
Abstract
Purpose:
To evaluate clinical outcomes and patency of endovascular stent-graft placement for iliac artery hemorrhage in patients with pelvic malignancy.
Methods:
We retrospectively reviewed 15 patients (21 cases) with pelvic malignancy undergoing emergency stent-graft placement for iliac artery hemorrhage from December 2011 to April 2025. Technical and clinical success, complications, primary patency, rebleeding rates, and survival were analyzed. Risk factors for rebleeding, specifically the degree of tumor invasion (encasement vs abutment), were assessed.
Results:
Technical and clinical success were 100%. Significant hemodynamic improvements were achieved: systolic blood pressure (85.5±32.8 vs 114.8±15.7 mmHg; p=0.014), and heart rate (110.7±24.0 vs 93.7±15.9 bpm; p=0.037). During a mean follow-up of 11.5 months, rebleeding occurred in 6 cases (28.6%). Tumor encasement was associated with a numerically higher rebleeding rate compared with abutment (40.0% vs 0%; p=0.123). Cumulative 1-year primary patency and survival rates were 82.9% and 52.5%, respectively.
Conclusion:
Stent-graft placement appears to be a feasible and potentially effective approach for immediate hemostasis in iliac artery hemorrhage associated with pelvic malignancy. However, careful surveillance is warranted due to a clinically notable risk of rebleeding, particularly in cases with tumor encasement.
Clinical Impact
Stent-graft placement offers a reliable, vessel-preserving endovascular option for achieving immediate hemostasis in catastrophic iliac artery hemorrhage associated with pelvic malignancy. This study demonstrates excellent technical and clinical success while identifying progressive tumor encasement as a potential marker for delayed hemorrhagic recurrence. These findings may help clinicians stratify rebleeding risk and tailor post-procedural surveillance according to the degree of tumor-vessel involvement. In cases of recurrent hemorrhage despite repeated stent-graft placement, collateral circulation should be carefully assessed, as therapeutic arterial sacrifice with coil embolization may represent an effective salvage strategy. This study provides practical guidance for managing a rare but life-threatening clinical condition.
Introduction
Massive hemorrhage from the iliac artery in patients with advanced pelvic malignancy is a rare but catastrophic complication associated with high mortality rates.1-3 This life-threatening condition can arise from direct tumor invasion, radiation-induced arteritis, or the formation of arterio-enteric or arterio-ureteral fistulas following extensive pelvic surgery and radiotherapy.4,5
Managing these patients poses a significant clinical challenge. Traditional open surgical repair is often precluded by the poor general condition of the patient and hostile surgical fields resulting from prior radical surgeries, radiation therapy, and extensive tumor infiltration.2,3 While transcatheter arterial embolization has been the mainstay for controlling pelvic hemorrhage, permanent occlusion of the common iliac artery (CIA) or external iliac artery (EIA) carries a high risk of severe ischemic complications, such as gluteal necrosis and lower-limb ischemia, which can devastatingly impact the quality of life in palliative care settings.6,7
Endovascular stent-graft placement has emerged as a viable alternative, offering the distinct advantage of excluding the bleeding focus while preserving distal arterial flow. 5 The efficacy of this vessel-preserving technique is already well recognized in other vital anatomic territories such as visceral, carotid, and subclavian arteries where maintaining perfusion to end-organs is critical.8-11 Although stent-graft utility is established in traumatic iliac injuries,12,13 literature regarding its specific use in malignant iliac artery erosion remains limited to small case series.1,2 Furthermore, concerns remain regarding the long-term durability of stent-grafts in infected or tumor-encased fields and the potential risk of delayed rupture or rebleeding complications. 14
Therefore, the purpose of this study was to evaluate the technical feasibility, clinical efficacy, and long-term patency of emergency stent-graft placement for the management of massive iliac artery hemorrhage in patients with pelvic malignancy. In addition, we sought to identify specific risk factors associated with rebleeding in this high-risk cohort.
Materials and Methods
Study Population
This retrospective study was approved by the institutional review board of our institution, and the requirement for informed consent was waived (approval no. SMC-2026-01-028-001). From December 2011 to April 2025, a total of 15 patients (21 procedural cases) with pelvic malignancy who underwent emergency stent-graft placement for iliac artery hemorrhage were included. The inclusion criteria were: (1) massive hemorrhage from the CIA or EIA confirmed by contrast-enhanced computed tomography (CT) or angiography; (2) underlying pelvic malignancy; and (3) unsuitability for surgical repair due to advanced disease or poor performance status. Patients were excluded if the hemorrhage originated from vessels other than the iliac arteries or if the bleeding was managed without the use of a stent-graft.
Interventional Procedures
All procedures were performed by experienced interventional radiologists under local anesthesia. Common femoral artery access was obtained, typically from the contralateral side (crossover approach) or the ipsilateral side depending on the lesion location and vascular tortuosity. Depending on the lesion location identified on CT, diagnostic aortography using a 5F pigtail catheter or ipsilateral iliac angiography was performed to identify the bleeding site. Once the lesion was localized, a stiff guidewire was advanced across the bleeding site. The stent-graft diameter was selected to be equal to or 1 to 2 mm larger than the reference diameter of the healthy proximal and distal vessel segments, as measured on pre-procedural CT scans. The length was chosen to ensure comprehensive segmental coverage of the lesion, providing at least 1 cm of overlap with the normal vessel wall at both the proximal and distal ends. The stent-grafts used in this study included self-expandable stent-grafts (Covera plus™; Becton Dickinson, Tempe, AZ, USA and Viabahn®; W.L. Gore & Associates, Flagstaff, AZ, USA) and balloon-expandable stent-grafts (Lifestream™; Becton Dickinson). The choice of stent-graft was determined by the availability of devices under national reimbursement guidelines or, otherwise, by the operator’s preference. Post-dilation was performed if necessary to ensure adequate wall apposition. Completion angiography was performed to confirm the exclusion of the bleeding focus and the preservation of distal flow.
