
Abstract
Background and Objective:
Radiofrequency ablation (RFA) is an established treatment for great saphenous vein (GSV) incompetence. However, neovascularization and residual reflux at the saphenofemoral junction (SFJ) remain concerning. Flush ablation, in which energy delivery is initiated directly after the SFJ, may improve outcomes. The objective was to compare clinical outcomes, pain, quality of life (QoL), and complications between flush and conventional standard RFA of the GSV.
Methods:
A prospective randomized comparative study was conducted on patients undergoing endovenous RFA, using flush and conventional standard ablation between January 2020 and December 2024 at a tertiary referral center. The primary endpoint was the change in pain score (Visual Analog Scale [VAS]) at 6 months. Secondary endpoints included QoL, recurrence, neovascularization, and endovenous heat-induced thrombosis (EHIT) ≥2.
Results:
A total of 602 consecutive patients were treated with RFA, divided into 2 equal groups: flush ablation (Group F, n = 301) and standard ablation (Group S, n = 301). Post-procedural pain scores were significantly lower in Group F compared with Group S (42.3 ± 6.9 vs 48.9 ± 8.0, P < .001), with a greater percentage reduction from baseline (33.1% vs 22.4%). In a median follow-up of 20 months, neovascularization occurred significantly less frequently in Group F (0.7% vs 4.0%, P = .012). Recurrence rates were low and comparable between groups (2.0% vs. 4.0%, P = .231). No deep vein thrombosis (DVT) occurred in Group F, while 1 case was reported in Group S.
Conclusion:
Flush RFA of the great saphenous vein was associated with significantly improved postoperative pain compared with conventional ablations. Lower rates of neovascularization were also observed. No increase in thrombotic or procedural complications was identified in this cohort. Given that this approach extends beyond current standard practice and considering the limited power for rare adverse events, these findings require confirmation in larger multicenter studies with longer follow-up before widespread adoption can be recommended.
Clinical Impact
Flush radiofrequency ablation represents a simple technical modification of standard endovenous therapy for great saphenous vein incompetence. By initiating ablation at the saphenofemoral junction under ultrasound guidance, this approach minimizes the residual venous stump and is associated with lower postoperative pain scores and a reduced rate of neovascularization, without an observed increase in thrombotic or procedural risk. Importantly, the absolute reduction in pain was modest, and the study was not powered for rare adverse events. As the technique can be implemented without additional equipment or cost, it offers a practical refinement of current workflows. These findings support further evaluation of a more proximal ablation strategy in larger multicenter studies to confirm its clinical benefit and long-term durability.
Keywords
Introduction
Chronic venous insufficiency due to truncal reflux is a common condition with significant socioeconomic and quality-of-life (QoL) implications. Endovenous thermal ablation techniques, particularly radiofrequency ablation (RFA), have largely replaced conventional surgery due to favorable efficacy, reduced morbidity, and faster recovery.1,2
Despite excellent occlusion rates, recurrence following RFA remains a clinical concern. Neovascularization and residual reflux at the saphenofemoral junction (SFJ) are recognized mechanisms contributing to recurrent varicosities. Conventional standard RFA typically initiates ablation several centimeters distal to the SFJ to minimize thermal injury to the common femoral vein; however, this may leave a residual stump that predisposes to neovascularization. 3
Flush ablation, in which energy delivery begins directly at the SFJ under ultrasound guidance, has been proposed as a strategy to eliminate residual reflux sources. However, evidence comparing this technique with standard ablation remains limited.4,5
The present study aimed to compare clinical outcomes, pain reduction, QoL improvement, and complication rates between flush RFA and standard RFA in patients with great saphenous vein (GSV) incompetence.
Patients and Methods
Study Design and Population
A prospective randomized study was conducted on patients treated with endovenous RFA for GSV incompetence between January 2020 and December 2024 at a tertiary referral center. Ethical approval was obtained from the Institutional Review Board (code R.22.09.1805). Written informed consent was obtained from all participants, with verbal consent permitted in rare instances in accordance with institutional policy. The study was conducted in accordance with the Declaration of Helsinki and reported in line with the Consolidated Standards of Reporting Trials (CONSORT) guidelines. 6
The diagnosis of GSV incompetence was established using duplex ultrasonography performed in the standing position, in accordance with international guidelines. Venous reflux was assessed using distal manual compression and/or the Valsalva maneuver, with pathological reflux defined as retrograde flow lasting ≥0.5 seconds.
Patients were considered eligible for endovenous RFA if duplex ultrasonography confirmed truncal GSV incompetence and demonstrated a vein diameter suitable for endovenous therapy. Diameter thresholds were defined as ≥5.0 mm in females and ≥5.5 mm in males, measured at the SFJ in the standing position. Although current guidelines do not define specific diameter thresholds for intervention, vein diameter is recognized as a factor influencing treatment selection. The 2022 European Society for Vascular Surgery (ESVS) 7 guidelines suggest ultrasound-guided foam sclerotherapy for saphenous trunks <6 mm. In this context, a pragmatic minimum diameter threshold was adopted in our study to ensure suitability for endovenous thermal ablation.
Patients with significant venous tortuosity precluding safe catheter advancement were excluded. Additional exclusion criteria included a history of deep vein thrombosis, phlebitis, prior venous surgery, lymphedema, or lipedema.
Patients were randomly allocated into 2 equal groups: Group F, undergoing flush RFA at the SFJ as demonstrated in Figure 1, and Group S, undergoing conventional RFA performed 2 cm distal to the SFJ.
