
Abstract
Context:
Anticoagulation therapy is common in thoracic transplant recipients. Direct oral anticoagulants (DOACs) are alternatives to warfarin therapy, but characterization of their use in solid organ transplant is absent.
Objective:
The primary objective of this study was to describe a thoracic transplant patient population initiated on DOAC therapy. Secondary objectives were to assess adverse reactions, venous thromboembolism (VTE) recurrence, and drug–drug interactions during DOAC therapy.
Study Design:
Single-center retrospective cohort study.
Setting:
A tertiary care medical center including inpatient hospitalization and outpatient transplant clinic visits.
Patients:
Thoracic transplant recipients who were initiated on DOACs between May 1, 2011, and March 1, 2015, at the University of Pittsburgh Medical Center were included.
Results:
A total of 37 patients were included in the analysis. A majority of the patients were lung transplant recipients (86.4%) with a median age of 60.7 years. Twenty-eight patients had a history of VTE. The primary indication for DOAC initiation was VTE (86.5%). Rivaroxaban (78.4%) was the most commonly utilized agent. Dose reductions for major drug interactions (37.8%), renal insufficiency (10.8%), or both (8.1%) occurred within the study. Two patients had breakthrough VTE during DOAC therapy. Eight bleeding events were reported in the cohort, one of which was considered a major bleed. There was no difference in the incidence of bleeding in patients with drug–drug interactions and without drug–drug interactions during DOAC therapy (26.0% vs 7.1%, P = .154).
Conclusion:
Direct oral anticoagulant therapy was well tolerated by thoracic transplant recipients. Drug interactions and renal dose adjustments were common.
Introduction
Direct oral anticoagulants (DOACs) have revolutionized the field of anticoagulation for both venous thromboembolism (VTE) prophylaxis and treatment and nonvalvular atrial fibrillation. By working on specific targets within the coagulation cascade, these agents exhibit predictable pharmacokinetic and pharmacodynamic characteristics that allow for fixed oral doses. 1 Conversely, vitamin K antagonists (VKAs) work on several steps within the coagulation cascade and possess several drawbacks in therapy, including unpredictable dosing, numerous drug and food interactions, and frequent laboratory monitoring. 1 Many of these limitations are reduced or eliminated with the advent of DOACs. Rivaroxaban, apixaban, edoxaban, and dabigatran have been approved by the Food and Drug Administration for a variety of indications including nonvalvular atrial fibrillation to prevent stroke, systemic embolism, and postoperative thromboprophylaxis. 2 –5
The incidence of atrial arrhythmias ranges from 9.5% to 20% in heart and lung transplant recipients. 6,7 A majority of these thoracic transplant recipients with atrial arrhythmias also meet the clinical criteria for anticoagulation for the prevention of ischemic stroke. 6,7 Additionally, the incidence of VTE is approximately 29% in lung transplant recipients and 8.5% in heart transplant recipients, with high rates of recurrence. 8,9 As a result, these patients often require temporary and, for some, indefinite anticoagulation. Many providers consider utilizing DOACs in place of traditional VKAs. However, there are no published data of DOAC utilization in thoracic transplant recipients.
The purpose of this study is to describe the thoracic patient population selected for DOAC therapy and to assess adverse drug reactions, VTE recurrence, and drug–drug interactions during anticoagulation.
Methods
Study Design
Adult thoracic transplant recipients who were ever on DOAC therapy with apixaban, rivaroxaban, or dabigatran from May 1, 2011, to March 1, 2015, were retrospectively reviewed. Patient’s demographics, transplant, anticoagulation, and medication information were collected from electronic medical records. Laboratory values were collected to calculate creatinine clearance using the Cockcroft-Gault equation. 10 In the absence of a validated survey tool for thrombosis in a transplant population, cohort CHA2DS-VAS2c and HAS-BLED scores were calculated to extrapolate the theoretical risk of thrombosis versus bleeding in this population. 11
Pharmacotherapy Management
All patients initially received tacrolimus, mycophenolate mofetil, and steroid posttransplantation per institutional protocols. Subsequent changes in the immunosuppressive regimens were patient specific and according to physician’s preference. Transplant recipients were on fungal prophylaxis with an oral nystatin solution or triazole antifungal for 1 to 3 months, viral prophylaxis for 6 to 12 months, and indefinite Pneumocystis jirovecii pneumonia prophylaxis posttransplantation.