Definitions and Follow-up
Technical success was defined as immediate exclusion of the bleeding sign such as extravasation or pseudoaneurysm and preservation of distal arterial flow. Clinical success was defined as the cessation of clinical signs of bleeding, stabilization of hemodynamic parameters, and no requirement for additional surgical or interventional procedures for hemostasis. Tumor invasion was classified as abutment (≤180o) or encasement (>180o) based on pre-procedural CT findings.15,16 Tumor necrosis was defined as a non-enhancing low-attenuation area within the tumor, with air-containing necrosis specifically identified by the presence of extraluminal gas bubbles.17,18 Prophylactic intravenous antibiotics (eg, piperacillin/tazobactam) were administered to patients with extensive tumor necrosis to prevent secondary infection. No graft-specific infectious complications were documented during the follow-up period. Follow-up contrast-enhanced CT was routinely performed at 1, 3, 6, and 12 months after the procedure, and additional imaging was performed as needed based on the patient’s clinical condition. Stent-graft patency was defined as the preservation of intraluminal flow through the stent-graft confirmed by follow-up CT or ultrasonography, without the need for any re-intervention. Rebleeding was defined as the reappearance of bleeding-related symptoms (eg, wound site bleeding, hematochezia, or hematemesis) following the initial treatment, with subsequent confirmation of a bleeding focus via CT or angiography that necessitated additional intervention or surgery.
Statistical Analysis
Continuous variables are presented as mean±standard deviation (SD) or median (range), and categorical variables are expressed as numbers and percentages. Paired t tests were used to compare pre- and post-procedural hemodynamic parameters (systolic blood pressure and heart rate). Univariate analysis using Fisher’s exact test or Pearson’s chi-square test was performed to identify risk factors associated with rebleeding. The cumulative rates of primary patency and patient survival were estimated using the Kaplan-Meier method. All statistical analyses were performed using SPSS software (version 27.0; IBM Corp., Armonk, NY, USA). A p value <0.05 was considered statistically significant.
Results
The baseline characteristics of the 15 patients (21 cases) are summarized in Table 1. The mean age was 62.7±15.9 years (range 34–93 years), and 60.0% were female. Gynecologic malignancies, including cervical, endometrial, and ovarian cancers, were the most common underlying pathologies (53.3%), followed by rectal cancer (13.3%) and liposarcoma (13.3%). The EIA was the most frequent site of bleeding (81.0%). Pre-procedural CT findings revealed tumor encasement of the affected vessel in 16 cases (76.2%) and tumor necrosis in 12 cases (57.1%) (Figure 1).
Baseline Demographics and Clinical Characteristics of Patients with Iliac Artery Hemorrhage (15 patients, 21 cases).
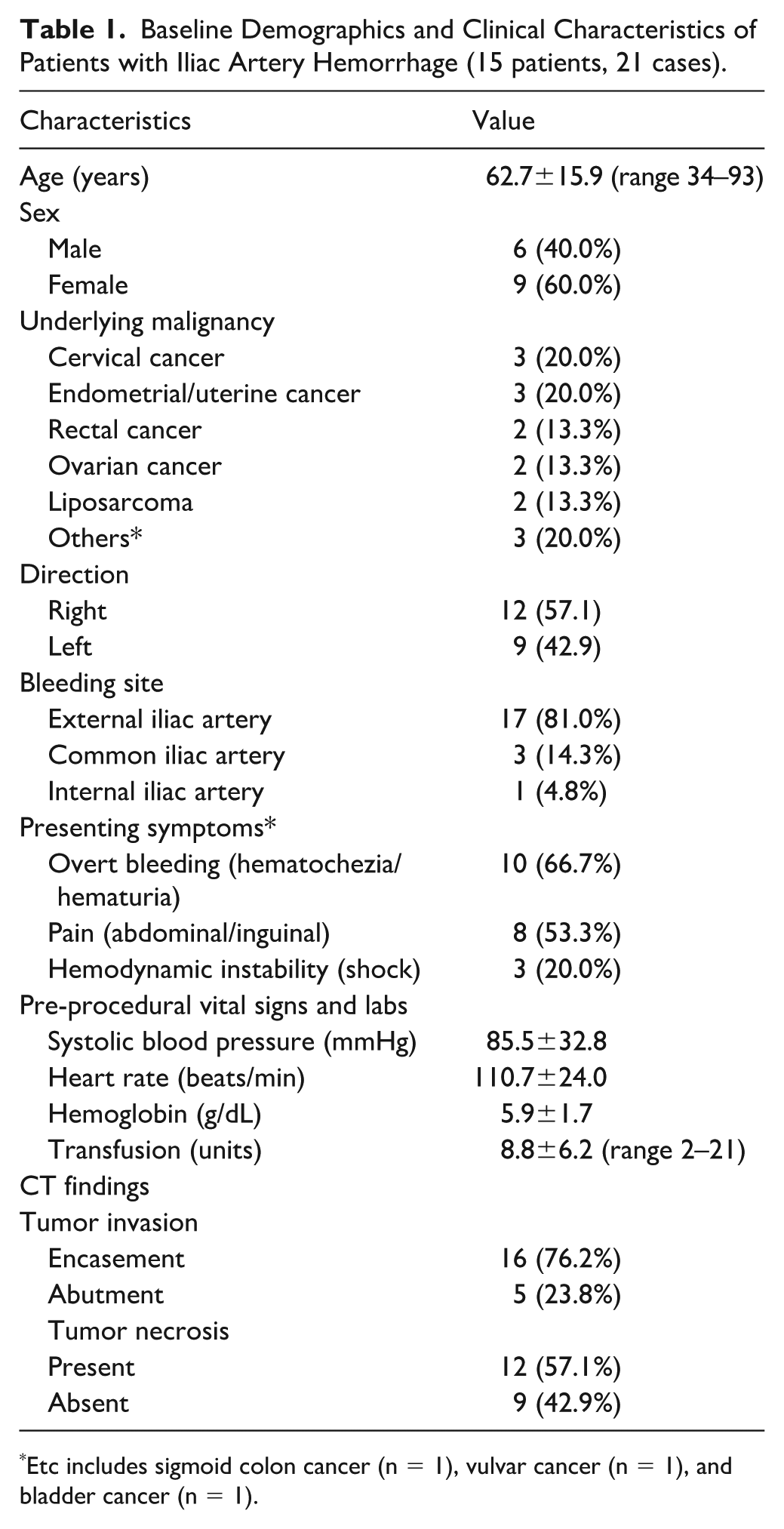
Etc includes sigmoid colon cancer (n = 1), vulvar cancer (n = 1), and bladder cancer (n = 1).
