
Abstract
Context:
Some living kidney donors report lost income during recovery from surgery. Little is known about whether concern for living donor’s lost income affects the decision to undergo donation evaluation and the willingness of transplant candidates to discuss living kidney donation (LKD) with others.
Objective:
To examine whether transplant patients were told by potential donors about lost income concerns and whether patients chose not to discuss LKD with others due to lost income concerns.
Design, Setting, and Patients:
Kidney transplant patients (185 wait-listed candidates, 171 deceased donor recipients, and 100 live donor recipients) at 2 centers completed a questionnaire to assess whether concern about donor’s lost income was a consideration in discussion about LKD with others.
Results:
One-third (32%) were told by a family member/friend that they were willing to donate but were concerned about potential lost income. The majority of those who expressed financial concern (64%) did not initiate donation evaluation. Many patients (42%) chose not to discuss living donation with a family member/friend due to concern about the impact of lost income on the donor. In the multivariable model, lower annual household income was the only statistically significant predictor of both having a potential donor expressing lost income concern and choosing not to talk to someone because of lost income concern.
Conclusion:
Findings from the current study underscore how concern about income loss for living donors may affect decision-making by both transplant candidates and potential donors.
Introduction
For those with advanced-stage kidney disease who are eligible for transplantation, live donor kidney transplantation (LDKT) is more likely to yield longer graft and patient survival than deceased donor kidney transplantation (DDKT) or dialysis. 1 –3 Therefore, patients approved for transplantation are strongly advised to discuss possible living kidney donation (LKD) with family members and friends. This is a challenging task for many patients, who may be concerned about altering their relationship with others, uncertain about how to ask others to consider donation, and worried about the inconvenience and the possibility of adverse health outcomes for the donor. 4 –7
Recently, the transplant community has turned its attention to the potential role of financial disincentives in LKD rates. For instance, the current decade-long decline in LKD rates in the United States coincided with a downturn in the economy and an increase in unemployment rates, thus contributing to speculation that the potential indirect costs of donation may deter patients from proactively pursuing LDKT and potential donors from initiating evaluation. 8,9 Although costs for donation are largely covered by the recipient’s health insurance, concerns about indirect costs are not unfounded. Recent studies have shown that many living kidney donors report lost wages or income directly attributable to donation, both before and after donation, and this monetary loss may represent a significant hardship for some donors and their families. 10 –13
The degree to which the concern for donor’s lost income affects the decision of others to undergo donation evaluation and the willingness of transplant candidates to discuss LKD with others is largely unknown. Therefore, we sought to examine whether transplant patients were told by potential donors about lost income concerns and whether patients chose not to discuss LKD with others due to lost income concerns. We hypothesized that transplant candidates and DDKT recipients and patients with lower household income would be less likely than LDKT recipients and patients with higher household income, respectively, to talk to others about donation due to lost income concerns.
Methods
We developed a brief questionnaire that asked patients about their transplant status (waiting list, DDKT recipient, and LDKT recipient), age, sex, race/ethnicity, and household income. Additionally, we asked: Did anyone tell you that they wanted to be a living kidney donor but could not afford to take so much time off from work because of lost wages or income? (yes/no) If a “yes” response was given, we asked: Did this person go through with the donor evaluation? (yes/no) Finally, we asked: Was there someone you chose not to talk to about LKD because you were concerned about the impact that lost wages or income would have on them or their family? (yes/no)
Patients were recruited to complete the questionnaire either by mail or during an outpatient clinic appointment at the Beth Israel Deaconess Medical Center (BIDMC) in Boston, Massachusetts, and the Medical University of South Carolina (MUSC) in Charleston, South Carolina. At BIDMC, an introductory letter and the questionnaire were sent to all active wait-listed kidney transplant patients and all surviving DDKT and LDKT recipients in the past 4 years. At MUSC, all wait-listed and transplant recipients attending a scheduled outpatient clinic appointment during 3 consecutive months were approached for the study and asked to complete the questionnaire. Study procedures were approved by the BIDMC Committee on Clinical Investigations and the institutional review board of MUSC.