Anticoagulation management differed between heart and lung transplant recipients. All heart transplant patients requiring anticoagulation were initially started on warfarin, and their international normalized ratios (INRs) were managed by an outpatient pharmacist-supervised program within a cardiology clinic. Patients were switched to DOACs if they were considered to be noncompliant with clinical monitoring, had low time in therapeutic range (TTR), or if it was requested by the patient. The DOAC selection was per physician and pharmacist discretion.
In contrast, DOAC agents were utilized as the first-line anticoagulation therapy in all lung transplant recipients per the institutional protocol. For lung transplant recipients being treated for VTE, the recommended treatment duration is 3 to 6 months, unless the patient has recurrent VTEs, in which case therapy is indefinite. Rivaroxaban is the preferred DOAC for patients requiring VTE treatment who have creatinine clearances above 30 mL/min (calculated using the actual body weight). Apixaban is the preferred agent in lung transplant recipients with nonvalvular atrial fibrillation or those who are being managed for VTE treatment with a creatinine clearance less than 30 mL/min or with end-stage renal disease. All DOAC doses are reduced by half if patients were on concomitant strong cytochrome P450 3A4 (CYP3A4) inhibitors such as azole antifungals (ie, voriconazole, posaconazole, itraconazole, and fluconazole) or macrolide antibiotics (ie, clarithromycin and erythromycin). Patients who require frequent biopsies are given specific instructions as to when they should hold their DOACs. In patients with normal renal function, rivaroxaban is held for 2 days prior to the biopsy. Table 1 details drug-specific protocol recommendations and adjustments. Warfarin was initiated if patients do not meet the protocol criteria or due to insurance coverage issues.
Metabolism of DOAC Therapies and Thoracic Transplant-Specific Protocol Dose Adjustments.
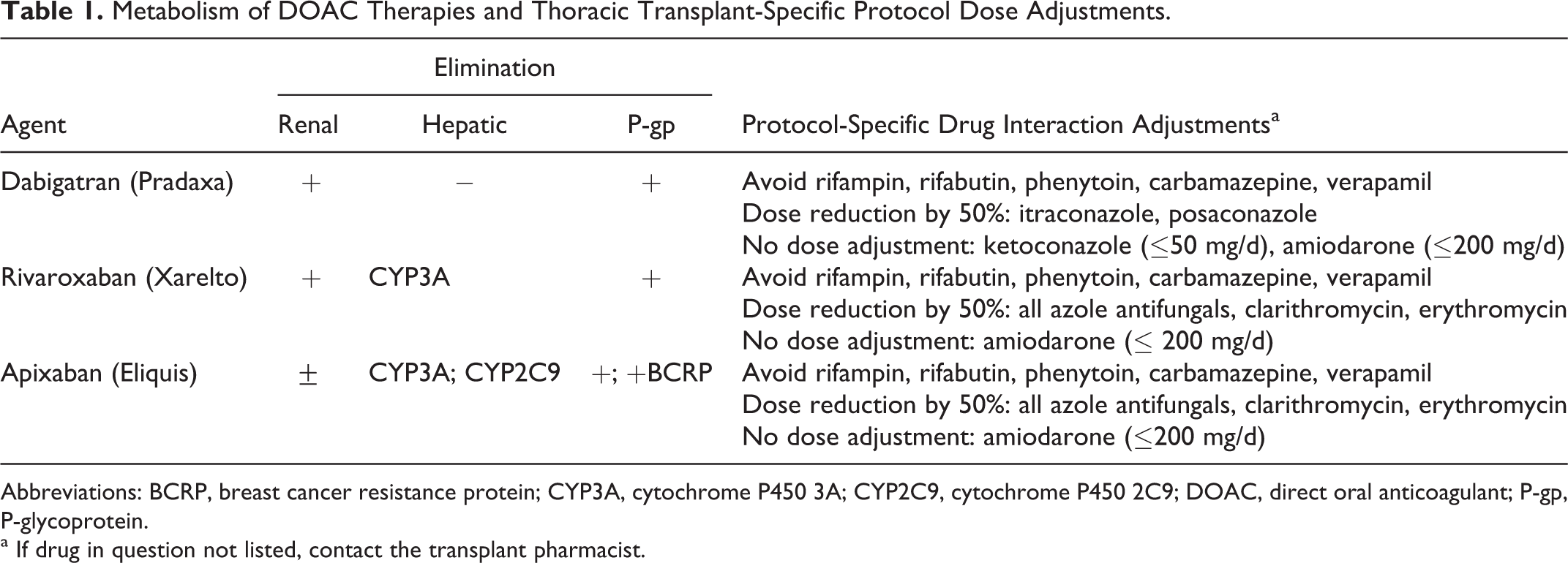
Abbreviations: BCRP, breast cancer resistance protein; CYP3A, cytochrome P450 3A; CYP2C9, cytochrome P450 2C9; DOAC, direct oral anticoagulant; P-gp, P-glycoprotein.
a If drug in question not listed, contact the transplant pharmacist.
