
Abstract
Purpose:
BK virus (BKV) nephropathy has increasingly become an important cause of morbidity in renal transplant recipients. We evaluated the frequency and associated factors for BKV infection in a center performing mainly living donor transplantations over a long time period.
Methods:
One hundred consecutive renal transplant patients were included. Quarterly visits were planned to examine urine for decoy cells and to measure the BKV DNA in the blood and urine. Renal biopsy was performed in case of deteriorated allograft function. Serological examinations for BKV immunoglobulin G (IgG) were performed in donors.
Results:
Throughout the entire follow-up period, the rates of viruria, viremia, and the positivity of decoy cells were 12%, 6%, and 13%, respectively. The negative and positive predictive values of decoy cells were 93.1% and 69.2%, respectively, for viruria, and 99.2% and 45.5%, respectively, for viremia. Biopsy-proven BKV nephropathy was observed in 1 patient. The BKV IgG was positive in all living donors. Viruria and viremia were associated with deceased donor transplantation, acute rejection, and pulse steroid therapy. In addition, viremia was associated with antithymocyte globulin therapy and a short duration of the posttransplant period.
Conclusions:
The frequency of BKV infection was lower in our transplant unit compared to previous reports. Reduced doses of immunosuppression seem to be the main factor that may explain the reduced frequency. However, an active screening strategy is still of importance for this patient group.
Introduction
The cause of the increased incidence of BK virus (BKV) infection is unclear, but it has emerged as an important cause of morbidity in renal transplant recipients. Modern and more efficient immunosuppressive drugs may play a role in this increase. 1
Primary BKV infections tend to occur early in childhood, are usually asymptomatic, and are thought to remain latent. 2 Seroprevalence studies have found antibodies for BKV (latent infection) in 80% of adults. 3 Immunosuppression can induce viral replication in patients who are previously exposed to BKV. Viral replication (active infection) progresses through consecutive stages: viruria, viremia, and BKV nephropathy (BKVN). 4 Nephropathy can cause allograft dysfunction or graft loss in 15% to 50% of affected cases. 5,6 Since specific effective antiviral therapy does not currently exist, the cornerstone of therapy is to reduce immunosuppressive medications. Therefore, screening for early diagnosis is essential. 7,8 Active infection most commonly occurs during the first 2 years following transplantation. 4 Different screening protocols until the fifth posttransplant year are recommended. 9,10
To the best of our knowledge, in previous studies, mainly patients in the early phase of transplantation have typically been examined. We aimed to investigate the frequency of BK, viruria, and viremia and the association with clinical data and allograft function in renal transplant recipients. We also aimed to investigate the role of seropositivity in living donors.
Patients and Methods
Design Setting
We performed the study in 2 consecutive phases. In the first cross-sectional phase, we examined demographic, clinical, laboratory data and selected patients according to inclusion and exclusion criteria. In the second follow-up phase, eligible patients were followed up with quarterly visits and screened for active BKV infection. Three quarterly follow-up visits were planned for each patient. The study protocol was approved by the local medical ethics committee (approval no 20678). All participants gave their informed consent.
Our transplant clinic is located in a tertiary care center, with 25 to 30 kidney transplantations performed yearly mainly from living donors. Approximately 350 transplant patients attend regular follow-up visits. The frequencies of regular visits were planned individually according to the clinical status of each patient. Generally, the following schedule was used: during the first year of the transplantation; monthly visits, 1 to 3 years after transplantation; visits every 2 or 3 months, following the third year of the transplantation; and visits every 4 or 6 months.
Inclusion–Exclusion Criteria and Selection of the Patients
Inclusion criteria were as follows: adult (>18 years of age) renal transplant patients who had a renal transplant in our transplantation center during the last 5 years and who can give informant consent were eligible for the study. Exclusion criteria were as follows: patients who had a glomerular filtration rate (GFR) calculated according to the Modification of Diet in Renal Disease formula of <20 mL/min/1.73 m2, had a diagnosis of malignancy, or did not regularly show up at follow-ups (Figure 1). In patients with a low GFR (<20 mL/min/1.73 m2), the risk of graft failure is higher, and they may not complete the 1-year follow-up period. Therefore, such patients were excluded from the study.
