
Abstract
Purpose:
Occupational radiation exposure remains a critical concern in modern health care due to cumulative health risks for procedural staff, stringent regulatory requirements, and the proliferation of advanced imaging technologies. This systematic review aimed to evaluate occupational radiation exposure among medical personnel during standard and complex endovascular aortic repair (EVAR) procedures, identify key determinants of radiation dose, assess the efficacy of protection strategies, and propose evidence-based recommendations to optimize staff safety in endovascular practice.
Methods:
A systematic review was conducted following PRISMA guidelines, searching MEDLINE, Cochrane Library, and Scopus databases from January 2019 to May 2025. Eligible studies reported quantitative dosimetric data for operating room staff during elective EVAR procedures, excluding ruptured aneurysm cases and non-English publications. Study selection and quality assessment was performed by 2 independent reviewers using ROBINS-I tool.
Results:
From 942 screened studies, 18 met inclusion criteria, revealing significant occupational intraoperative radiation exposure variability. Eligible studies reported dosimetric data in terms of absorbed dose (D), effective dose (ED), personal dose equivalent Hp(10) for whole-body exposure, Hp(3) for eye lens dose, Hp(0.07) for skin and extremities dose, as well as peak skin dose (PSD). The ranges of D, ED, Hp(10), Hp(3), Hp(0.07), and PSD were 0.02 to 0.12 μGy, 0.40 to 4350.00 μSv, 0.00 to 6112.70 μSv, 0.25 to 2500.00 μSv, 0.20 to 971.00 μSv, and 190.00 to 8430.00 μGy, respectively. Operator exposure patterns showed consistent left-sided predominance (left eye 200.00 vs right eye 30.00 μSv; left hand 76.90 vs right hand 46.70 μSv). Advanced imaging technologies demonstrated substantial protective benefits: 3D image fusion reduced operator ED by approximately 55% to 66%, while dual fluoroscopy with digital zooming decreased median doses by 62%. Suspended lead shielding systems eliminated axillary exposure in some cases. Supporting staff received lower but non-negligible exposure, with scrub nurses sustaining higher doses than circulating nurses.
Conclusion:
Complex EVAR procedures continue to pose significant occupational radiation risks despite technological advancements. The findings emphasize the need for optimized protection protocols, particularly for ocular exposure, standardized dosimetric reporting practices across institutions, and continued development of low-radiation or radiation-free navigation technologies. Future research should prioritize multicenter prospective studies with standardized metrics to evaluate long-term health outcomes among surgeons performing complex EVAR operations.
Clinical Impact
This systematic review offers a comprehensive synthesis of current evidence on occupational perioperative radiation exposure during minimally invasive endovascular stent grafting, providing vascular teams with insights to enhance radiation safety protocols. By analyzing dose patterns across different procedure types and technologies, the study highlights effective protective measures, incorporating newfangled imaging systems and shielding solutions. The findings support clinical decision-making by demonstrating how specific interventions can reduce staff exposure while maintaining procedural efficiency. Using an evidence-based approach, this framework guides institutions in optimizing radiation safety programs, improving staff training, and facilitating the integration of dose-reduction technologies in contemporary endovascular practice.
Introduction
Endovascular aortic repair (EVAR) has undergone remarkable evolution since its inception, progressing from standard infrarenal aneurysm exclusion to increasingly complex procedures along the entire aorta. 1 Fenestrated and branched EVAR (f/bEVAR), in particular, has expanded the treatment spectrum of aortic aneurysms but requires prolonged fluoroscopy and advanced imaging, substantially increasing radiation exposure risks for operators. Nonetheless, despite improvements in radiation protection strategies and imaging technologies, exposure to ionizing radiation during fluoroscopically guided interventions (FGIs) poses significant patient and occupational health risks, from cataract formation to carcinogenesis and hereditary genetic effects.2-5 The scatter radiation dose accumulation from repeated interventions coupled with the rapid adoption of complex EVAR at high-volume centers has brought renewed attention to occupational radiation protection, particularly as procedures become more intricate and prolonged. 6
To mitigate radiation exposure risks for interventionalists performing FGIs, the International Atomic Energy Agency (IAEA) has established comprehensive safety guidelines through its Safety Standards Series.7,8 Developed in accordance with International Commission on Radiological Protection (ICRP) recommendations, these standards define strict occupational dose limits and mandate rigorous adherence to the As Low As Reasonably Achievable (ALARA) principle.9,10 Despite universal implementation of the ALARA protocol in clinical settings, operator radiation exposure during EVAR procedures continues to vary significantly. The inconsistency in the reported dose levels arises not only from procedural complexity and variations in imaging technology but also from the operator’s proximity and positioning relative to the patient and the x-ray source.11-14 This variability is further compounded by inherent challenges in occupational dosimetry, including discrepancies in dosimeter placement across body regions, inconsistent use of lead protection, and the difficulty of comprehensively measuring exposure for unprotected areas such as the eyes, hands, and lower limbs.
While earlier reviews by Monastiriotis et al, 15 Dindyal et al, 16 and Hertault et al17,18 provided valuable insights, the introduction of next-generation imaging systems, innovative lower-profile endografts, and refined EVAR protocols has transformed clinical practice, necessitating an updated evaluation of occupational radiation exposure risks.
The objective of this systematic review is to summarize and analyze existing evidence on occupational radiation exposure during standard and complex EVAR procedures, identify case-specific risk factors, highlight best practices for radiation safety, and propose future research directions to optimize radiation protection for medical personnel involved in such interventions.
Materials and Methods
Published evidence on intraoperative radiation exposure on operating room staff during standard and complex EVAR cases was systematically reviewed using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) framework. 19
Databases and Search Strategy
Identification of the studies was accomplished through an all-inclusive search of electronic databases and by manual review of relevant articles’ reference lists. The search encompassed National Library of Medicine’s MEDLINE database (via PubMed), Cochrane library, and Scopus, covering studies from January 2019 to May 2025. The last search was conducted on June 1, 2025. Initial screening was conducted without language restrictions to ensure comprehensive coverage. The search strategy included database-specific controlled vocabularies, namely Medical Subject Headings (MeSH) for PubMed and Cochrane, and both MeSH and Emtree terms for Scopus. A comprehensive search approach that involved both exploded MeSH terms and free-text keywords was performed. These elements were conjoined with the “AND”/“OR” Boolean operators for optimal retrieval of apposite reports. The complete search syntax for each database is documented in Table 1. Prior to commencing the present review, the study protocol was registered in PROSPERO (International Prospective Register of Systematic Reviews) to guarantee methodological disclosure and prevent duplication of research efforts (Registration ID: CRD420251087283).