Statistical Analysis
All data were tested for normality using the Shapiro-Wilk test. Normally distributed variables were assessed using parametric tests, whereas nonnormally distributed variables were assessed using nonparametric tests. Continuous variables are described as median (interquartile range [IQR]) or mean (±standard deviation [SD]). Categorical variables are compared using χ2 square test or Fisher exact test. Statistics were performed using SPSS for Windows, version 21 (IBM Corp, Armonk, New York).
Results
Patients
A total of 37 thoracic transplant recipients were initiated on DOAC therapy. Patients were transplanted between October 2006 and October 2014. Patients were started on DOAC therapy 438.5 days (IQR: 58-1119.5) after transplantation. The majority of patients were lung transplant recipients (86.5%) and had a history of VTE or a clotting disorder (see Table 2). All patients received some form of induction and many were maintained on a calcineurin inhibitor (97%) and mycophenolate (78%; Table 3). Most patients were warfarin experienced (78.4%). Baseline renal insufficiency at DOAC initiation was common with a median calculated creatinine clearance of 59.5 mL/min (IQR: 48.6-82.6 mL/min). Median CHADS2-VASc and HAS-BLED scores were both 3 (IQR: 2-4), respectively.
Patient Demographic Information of Thoracic Transplant Recipients Selected for DOAC Therapy.a
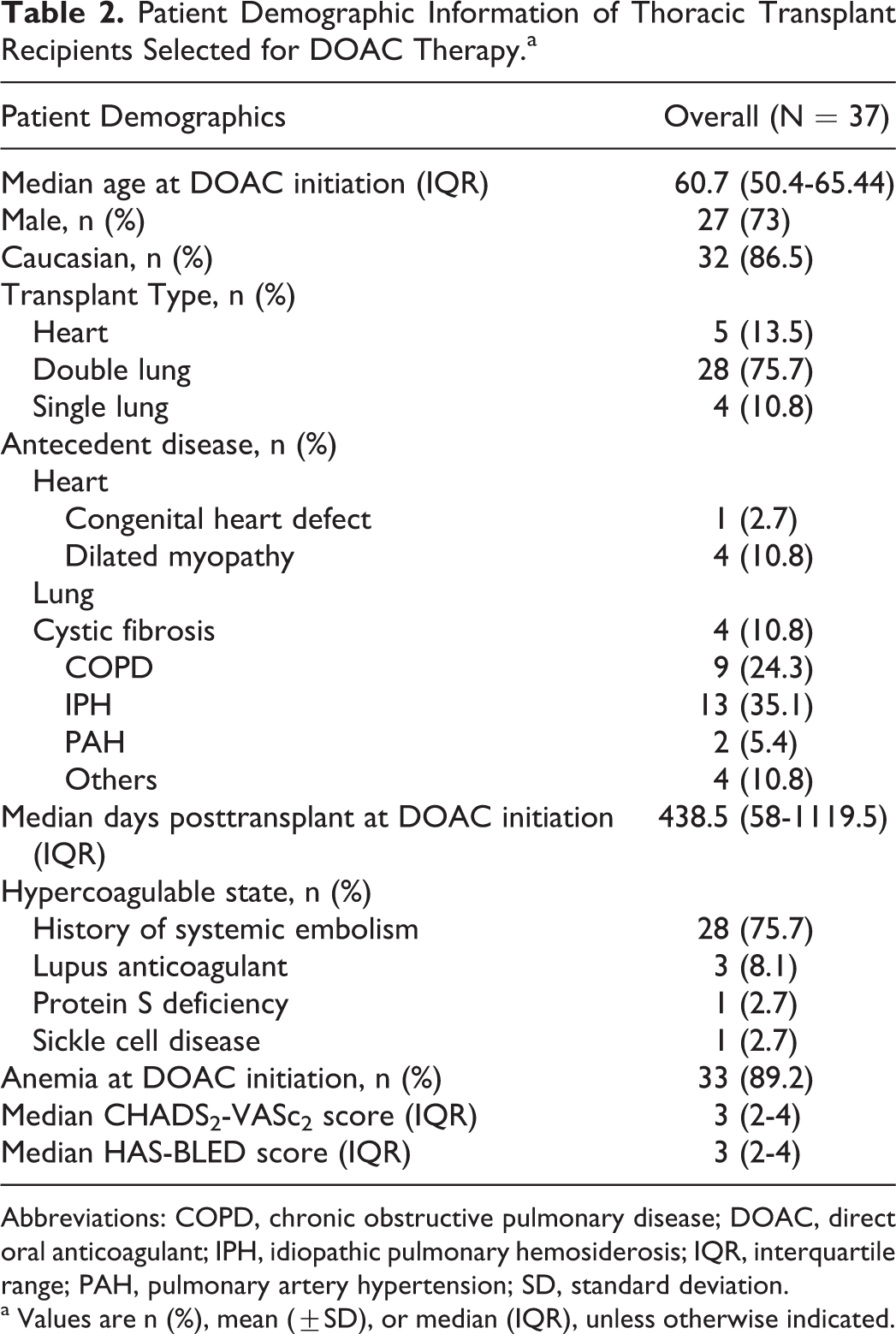
Abbreviations: COPD, chronic obstructive pulmonary disease; DOAC, direct oral anticoagulant; IPH, idiopathic pulmonary hemosiderosis; IQR, interquartile range; PAH, pulmonary artery hypertension; SD, standard deviation.
