is sewn to self-expanding nitinol stent-struts (Figure 7). This may be responsible for the fact that almost no cases of BMS-SSS have been described so far for the Medtronic Endurant II stent-graft in the literature. However, 2 of the 3 implantations we reported were performed in accordance with the IFU. Regarding the treatment options, conservative, endovascular, or open repair therapies, 34 depending on the anatomical features and the current or expected complications, may be selected.
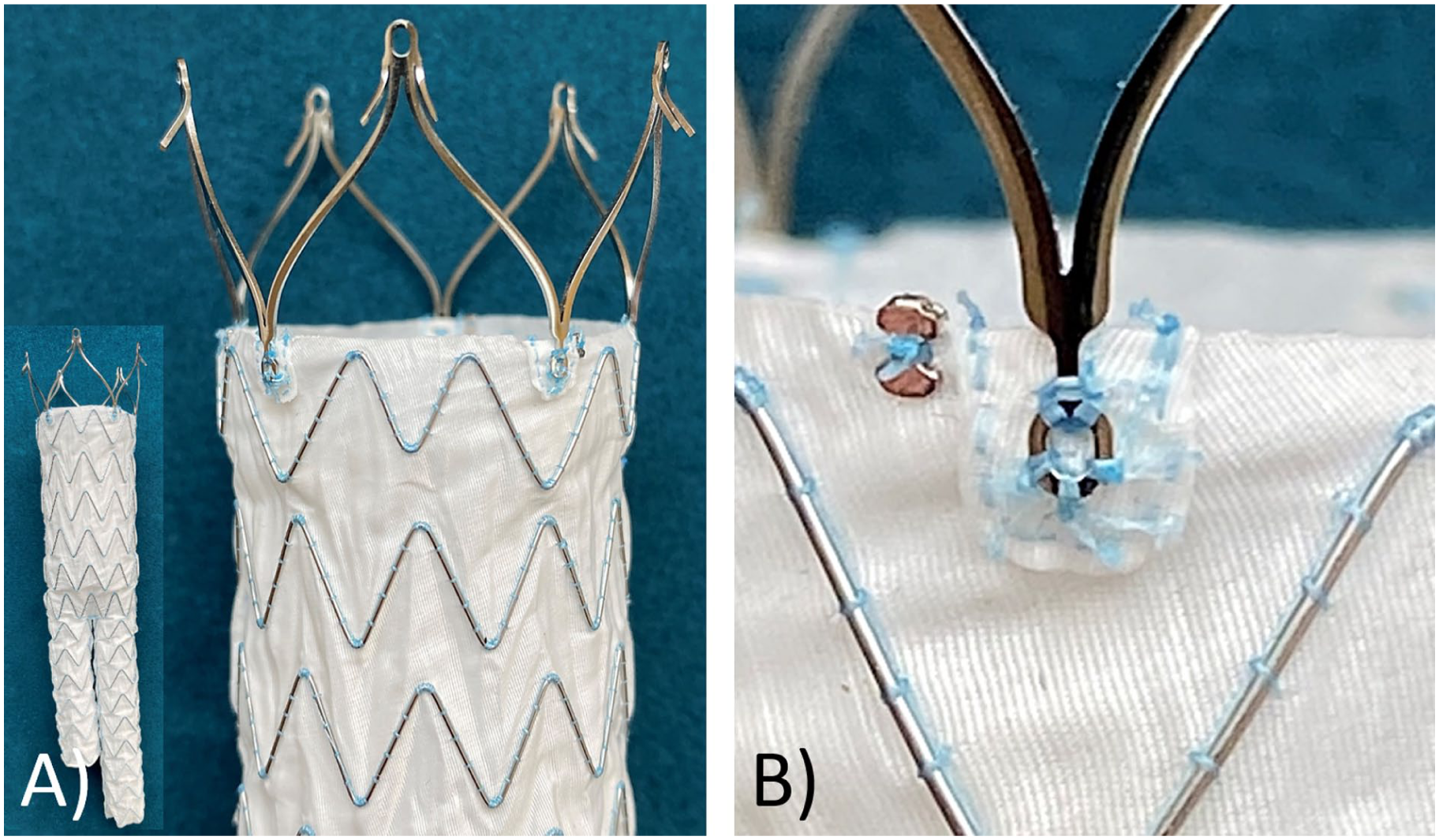
Medtronic Endurant II stent-graft for EVAR. (A) Proximal part of the stent-graft prosthesis (whole stent-graft prosthesis in the small image), showing the uncovered bare metal stent-struts with the proximal barbs for the fixation to the aortic wall as well as the covered part with the woven polyester, sewn to the self-expanding nitinol scaffold. (B) Close-up of the reinforced fixation of the uncovered bare metal stent-struts to the covered part of the stent-graft prosthesis.