PASW 17.0 (SPSS, Inc, Chicago, Illinois) was used for data entry and analysis. Data are presented as the number and percentage of patients with specific item responses. The MUSC had a higher percentage of black participants than the BIDMC (54% vs 17%, P < .001); however, there were no other statistically significant demographic differences between the 2 centers, and thus, survey responses were combined. Chi-square tests were used to examine the differences between wait-listed patients, DDKT recipients, and LDKT recipients, as well as for response differences by age group, sex, race, and household income. Fisher exact test was used if cell sizes did not meet the requirements of χ2 tests. All variables were included in a stepwise logistic regression analysis to identify demographic predictors of “yes” responses to the 2 primary survey questions.
Results
Patient Characteristics
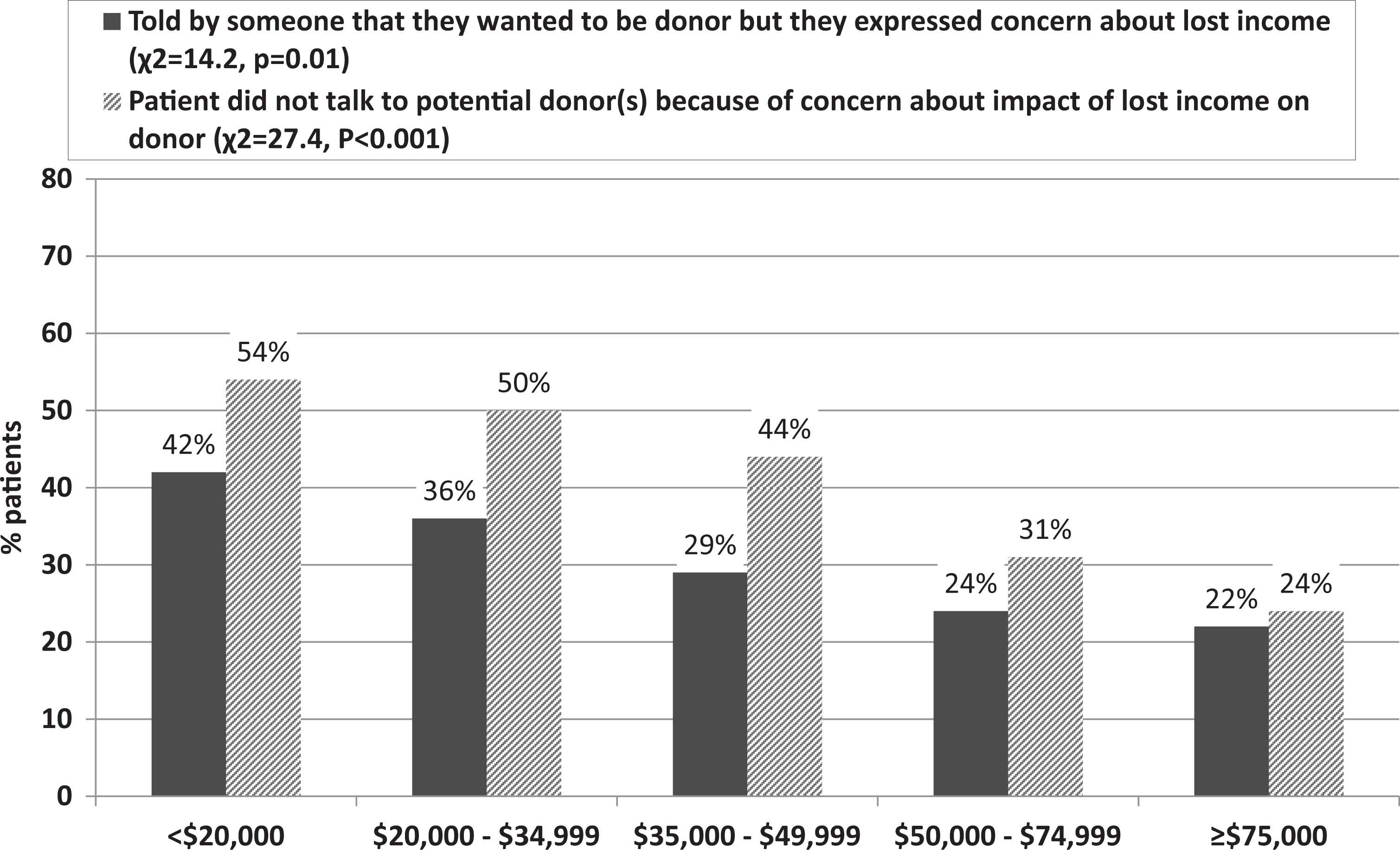
A total of 456 patients completed the survey (329 at BIDMC and 127 at MUSC), which reflects an overall participation rate of 59%. Participation rates were the highest for LDKT recipients (78%) and DDKT recipients (69%) than for wait-listed candidates (48%). Table 1 summarizes demographic characteristics of wait-listed patients, DDKT recipients, and LDKT recipients.