a Values are n (%), mean (±SD), or median (IQR), unless otherwise indicated.
Immunosuppressant and Anti-Microbial Regimens.a
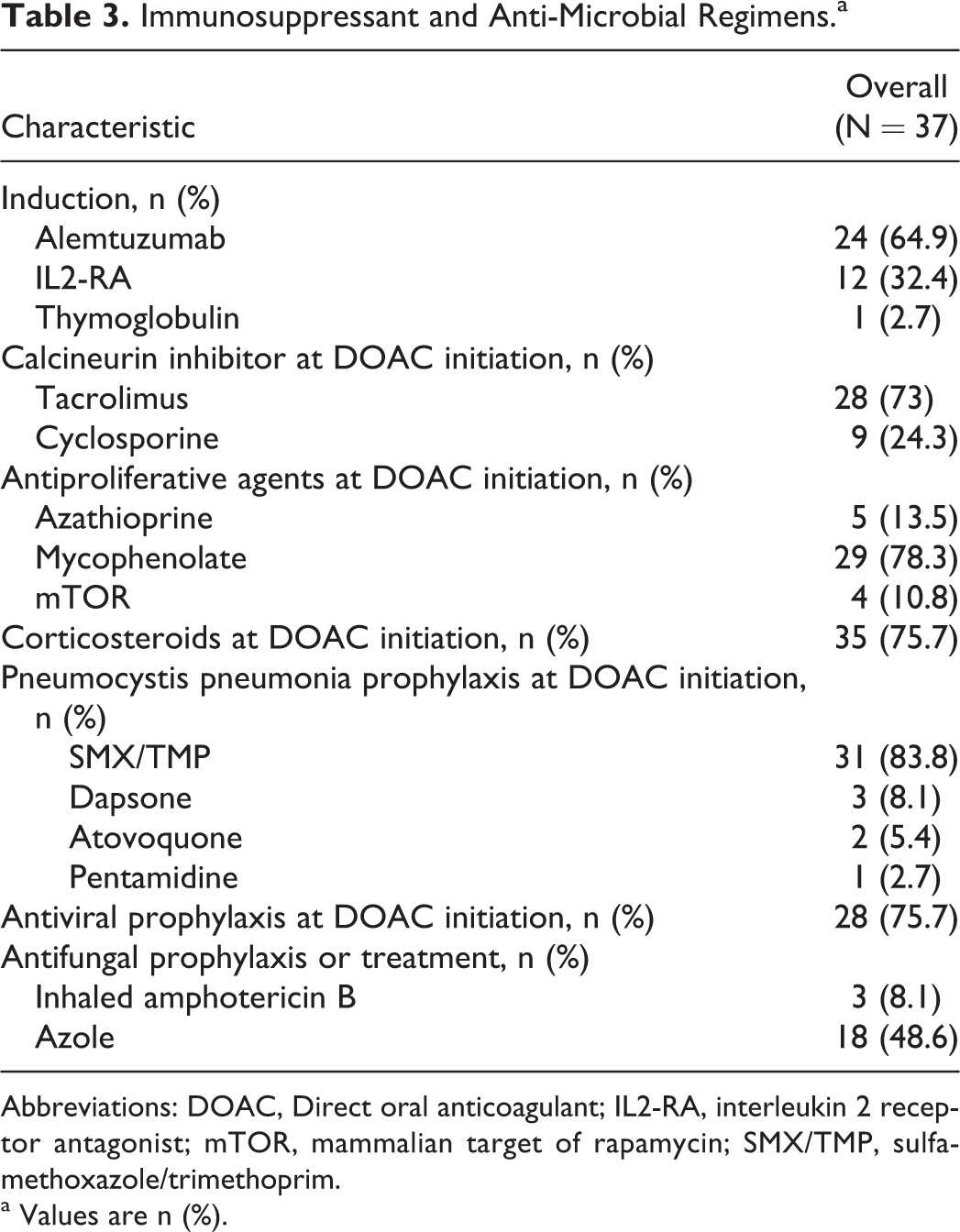
Abbreviations: DOAC, Direct oral anticoagulant; IL2-RA, interleukin 2 receptor antagonist; mTOR, mammalian target of rapamycin; SMX/TMP, sulfamethoxazole/trimethoprim.