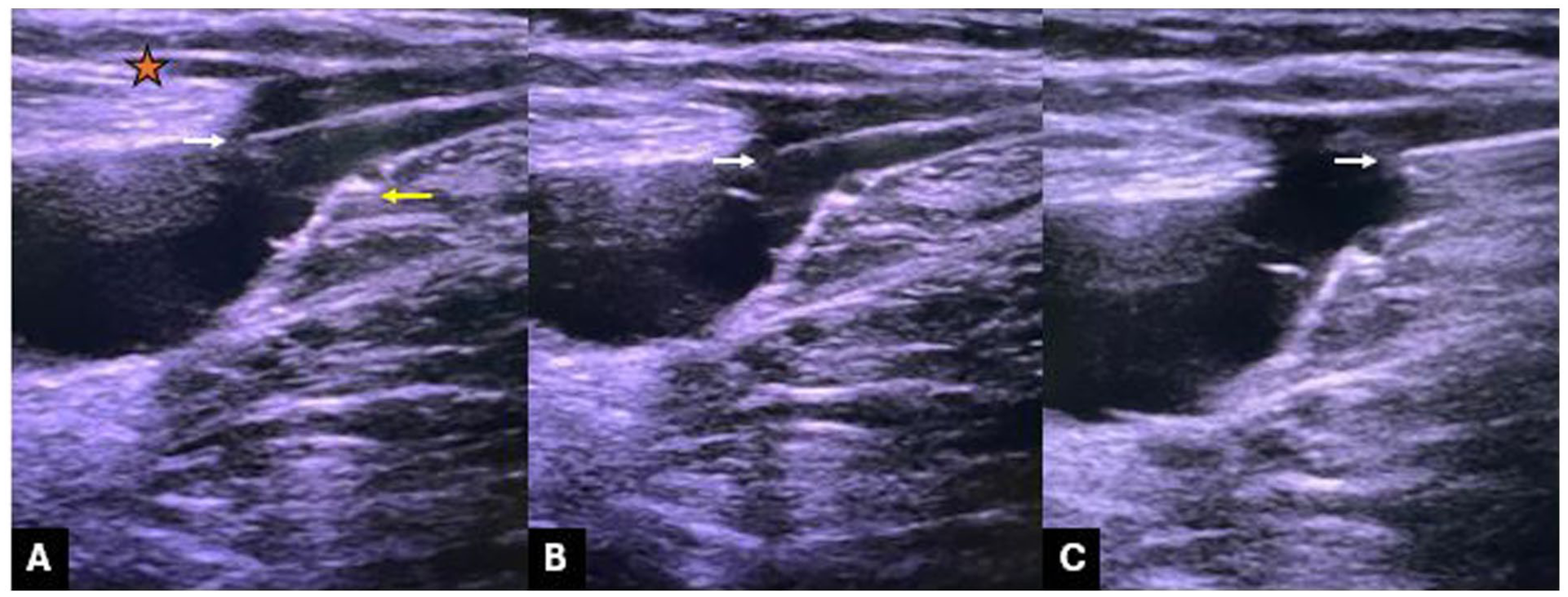
Flush radiofrequency ablation (RFA) technique of the great saphenous vein (GSV). (A) Initiation of flush ablation of the GSV immediately distal to the terminal valve under duplex ultrasound guidance. The orange star denotes the epigastric vein, the white arrow indicates the tip of the radiofrequency catheter, and the yellow arrow marks the terminal valve. (B and C) Sequential images demonstrating continuous catheter pullback during radiofrequency ablation of the GSV.
Randomization
A total of 684 patients were screened during the study period. Eighty-two patients were excluded prior to randomization due to failure to meet inclusion criteria or incomplete baseline data. The remaining 602 patients were randomized in a 1:1 allocation ratio using a computer-generated random sequence. Allocation concealment was ensured using sequentially numbered, opaque, sealed envelopes prepared by an independent investigator not involved in patient recruitment or treatment. Details are summarized in the flowchart (Figure 2).