Conservative treatment options can be provided to patients who are asymptomatic and who do not show any evidence for (L)ASE, analogous to cases of common EL III.20,37 In the case of symptomatic patients or an EL Ia/IIIb with (L)ASE, however, the indication for endovascular or open therapy must be made. 6 In our case 1, we refrained from invasive therapy due to the patient’s age and poor general condition, the stable conditions of the aneurysm sac as well as the chEVAR configuration of the stent-graft and recommended close follow-up investigations using CEUS, X-ray and CTA (Figures 1 and 2).
Choosing an endovascular therapy attempt, the re-alignment of the proximal EVAR main body stent-graft is the primary goal. Here, off-the-shelf18,21 or custom-made 24 cuffs, also with multiple fenestrations 17 may be applied. Also, a reimplantation of a main body of the EVAR prosthesis has been described to treat BMS-SSS. 24 In our case 2, an off-the-shelf cuff was implanted and additionally attached to the aortic wall, using endo anchors (Figure 4).
As a last resort, if no conservative or endovascular therapy option is possible, a late open conversion should be performed.27,29 This can be done as a full conversion with complete removal of the EVAR prosthesis, but also, if possible, as a partial conversion with removal of only parts of the EVAR prosthesis or as a semi-conversion with complete preservation of the EVAR prosthesis.5,10,38-41 For the latter semi-conversion, there is evidence of lower postoperative mortality and morbidity compared with, above all, a full conversion.40,41 The choice of the appropriate late open conversion procedure depends on the extent of the damage to the EVAR prosthesis and the possibility of its (partial) preservation.
Regarding preventing serious complications from BMS-SSS like stent-graft dislocation, (L)ASE and late secondary aneurysm rupture, an early detection of BMS-SSS and, therefore, a strict surveillance regime not to miss a partial or complete BMS-SSS is mandatory.17-19,21 In the case of the absence of an EL and a stable size aneurysm sac, a conservative approach may be justifiable by means of a strict follow-up regime using CEUS, conventional abdominal X-ray and CTA. In such a rare and potentially-life-threatening complication, the indication for therapy must be carefully considered and the optimal conservative, endovascular, or open therapy option selected for the patient. Although we can provide key information on the detection and treatment options of BMS-SSS, our study is limited by the small number of patients. For a more meaningful conclusion, it is necessary to detect and treat more patients with a BMS-SSS with the proposed therapy options.
Footnotes
Acknowledgements
Not applicable.
Ethical Considerations
Ethical approval was not required for this study, as no experiments involving humans or animals were performed.
Consent for Publication
All patients provided written informed consent for participation and publication.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used and analyzed during the current study are available from the corresponding author on reasonable request.
Publication Declaration
Parts of the work and patient data included in this manuscript have been previously published, the authors disclose this information explicitly hereby in the manuscript. One of the three cases described in the present manuscript has previously been published as a “Clinical Snapshot” in a national journal. The English text of that publication comprised 289 words and 1722 characters, which corresponds to approximately 7% of the total content of the current manuscript. A 3D reconstruction and a CTA image were also included in the prior publication; however, both visual materials are not part of the currently submitted manuscript.