a Values are n (%).
Direct Oral Anticoagulation Therapy
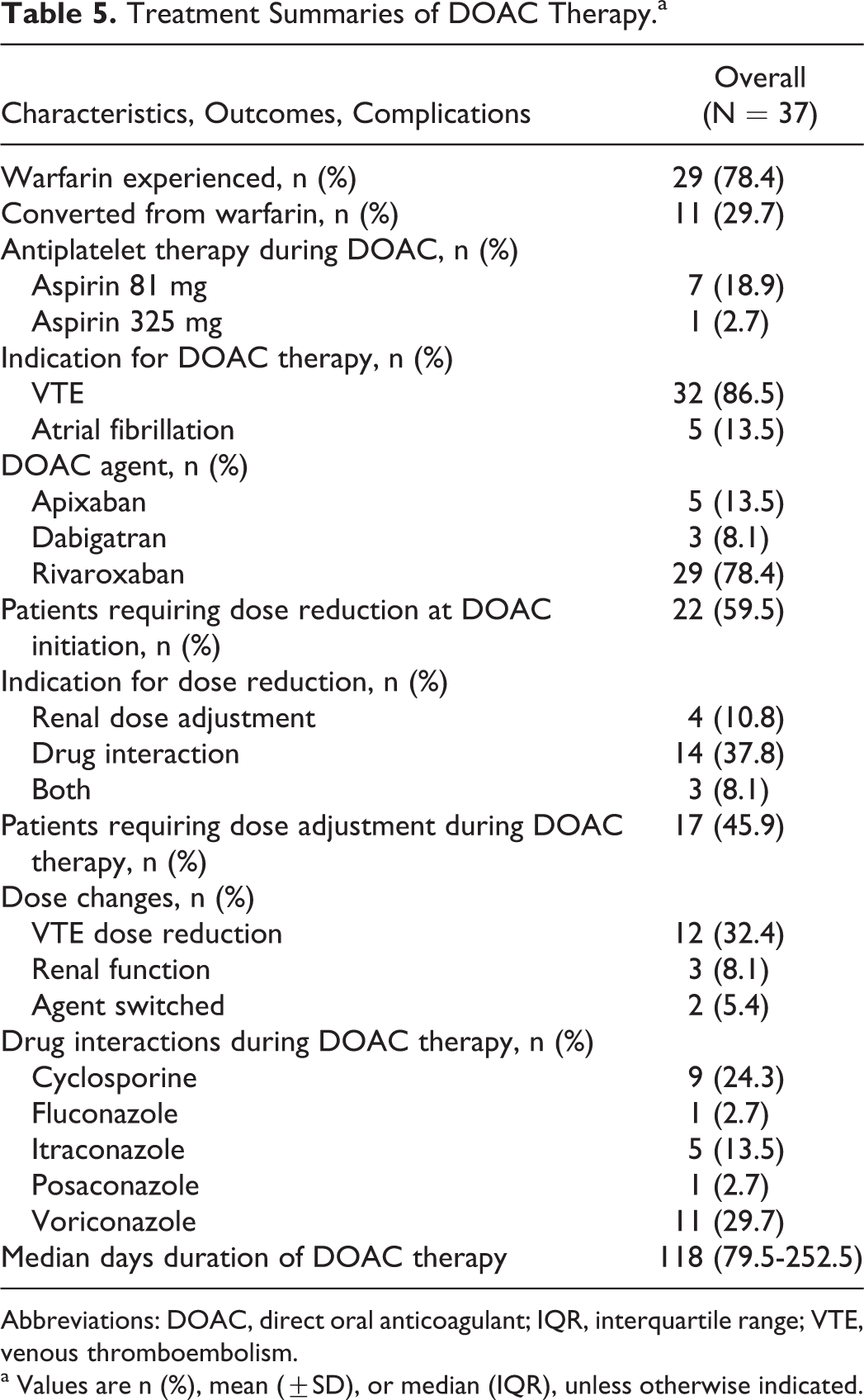
The median duration of DOAC therapy was 118 days (IQR: 79.5-252.5 days). Venous thromboembolism (86.5%) was the most common indication for DOAC initiation, and rivaroxaban (78.4%) was the most commonly used agent. A majority of the patients required preemptive DOAC dose reductions for major drug interactions (37.8%), renal insufficiency (10.8%), or both (8.1%). Dose adjustments occurred in 15 (40.5%) patients over the course of DOAC therapy for changes in renal function over time. Two patients were switched from rivaroxaban to apixaban, one due to hypersensitivity vasculitis and the other after the initiation of hemodialysis. Patient laboratory and treatment summaries are detailed in Table 4 and Table 5, respectively.