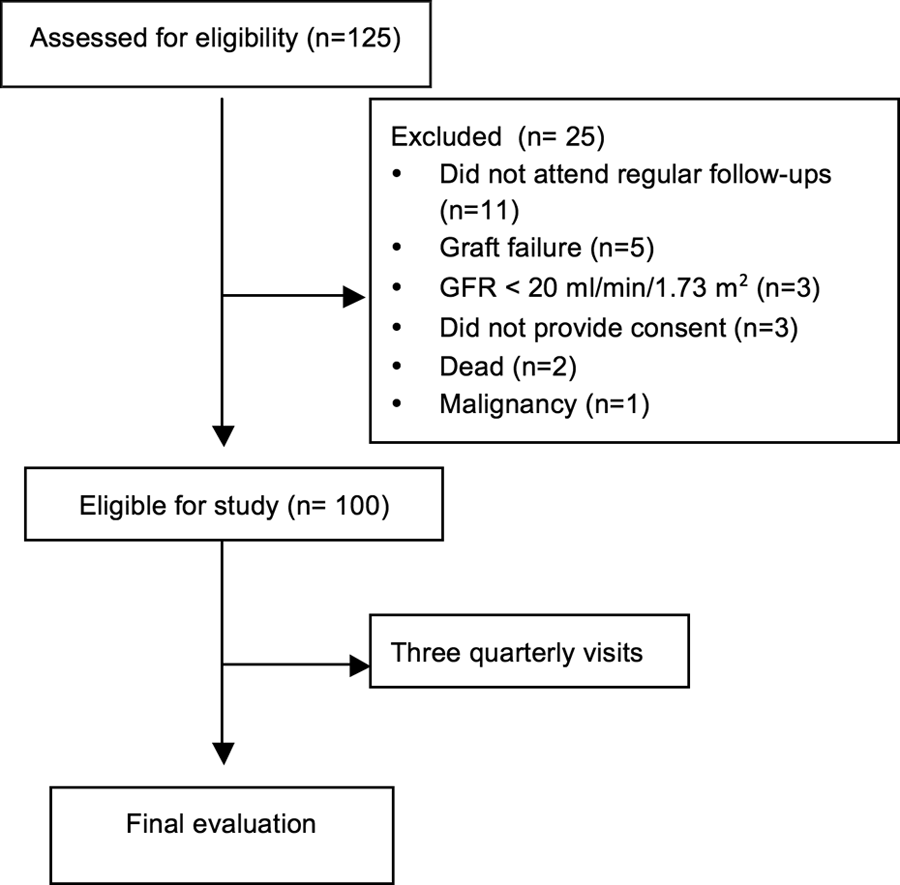
Flow diagram showing patient selection.
Between February 2006 and April 2010, a total of 125 adult renal transplantations were performed. We screened those patients between February 2010 and November 2010. Eleven patients did not show up for their regular follow-up visits, 3 patients had low GFR (<20 mL/min/1.73 m2), 1 patient had malignancy, 3 patients refused to participate in the study, 2 patients were dead, and 5 patients had graft failure (due to vascular thrombosis in 4 patients and severe acute tubular necrosis in 1 patient). Therefore, 100 patients were eligible for the study (Figure 1).
Data Collection and Definitions
Information on sex, date of birth, height, weight, blood group, etiology of end-stage renal disease (ESRD), the type and duration of pretransplant renal replacement therapy, the number of human leukocyte antigen (HLA) mismatches, hepatitis B virus, hepatitis C virus (HCV), and cytomegalovirus (CMV) status, and CMV prophylaxis was retrieved from the patient files. In addition, type of the induction treatment; the immunosuppressive drugs and their doses used in the first month, the first year, and the last visit; biochemical data at the first year and last visit; delayed graft function (DGF); and presence of acute rejection were recorded.
The DGF was defined as the need for dialysis within the first week after transplantation. Acute rejection was defined as rejection diagnosed according to renal biopsy findings.
Data on hepatitis B surface antigen (HBsAg) positivity and presence of anti-HCV antibodies were collected. Acyclovir, ganciclovir, and valganciclovir treatment used for CMV prophylaxis and antithymocyte globulin (ATG) and basiliximab used in induction treatment were recorded.
Pretransplant latest applied dialysis type was recorded and its duration was expressed as months. Donor age, type (living/deceased donor), blood group, and CMV status were recorded from the medical records.