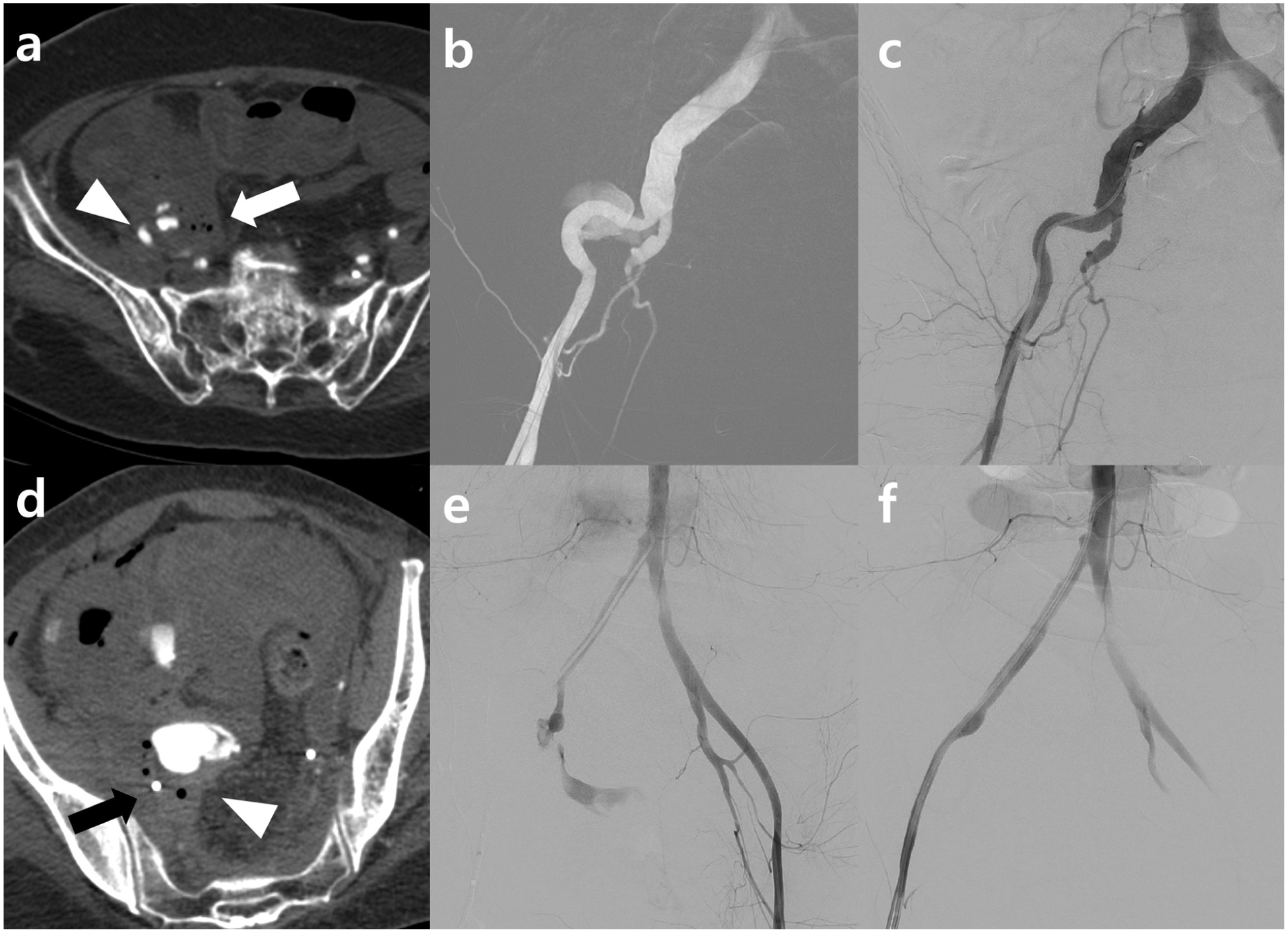
Comparison of tumor-vessel relationships and endovascular management. (
Procedural details and immediate outcomes are presented in Table 2. On initial angiography, contrast extravasation was observed in 13 cases (61.9%) and pseudoaneurysm in 8 cases (38.1%). Technical success was achieved in all 21 cases (100%). Notably, in one case involving the internal iliac artery, a stent-graft was selected over embolization to preserve pelvic circulation and prevent ischemia, as the patient had previously undergone contralateral internal iliac artery ligation. Clinical success was also 100%, with immediate hemodynamic stabilization in all patients. Following the procedure, systolic blood pressure significantly increased from 85.5±32.8 to 114.8±15.7 mmHg (p=0.014), and heart rate significantly decreased from 110.7±24.0 to 93.7 ± 15.9 bpm (p=0.037).
Procedural Details and Clinical Outcomes of Endovascular Stent-Graft Placement.