Laboratory Parameters at DOAC Initiation.a.
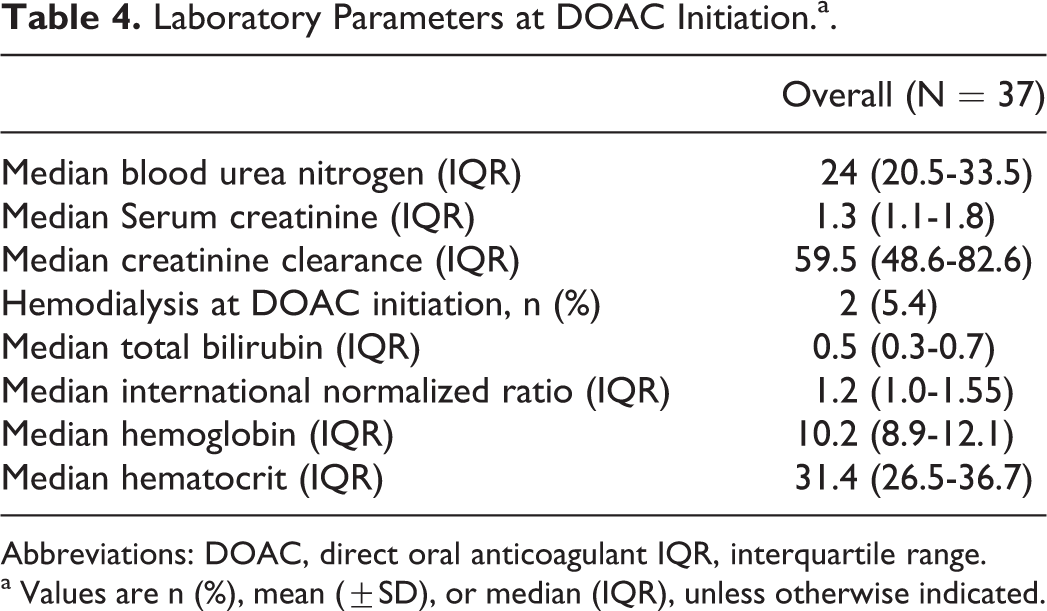
Abbreviations: DOAC, direct oral anticoagulant IQR, interquartile range.
a Values are n (%), mean (±SD), or median (IQR), unless otherwise indicated.
Treatment Summaries of DOAC Therapy.a
Abbreviations: DOAC, direct oral anticoagulant; IQR, interquartile range; VTE, venous thromboembolism.
a Values are n (%), mean (±SD), or median (IQR), unless otherwise indicated.
Safety and Adverse Effects
Overall, DOACs were well tolerated. No strokes or transient ischemic attacks were reported throughout the therapy. No patients required emergent reversal of their DOAC agent with factor products or dialysis due to bleeding. During DOAC therapy, there were a total of 38 unrelated hospitalizations in 24 patients. The median hospital length of stay was 6 days (IQR: 3.8-9.5 days). A majority of the patients were admitted for respiratory failure due to either suspected infection or rejection (45.8%). No patients were admitted due to adverse reactions from their DOAC. Additionally, 3 lung transplant recipients experienced acute cellular rejection during DOAC administration.