Search Strategy of the Electronic Databases.
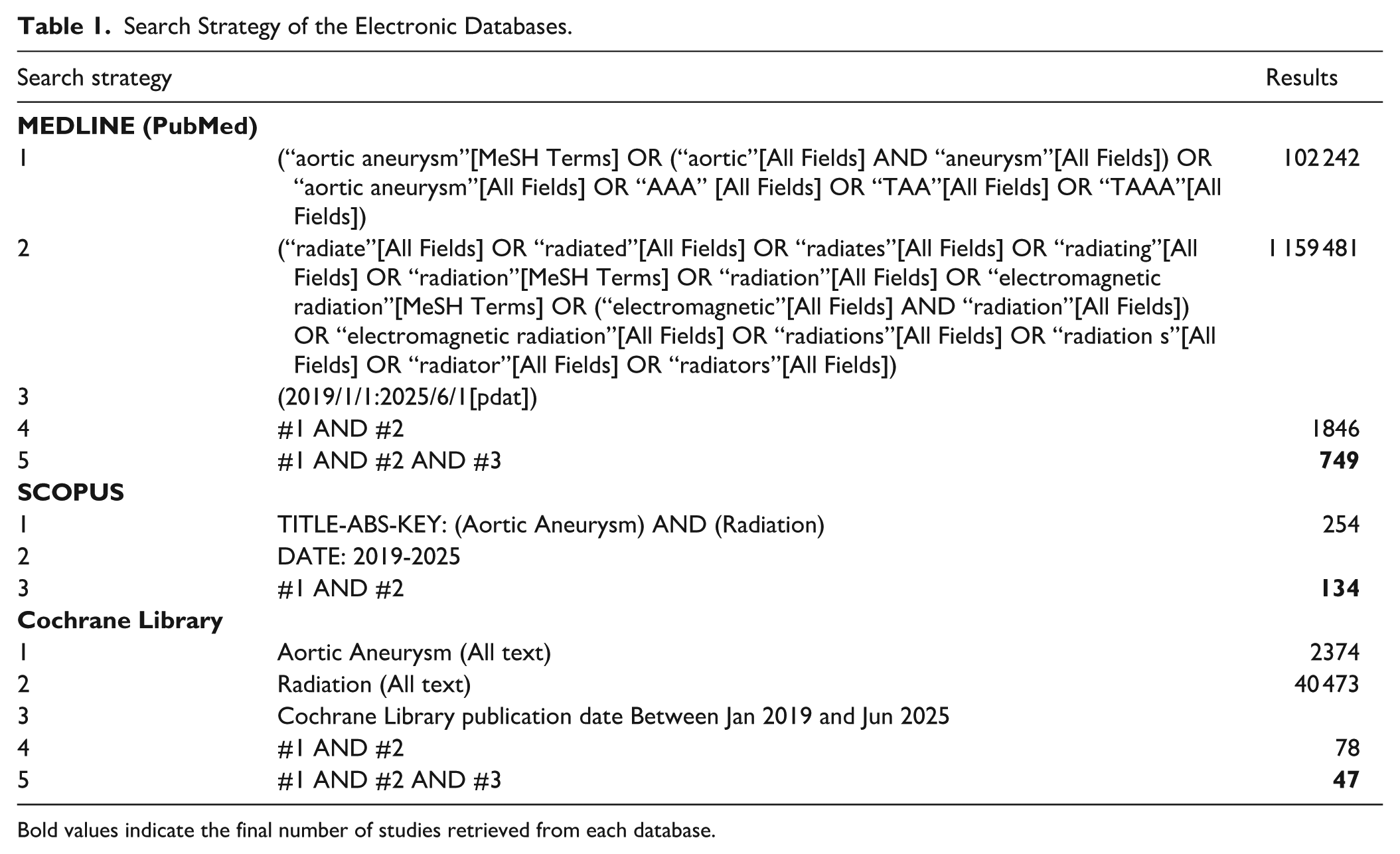
Bold values indicate the final number of studies retrieved from each database.
Study Selection and Risk-of-Bias Assessment
The identified studies were compiled using the Mendeley software (Elsevier B.V., Amsterdam, The Netherlands), while the duplicates were removed using the Ablebits Duplicate Remover extension (4Bits Ltd, Gomel, Belarus) in Microsoft Excel (Microsoft Corp., Redmond, Wash). Two independent reviewers conducted the eligibility assessment in an unblinded standardized manner. Discrepancies regarding study inclusion were resolved through consensus. In cases where consensus could not be immediately achieved, a third senior reviewer was consulted to provide the final decision. The ROBVIS (Risk Of Bias VISualization) online application as well as the latest version of ROBINS-I (Risk Of Bias In Non-randomized Studies – of Interventions, Version 2) 20 tool was used to illustrate the risk-of-bias in the shape of “traffic light” (Figure 1) and weighted bar plots (Figure 2).