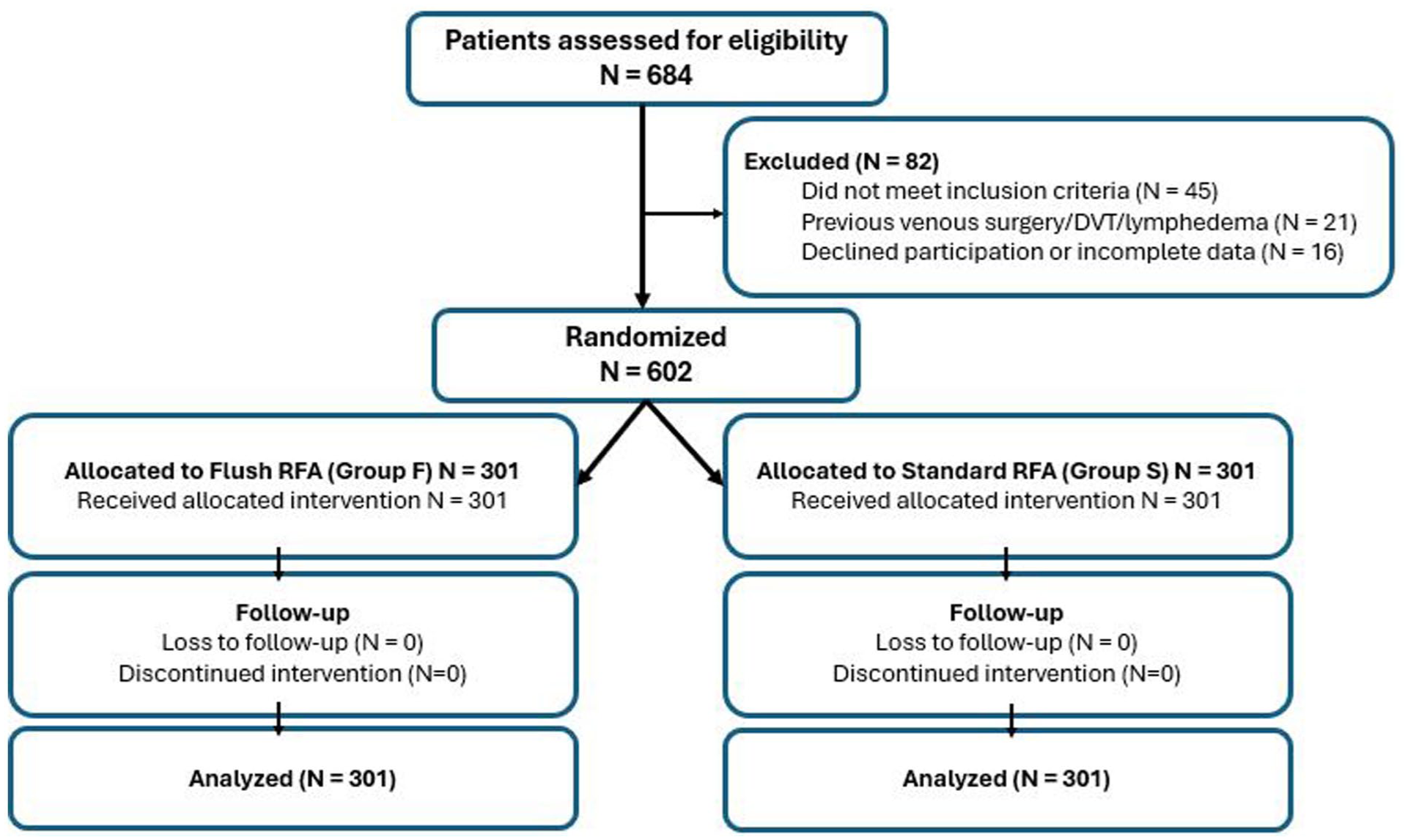
CONSORT flow diagram showing patient enrollment, randomization, allocation, follow-up, and analysis.
Randomization was carried out at the patient level, with only 1 limb per patient included in the analysis. In patients with bilateral GSV incompetence, the first treated limb was included. Treating physicians were aware of the allocated intervention, while outcome assessment was performed according to a predefined protocol. Outcome assessment was performed independently of the treating physician whenever possible.
Procedure
Diagnosis was confirmed with a duplex study, while the patient was standing by an independent radiologist using universally standardized protocols. 7 All procedures were performed under ultrasound guidance using a commercially available RFA system “Med-RF” (F-Care Systems, Antwerp, Belgium). In Group F, the ablation catheter was positioned flush at the SFJ just behind the terminal valve, and energy delivery was initiated at this level. In Group S, ablation was initiated 2 cm distal to the SFJ following conventional practice.
For tumescent anesthesia, a mixture was prepared by adding 60 mL of 8.4% sodium bicarbonate, 30 mL of 2% prilocaine, and 0.6 mg adrenaline to 1000 mL of isotonic solution at +4 °C and injected along the GSV from the introducing sheath level below the knee up to the SFJ. During ablation, radiofrequency energy was delivered using segmental thermal cycles, with the catheter heating element reaching 120 °C for approximately 20 seconds per 0.5-cm segment, in accordance with the manufacturer’s system specifications (Med-RF; F-Care Systems). This temperature reflects the catheter tip setting rather than direct tissue temperature.
Peri-procedural care was standardized for both groups with postoperative rivaroxaban 10 mg prescribed once daily in the evening for 10 days, as well as the use of venoactive drugs and a class II elastic stocking for at least 6 months.
Endpoints
The primary endpoint was the change in pain score (Visual Analog Scale [VAS]) from baseline to 6-month follow-up. Secondary endpoints included changes in QoL scores, occurrence of endovenous heat-induced thrombosis (EHIT ≥ 2), recurrence, neovascularization, and deep vein thrombosis (DVT). 7
Neovascularization was defined, in accordance with the 2022 ESVS guidelines, as the presence of newly formed tortuous vessels at the SFJ bridging previously disconnected venous segments, as confirmed by duplex ultrasound (DUS). Recurrence/recanalization was defined as the reappearance of flow within a previously ablated segment of the GSV confirmed on DUS. 7
Pain was assessed using the VAS, 8 and QoL was assessed using the Chronic Venous Disease Quality of Life Questionnaire (CIVIQ)-20 questionnaire. 9 Both were assessed at baseline (preoperative) and at 6 months post-procedure.
Follow-up Protocol
The follow-up protocol consisted of postoperative clinical examination and duplex scan at 1 week, 6 months, 12 months, and annually thereafter. Duplex scans were performed by the same radiologist working in the facility.
Statistical Analysis
Data were analyzed using IBM SPSS version 29 for Windows. Normality of the numerical data was assessed using the Kolmogorov-Smirnov test. Continuous variables were expressed as mean ± SD (standard deviation) and compared using independent t-tests. Categorical variables were expressed as numbers and percentages and analyzed using the chi-square test.
Time-to-event analyses were performed to account for variable follow-up duration. The Kaplan-Meier survival estimates were used to assess recurrence-free and neovascularization-free survival. Patients were censored at their last available follow-up. Differences between groups were assessed using the log-rank test.