In total, 8 bleeding events occurred across 7 patients. There was no difference between the incidence of bleeding events between patients with identified drug–drug interactions on the profile and those without drug–drug interactions (26.0% vs 7.1%, P = .154).
One major bleeding event was observed. It was in a 61-year-old double lung transplant recipient with a gastrointestinal bleed requiring transfusion. The patient was on rivaroxaban 10 mg by mouth daily, dose reduced for concurrent azole therapy with itraconazole.
Seven minor bleeding episodes were identified in 6 patients. These events included epistaxis (10.8%), hematuria (2.7%), or hemoptysis after bronchoscopy (2.7%). The median calculated creatinine clearance in all patients with reported bleeding events was 61.77 mL/min (IQR: 53.0-81.52 mL/min), which was not significantly less than the cohort. One patient experienced gum bleeding while on rivaroxaban, but this adverse effect was attributed to concurrent cyclosporine use as opposed to DOAC therapy.
Conversely, 2 patients experienced breakthrough VTEs during DOAC therapy. The first was in a 61-year-old female single lung transplant recipient who was converted from warfarin to rivaroxaban 15 mg daily for a history of recurrent VTEs in the setting of active post-transplant proliferative disorder (PTLD). No hereditary hypercoagulable disorders were identified in the past hematologic evaluations. Rivaroxaban was initially dose reduced for renal dysfunction and concomitant azole therapy. This patient was on DOAC therapy for a total of 111 days before presenting with lower extremity VTE. At the time of diagnosis, the patient’s renal function had improved, leading to DOAC underdosing.
The second treatment breakthrough VTE occurred in a 45-year-old male heart transplant recipient on rivaroxaban 15 mg by mouth daily for an initial VTE resulting from prolonged hospitalization. The rivaroxaban was dose reduced for renal dysfunction. Approximately 2 months into therapy, the patient presented to the hospital with infection and shortness of breath. He quickly decompensated to a combination of septic and cardiogenic shock. A left ventricle apical thrombus was diagnosed 2 days prior his admission. The patient had no prior left ventricle dysfunction.
Discussion
This study was a retrospective, single-center analysis of 37 thoracic transplant recipients initiated on DOACs for the treatment of VTE and primary prevention of systemic embolism associated with atrial fibrillation. Overall, the patients included in this analysis tolerated anticoagulation therapy over the course of the study period, despite dose reductions and adjustments. Bleeds occurred in 21.6% of the population, but only 1 patient had a major bleeding episode requiring product transfusion.
Solid organ transplant recipients have an overall higher incidence of VTE compared to other populations due to several proposed mechanisms, including impairment of fibrinolysis by prolonged corticosteroid utilization, in vitro procoagulant effects of calcineurin inhibitors and proliferation signal inhibitors, endothelial damage due to cytomegalovirus infections, and allograft-specific factors. 12 The incidence of VTE after lung transplantation is between 8% and 27%, with older age, diabetes, pretransplant interstitial pulmonary fibrosis, and pneumonia being independent risk factors in this allograft population for thrombosis events. 8,13 –17 Additionally, the incidence of VTE is similar in heart transplant recipients (5%-34%). 18 The development of VTE was independently associated with chronic renal dysfunction, older age, obesity, and mammalian target of rapamycin utilization in heart transplant recipients. 18 –20 Thoracic transplant recipients are also at risk for VTE recurrence, making indefinite anticoagulation a distinct possibility.
Warfarin therapy in transplant recipients is difficult to manage. The TTR is a crucial factor to reducing breakthrough VTEs and adverse bleeding events. 21 Although the TTR has not been described in transplant recipients, previous studies in nontransplant populations have identified that the number of medications, female sex, cancer, and numerous hospitalizations are all predictors of lower TTR percentages. 22 The average TTR in nontransplant recipients is 48% to 61%, but this value is much lower in complex patient populations, such as those with ventricular assist devices, where the TTR can be as low as 31%. 23 A meta-analysis found that patients on DOACs had lower risk of bleeding compared to those maintained on warfarin with the TTR less than 66% (relative risk: 0.69, 95% confidence interval: 0.59-0.81). 23 For these reasons, DOAC therapy is a promising pharmacological option in thoracic transplant recipients with VTE or nonvalvular atrial fibrillation.