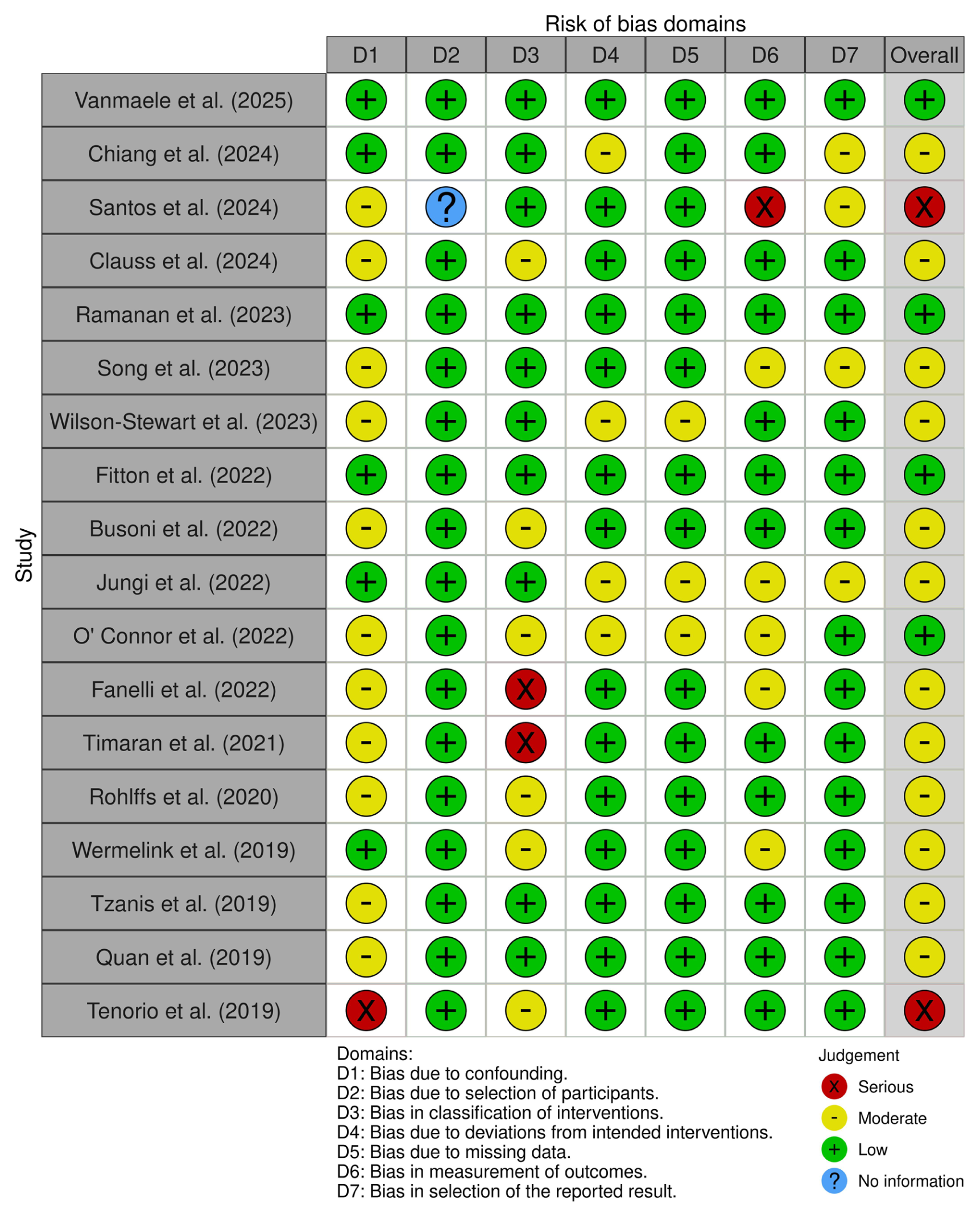
Domain-level risk-of-bias assessment for individual studies, presented as a “traffic light” plot.
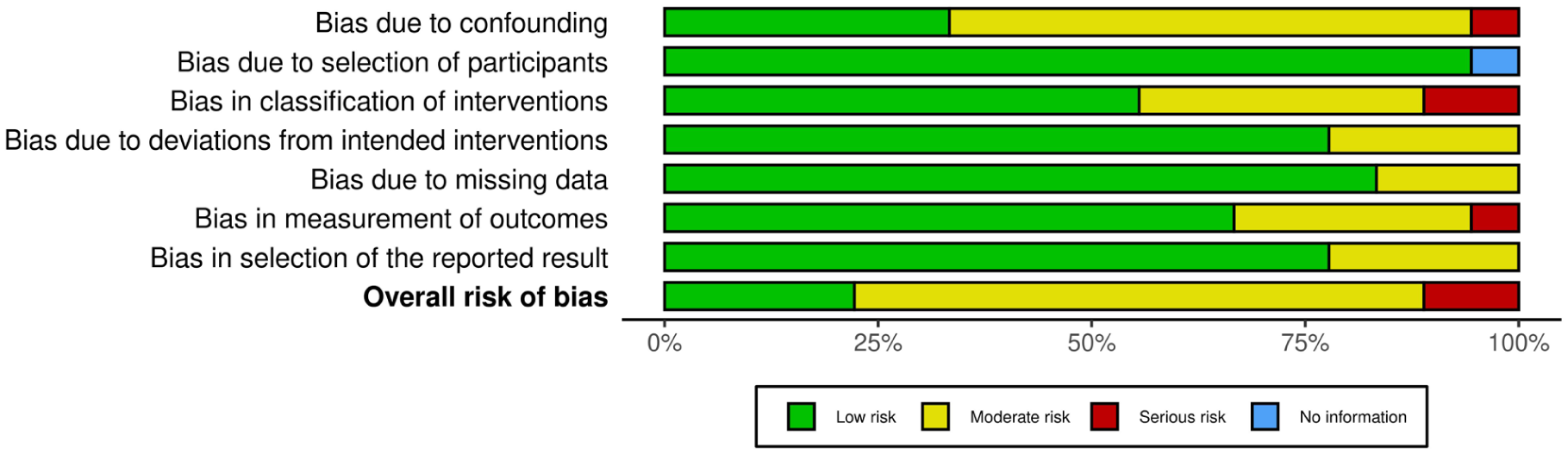
Weighted bar plot of the allocation of risk-of-bias judgments within each bias domain.
Eligibility Criteria
Table 2 summarizes the inclusion and exclusion criteria applied during study selection.
Inclusion and Exclusion Criteria for EVAR Radiation Exposure Studies.