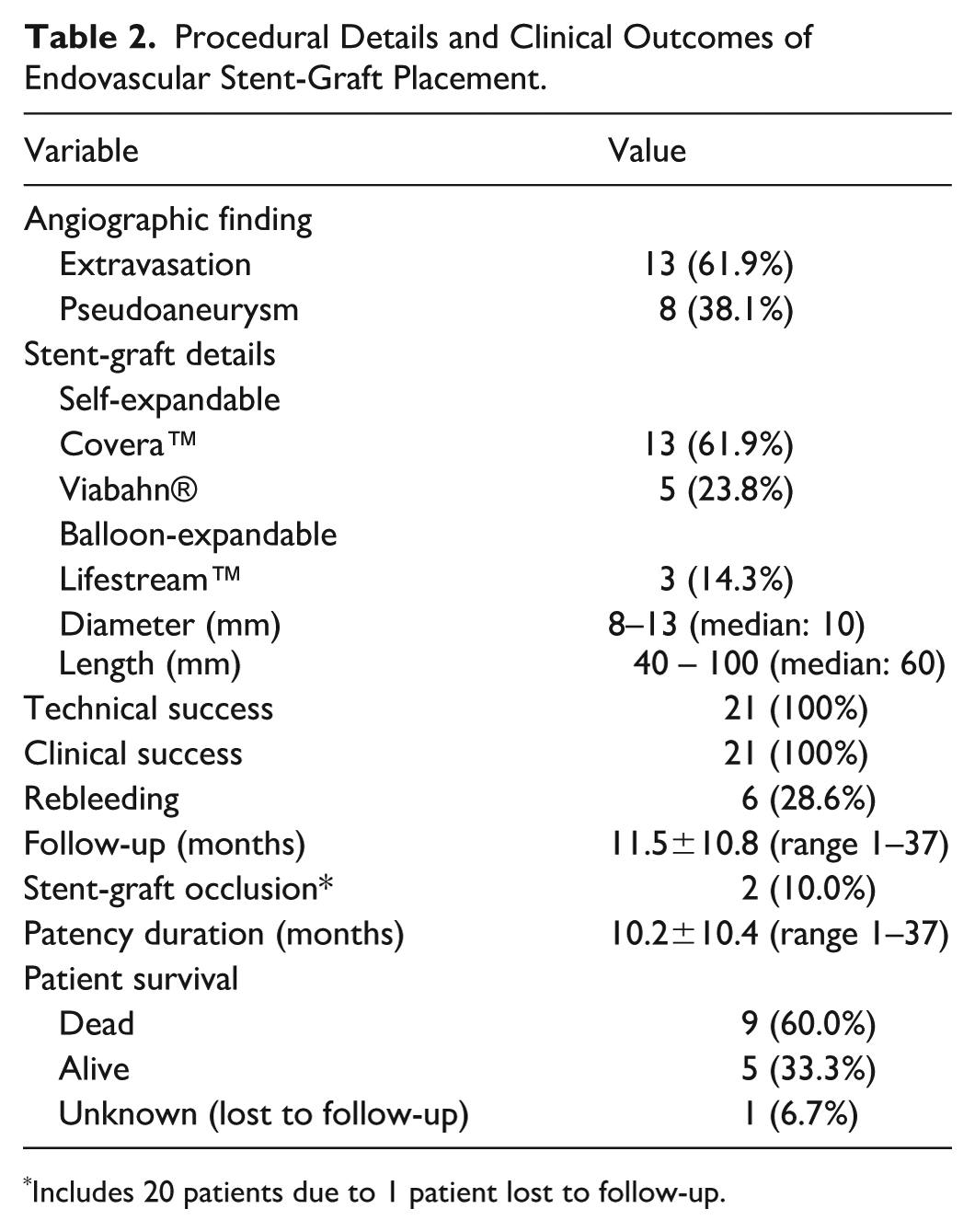
Includes 20 patients due to 1 patient lost to follow-up.
The mean follow-up period was 11.5±10.8 months (range 1–37 months), with one patient lost to follow-up. During the follow-up, stent-graft occlusion occurred in 2 cases (10.0%). The cumulative 1-year primary patency rate was 82.9%. Nine patients (60.0%) died during the follow-up period due to disease progression. The estimated median survival time was 26 months, and the cumulative 1-year survival rate was 52.5% (Figure 2).
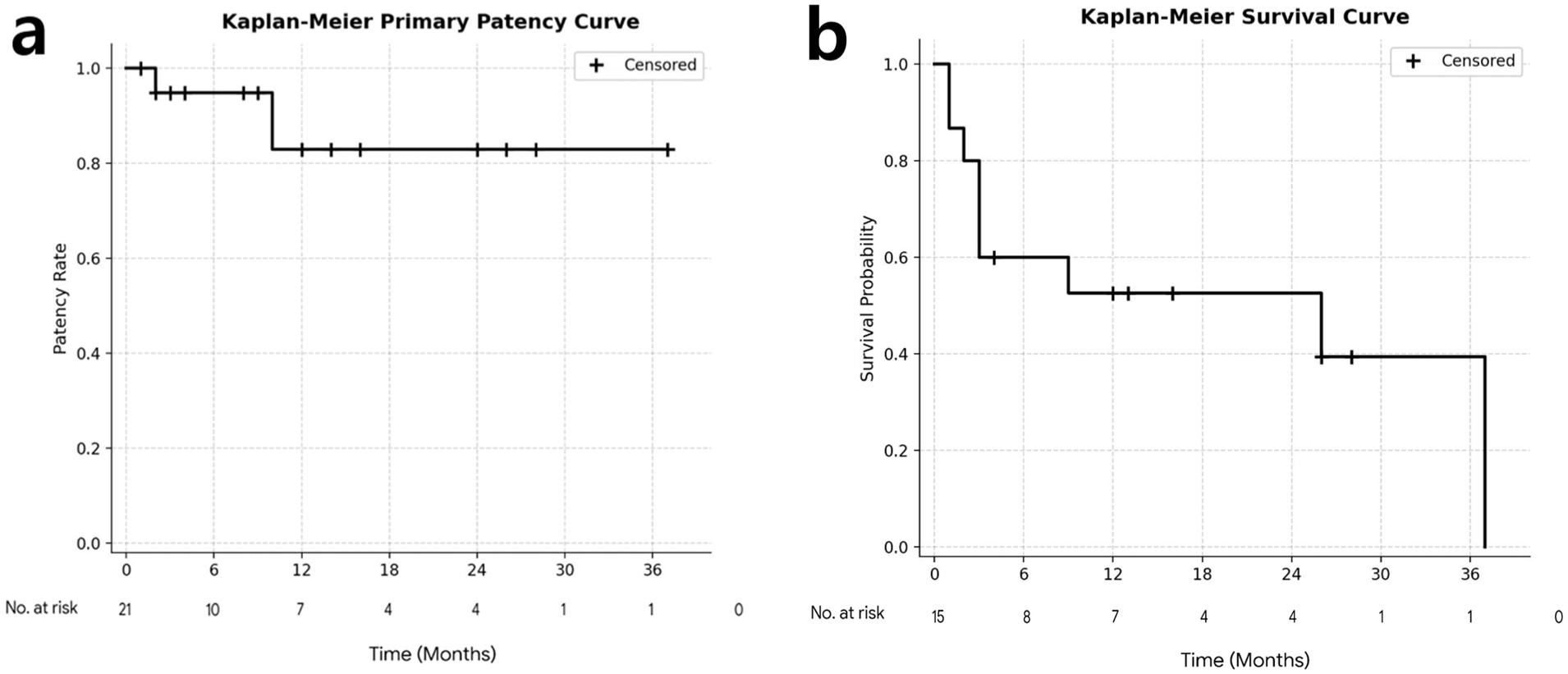
Kaplan-Meier analyses of clinical outcomes. (
Rebleeding occurred in 6 cases (28.6%) during the follow-up period. The results of the univariate analysis for factors associated with rebleeding are shown in Table 3. Although formal statistical significance was not reached, tumor encasement on pre-procedural CT was associated with a