To identify independent predictors of neovascularization, multivariable logistic regression analysis was performed. Variables with a P-value <.20 on univariate analysis were entered into the multivariable model. Adjusted odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. Statistical significance was set at P < .05.
Results
General Cohort
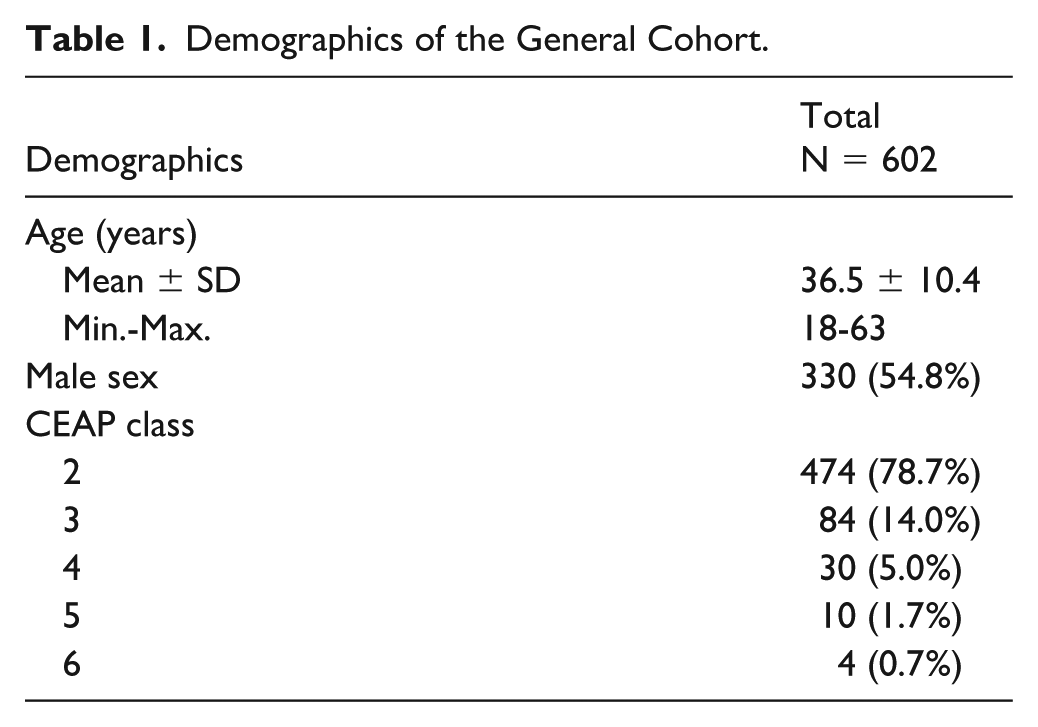
The study included 602 patients treated with endovenous RFA for GSV incompetence. The mean age of the study population was 36.5 ± 10.4 years, with 330 (54.8%) males (Tables 1 and 2). Patients were divided into 2 equal groups; Group F included patients treated with flush RFA at the SFJ (n = 301), and Group S, which included patients treated with standard RFA (n = 301). The mean diameter of the SFJ was significantly larger in Group F compared to Group S (1.14 vs 1.05 cm, P = .040). The majority of patients presented with CEAP (Clinical - Etiology - Anatomy - Pathophysiology) class C2 disease (78.7%), followed by C3 (14.0%), C4 (5.0%), C5 (1.7%), and C6 (0.7%).
Demographics of the General Cohort.
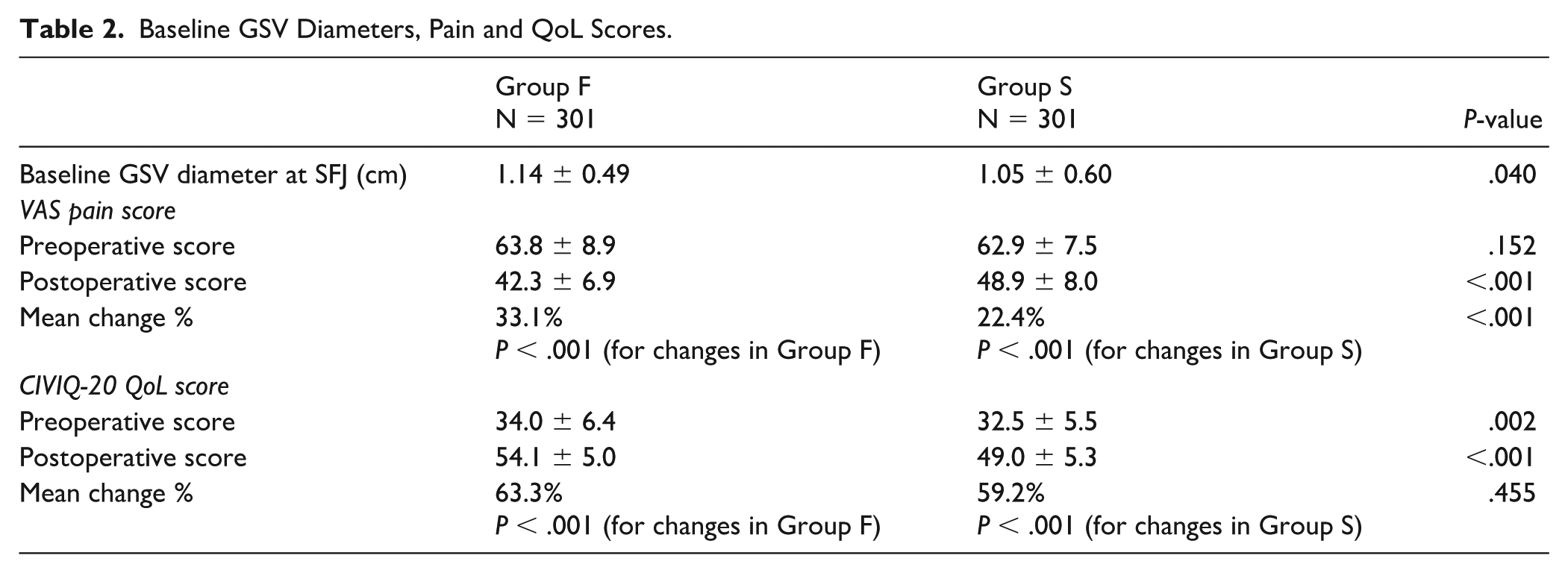
Baseline GSV Diameters, Pain and QoL Scores.