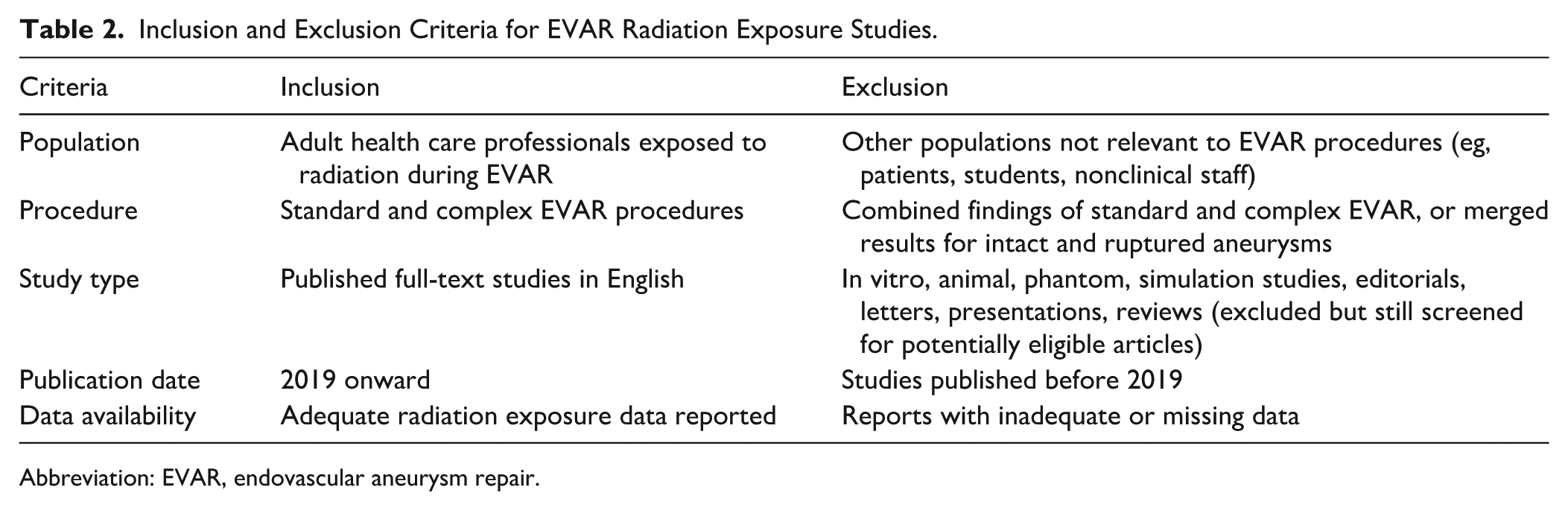
Abbreviation: EVAR, endovascular aneurysm repair.
Dosimetric Quantities
In the present review, staff’s dosimetry is reported by the means of ED, which is the risk of a nonuniform, whole-body exposure, equivalent doses Hp(10) (occasionally correspondent to ED), Hp(3) (corresponds to eye lenses’ dose), and Hp(0.07) (typically correspondent to skin and extremities dose), all measured in Sievert (Sv). The values in the parentheses denote the tissue depth (in millimeters) at which the dose is measured. For eye lens dose assessment, Hp(3) was measured using dosimeters placed at the temporal or periorbital region. Depending on the study protocol, dosimeters were positioned either outside protective lead eyewear or inside the glasses. Table 3 specifies which approach was used in each included study. The absorbed dose (D), as well as the PSD, which is the maximum dose absorbed by the skin at a single region, both measured in gray (Gy), is also used to assess the occupational radiation exposure. An elaborate description of the used dosimetric quantities can be found in the ICRP’s Publication 103. 9
Studies Reporting Occupational Doses in Standard and Complex EVAR Procedures.
Abbreviations: EVAR, endovascular aneurysm repair; EVARib, endovascular aneurysm repair with iliac branch; fEVAR, fenestrated endovascular aneurysm repair; TEVAR, thoracic endovascular aneurysm repair; f/bEVAR, fenestrated/branched endovascular aneurysm repair; EPD, electronic personal dosimeter; OSLD, optically stimulated luminescent dosimeter; TLD, thermoluminescent dosimeter; D, absorbed dose (measured in mGy); Hp, equivalent dose; ED, effective dose; PSD, peak skin dose (measured in μGy); SD, standard deviation; mm, millimeters; NA, not available; NS, not specified.
Dose values reported as median (interquartile range).
Dose values reported as median (range).
Dose values representation is not reported.
Dose values reported as median (interquartile range), (range).
Dose values reported as geometric mean (95% confidence interval).
Dose values reported as median.
Dose values reported as mean ± standard deviation.
Dose values reported as median (standard deviation), (range).
The Niklason algorithm requires a dosimeter placed over the thyroid lead collar and a dosimeter placed under the lead apron.
Results
Following the described methodology, 942 studies were yielded by the search, of which 18 met our inclusion criteria by specifically evaluating intra-procedural occupational radiation exposure during standard and complex EVAR interventions. The findings from the qualified studies form the core evidence base of our analysis (Figure 3). The included studies reported occupational exposure in terms of D, 21 ED,13,32,34,35,37 Hp(10),22-24,28,31,33 Hp(3),21,23,24,27-30 Hp(0.07),24,25,28 and PSD 36 (Table 3). Table 3 provides additional information on the fluoroscopy system used, the specific EVAR technique, the number of interventions performed, the dosimeter type, and the badge placement.
Selection process flowchart for publications reporting occupational radiation exposure in standard and complex EVAR procedures. EVAR, endovascular aneurysm repair.
Staff radiation doses were measured using electronic (“active”) dosimeters with live readout, thermoluminescent dosimeters (TLD), and optically stimulated luminescent dosimeters (OSLD). Some studies assessed ED without specifying dosimeter type32,37 or PSD. 36 Six studies used passive dosimetry (TLD or OSLD),21,24,25,29,30,35 7 used active dosimetry,13,22,26,28,31,33,34 and 2 combined both methods.23,27 Dosimeters were placed across multiple anatomical sites including the head, temporal or periorbital region, neck, torso, and extremities. Hp(3) was most frequently assessed, followed by ED and Hp(10), whereas Hp(0.07), D, and PSD were less commonly reported. All studies applied radiation shielding according to ALARA principles.
Radiation Exposure During Standard EVAR
Nine studies exclusively reported standard EVAR procedures.21-24,26,27,29,30,32 In all reported cases, the primary operator was positioned on the right side of the patient, and vascular access was predominantly transfemoral, with 1 study not specifying the access site.