Clinically significant viruria and viremia were defined as >107 copies/mL of BKV DNA in urine samples and >104 copies/mL of BKV DNA in blood samples, respectively
Follow-Up Visits
During quarterly visits, routine clinical and laboratory evaluation of the patient was done by the physician who followed up the patient. Moreover blood and urine samples were collected for the measurement of BKV DNA. At the same visit, cytological examination was done to reveal decoy cells in fresh urine. The limited number of BKV DNA measurement kits that were available for the study prevented us from performing quarterly measurements, and all of the samples were studied at the end of follow-up. Therefore, physicians who followed up the patients throughout the study did not know the results of the BKV DNA. However, the results of the decoy cells were known. In patients with positive decoy cells, urine and blood BKV DNA was measured in a separate laboratory without delay (Figure 2). Agreement for BKV DNA positivity was good between this laboratory and our study laboratory (κ = .77, P = .001). Further management of the patient was decided by the physician who followed up the patient.
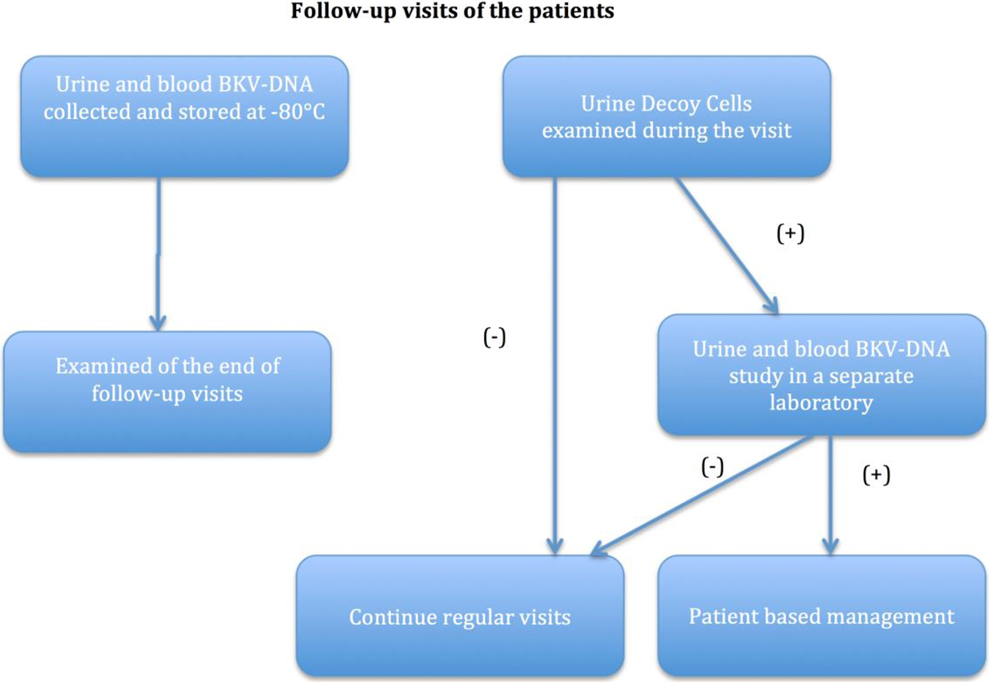
BK virus (BKV) DNA and decoy cell examinations during patient follow-up.
Laboratory Procedures
Urine samples and centrifuged blood samples that were collected during follow-up visits were stored at −80°C. Then at the end of the follow-up, all the samples were studied (Figure 2).
Nucleic acid extraction in the samples was performed automatically by the MagNA pure LC (Roche, Mannheim, Germany) device using the MagNA pure LC kit (Roche). After the nucleic acid was obtained, BKV presence and quantification were measured with a LightCycler instrument (Roche) using a Lightmix polyomavirus JC/BK (TIB MOLBIOL, Berlin, Germany) kit and the real-time polymerase chain reaction (PCR) method according to the manufacturer’s instructions.
Immunoglobulin level against BKV was measured only on donors. As we were searching for active infection, we studied BKV DNA in recipients. However, in donors, we looked for latent infection. Therefore, we studied BKV immunoglobulin G (IgG). Blood samples were collected in dry tubes for serological examination. The enzyme-linked immunosorbent assay (ELISA) plates were coated with BKV VP1 major capsid protein (Abcam, Cambridge, United Kingdom) for serological examination at the Department of Microbiology of Cerrahpasa Medical Faculty. The BKV IgG was investigated in serum samples using the ELISA method, with labeled goat antihuman IgG (Abcam, Cambridge, UK) used as the secondary antibody.