Pain
Baseline VAS of pain scores did not differ significantly between groups (P = .152). Post-procedural pain, assessed at 6 months, was significantly lower in Group F compared with Group S (42.3 ± 6.9 vs 48.9 ± 8.0, P < .001). Both groups demonstrated significant pain reduction; however, the percentage reduction was greater in Group F (33.1%) than in Group S (22.4%), P < .001 (Table 2).
Quality of Life
Group F demonstrated significantly better QoL scores both pre- and 6 months post-procedure compared with Group S (P < .001). Although both techniques resulted in statistically significant QoL improvement, the percentage change was slightly greater in Group F (63.3%) compared with Group S (59.2%), P = .455 (Table 2).
Endovenous Heat-Induced Thrombosis
No cases with EHIT ≥2 were reported for both groups in the postoperative period and at 6 months (Table 2).
Follow-up Outcomes
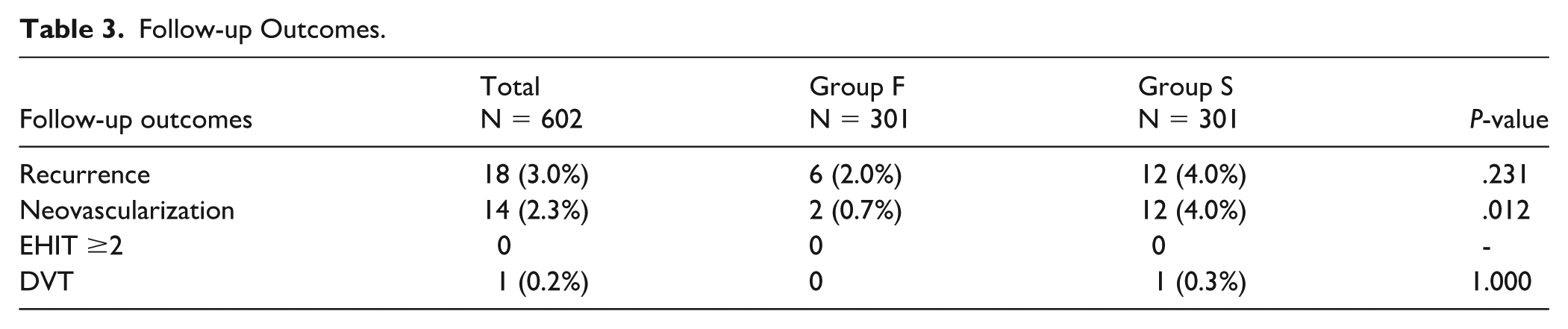
Over a median follow-up of 20 months (interquartile range [IQR] = 12-36 m), recurrence rates were low and comparable between groups (2.0% in Group F vs 4.0% in Group S, P = .231). Neovascularization occurred significantly less frequently in Group F (0.7%) compared with Group S (4.0%), P = .012.
No cases of DVT were reported in Group F, while 1 case (0.3%) occurred in Group S, discovered during regular follow-up, with no significant difference between groups. This case was evaluated with duplex ultrasonography and did not demonstrate thrombus extension from the treated GSV into the common femoral vein; therefore, it did not meet criteria for EHIT and was considered a separate thrombotic event (Table 3).
Follow-up Outcomes.
The Kaplan-Meier analysis demonstrated no significant difference in recurrence-free survival between the 2 groups (log-rank P = .144) (Figure 3). At 36 months, recurrence-free survival was 97.8% in the flush ablation group and 95.2% in the standard ablation group.