For primary operators, Hp(10) ranged from 0.00 to 66.00 μSv, Hp(3) from 0.25 to 150.00 μSv, ED from 0.01 to 435.00 μSv, and PSD from 180.00 to 843.00 μGy. Supporting staff received lower but measurable doses, with scrub nurses generally experiencing higher exposure than circulating nurses, while anesthesiologists remained relatively protected.
Standard EVAR procedures were consistently associated with lower and less variable radiation exposure for both operators and staff compared with complex f/bEVAR, representing a relatively low occupational risk under typical protective measures.
Radiation Exposure During Complex f/bEVAR
Nine studies evaluated complex f/bEVAR procedures.13,21,24,25,28-30,33,37 In 8 of these studies, the primary operator was positioned on the right side of the patient, whereas 1 study reported an operator on the left side, although no radiation exposure data were available for this individual. 28 Vascular access was primarily transfemoral, with 2 studies also incorporating right brachial access. In 1 of these studies, 37 radiation exposure by access site was not reported. In contrast, Rohlffs et al 13 demonstrated that relocation of the operator to the brachial access position was associated with higher radiation exposure, consistent with closer proximity to the x-ray tube and greater backscatter.
For primary operators, Hp(10) ranged from 11.00 to 266.00 μSv, Hp(3) from 7.55 to 2500.00 μSv, ED from 4.70 to 4350.00 μSv, and PSD from 180.00 to 8430.00 μGy. Supporting staff doses were generally lower but non-negligible, with scrub nurses sustaining higher exposure than circulating nurses, whereas anesthesiologists remained relatively protected.
Advanced imaging systems, protective devices such as Zero Gravity and leg wraps, and procedural optimizations demonstrated substantial dose reductions in several studies. Operator position and vascular access influenced exposure, particularly during complex procedures, where proximity to the x-ray tube during brachial access increased radiation dose compared with transfemoral access. Compared with standard EVAR, complex f/bEVAR procedures were associated with higher exposure and greater inter-study variability for both operators and staff.
Clinically Meaningful Differences Between Standard and Complex EVAR
Direct comparison between standard EVAR and complex f/bEVAR highlights substantial and clinically relevant differences in occupational radiation burden. Primary operators performing complex f/bEVAR experience notably higher doses across all measured quantities, with ocular exposure potentially exceeding ICRP annual limits in high-volume centers, whereas standard EVAR typically remains well below regulatory thresholds. Supporting staff, although generally exposed to lower doses, also experience higher radiation levels during complex procedures, particularly scrub nurses working close to the operative field. Advanced shielding, dose-minimization strategies, and careful planning are particularly critical in complex f/bEVAR workflows, where prolonged fluoroscopy time and multiple access routes significantly increase scatter radiation.
Discussion
Existing systematic and narrative reviews on occupational radiation exposure during EVAR procedures have been constrained by outdated fluoroscopic equipment and shielding systems and were further limited by inconsistent reporting of staff doses and dosimeters used.15-18 The current work provides a comprehensive analysis on occupational dosimetry encompassing all relevant dosimetric quantities and explicitly documenting the specific dosimeter models employed across studies. Furthermore, this review synthesizes contemporary data on advanced imaging and radiation protection solutions, such as digital zooming, CBCT fusion, Zero Gravity, and Fiber Optic RealShape (FORS), offering a meticulous assessment of their dose-reduction efficacy. By analyzing data from 18 studies published between 2019 and 2025, this review demonstrated that despite technological advancements in imaging systems, radiation protection strategies and gear, significant variability persists in staff exposure levels. Our findings underscore a clinically significant disparity in occupational radiation exposure between standard EVAR and complex f/bEVAR procedures. Whereas standard EVAR generally maintains operator and staff doses well below regulatory limits, complex f/bEVAR can result in exposure approaching the ICRP annual limits for the eye lens and other tissues, particularly in high-volume centers or during brachial access. These differences reinforce the importance of dedicated radiation protection strategies, including optimal operator positioning, lead shielding, adoption of advanced imaging technologies, and staff training. Clinically, this information informs risk-benefit assessments, workflow planning, and institutional safety protocols for high-complexity EVAR interventions.
Main or Assistant Operator
All studies included in this review assessed radiation exposure to primary or secondary operators by means of D, ED, Hp(10), Hp(3), Hp(0.07), and PSD. In every case, the operator was either the main or the assistant vascular surgeon performing the EVAR interventions.
Vanmaele et al 21 examined the impact of 114 f/bEVAR procedures on the unprotected periorbital skin, demonstrating that the main operator’s left eye lens, which is located closest to the x-ray tube, received the highest D and Hp(3) compared with his right periorbital side (0.12 vs 0.02 mGy and 200.00 vs 30.00 μSv, respectively).
Chiang et al 22 compared the measured occupational doses with the estimations attained during an EVAR-simulation phantom experiment, concluding that the actual staff doses may be up to 4.62 times greater than the dosimeter’s reading, depending on the personnel’s role, location, and body part exposed. Regarding the operators, the primary operator’s Hp(10) registered 257.60 μSv at the left chest level, measured above lead shielding. By comparison, the assistant operator’s exposure at the same anatomical site was significantly lower at 20.00 μSv, reflecting a 92.2% reduction in radiation dose relative to the primary operator.
Serna Santos et al 23 quantified the primary operator’s Hp(10) across multiple anatomical sites using conventional shielding and the suspended Zero Gravity (ZG; Biotronik, Berlin, Germany) radiation protection system. While both systems reduced scattered radiation, dosimeter beneath the lead apron at the surgeon’s left axilla detected no measurable exposure during Zero Gravity deployment (1.50 vs 0.00 μSv, P < .001). Although Zero Gravity reduced Hp(10) at the left temple by 82.5% relative to conventional shielding (1.10 vs 6.30 μSv, P < .001), the latter yielded lower doses at all other measured anatomical sites.
Clauss et al 24 appraised radiation exposure during endovascular repair of thoracic, thoracoabdominal, infrarenal, and aortoiliac aneurysms, denoting that main operators received considerably higher whole-body, hand, and ankle doses contrasted with assistant surgeons. It is worth noting that assistant operators sustained greater ocular irradiation. Furthermore, their study identified a direct correlation between procedural complexity and increased radiation exposure to main operators.