Statistical Methods
Data are expressed as mean (standard deviation), if not stated otherwise. The patients were categorized according to the presence of viruria and viremia. Categorical variables were compared using χ2 or Fisher exact test, when appropriate. Continuous variables were first analyzed for normality by examining histograms and normal Q-Q plots and then compared using Student t test or Mann-Whitney U test, when appropriate. Thus, factors associated with viruria and viremia were investigated. Positive and negative predictive values of decoy cell examination were calculated using formulas described elsewhere. 11 Agreement between different laboratories about the presence of viruria and viremia was evaluated using κ statistics. All tests were performed using SPSS for Windows version 17.0 (SPSS Inc, Chicago, Illinois) software. Two-tailed significance was set at ≤.05.
Results
Patients, Donors, and Early Posttransplant Period
The patient baseline characteristics are shown in Table 1. Patients were mostly middle-aged or young (median: 35, range: 20-65 years) individuals with a higher prevalence of males. The most common cause of ESRD was glomerulonephritis (24%). This was followed by hypertension (18%), vesicoureteral reflux (8%), and amyloidosis (8%). Etiology in a major portion (23%) of the patients could not be detected. Various causes of ESRD such as pyelonephritis, polycystic kidney diseases, diabetes, vasculitis, and postrenal causes were reported in the remaining 19% patients.
Baseline Characteristics of Kidney Transplant Recipients.

Abbreviations: ATG, antithymocyte globulin; BMI, body mass index; HLA, human leukocyte antigen.
aIn living transplantations, ATG was used in conjunction with basiliximab due to delayed graft function in 2 recipients and for the treatment of acute rejection in other 2 recipients.
Anti-HCV positivity was noted in 1 patient. The HBsAg positivity was also found in another patient. There was no CMV immunoglobulin M (IgM) positivity, and CMV IgG positivity was found in 96.8% of the patients. Antiviral prophylaxis, typically with valganciclovir, was used for 3 months for CMV infection (data not shown).
Most recipients received living donors (81%). Most of the living donors were mothers (45.7%), followed by fathers (19.8%), spouses (16%), siblings (13.6%), and other relatives (4.9%). The mean age was 47.1 (8.7) and 37.8 (13.6) years for living and deceased donors, respectively. The average number of mismatch was 2.8 ± 1.3. While 80 patients’ mismatch number was 3 or less, it was greater than 3 for 20 patients. The CMV information was available for 84 of the 100 donors (81 living and 3 deceased donor). The CMV IgG positivity was 95.2%, and CMV IgM was negative in all donors.
The DGF developed in 16 patients in the early posttransplantation period. The cause of DGF was acute tubular necrosis in 14 patients, acute rejection in 1 patient, and calcineurin inhibitor toxicity in 1 patient. Acute rejection occurred in an additional 13 patients during follow-up. All rejections were biopsy proven. Rejections were seen in the first year in 11 patients, while the other 2 rejections developed in the second and third years.
Immunosuppressive Treatment
The biological agents used in the recipients are shown in Table 1. The ATG was used in induction therapy for deceased donor transplantations. Basiliximab or ATG was used in patients with living donors, according to the immunological risks of the patient. The use of basiliximab was higher than ATG due to the higher proportion of live kidney transplantations.
Generally, calcineurin inhibitor–based immunosuppression therapy was used. All patients were using steroids. Steroid therapy was not stopped during the follow-up period in any patient. Mycophenolic acid, azathioprine derivatives, and the mammalian target of rapamycin were used as the secondary treatment.