higher rebleeding rate compared with tumor abutment (40.0% vs 0%; none of the 6 abutment cases experienced rebleeding; p=0.123). Other factors, including sex (p=1.000), bleeding site (p=0.803), stent-graft type (p=0.526), and history of prior pelvic radiation therapy (p=0.598), were not significantly associated with rebleeding. There were no procedure-related major complications. One patient experienced a minor complication, specifically a pseudoaneurysm at the puncture site, which was successfully resolved with ultrasound-guided compression.
Univariate Analysis of Risk Factors Associated with Rebleeding (n=21).
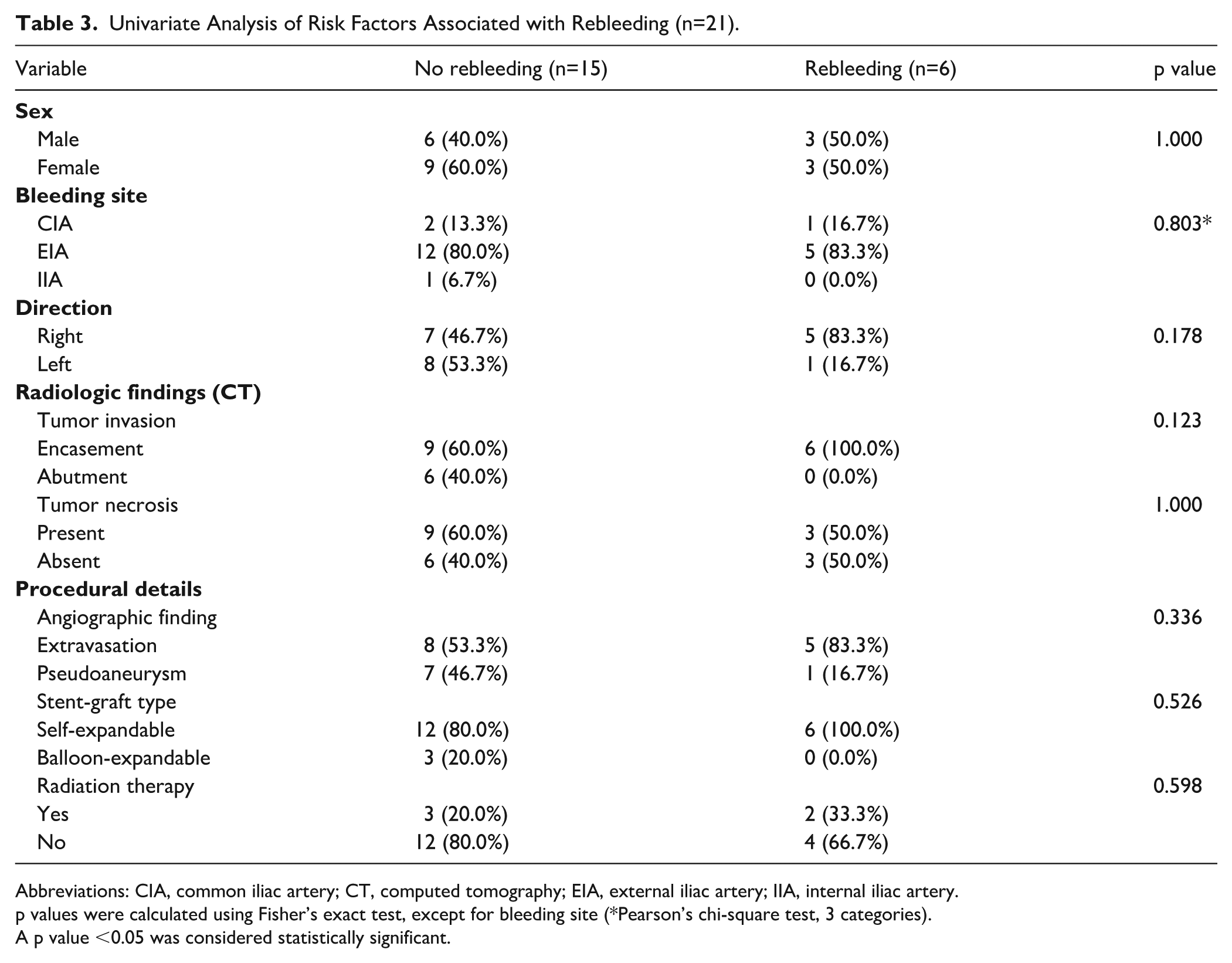
Abbreviations: CIA, common iliac artery; CT, computed tomography; EIA, external iliac artery; IIA, internal iliac artery.
p values were calculated using Fisher’s exact test, except for bleeding site (*Pearson’s chi-square test, 3 categories).