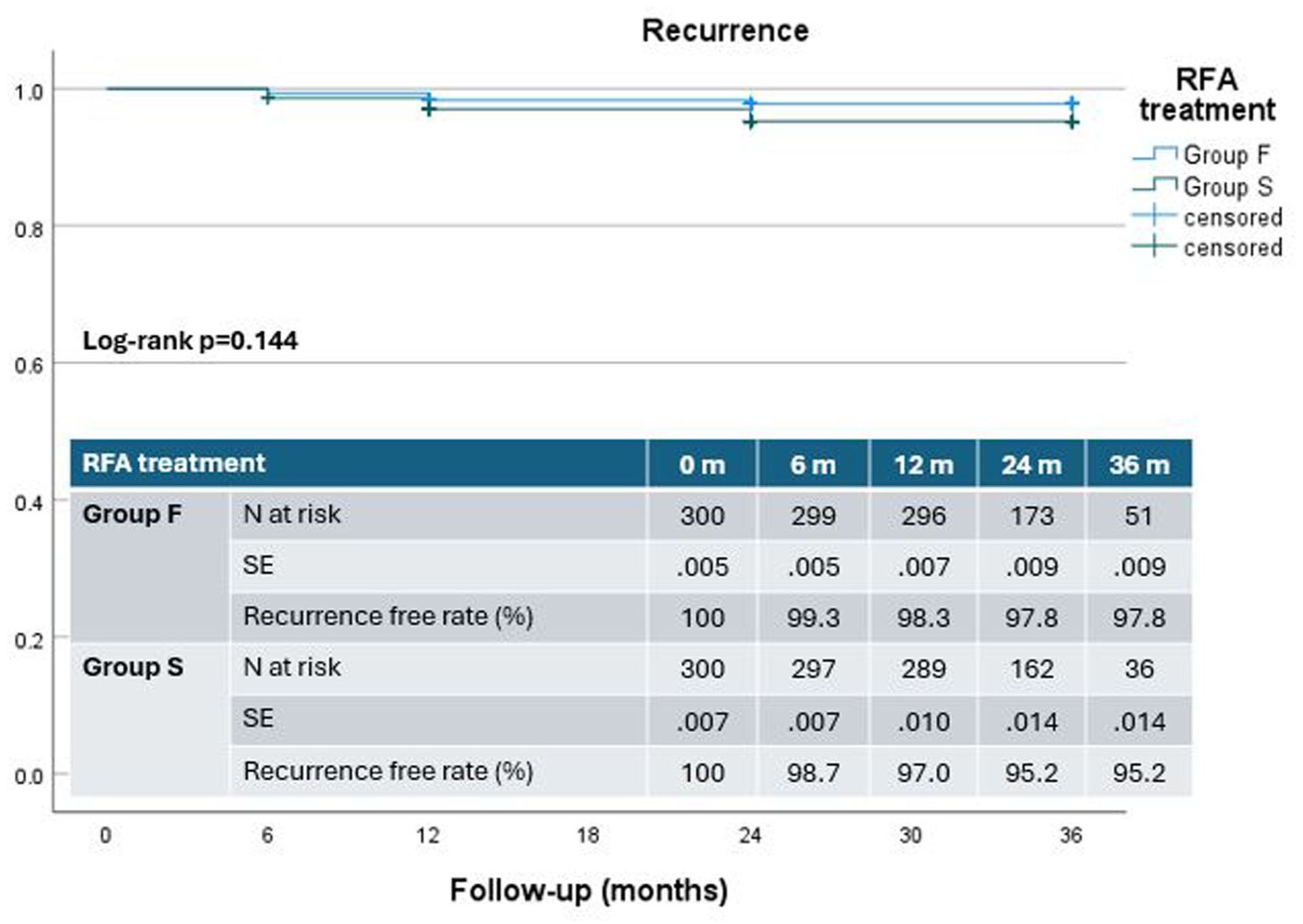
Kaplan-Meier analysis of recurrence-free survival following radiofrequency ablation.
In contrast, neovascularization-free survival was significantly higher in the flush ablation group compared with the standard ablation group (log-rank P = .006) (Figure 4). At 3 months, neovascularization-free survival was 99.1% in Group F and 95.0% in Group S.
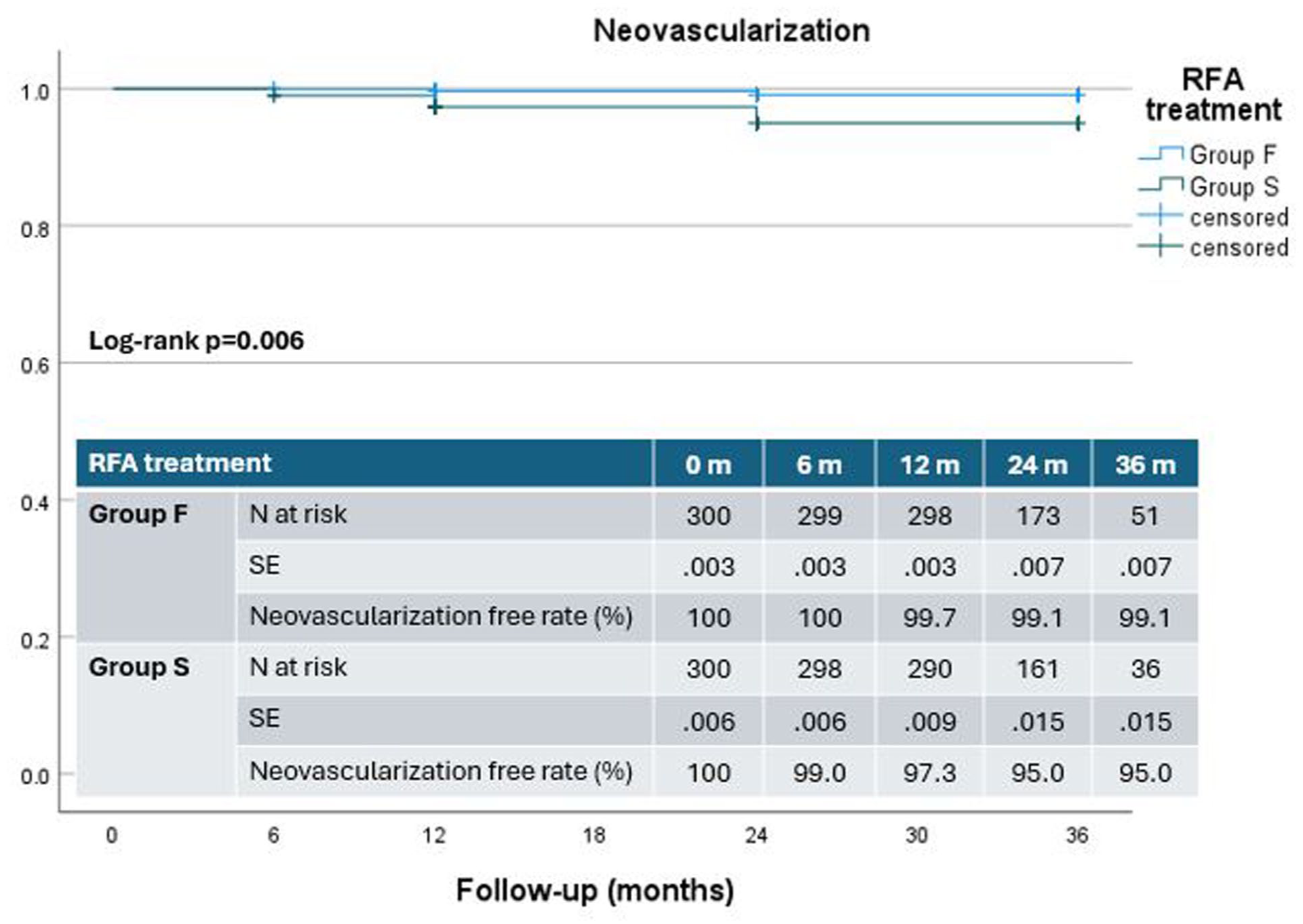
Kaplan-Meier analysis of neovascularization-free survival following radiofrequency ablation.