Sample Characteristics.
a Total n < 456 due to missing data.
Compared to their counterparts, DDKT recipients were older (P < .001) and more likely to be of minority race (P < .001), whereas LDKT recipients were more likely to have higher household income (P = .02).
Concern for Donor’s Lost Income
One-third (32%, n = 146) of the entire sample reported being told by a family member or a friend that they were willing to donate but were concerned about the potential lost income. The majority of these potential donors who expressed financial concern (64%, n = 93 of the 146) did not initiate donation evaluation. Forty-two percent (n = 190) of the patients chose not to discuss living donation with at least 1 person due to concerns about the impact of lost income on the donor or their family. Finally, 21% (n = 97) had affirmative answers to both questions, that is, they had a potential donor expressing concern about lost wages and chose not to talk to anyone about donation due to lost income concerns.
Associations Between Concern for Lost Income and Demographic Characteristics
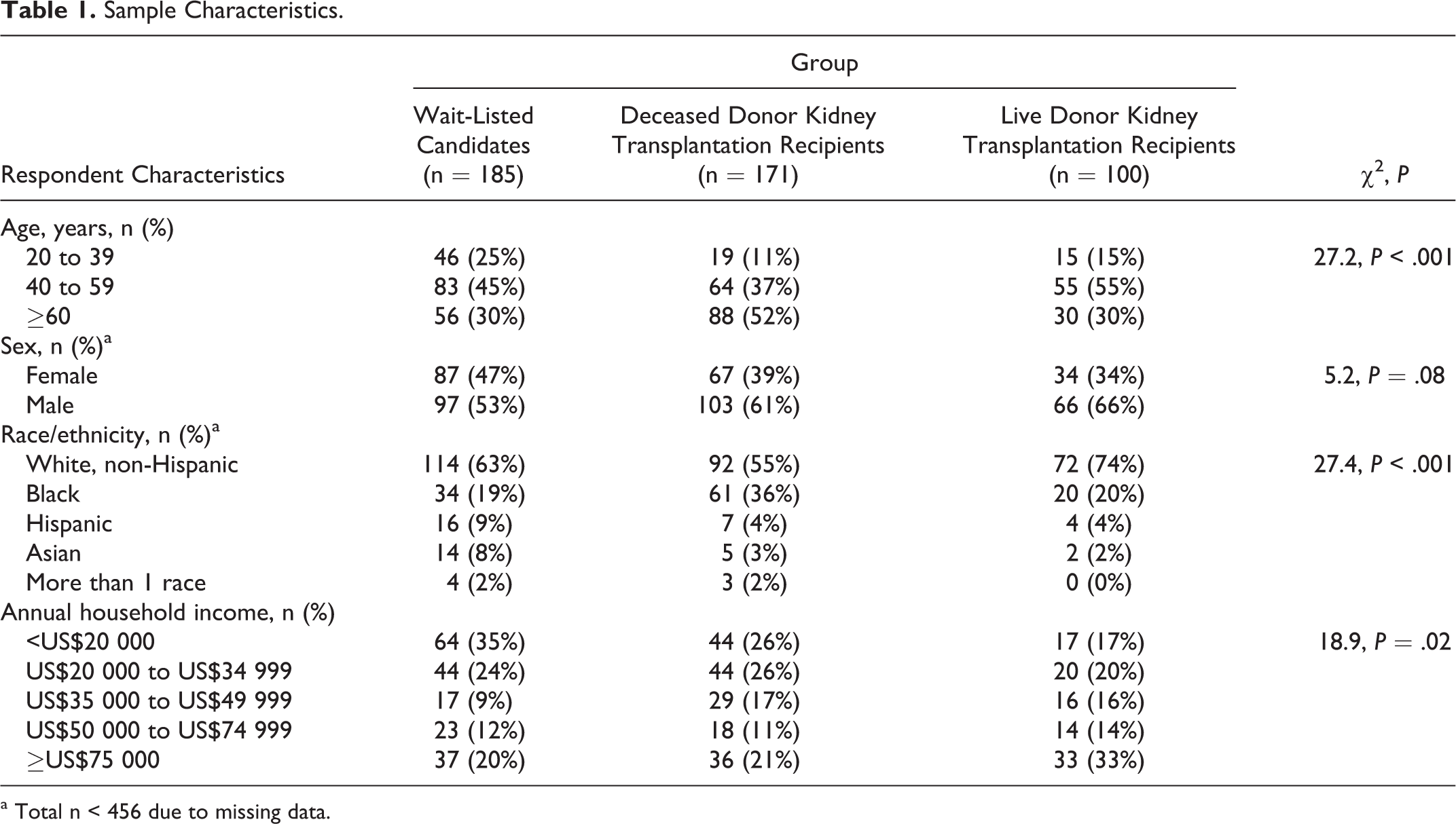
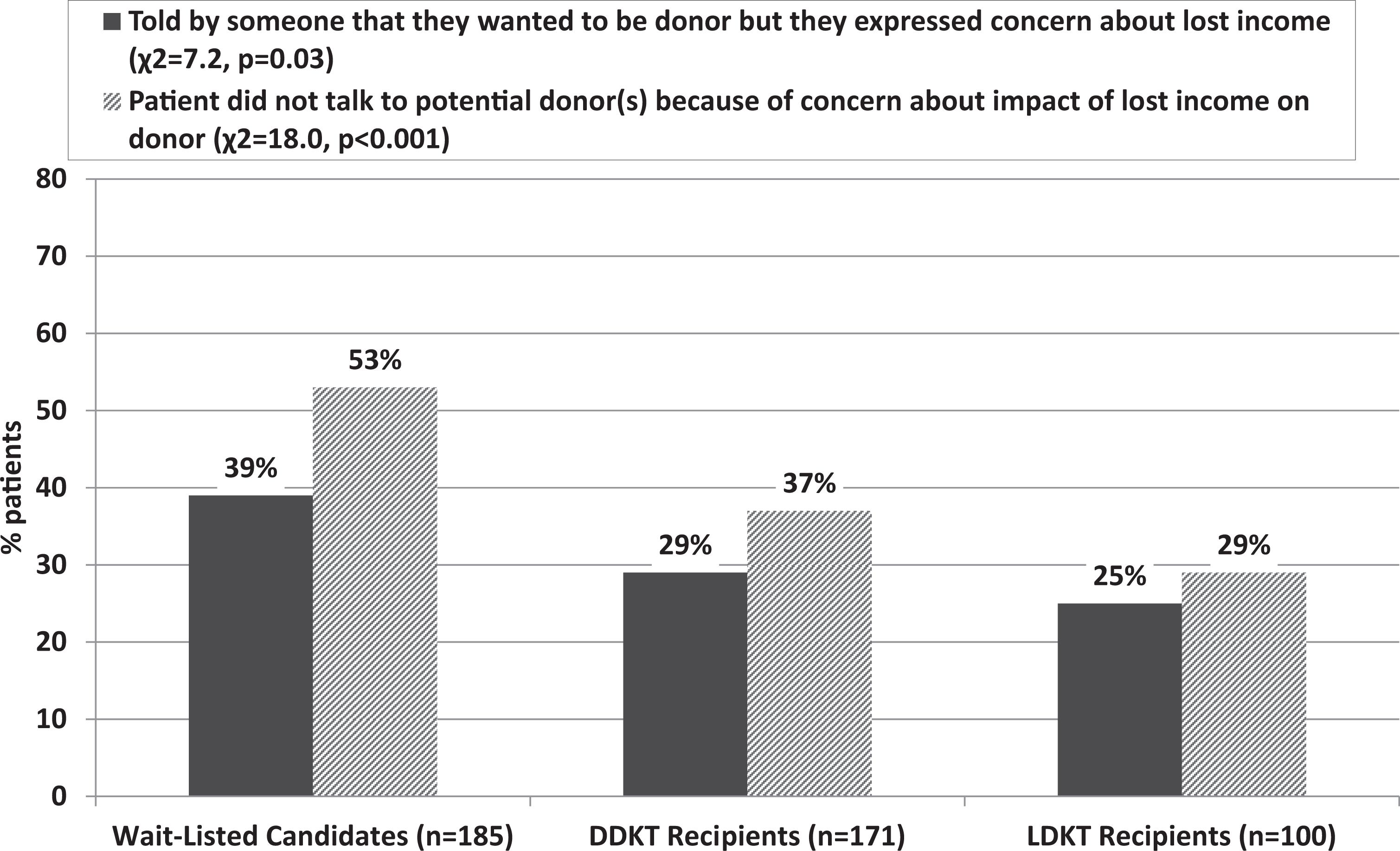
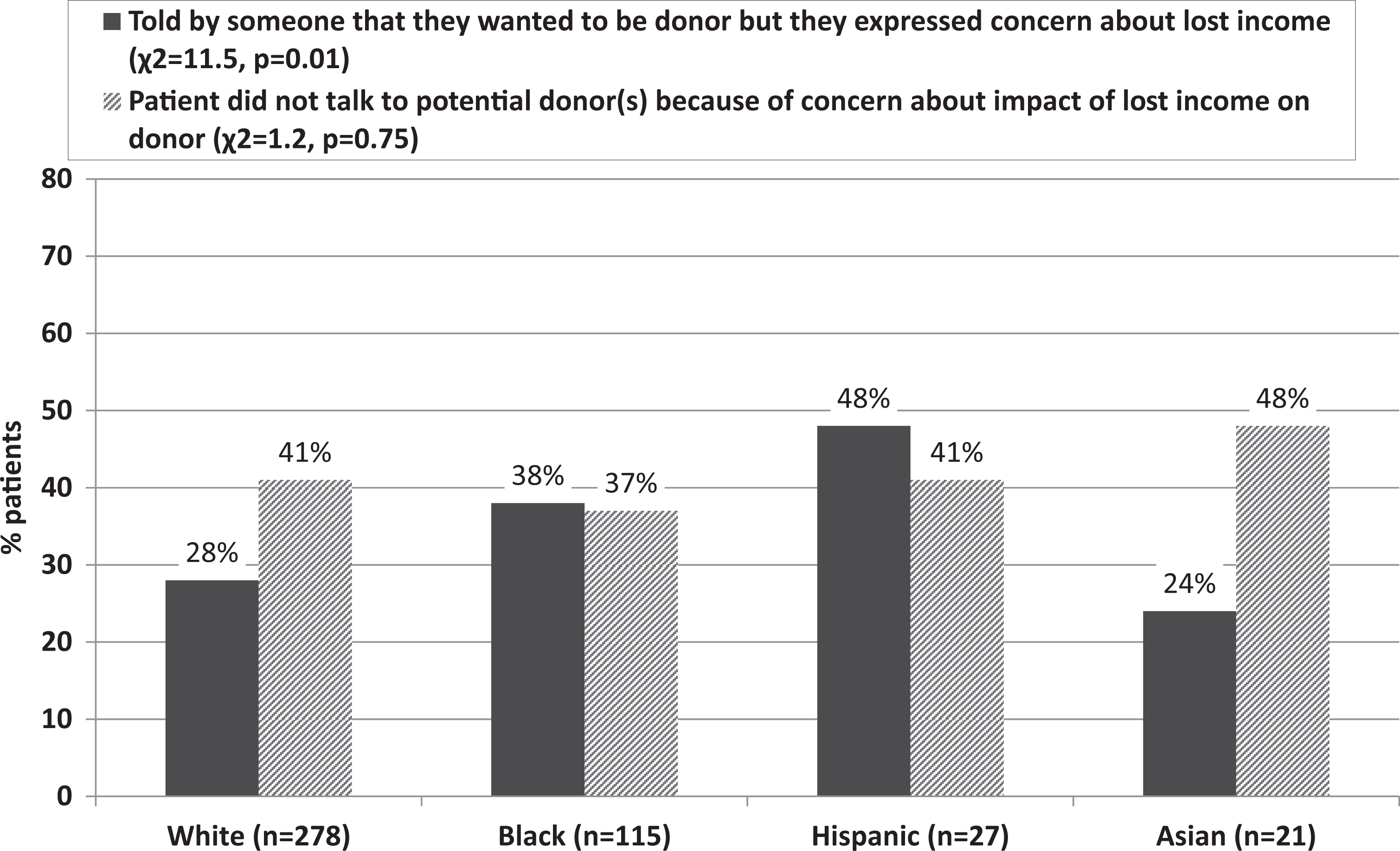
Wait-listed candidates (Figure 1; P = .03), black and Hispanic patients (Figure 2; P = .01), and patients with lower annual household income (Figure 3; P = .01) were most likely to have had a potential willing donor expressing concern about lost income due to the time away from work. Wait-listed