Frequency of BKV Infection
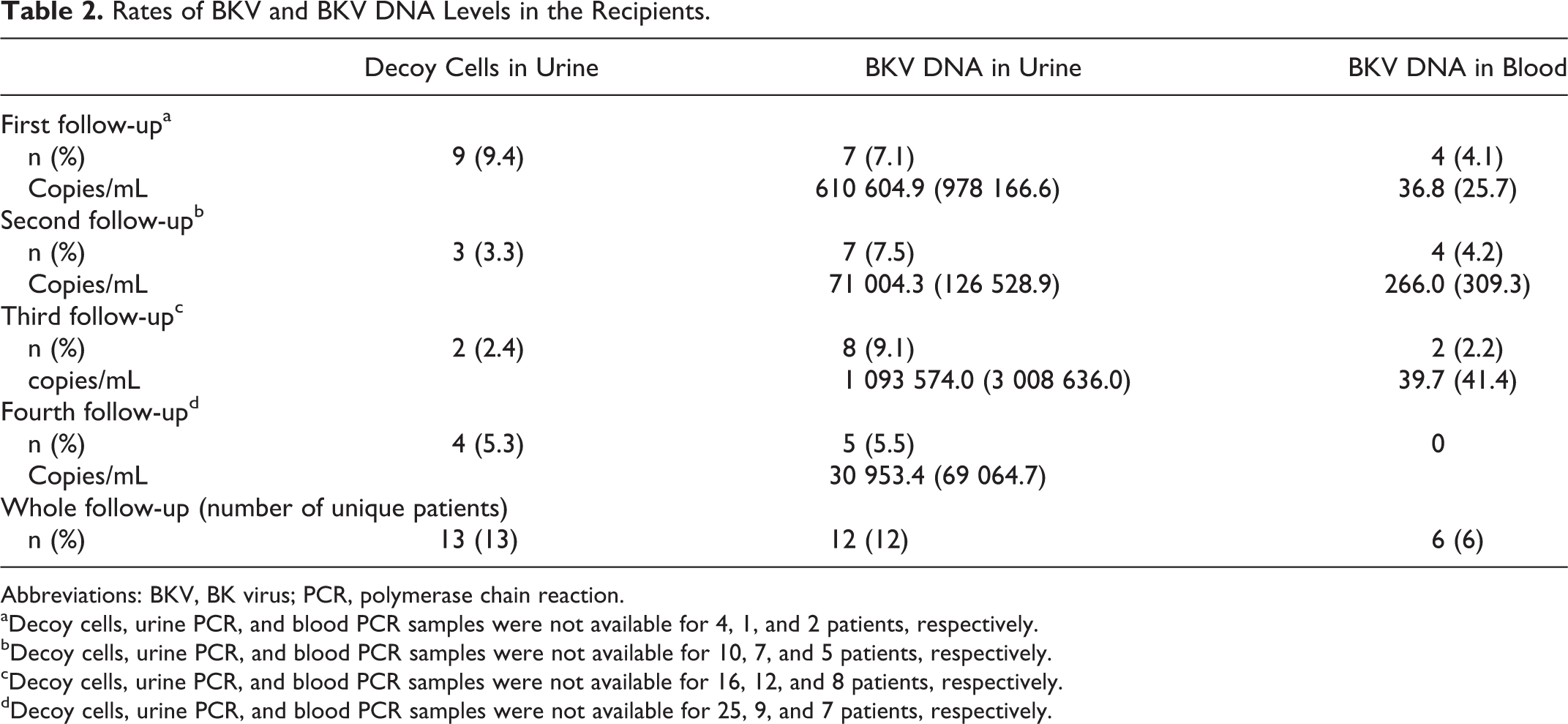
The detection rates of BKV in blood and urine samples with PCR and cytological examination are shown in Table 2. Decoy cell positivity, viruria, and viremia were detected in 13, 12, and 6 patients, respectively, during the follow-up period. The positive predictive values for the presence of decoy cells for viruria and viremia were 69.2% and 45.5%, respectively. The negative predictive values for the same parameters were 93.1% and 99.2%, respectively.
Rates of BKV and BKV DNA Levels in the Recipients.
Abbreviations: BKV, BK virus; PCR, polymerase chain reaction.
aDecoy cells, urine PCR, and blood PCR samples were not available for 4, 1, and 2 patients, respectively.
bDecoy cells, urine PCR, and blood PCR samples were not available for 10, 7, and 5 patients, respectively.
cDecoy cells, urine PCR, and blood PCR samples were not available for 16, 12, and 8 patients, respectively.
dDecoy cells, urine PCR, and blood PCR samples were not available for 25, 9, and 7 patients, respectively.
Of the 87 patients whose decoy cells were negative, urine BKV DNA was positive in 8 patients and blood BKV DNA was positive in 1 patient throughout the follow-up period. All patients became negative for BKV DNA. None of the patients experienced renal dysfunction.
Serologic evaluation was performed in the kidney donors. We reached 70 of the 81 kidney donors. All kidney donors were positive for BKV IgG. Serologic evaluation was not performed on kidney recipients.
Management of Patients With Positive Decoy Cells
Decoy cells were positive in 9 patients at the first follow-up visit. Four of these patients had BKV DNA positivity in the blood and >107 copies/mL of BKV DNA in urine samples. The treatment regimen changed in those patients. The antimetabolites and calcineurin inhibitor doses were reduced by 50% and 30%, respectively. Additionally, in 1 of those 4 patients, the creatinine levels were also increased, and a kidney biopsy was performed and revealed BKVN. In that particular patient, antimetabolites were stopped and leflunomide was introduced. Viremia disappeared completely in the follow-up of all patients, while viruria disappeared in 2 patients and regressed in 2 patients.