The prospective study carried out by Ramanan et al 25 on 40 complex f/bEVAR procedures exhibited that properly positioned lead-equivalent leg wraps dramatically attenuated scattered radiation exposure to primary operators’ lower extremities by 95% compared with unprotected conditions (2.70 vs 54.20 μSv, P < .001).
Song et al 26 demonstrated a remarkable reduction in operator radiation exposure during robotic-assisted EVAR compared with conventional manual procedures. The radiation dose to the surgeon at the robotic console was 96.5% lower than that recorded at the procedure table, highlighting the system’s potential to eliminate occupational hazards (4.00 vs 110.00 μGy). This reduction is attributed to the remote operation capability, which allows the surgeon to perform EVAR from a shielded workstation, significantly decreasing scatter radiation exposure. Wilson-Stewart et al 27 found that EVAR procedures resulted in significantly higher operator eye doses (7.55 μSv) compared with other FGIs of the chest, abdomen, pelvis, or limbs, even when additional table-mounted shielding was in place.
The study by Fitton et al 28 demonstrated a significant reduction in radiation exposure for both primary and secondary operators after implementing improved ancillary shielding barriers during complex f/bEVAR procedures. For the main operator, median dose reductions were most notable at the lower limbs (99.1%), neck (45.4%), and left hand (41%), while eye exposure decreased by 27.7%. The second operator also showed substantial reductions, particularly at the lower limbs (97.7%), neck (72.9%), and hands (37%-68%). Interestingly, no detectable dose was recorded at the upper chest (under the apron) for either surgeon, confirming the effectiveness of lead aprons in shielding the torso.
Busoni et al 29 measured surgeon eye lens doses during various FGIs, finding a remarkable difference between standard EVAR and complex fenestrated endovascular aneurysm repair (fEVAR). For EVAR, the median eye lens dose per procedure was 49.00 μSv, whereas fEVAR resulted in a much higher dose of 2500.00 μSv; the greatest Hp(3) value included in the present systematic review.
Jungi et al 30 found that implementing a modern dose reduction program significantly decreased surgeons’ eye lens radiation exposure during EVAR, thoracic endovascular aneurysm repair, and f/bEVAR procedures in hybrid suites, with reductions of 74.7% (from 470 to 119 μSv, P = .001), 79.3% (from 570 to 118 μSv, P < .001), and 55.4% (from 700 to 312 μSv, P = .036), respectively.
In their study, O’Connor et al 31 recorded an Hp(10) value of 11.00 μSv for the primary operator during an EVAR procedure, using an active personal dosimeter placed over the lead apron on the left chest.
Fanelli et al 32 compared radiation exposure between 2 equal-sized groups undergoing EVAR, an intravascular ultrasound (IVUS)-guided group and a control group treated using conventional iodinated contrast-enhanced approach. Results showed a 53% reduction in operator’s ED when IVUS was used (21.00 vs 45.00 μSv, P = .040).
The complex procedures evaluated in the prospective study of Timaran et al 33 gave rise to operator Hp(10) values, which, as expected, depend on the number of vessels involved in the treatment. Specifically, for devices designed to involve 4 fenestrations/branches, the median operator dose was higher when compared with those involving 3 or less fenestrations/branches (262.00 vs 171.00 μSv, P < .010). Furthermore, the authors identified dual fluoroscopy as the imaging method leading to significantly lower median operator dose in comparison with conventional imaging (128.50 vs 309.00 μSv, P = .010). Dual fluoroscopy provides real-time, complementary views of the operative field by using 2 fluoroscopic images simultaneously, without the need to move the C-arm or increase radiation output. When combined with live-image digital zooming, one image shows the primary live view, whereas the second displays a digitally zoomed reference view on a monitor. This approach enhances visualization of vascular anatomy and device positioning without relying on standard electronic magnification. Digital zooming uses image processing rather than reducing the detector field, preserving image size while avoiding increased radiation exposure, which helps minimize scatter radiation for both patients and operating room staff. In line with these advantages, Timaran et al 33 demonstrated a substantial reduction in radiation exposure for the primary operator when using dual fluoroscopy with live-image digital zooming, with median operator dose decreasing from 266 to 101 μSv (P < .010), representing a 62% reduction compared with standard electronic magnification.
Rohlffs et al 13 conducted an extensive analysis comparing radiation exposure during fEVAR and bEVAR procedures. Their findings revealed that fEVAR performed with the Allura Xper system resulted in significantly higher first and second operator radiation doses compared with bEVAR (208.00 vs 57.00 μSv and 52.00 vs 10.00 μSv, respectively). A comparison was also conducted between the standard Allura Xper FD20 and the advanced Allura ClarityIQ systems. The results showed a substantial 66.1% reduction in Hp(10) for the first operator (from 230.00 to 78.00 μSv, P = .160) and, interestingly, a minor increase of 13% for the second operator (from 23.00 to 26.00 μSv, P = .700).
Wermelink et al 34 estimated the ED across 4 experienced vascular surgeons. Two surgeons who consistently used 3D fusion technology had the lowest ED (13.00 μSv). In contrast, the other 2 surgeons showed significantly higher EDs (24.00 and 44.50 μSv, respectively), probably owing to less frequent use of 3D fusion and differences in procedural technique. Interestingly, no significant decrease in ED was observed across 3 consecutive half-year periods following the introduction of EVAR in their hybrid suite (0-6 months: 180.00 μSv; 7-12 months: 25.00 μSv; 13-18 months: 22.00 μSv), despite the apparent downward trend. This suggests that the learning curve for radiation dose optimization in EVAR procedures may plateau early among experienced operators, with individual technique and technology adoption playing a more critical role than cumulative experience alone.
The highest Hp values reported by Tzanis et al 35 were recorded for the left hand of the primary operator (76.90 μSv), followed by chest (72.60 μSv, above the lead apron) and right hand (46.70 μSv). Noteworthy doses were also measured at the head, eye lenses, and thyroid, whereas the exceptionally low ED of 4.70 μSv, estimated using the Niklason algorithm, is the lowest value documented in this review for operators during EVAR procedures.