candidates (Figure 1; P < .001) and patients with lower household income (Figure 3; P < .001) were also most likely to have chosen not to talk to others about living donation due to financial concerns of the potential donor or their family. Age and gender were not significantly associated with concerns about lost income for living donors (P > .05). In the subsequent multivariable models, lower annual household income was the only statistically significant variable in both models (potential donor expressed lost income concern: model χ2 = 46.4, P < .001; income χ2 = 5.9, P = .03; patient did not talk to anyone because of lost income concern: model χ2 = 57.7, P < .001; income χ2 = 25.2, P < .001).
Relationship between respondent type and concern for lost income after living kidney donation (LKD; n = 456).
Relationship between race/ethnicity and concern for lost income after LKD (n = 456).
Relationship between annual household income of transplant patient and concern for lost income after LKD (n = 456).
Discussion
Many living kidney donors incur both direct and indirect costs, including lost wages or income, associated with the donation evaluation process and/or recovery from surgery. 9 –13 For potential donors with sufficient financial resources, this loss of income may have a negligible impact on their decision to pursue LKD. 4,7,14 However, for those in low-wage jobs or without paid medical, vacation, or short-term disability benefits, it is possible to lose the equivalent of 1 month’s wages or income following donation. 10,11,15 Findings of the current study underscore how concerns about such income loss for living donors may affect decision-making by both transplant candidates and potential donors.
Patients with higher annual household income were less likely to report lost income concern as a barrier to potential LKD. For instance, only 24% of those with an annual income exceeding US$75 000 chose not to talk to someone about donation due to lost income concerns, compared to more than half (54%) of the patients with an annual income less than US$20 000. It is clear that this type of financial concern is more salient for lower-income patients, which may deter them from proactively pursuing LDKT. Although most of the direct costs associated with LKD in the United States are covered by the recipient’s insurance and financial assistance programs are available to those who meet financial eligibility criteria, 16 lost income for the donor is not covered and represents a substantial financial consequence for some. Transplant recipients are legally and ethically permitted to reimburse donors for lost wages, yet those with lower household income are less likely to have the resources to offset donation costs. Given the finding that most transplant recipients have moderate household incomes similar to that of their donors, 17 lower-income patients may be less likely to pursue LDKT if they are concerned about economic hardship of their donors and unable to provide assistance to ease their financial burden.
Whether concern about donor’s lost income directly impacts the likelihood of receiving LDKT could not be examined in this cross-sectional study, we found that LDKT recipients had higher annual household income than DDKT recipients and those still on the waiting list. Additionally, two-thirds of the potential donors who expressed financial concern to the transplant candidate reportedly did not initiate LKD evaluation. Although there may be other factors contributing to the decision not to pursue LKD, the finding that these potential donors discussed the financial concern directly with the transplant candidate suggests that it was a prominent consideration. It is possible, of course, that there are many additional family members or friends who consider LKD and dismiss it due to financial concerns but never discuss it with the transplant candidate. Importantly, in their study of transplant candidates, Reese et al 14 found that lower-income patients were less likely to have a potential living donor contact the transplant center for evaluation. Although the true LKD potential that is lost due to limited household income and financial concern is unknown, findings from these studies strongly suggest potential for income disparity in LDKT, and this warrants further investigation. Moreover, educational strategies and policies should be developed to ensure that lower-income patients are not priced out of this most optimal transplant option.