In the patient with a biopsy demonstrating BKVN following a reduction in immunosuppressive doses, creatinine levels continued to increase; a second kidney biopsy was performed, and acute cellular rejection was found. The dose of calcineurin inhibitor was increased. Creatinine levels remained stable, however, due to progressive heavy proteinuria, and a third biopsy was performed and revealed membranoproliferative glomerulonephritis (possibly recurrent). Eventually, the patient had graft loss due to recurrent glomerulonephritis.
Factors Associated With Viruria and Viremia
Patients were grouped according to the presence of viruria and viremia. The demographic, laboratory, and clinical characteristics of the viruria-positive and viruria-negative renal recipients were compared. The presence of viruria was found to be related to deceased donor transplantation (P = .048), acute rejection (P = .000), pulse steroid therapy (P = .000), and the presence of viremia (P = .022). Moreover, there was a trend for a higher frequency of viruria (especially >107 copies/mL) in the early posttransplant period (Figure 3). The mean time at diagnosis was 23.6 (18.8; median: 21, range: 2-59 months) for viruria and 12.3 (5.3; median: 12.5, range: 7-21 months) for viremia.
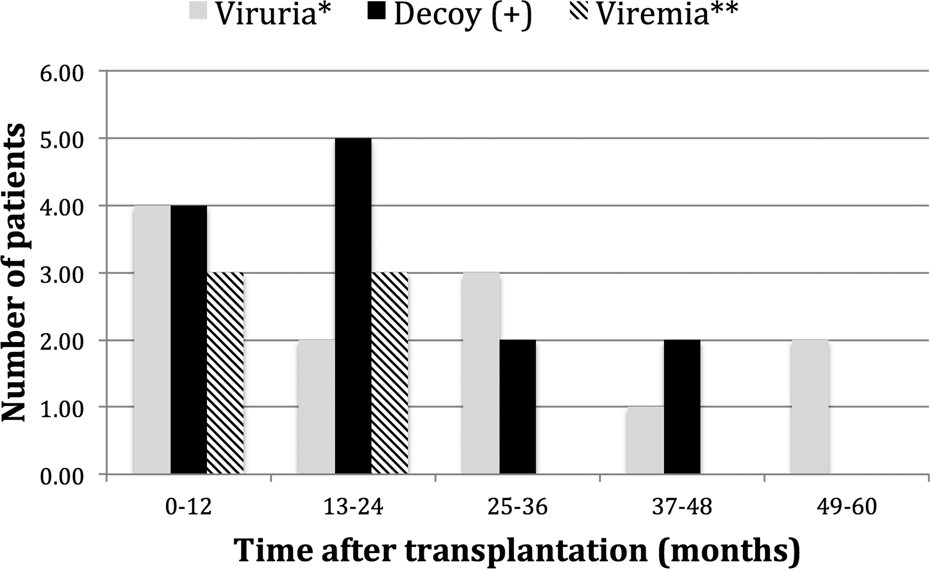
Viruria, viremia, and the presence of decoy cells according to time after transplantation. *There were no patients with >107 copies/mL of BK virus (BKV) DNA in urine after 24 months of transplantation. **There were no patients with >104 copies/mL of BKV DNA in blood.
The comparisons of the demographic, laboratory, and clinical characteristics of the viremia-positive and viremia-negative patients are shown in Table 3. The presence of viremia was found to be associated with deceased donor transplantation (P = .011), a short duration of the posttransplant period (P = .01), acute rejection (P = .000), ATG therapy (P = .004), pulse steroid therapy (P = .013), and the presence of viruria (P = .022). Due to the small number of patients with viremia, it was not possible to perform a statistically appropriate multivariate analysis.
A Comparison of the Characteristics of Viremia-Positive and Viremia-Negative Renal Recipients.