Quan and Lee 36 represent the sole researchers in this analysis to assess operator PSD, a metric previously restricted to patient radiation monitoring. Their comparative analysis between mobile C-arm and hybrid room setups revealed that the right neck and shoulder absorbed the highest doses with C-arm use (1770.00 and 1480.00 μSv, respectively), while the lower apron region received maximal exposure (8430.00 μSv) in hybrid rooms. It should be stated that the applicability of PSD to operators warrants caution. By definition, PSD represents the dose delivered at the skin’s most irradiated area from both primary beam and scatter radiation. 6 However, qualified staff is exposed solely to scatter radiation, limiting the validity of PSD as an operator-specific metric.
Tenorio et al 37 demonstrated a significant reduction in operator ED during f/bEVAR as imaging technology advanced. Despite increasing procedural complexity and case volume, the operator’s monthly radiation exposure significantly decreased from 3260.00 μSv with early systems to 2180.00 μSv with modern cone beam computed tomography (CBCT) capabilities. Per-case doses also declined pronouncedly, from 260.00 to 90.00 μSv (P = .001), highlighting the effect of onlay fusion and CBCT on minimizing operator radiation exposure.
Operator radiation exposure during EVAR procedures shows wide variability, with ED and Hp values influenced by procedural complexity, imaging technology, and protective shielding. Reported EDs for primary operators range from as low as 4.70 to above 260.00 μSv in more complex f/bEVAR cases. Hp(10) values at the chest have been reported from 11.00 μSv up to 257.60 μSv, while the left hand, which is typically closest to the radiation source, can absorb doses up to 76.90 μSv. Ocular exposure range widely, spanning from 7.55 μSv in standard EVAR to as high as 2500.00 μSv in complex fEVAR interventions. Use of advanced imaging systems like CBCT and protective solutions such as Zero Gravity or leg wraps has been shown to reduce operator doses by 60% to 99.1%, highlighting the importance of technological and procedural optimization to minimize occupational radiation exposure.
While the present systematic review did not consider simulation-based studies, the work of Harbron et al 38 represents a pioneering effort in estimating operator organ doses (ODs). Future radiation safety protocols may benefit from OD assessments, leading to more robust occupational hazard analyses in EVAR interventions.
Nursing, Anesthesiology, and Other Staff
During an EVAR procedure, multiple team members besides the primary operators are exposed to scattered radiation, including anesthesia providers, scrub and circulating nurses, radiology technologists, and occasionally industry representatives or trainees. Their proximity to the x-ray source varies depending on their role, with anesthesia teams typically positioned near the patient’s head, whereas nursing staff and radiology technologists assist near the operative field. While their exposure is ordinarily inferior to that of the main and assistant operators, their prolonged presence in the surgical suite entails strict compliance with ALARA principle.
In the study by Chiang et al, 22 the sterile nurse received the lowest occupational radiation dose among the staff involved in EVAR procedures. Median Hp(10) dose measured at the left chest and above the protective apron was 3.70 μSv, with a range from 1.10 to 92.60 μSv.
In the EVAR procedures analyzed by Wilson-Stewart et al, 27 circulating nurses received an average eye dose of 0.25 μSv – the lowest Hp(3) value encompassed in this review – which was significantly lower than the scrub nurses’ dose of 3.37 μSv.
The study by Timaran et al 33 reported major reductions, up to 66%, in radiation exposure for operating room staff during f/bEVAR procedures using dual fluoroscopy with digital zooming. Compared with standard electronic magnification, the median Hp(10) figures for the first assistant (fellow), scrub and circulating nurses, as well as anesthesia staff were notably lower with the digital zooming technique.
In the work by Rohlffs et al, 13 both the sterile and nonsterile nurses were the sole members among the entire surgery team that exposed to significantly lower EDs when, instead of the stock Allura Xper FD20, the leading-edge Allura ClarityIQ technology was used (6.90 vs 2.20 μSv and 1.00 vs 0.40 μSv, respectively). The anesthesiologist’s ED showed an insignificant 84.1% reduction, decreasing from 4.40 to 0.70 μSv (P = .640). Compared with fEVAR procedures, bEVAR interventions performed with the Allura Xper led to significantly higher radiation doses for the nonsterile nurse (1.50 vs 0.40 μSv, P = .049). The sterile nurse’s ED showed an insignificant reduction of 54.6%, decreasing from 11.00 to 5.00 μSv (P = .110), whereas the anesthesiologist’s ED demonstrated a nonsignificant 30% increase (4.00-5.20 μSv, P = .800). On the contrary, neither bEVAR nor fEVAR interventions conducted with Allura ClarityIQ technology resulted in significant differences in occupational EDs for the sterile and nonsterile nurses as well as the anesthesiologist.
Nursing, anesthesiology, and other clinical staff involved in EVAR procedures sustain measurable but in general low radiation doses, with exposure levels differing by capacity and proximity to the x-ray source. Scrub nurses, working closest to the operative field, typically experience higher doses compared with circulating nurses. Anesthesia providers, positioned near the patient’s head, receive low to moderate exposure levels, though doses can alter depending on imaging equipment and procedural complexity. Advanced imaging technologies, such as Allura ClarityIQ and digital magnification, have exhibited significant dose reductions – up to approximately 66% in some cases – particularly for nursing staff.
Radiation Safety in EVAR – Key Recommendations and Future Directions
Although innovations in fluoroscopy equipment and technological advancements in shielding materials have shown notable dose mitigation, disparities persist in occupational radiation exposure during standard and complex EVAR interventions due to variations in procedural complexity, lead shielding compliance, as well as staff role and positioning inside the operating room. Dependent on numerous adjustable and intractable factors, the scattered radiation from the patient consists the sole source of clinical staff exposure in justified and optimized procedures.39,40 This becomes of crucial importance in complex f/bEVAR cases which pose the highest risk due to prolonged fluoroscopy time (FT). 41
Given these persistent radiation exposure challenges and their critical implications for complex endovascular procedures, the subsequent section outlines some pivotal strategies and emerging innovations to minimize occupational hazards in EVAR workflows.