A p value <0.05 was considered statistically significant.
The detailed characteristics and mechanisms of the 6 rebleeding events are summarized in Table 4. Notably, 5 of the 6 events (83.3%) occurred at the distal edge of the stent-graft, despite angiographic and radiologic confirmation that the devices had been placed with sufficient longitudinal margins. Among these distal edge complications, the recurrences were primarily driven by progressive tumor encasement at the transition site (events 1, 4, 5, and 6). The remaining distal edge case (event 2) was attributed to mechanical failure, specifically proximal migration of the stent-graft leading to distal dissection. In contrast, one rebleeding event (event 3) occurred at the right CIA and was caused by arterial wall erosion secondary to progressive tumor invasion.
Detailed Characteristics and Mechanisms of Rebleeding Events (6 Events in 5 Patients).
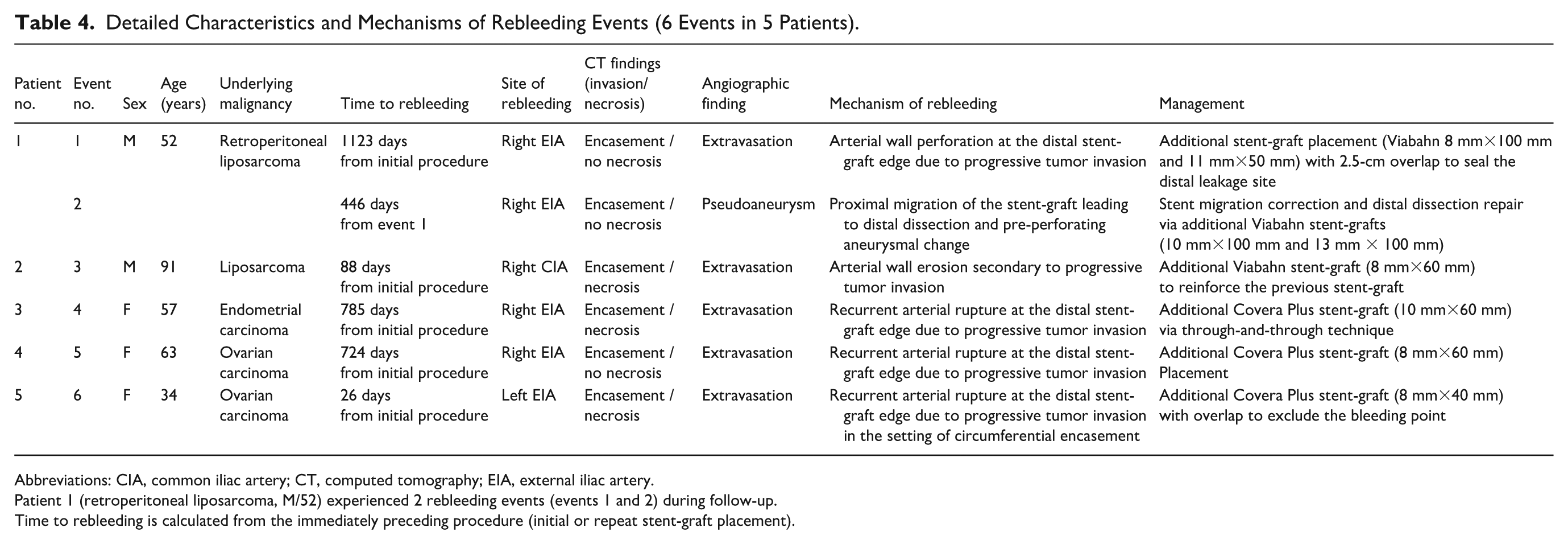
Abbreviations: CIA, common iliac artery; CT, computed tomography; EIA, external iliac artery.
Patient 1 (retroperitoneal liposarcoma, M/52) experienced 2 rebleeding events (events 1 and 2) during follow-up.
Time to rebleeding is calculated from the immediately preceding procedure (initial or repeat stent-graft placement).
Among the patients with rebleeding, 2 required complex repeated interventions. One patient underwent a total of 3 stent-graft procedures due to stent migration and subsequent dissection which was successfully managed with an additional stent-graft placement. Another patient experienced recurrent hemorrhage despite 2 successful stent-graft placements. Upon the third bleeding episode, angiography demonstrated robust collateral circulation from the internal iliac artery to the ipsilateral superficial femoral artery. Given the recurrent nature of the bleeding and the presence of adequate collaterals, the decision was made to sacrifice the EIA. The vessel was permanently occluded using coil embolization, which effectively controlled the hemorrhage without causing limb ischemia (Figure 3).