Although the National Living Donor Assistance Center in the United States provides travel and lodging reimbursement to donors when both the donor and recipient meet financial eligibility criteria, legislation authorizing this program specifically prohibits, in part or in whole, reimbursement of a living donor’s lost wages. 16,18 Numerous studies highlight favorable attitudes toward the payment of donor lost wages by the general public, health professionals, and adults with chronic kidney disease, 19 –24 and several countries provide reimbursement for lost income due to donation. 9,25 Achieving financial neutrality for living donors in the United States appears to be at a critical juncture and may mitigate both the decline in LKD rates and the potential disparity in LDKT based on financial impact concerns for those who donate. 9,26 –28
Our findings have led us to evaluate how much information and guidance the transplant candidates receive about the potential financial impact of LKD on living donors, the financial resources available to living donors, and how best to discuss financial issues with potential donors. In our 2 programs, the transplant candidates are advised that LDKT is their best treatment option, encouraged to talk to others about LKD, and provided with printed materials explaining that the majority of costs for donor evaluation, surgery, hospitalization, and follow-up care is covered by the recipient’s insurance. However, our data suggest that we should be more proactive in educating patients, particularly those with lower annual household income, about resources that may be available to offset concern for donor lost wages as a barrier to LDKT. A summary of typical direct and indirect donation costs, employer-based benefits for donors (eg, donation-specific policies, short-term disability), organizations that provide financial assistance to those meeting eligibility criteria, and strategies for fundraising may help patients understand the possible financial impact of LKD and facilitate discussion with potential donors. Transplant candidates who are provided with a summary of financial resources available to donors may be more likely to ask family members and friends to consider donation. It is noteworthy that a Living Donation Financial Toolkit encompassing these financial considerations that could be disseminated to patients, potential donors, and transplant programs was a primary recommendation from the 2015 Consensus Conference on Best Practices in Living Kidney Donation and it is currently under development.9,18 Should such a toolkit be developed, it would provide an opportunity to study whether such financial education and counseling increase the likelihood of LDKT, particularly in lower-income patients.
Noteworthy strengths of this study are its moderate sample size, reasonable response rate for survey research, data collection at 2 transplant centers, the inclusion of patients who received a transplant and those still waiting, and the focus on concerns about donor lost income (vs general financial concerns). However, there are several limitations that must be acknowledged and considered in interpreting the study findings. Surveys asking respondents to reflect on past experiences are prone to response and recall bias. Those who responded to the survey may be more (or less) likely to have thought about lost income in the context of living donation and to even have had potential donors within their social network. Importantly, this was a cross-sectional study and causal inferences about the relationship between lost income concerns and subsequent receipt of a LDKT cannot be made. Future prospective research is necessary to characterize the degree to which such financial concerns directly impact LDKT rates. Although we recruited participants from 2 diverse programs, it is unknown whether other transplant programs with different patient demographics and in different regions of the United States would find results similar to ours. Also, we focused exclusively on the transplant patient’s experience and did not survey potential or former living donors about lost income concerns. It is possible that the pool of potential living donors who have concerns about lost income is much larger than what was expressed directly to the patient. It is also possible that some potential donors did not want to pursue LKD for other reasons but viewed concern about lost wages as a reason that may be more acceptable and easier to discuss with the patient. Finally, we did not assess how many potential donors were available to the patient and whether financial concerns were specific to certain types of potential donors (eg, related, unrelated, young, old).
In conclusion, findings from this study suggest that concern about lost income is likely a barrier to LDKT for some patients and to LKD for some potential donors. More refined and robust examination of the relationship between these financial concerns and the eventual receipt of LDKT is warranted.
Footnotes
Authors’ Note
This content is solely the responsibility of the authors and does not necessarily represent the official views of the NIDDK or the National Institutes of Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Award No. R01DK085185 and R01DK098727 from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). The preparation of this manuscript was also supported, in part, by the Julie Henry Research Fund and the Center for Transplant Outcomes and Quality Improvement, The Transplant Institute, Beth Israel Deaconess Medical Center, Boston, MA.