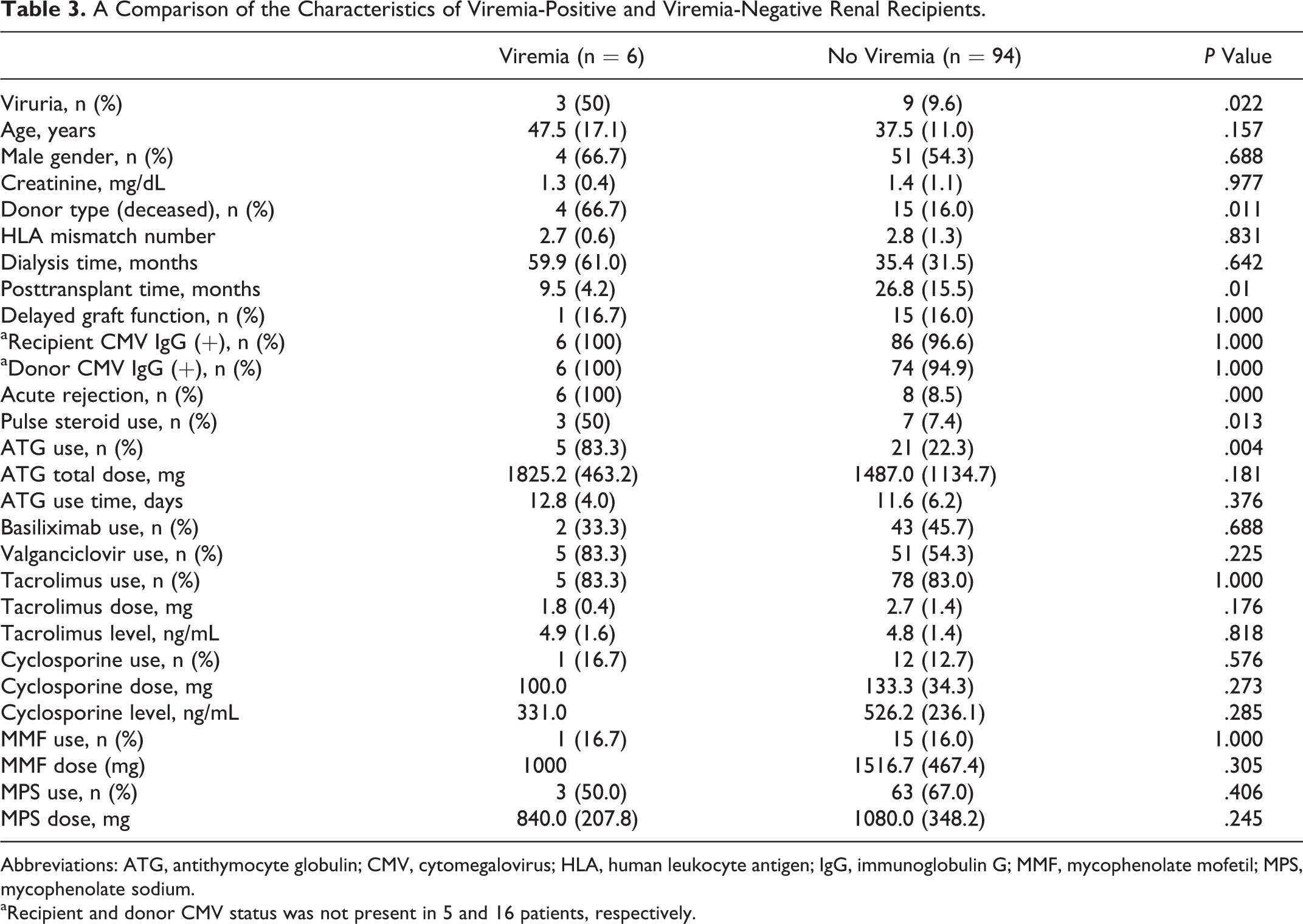
Abbreviations: ATG, antithymocyte globulin; CMV, cytomegalovirus; HLA, human leukocyte antigen; IgG, immunoglobulin G; MMF, mycophenolate mofetil; MPS, mycophenolate sodium.
aRecipient and donor CMV status was not present in 5 and 16 patients, respectively.
Discussion
In our study, the frequencies of viruria and viremia were 12% and 6%, respectively. Viremia was seen in patients with a short posttransplant period, and most cases remained subclinical. Graft failure was observed only in 1 case in which the cause was recurrent glomerulonephritis, which cannot be attributed to BKVN.
Viruria was first shown in a renal recipient and found to be related to BKVN. 12 Munoz et al found the frequency of viruria among renal recipients to be 26.5% in a prospective study of 156 heart, liver, or kidney transplantation patients. 13 Splendiani et al studied 118 liver or kidney transplants and found the frequency of viruria to be 13.6% in renal recipients. 14 In a prospective randomized trial by Brennan et al, the frequency of viruria was found to be 35% in the first year in a series of 200 renal transplantation patients. 8
The frequencies of viruria and viremia were lower in our study compared to other studies. This finding can be related to different causes, which are not mutually exclusive: first, the screening of patients with decoy cells and the reduction of immunosuppressive drugs in BKV DNA-positive patients, and second, in our institution, the number of transplantations from living donors was higher than deceased donor transplantations and immunosuppressive drugs are used in lower doses. For instance, 33% of our patients did not use induction therapy. Additionally, in our cohort, the posttransplantation time period was longer than the usually recommended screening period for BKV, which is 2 years. Therefore, patients with longer posttransplantation times might contribute to the lower overall incidence. However, it should be noted that even after second posttransplantation year, we detected patients with viruria.