Prioritize Eye Lens Protection
While the entire staff receive low yet considerable doses, the main operator remains at greatest risk, particularly regarding eye lens exposure, where the accumulated Hp(3) in high-volume centers could exceed the ICRP annual limit of 20 mSv.21,29,30 Owing to its contiguity to the x-ray tube, the main operator’s left eye receives important amounts of scatter radiation. 21 Wrap-around lead eyewear is mandatory and should be combined with full-face radiation shields for optimal protection. 42
Enforce Real-Time Dosimeters
In addition to the mandatory passive dosimetry, vascular surgeons should consider active dosimeters as supplementary protection. 10 Wireless real-time dosimeters offer continuous monitoring and immediate feedback on radiation exposure levels and must be configured with both visual and audible alerts when approaching preset dose and dose rate thresholds. Active dosimeters should be visible to the entire vascular team to encourage collective awareness and safer practices. For optimal monitoring, integration with novel smartphone applications is recommended. 43
Shift Toward Novel Shielding Systems
While traditional lead aprons remain essential, newer suspended shielding systems like Zero Gravity eliminate physical strain and provide superior protection for the operator’s axilla and eyes. However, current evidence shows these systems restrict mobility, complicate ancillary shield use, and impair communication, demonstrating a clear trade-off between ergonomic considerations and radiation safety. 23 Until these limitations are addressed, the integration of lightweight, lead-free materials in protective gear has shown particular promise in reducing fatigue and musculoskeletal disorders without compromising radiation safety. 44
Minimize Fluoroscopy Duration
Reducing FT is essential for radiation safety. Operators should use short bursts of imaging rather than continuous exposure, particularly during catheter or guidewire manipulations. Techniques like “last image hold” allow image review without additional radiation. Keeping “beam on” time to an absolute minimum directly reduces dose to both patients and staff. 45
Maximize Personnel-to-Radiation Source Distance
Maintaining maximum distance from the radiation source is of paramount importance. The inverse square law dictates that radiation exposure decreases dramatically with distance; doubling the distance from the x-ray source reduces exposure by a factor of 4 (75%). All personnel in the operating theater should also develop a reflexive safety behavior of stepping back during the high-dose digital subtraction angiography (DSA) runs. 46
Remember the Legs
Despite the widespread use of protective drapes beneath the patient table, most vascular teams skip leg wraps during EVAR interventions, assuming adequate radiation shielding. While this practice may seem reasonable, recent studies demonstrated outstanding reduction in lower limb radiation exposure, up to 99.1%, when leg wraps are worn.25,28 Even though dose delivered to the legs is typically low, the potential long-term risks should not be overlooked.
Avoid Oblique Projections
Steep C-arm angulation, frequently required during complex aortic repairs, significantly increases scatter radiation, particularly at head level. Operator exposure escalates dramatically when positioned on the same side as the x-ray source, with doses up to 6 times higher compared with contralateral positioning. The cranial left anterior oblique projection poses the greatest risk, as the x-ray tube’s proximity to the operator maximizes backscatter radiation. 46 To diminish radiation exposure, the x-ray tube should ideally be positioned opposite the operator whenever feasible.
Establish Structured Radiation Safety Education and Simulation Training Programs
Comprehensive education forms the foundation of effective radiation protection. All staff should receive training in radiation physics, biological risks, and hands-on dose-reduction techniques. Recent advancements in virtual reality simulation, augmented reality, and 3D printing now enable patient-specific rehearsal for complex endovascular procedures.47-49 While large randomized trials are lacking, these novelties allow vascular surgeons to master skills in a radiation-free and patient harm-free environment, reducing FT during actual EVAR procedures. 50 Institutions should prioritize these training tools to minimize unnecessary exposure while maintaining educational value.
Exploit Nonionizing Radiation Technologies When Feasible
State-of-the-art radiation-free technologies are transforming EVAR by enabling real-time, high-resolution 3D visualization. The FORS detect shape changes through light signal distortions, 51 whereas magnetic resonance imaging–compatible systems and electromagnetic tracking devices use magnetic fields to deliver high-fidelity intraoperative guidance.52,53 Recent clinical research proves that EVAR can be performed entirely with ultrasound guidance – combining IVUS for navigation and contrast-enhanced ultrasound for completion control – delivering excellent outcomes while eliminating radiation exposure for both patients and surgical teams. 54
Integrate Robotic and Artificial Intelligence-Driven Technologies
Robotic endovascular systems show particular promise as they enable remote control, allowing surgeon to operate behind lead shielding and potentially minimize radiation. 55 Phantom and clinical studies demonstrate reduced cannulation, procedure, and fluoroscopy durations compared with manual techniques.26,56,57 Microrobots are poised to revolutionize EVAR procedures, offering precise navigation and targeted therapy; their progress is worth monitoring closely. 58 Concurrently, artificial intelligence–enhanced fluoroscopy systems are being developed to automatically optimize endograft visualization and tracking through real-time segmentation and color enhancement, potentially decreasing radiation requirements. While preliminary results are encouraging, prospective validation is needed to confirm these technologies’ clinical benefits in EVAR cases. 59
Limitations
This systematic review has several limitations. The appreciable heterogeneity in dosimetric methods due to inconsistent dosimeter placement, shielding protocols, and reporting metrics prohibited direct comparisons between studies. Furthermore, some studies included mixed cohorts of both standard and complex EVAR, precluding a meaningful comparison between the 2 endovascular approaches. The predominance of small, single-center studies may affect generalizability, while the restriction to English-language publications may have excluded relevant data from non-Anglophone high-volume EVAR centers, potentially introducing selection bias. Finally, the exclusion of conference abstracts and presentations, while improving quality control, could have omitted pioneering technical advances presented preliminarily.
Conclusion
The present work highlights the persistent variability in occupational intraoperative radiation exposure during standard and complex EVAR interventions. Key findings underscore that main operators remain at highest risk, particularly for ocular exposure, which can approach or even exceed annual regulatory limits in large-scale centers. The adoption of advanced imaging systems and suspended shielding has demonstrated significant dose reductions, yet disparities persevere owing to procedural complexity and inconsistent adherence to best practices. As complex EVAR procedures push occupational exposure closer to regulatory limits, ongoing advancements in equipment design, dosimetric monitoring, and staff training are essential to protect endovascular operators and support staff against the long-term harmful effects of ionizing radiation.
Footnotes
Ethical Considerations
As this study did not involve human or animal subjects, formal ethics approval was not required. The authors are accountable for the accuracy and completeness of this review.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.