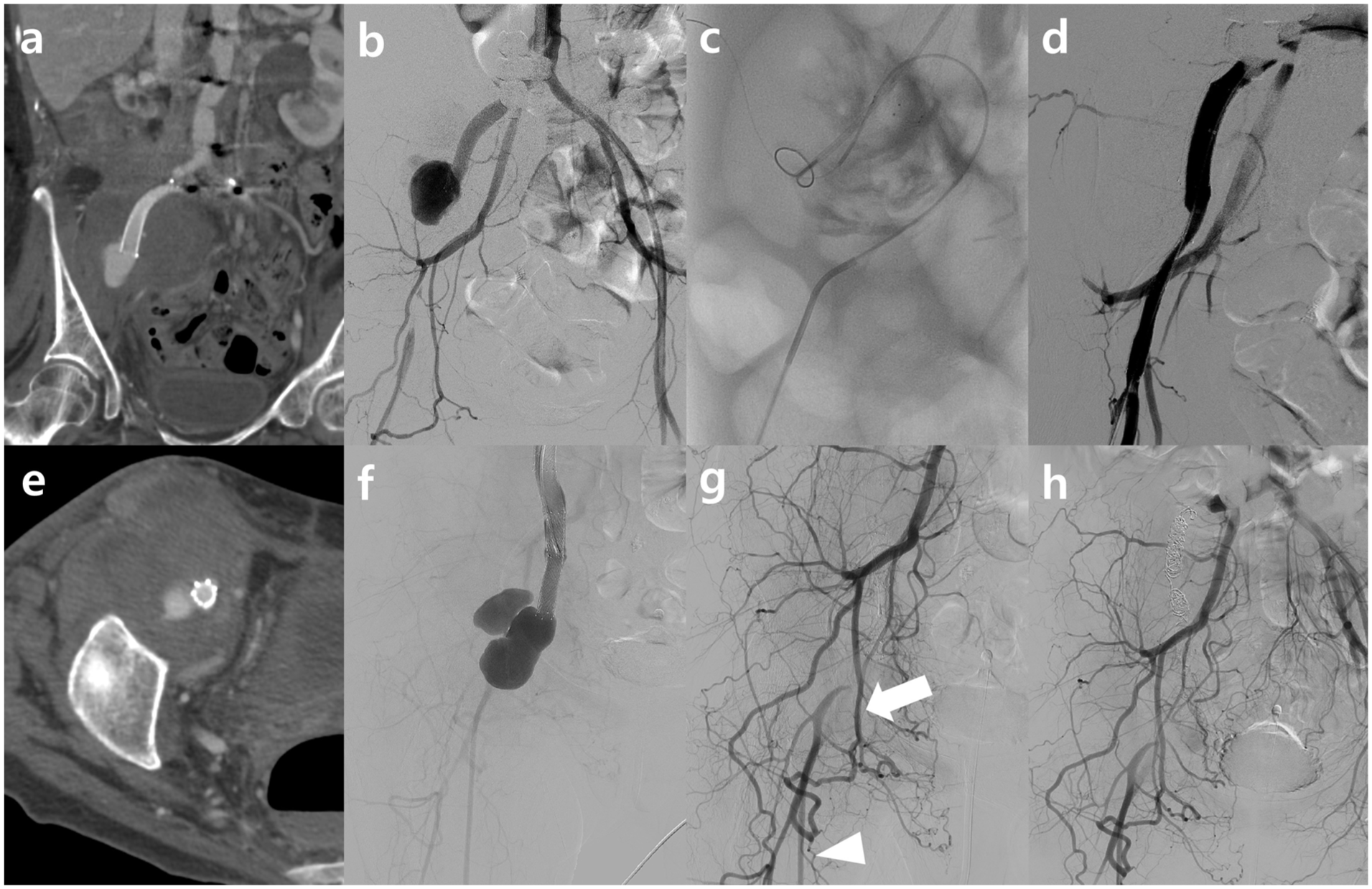
Sequential management of refractory hemorrhage in a 57-year-old female with endometrial cancer. (
Discussion
In this study, endovascular stent-graft placement demonstrated 100% technical and clinical success in controlling massive iliac artery hemorrhage in patients with pelvic malignancy. These findings underscore the effectiveness of stent-grafts as a rapid and reliable method for achieving hemostasis and hemodynamic stabilization in emergency settings. The cumulative 1-year primary patency rate was 82.9%. While this result is clinically acceptable given the patients’ critical condition, it is slightly lower than the outcomes reported in benign settings. In patients treated with stent-grafts for atherosclerotic iliac artery occlusive disease, the 1-year primary patency rates are reported to be as high as 91% to 96%. 19 Similarly, stent-grafts used for iatrogenic iliac artery rupture typically show excellent long-term patency with minimal complications.12,13,20 The comparatively lower patency in our study may be attributed to the patients’ poor general condition and hemodynamic instability, which frequently result in a low-flow state, predisposing to graft thrombosis. Furthermore, unlike benign lesions that merely compress the vessel, malignant tumors actively invade and destroy the arterial wall structure. This transmural erosion compromises the vessel’s integrity, creating a fragile hostile environment where the stent-graft lacks a healthy landing zone, thereby increasing the susceptibility to rebleeding or delayed rupture.14,21
In managing hemodynamically-unstable cases, we prioritized immediate and definitive stent-graft deployment. This approach is consistent with previous literature demonstrating that emergent endografting can successfully stabilize patients in hypovolemic shock by providing rapid and reliable exclusion of the bleeding focus. 22 Given that appropriate devices are typically accessible in emergency settings, direct stent-graft placement allows for streamlined hemostasis and effective clinical stabilization without the need for additional preparatory endovascular steps.
A notable finding in our study was the rebleeding rate of 28.6% during the follow-up period. This stands in sharp contrast to iatrogenic or traumatic iliac artery injuries, where rebleeding is extremely rare once the vessel is successfully excluded with a stent-graft.12,20 The degree of tumor invasion emerged as the most clinically relevant factor associated with rebleeding. Although univariate analysis did not demonstrate a statistically significant association between tumor encasement and rebleeding (p=0.123), likely attributable to the limited statistical power of this small cohort, the absolute difference in rebleeding rates between the two groups was clinically noteworthy. Rebleeding occurred in 6 of 15 encasement cases (40.0%), whereas none of the 6 abutment cases (0%) experienced any rebleeding event. In this small cohort, the absence of rebleeding among abutment cases may suggest that the degree of circumferential tumor involvement could serve as a potential prognostic indicator for hemorrhagic recurrence; however, given the small number of abutment cases (n=6 at the case level; n=5 at the patient level), these findings should be considered exploratory and hypothesis-generating, requiring validation in larger future studies. Radiologically, tumor encasement often implies transmural invasion of the vessel wall by the malignancy. 16 In such cases, the chronic radial force exerted by the stent-graft against a friable, tumor-infiltrated arterial wall may accelerate vessel erosion, potentially leading to delayed rupture. 14 In contrast, vessels with only partial tumor abutment likely retain some residual structural integrity of the arterial wall, allowing them to withstand the mechanical stress imposed by the stent-graft. If confirmed in larger studies, these exploratory findings could have potential clinical implications for risk stratification and post-procedural surveillance planning in this patient population.