Multivariate Analysis
To identify factors associated with neovascularization, univariate and multivariable analyses were performed (Table 4). On multivariable analysis, conventional standard RFA was independently associated with a significantly higher risk of neovascularization (OR = 6.3, 95% CI = 1.38-28.77, P = .017).
Multivariate Analysis of the Factors Associated With Neovascularization.
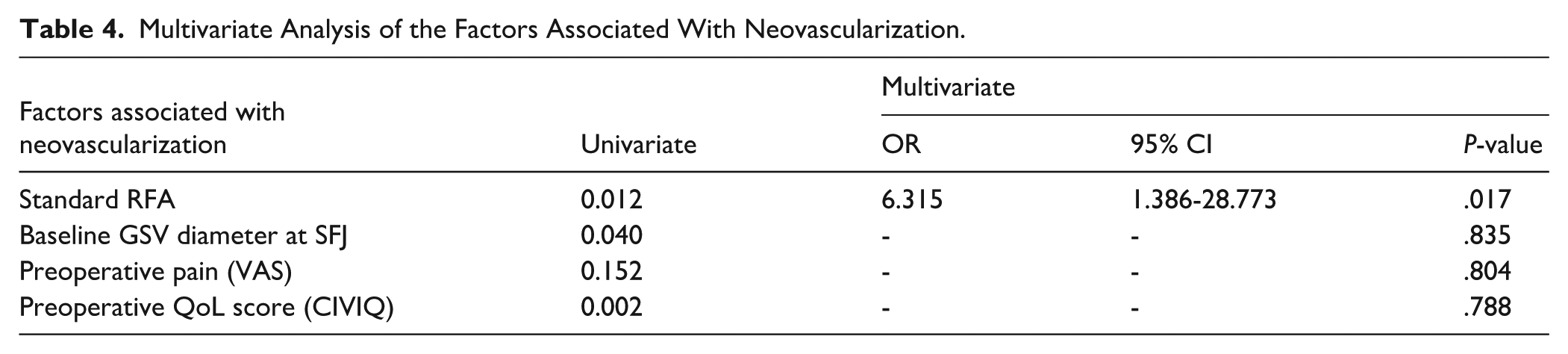
In contrast, baseline GSV diameter, preoperative pain, and baseline QoL scores were not significant predictors. These findings suggest that the observed difference in neovascularization is primarily related to the procedural technique rather than baseline patient characteristics.
Discussion
This prospective randomized study demonstrates that flush RFA of the GSV is associated with significantly improved pain outcomes and a lower incidence of neovascularization compared with conventional ablation. Importantly, within the limits of the present study, no increase in thrombotic or procedural complications was observed. However, these findings should be interpreted with caution, as flush ablation represents a modification beyond the current instructions for use (IFU), and robust evidence is required before broad clinical adoption can be recommended.
Neovascularization following treatment of the SFJ remains a well-recognized mechanism of varicose vein recurrence. 10 Conventional RFA techniques intentionally initiate ablation several centimeters distal to the SFJ to minimize thermal injury to the common femoral vein; however, this approach may leave a residual proximal stump that serves as a stimulus for angiogenesis and recurrent reflux. The significantly lower neovascularization rate observed in the flush ablation group supports the hypothesis that complete elimination of the proximal reflux source reduces angiogenic signaling and subsequent varicose vein formation.4,11 Importantly, this observation is further supported by multivariable analysis, which identified conventional standard RFA as an independent predictor of neovascularization, with an approximately 6-fold increase in odds compared with flush ablation. Notably, baseline variables such as GSV diameter, preoperative pain, and QoL were not significant predictors. This suggests that the reduction in neovascularization is primarily attributable to the technical approach itself rather than underlying patient characteristics, reinforcing the mechanistic rationale of more complete proximal reflux elimination.