However, there are several considerations prior to starting DOAC therapy in transplant recipients. Dose reduction was common (59.4%) within our cohort due to identified drug interactions and renal dysfunction. Over 50% of thoracic transplant recipients experience renal dysfunction 5 years after transplantation. 24 Patients within our study had a median-calculated creatinine clearance of 59.5 mL/min (IQR: 48.6-82.6), with 18.9% of patients requiring initial dose reduction due to impaired renal function. Additionally, dose adjustments during DOAC therapy occurred in about half of the population (45.9%) due to fluctuating renal function. This variation in renal function in a transplant population is more common due to immunosuppression, aging, and other chronic disease states such as hypertension and diabetes mellitus. Since all DOAC agents require renal dose adjustment, judicious monitoring of renal and electrolyte laboratory parameters is imperative to ensure adequate and safe dosing strategies over time.
Additionally, drug interactions are a common phenomenon in a transplant population, especially in those requiring antifungal therapies. This poses a serious problem to patients maintained on DOAC and warfarin anticoagulation therapy. Unlike warfarin therapy, there is no proven laboratory surrogate marker to guide dose changes, such as INR, in patients receiving DOAC therapy. The inhibitory potential of azole antifungals also varies. Itraconazole and posaconazole are more potent CYP3A4 inhibitors compared to fluconazole and voriconazole. In addition, fluconazole and voriconazole inhibit CYP2C9 and CYP2C19, whereas posaconazole and itraconazole inhibit P-glycoprotein. 25 The effect of these agents on DOACs is not fully known at this time. In the setting of concomitant fluconazole in vivo, the exposure to rivaroxaban increases 42%, although no dose adjustment recommendations exist in the setting of drug interactions. 26 Dose reductions for such drug interactions only recommended in the apixaban prescribing information are based on pharmacokinetic modeling. 4
At our institution, protocols recommend reduction in both rivaroxaban and apixaban doses in the setting of select azole antifungals. Patients frequently (45.9%) required this type of dose reduction at the initiation of DOAC therapy. With this novel dosing strategy, we identified no significant differences in bleeding events between with and without DOAC drug interactions. Specific dose reductions are included in Table 5. This dose modification is only used in the presence of select drugs and does not account for other drug interactions that may impact P-glycoprotein or other CYP450 enzymes.
Limitations
Several limitations exist within this study. This study was a retrospective, single-center cohort study evaluating thoracic transplant recipients treated with DOACs for either VTE or atrial fibrillation. Our data were dependent on documentation in the medical record, which may have led to underreporting of outcome data, including adverse drug events. Our study was limited by small sample size and was not sufficiently powered to detect clinical differences between groups. There were also protocol differences between the allografts regarding anticoagulation. Finally, there is no current validated tool in transplant recipients to assess the risk of thrombosis and bleeding events. To provide some insight into risk stratification, our group calculated CHA2DS-VA2Sc and HAS-BLED scores to describe the score-specific grading characteristics in our population. The CHA2DS-VA2Sc scoring stratifies the risk of stroke; on the other hand, the HAS-BLED score estimates the 1-year risk for major bleeding in patients maintained on anticoagulation for thromboprophylaxis. In our analysis, no thoracic transplant recipient required reversal agents for bleeding events. However, there are only limited reversal options for patients on DOAC therapy The recently approved idarucizumab (Praxbind) has demonstrated complete reversal of the dabigatran anticoagulant effect within minutes. 27 Additionally, the impeding release of investigational agents andexanet alfa (ANNEXA-A and R) and aripazine (PER977, ciraparantag) may expand reversal options for factor Xa inhibitors.
This analysis also has strengths. This is the largest reported cohort of thoracic transplant patients to be initiated on DOACs and is meant to be hypothesis-generating research. Given the potential benefit of these agents within a transplant population, this study helps clinicians gain insight into our anticoagulation experience. Our protocols also include information of patient-specific factor and drug interaction into the decision tree for practitioners, potentially decreasing dosing errors at DOAC initiation.
Conclusion
Direct oral anticoagulant therapy is utilized at our center as an alternative to warfarin for the treatment of VTE and prophylaxis of embolization in nonvalvular atrial fibrillation in thoracic transplant recipients. Renal functional assessment and drug interactions should be assessed at initiation and throughout DOAC therapy to minimize adverse effects. Larger, randomized clinical trials are needed to provide a definitive place in therapy for DOACs after thoracic transplantation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. C. R. E. is an advisory board member of Baxter Immunosciences. J. J. T. is an advisory board member and invited speaker of HeartWare, Thoratec, CI Clinical Trial for the HeartMateIII, and an advisory board member of Abiomed. M. A. S. is an advisory board member and a speaker of CareDx.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: C. R. E. and J. F. M. received grant support from Amgen/Onyx Pharmaceuticals.