Given the high rebleeding rate associated with tumor encasement, the extent of stent-graft coverage remains a critical procedural consideration. In our series, we primarily adopted a comprehensive segmental coverage strategy, ensuring the stent-graft encompassed the active bleeding site and the arterial segment significantly narrowed or encased by the tumor. However, we intentionally avoided extending the stent-graft into adjacent segments that appeared structurally intact on pre-procedural imaging. This decision was made to minimize potential mechanical complications, such as stent kinking or thrombotic occlusion. Therefore, we prioritized a balanced approach: providing definitive coverage for the vulnerable, tumor-involved segment while preserving the flexibility and patency of the surrounding vessel.
A characteristic finding in our rebleeding cases was that the majority of recurrent hemorrhages occurred specifically at the distal edge of the stent-graft, despite ensuring adequate coverage of the initially tumor-involved arterial segments. This observation suggests that rebleeding was not merely a result of insufficient initial coverage, but rather a consequence of progressive tumor invasion into the distal landing zone, where it synergistically interacted with existing biomechanical stresses. This mechanism parallels the biomechanical principles underlying a well-recognized complication of aortic endovascular repair, in which a mechanical mismatch between a rigid stent-graft and a fragile arterial wall at the distal landing zone generates excessive strain at the transition zone, leading to arterial wall injury. 23 The stiffness of a stented segment is significantly higher than that of the adjacent non-stented vessel, concentrating mechanical stress at the stent edge.
In the context of the iliac artery, its inherent mobility during hip movement may further exacerbate this stress. 24 The tendency of self-expanding stents to recoil toward their original straight configuration exerts continuous radial pressure and shear stress specifically at the distal landing zone. 23 As the malignancy progresses beyond the initially protected segment, this newly invaded distal wall, already weakened by tumor infiltration, becomes highly susceptible to erosion or new tear formation under such chronic mechanical irritation. Therefore, our findings underscore that even with sufficient initial coverage, the distal landing zone remains a vulnerable site for ongoing tumor-mediated destruction and mechanical failure, necessitating vigilant long-term surveillance.
Although prior radiation therapy and tumor necrosis were not statistically significant risk factors for rebleeding in our small cohort (p>0.05), their detrimental effects on vascular integrity are well-documented in other anatomical territories. A parallel can be drawn with carotid blowout syndrome (CBS) in head and neck cancer patients, which shares a similar pathophysiology of radiation-induced arteritis and tissue necrosis. Chang et al 10 and Wan et al 21 reported that while stent-grafts achieve high immediate hemostasis in CBS, they are associated with high rates of rebleeding and infection due to the hostile irradiated neck environment. Similarly, in cases of post-pancreaticoduodenectomy hepatic artery hemorrhage, which often involves skeletonized arteries exposed to pancreatic juice, stent-grafts are lifesaving but prone to long-term occlusion or infection. 25 Our study’s outcomes may align with these findings, suggesting that in a hostile pelvis characterized by radiation, malignancy, and potential infection, the stent-graft is vulnerable to similar complications, necessitating vigilant surveillance.
The management of rebleeding or mechanical failure following stent-graft placement presents a significant clinical challenge in patients with pelvic malignancy. As observed in our study, the hostile pelvic environment can lead to progressive vessel erosion or stent migration. In such complex situations, while vessel preservation remains the primary goal, permanent embolization can serve as a crucial bailout option when stent-grafts fail repeatedly. In our study, one patient experienced recurrent hemorrhage despite multiple stent-graft placements. Angiography revealed robust collateral circulation from the internal iliac artery to the ipsilateral femoral artery. Consequently, therapeutic occlusion of the EIA was performed, which successfully secured hemostasis without compromising limb viability. This approach is supported by previous studies suggesting that ligation or occlusion of the EIA can be well tolerated if the internal iliac artery and deep femoral artery are patent, allowing for adequate collateral perfusion. 26 This underscores the importance of individualized salvage strategies that adapt to the changing vascular anatomy and collateral status of the patient.
This study has several limitations. First, it is a retrospective study from a single center with a relatively small sample size, which limits the statistical power of our analyses. In particular, the limited number of abutment cases (n=6) precluded adequate statistical power to detect a formally significant difference in rebleeding rates (40.0% vs 0%), despite the clinically notable absolute risk difference. Second, the study population was heterogeneous, including patients with various primary malignancies, such as cervical, bladder, and rectal cancers, making it difficult to assess disease-specific outcomes. Third, due to the advanced stage of the underlying malignancies, the overall survival of the patients was short, preventing the assessment of long-term stent-graft durability and very late complications. Future multicenter studies with larger cohorts are needed to validate these findings.
Conclusion
Endovascular stent-graft placement appears to be a feasible and potentially effective palliative option for iliac artery hemorrhage in patients with pelvic malignancy. However, close surveillance is warranted, particularly in patients with tumor encasement, given the clinically notable risk of rebleeding. The exploratory observation that no rebleeding occurred among abutment cases warrants further investigation in larger prospective studies.
Footnotes
Ethical Considerations
This study was performed in line with the principles of the Declaration of Helsinki. The approval was granted by the Institutional Review Board of Samsung Medical Center (approval no. SMC 2026-01-028-001).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Informed Consent
The requirement for informed consent was waived by the institutional review board due to the retrospective nature of the study.
Trial Registration
Not applicable (Retrospective study).