Decoy cell positivity was 13% in our study. The positive and negative predictive values of decoy cells for viruria were 69.2% and 93.1%, respectively. The positive and negative predictive values of decoy cells for viremia were 45.5% and 99.2%, respectively.
Randhawa et al studied 100 urine samples and found the positivity of decoy cells to be 13%. All decoy cell–positive samples were also viruria positive, and 18% of viruria-positive samples were detected in decoy-negative patients. The sensitivity, specificity, and positive and negative predictive values of decoy cell positivity for viruria were 41.9%, 100%, 100%, and 82.8%, respectively. 15 In a prospective study by Hirsch et al among 78 renal recipients, the frequency of decoy cells was 30%, and the sensitivity, specificity, and positive and negative predictive values of decoy cells for BKVN were 100%, 71%, 29%, and 100%, respectively. 16 Strongest aspect of decoy cell examination is its high negative predictive value. The cost of the screening method is another point to consider. For example, in our unit, the cost for decoy cell is US$16 and cost for PCR analysis is US$51 (price paid by the social security agency and calculated according to current exchange rate).
In our study, viruria and viremia were associated with acute rejection, pulse steroid use, and deceased donor transplantation. We also found that viremia was higher in patients who used ATG and those with a short posttransplant period. The high rates of viruria and viremia for deceased donor transplantation might be related to the intensive use of immunosuppressive drugs, the cold ischemia period, and DGF, as indicated in previous studies.
Awadalla et al studied 444 renal recipients and observed 40 BKVN-positive patients. The mismatch numbers of HLA, the frequency of acute rejections and pulse steroid, and ATG usage were significantly higher in patients with BKVN. 17 Hirsch et al also found an association between BKVN and acute rejection and acute rejection treatment. 16
We could not find any relationship between the type of immunosuppressive drug used and viruria or viremia in this study. This could be due to a type 2 statistical error, as the number of patients with viremia or viruria was relatively low.
It has been reported that the degree of immunosuppression is the most important risk factor for BKV infection. Gralla et al reported that BKV replication is a reliable indicator of excessive immunosuppression. 1 The tacrolimus and tacrolimus–mycophenolate mofetil combination has been reported to be associated with BKVN. 18 Hirsch et al found that BKV viruria and viremia levels were higher in patients treated with tacrolimus compared to cyclosporine. 19 However, Brennan et al did not confirm this finding. 8 In addition, an association between BKVN and calcineurin inhibitor–free regimens has been shown in the literature. 20
In our study, a serological investigation was performed in 70 living kidney donors. All samples were positive for BKV IgG. In other studies, the seropositivity for BKV in the healthy adult population ranged between 70% and 87%. 21 –23 Ginevri and Smith determined that BKV seronegativity in the recipient was a risk factor for BKVN. 24,25
One of the limitations of our study was that BKV DNA levels in the urine and blood samples were studied after the collection of all samples. Therefore, physicians who followed up the patients throughout the study were blinded to the BKV DNA results during the follow-up. On the other hand, the results of the decoy cells were known. The BKV DNA was studied in the urine and blood samples of patients with positive decoy cells. Further evaluation and changes in the treatment of the patients with BKV were decided by the physician who followed up the patients. There were 4 such patients, and treatment modifications were made in these patients. Another limitation of the study was the relatively small number of patients.
In conclusion, we obtained important data about BKV infection, which is becoming a serious problem in transplant centers. Our study was conducted in a transplant center that performs mainly living donor transplantations, which is a different population than those described in previous works. In our cohort, screening with decoy cell examination might have contributed to lower rate of BKV infection. We believe that this information will be valuable in the diagnosis and follow-up of BKV infection.
Footnotes
Authors’ Note
A part of this study, with preliminary data, was presented at the 52nd ERA-EDTA Congress, London, 2015 (poster presentation).
Acknowledgments
The authors would like to thank Emine Ozel Cakır, nurse, Burhan Cagcag, medical biologist, and Hızır Sutlu, biologist, for their great help in data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: The present work was supported by Scientific Research Projects Coordination Unit of Istanbul University (project no 7821) and the Istanbul Branch of Turkish Society of Nephrology.