Previous studies have suggested that surgical high ligation of the SFJ may itself contribute to or accelerate groin neovascularization, likely due to disruption of normal venous anatomy and stimulation of angiogenic pathways. This phenomenon has been described as a potential mechanism underlying recurrent varicose veins following open surgery. In contrast, endovenous approaches avoid surgical dissection at the junction and may therefore reduce this angiogenic stimulus. The lower rate of neovascularization observed in the flush ablation group in the present study may, in part, be explained by this less disruptive approach to the SFJ.7,12
A key finding of this study is the significantly lower pain scores observed in the flush ablation group. Importantly, pain was assessed at 6 months, reflecting sustained symptom burden rather than early post-procedural or inflammatory pain. This suggests that the observed difference is primarily driven by hemodynamic factors rather than procedural extent. Flush ablation enables more complete elimination of reflux at the SFJ, thereby reducing residual venous hypertension within the treated limb. In contrast, conventional ablation leaves a proximal stump that may permit persistent pressure transmission or residual reflux into tributaries, contributing to ongoing venous congestion and symptoms. This supports the concept that long-term pain outcomes following endovenous interventions are closely linked to the completeness of reflux elimination. Importantly, despite the more proximal ablation, no increase in EHIT ≥ 2 or other complications was observed in our cohort, suggesting that the technique does not result in excessive tissue injury and supporting the procedural feasibility of flush ablation when performed under careful ultrasound guidance. 13 The single DVT observed in the standard ablation group was not related to EHIT progression, supporting the absence of increased thrombotic risk associated with flush ablation at the SFJ.
The observed between-group difference in VAS scores (~6.6 points on a 100-point scale) is below commonly reported minimal clinically important difference (MCID) thresholds (~12 mm), suggesting that the absolute difference may be modest at an individual patient level. However, the flush ablation group demonstrated a substantially greater relative reduction in pain from baseline (33.1% vs 22.4%), indicating a more pronounced overall treatment effect. Furthermore, MCID thresholds are primarily designed to assess within-patient change rather than between-group differences and may therefore underestimate clinically relevant effects in comparative studies.14,15
Quality-of-life outcomes improved significantly in both groups, reflecting the established benefits of endovenous ablation in chronic venous insufficiency secondary to GSV incompetence. Although absolute QoL scores were higher in the flush ablation group, the percentage improvement was comparable between techniques, suggesting that both approaches effectively address symptomatic burden, with flush ablation providing incremental benefits primarily in pain reduction and anatomical durability.
Importantly, recurrence rates were low and did not differ significantly between groups over a median follow-up of 20 months. This may reflect the overall high technical success rate of RFA and the relatively short-to-mid-term follow-up period, during which anatomical failure may precede clinically apparent recurrence. Longer-term follow-up will be required to determine whether the observed reduction in neovascularization translates into sustained reductions in late recurrence.
Collectively, these findings suggest that flush RFA may represent an effective modification of the conventional standard RFA technique, offering improved postoperative comfort and favorable anatomical outcomes without an observed increase in complications in this cohort. The present findings should therefore be considered hypothesis-generating rather than definitive. Although flush ablation has been increasingly explored in recent studies, including reports on flush endovenous thermal techniques with comparable short-term safety profiles, the current evidence remains limited. Larger, multicenter studies with longer follow-up are required to confirm the safety and durability of this approach before it can be widely recommended in routine clinical practice.
Limitations of the Study
This study has several limitations. First, although randomized, it was conducted at a single tertiary referral center, which may limit generalizability to other practice settings. A formal a priori sample size calculation was not performed, which may reduce statistical power for detecting differences in rare outcomes such as thrombotic events. Second, patients were not blinded to the intervention, which may introduce bias in patient-reported outcomes such as pain and QoL. Blinding of treating physicians was not feasible due to the nature of the intervention, introducing potential performance bias; however, outcome assessment followed a standardized protocol. Third, only 1 limb per patient was included in the analysis, which strengthens internal validity but may underestimate real-world bilateral disease patterns. Fourth, although the median follow-up of 20 months is adequate for assessing early recurrence and neovascularization, longer-term follow-up is required to confirm durability beyond 3 to 5 years.
In addition, adjunctive treatments such as sclerotherapy or phlebectomy for residual varicosities were not systematically recorded or standardized, representing a potential confounding factor influencing both recurrence and patient-reported outcomes. Important prognostic variables, including body mass index, treated GSV segment length, and the presence of concomitant below-knee or tributary insufficiency, were not systematically captured, limiting risk stratification and external validity. Operator experience and potential learning curve effects were also not formally assessed and may have influenced procedural performance and outcomes. Furthermore, although CEAP clinical class distribution was reported descriptively, it was not incorporated into stratified outcome analyses. Finally, the routine use of postoperative rivaroxaban may have contributed to the low incidence of thrombotic events and may limit generalizability to centers with different thromboprophylaxis protocols.
Conclusion
Flush RFA of the GSV was associated with significantly improved postoperative pain compared with conventional ablations. Lower rates of neovascularization were also observed. No increase in thrombotic or procedural complications was identified in this cohort. Given that this approach extends beyond current standard practice and considering the limited power for rare adverse events, these findings require confirmation in larger multicenter studies with longer follow-up before widespread adoption can be recommended.
Footnotes
Ethical Considerations
Ethical approval was obtained from the Institutional Review Board (code R.22.09.1805). Written informed consent was obtained from all participants, with verbal consent permitted in selected cases in accordance with institutional policy.
Author Contributions
MS and AA conceived and designed the study. MS, KAM, MS, and ME were involved in patient recruitment, data collection, and clinical procedures. RS contributed to data organization and follow-up coordination. AA performed the statistical analysis and drafted the manuscript. All authors critically reviewed the manuscript for important intellectual content, approved the final version for publication, and agreed to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data sets generated and analyzed during the current study are not publicly available due to institutional regulations and patient confidentiality requirements. De-identified data supporting the findings of this study may be made available from the corresponding author upon reasonable request and following approval by the relevant institutional review board.