
Abstract
Introduction:
Maximizing education about living donor kidney transplant (LDKT) during the in-person evaluation at the transplant center may increase the numbers of kidney patients pursuing LDKT.
Research Questions and Design:
To test the effectiveness of a 1-time LDKT educational intervention, we performed a cluster-randomized trial among 499 patients who presented for evaluation of kidney transplant. We compared usual care education (n = 250) versus intensive LDKT education (n = 249), which was implemented only on the evaluation day and consisted of viewing a 25-minute video of information and stories about LDKT and discussion of LDKT possibilities with an educator. Our primary outcome was knowledge of LDKT, 1 week after the transplant evaluation.
Results:
One week after evaluation, patients who received intensive education had higher knowledge than patients who received usual care (12.7 vs. 11.7; P = .0008), but there were no differences in postevaluation readiness for LDKT. Among patients who had not previously identified a potential living donor, receiving intensive education was associated with increased willingness to take steps toward LDKT.
Discussion:
In conclusion, expansion of LDKT education within the evaluation day may be helpful, but interventions that are implemented at multiple times and for greater duration may be necessary to ensure larger and long-term behavioral changes in pursuit of LDKT.
Introduction
The best treatment for end-stage renal disease (ESRD) is usually a kidney transplant, with living donor kidney transplant (LDKT) preferable to deceased donor kidney transplant (DDKT) due to the better allograft and patient survival associated with LDKT. 1 Ideally, prior to evaluation, patients with ESRD, along with their family and friends who may consider serving as donors, would be educated about LDKT so that they are sufficiently informed about its advantages and disadvantages 2,3 and are prepared to ask questions. However, many patients come to transplant evaluation with very little knowledge of transplant. 4
At many centers, the bulk of transplant education occurs during half- or full-day transplant evaluation, when the transplant candidates appear in person to meet the transplant team. The evaluation usually includes a formal education presentation covering mandated topics, followed by meetings and discussions with nephrologists, surgeons, nurse coordinators, social workers, and other transplant providers. 5 –7 While comprehensive, this evaluation mainly focuses upon determining whether the patient is suitable for transplant and what further testing is required, rather than upon educating candidates about LDKT. Transplant providers may lack the time to discuss LDKT in detail or to address patients’ general fears about both transplant and LDKT. 8,9 After the evaluation, many transplant candidates remain unaware of basic facts regarding kidney transplant and live donation. 10
The recent American Society of Transplantation Best Practices in LDKT Consensus Conference recommended that patients receive culturally tailored education about LDKT as early as possible and at multiple stages in the transplant process. 11,12 For transplant centers, the most effective and efficient methods and mediums for educating potential transplant candidates about LDKT remain unknown. For many centers, expanding discussion about LDKT within the evaluation day itself would be helpful and feasible.
Thus, to test the efficacy of a pragmatic educational intervention, we designed and performed a cluster randomized controlled trial to test the effect of an expanded LDKT educational intervention, Enhancing Living Donor Kidney Transplant Education (ELITE), implemented within the transplant center, upon potential transplant candidates’ knowledge of transplant, readiness to pursue LDKT, and self-efficacy. The ELITE LDKT intervention included a 25-minute video about living donors’ experiences and a 1-on-1 meeting with a transplant educator to discuss LDKT in more detail.
Design/Methods
Study Design
The ELITE study was a single-center, cluster randomized, 2-arm parallel group randomized trial of 499 potential transplant candidates whose protocol has been described in detail elsewhere. 13 The protocol was registered on clinicaltrials.gov (NCT01261910) 14 and approved by the human subjects institutional review boards (IRBs) at Saint Barnabas Medical Center (SBMC) and Rutgers University.
Setting and Population
Study participants were recruited at the kidney transplant center located in suburban Livingston, New Jersey. Our inclusion criteria were that study participants had to (1) appear for initial kidney transplant evaluation at SBMC; (2) be ≥18 years old; (3) be able to provide informed consent; and (4) be able to speak, hear, and understand English. Our exclusion criteria were (1) significant neurocognitive disability that would prevent participants from understanding the study or completing the questionnaires; (2) inability to speak, hear, and understand English; (3) visual impairment and inability to complete self-administered questionnaires; and (4) self-described unwillingness or inability to complete phone questionnaires.
Enrollment and Randomization
Potential transplant candidates on a given evaluation day were cluster randomized to either the usual care (control or standard-of-care) arm or the intensive education (intervention) arm (evaluation day was the cluster unit). 13 Study personnel and participants were not blinded or masked regarding allocation groups. The study arm was unknown at the time the potential candidates scheduled their evaluations.
Usual Care (Control Arm)
Potential transplant candidates randomized to the standard-of-care (Usual Care) arm received the standard transplant education and evaluation. This education included an approximately 90-minute slide presentation, given by the transplant nurse coordinator, which provided education about kidney transplant, including LDKT. 13 After the presentation, potential transplant candidates were evaluated in an unsystematic order by a transplant nurse coordinator, social worker, nephrologist, dietician, and financial coordinator (if needed). The research nurse or assistant also met privately with each candidate to determine eligibility for the study, obtain informed consent, and administer the initial questionnaires.
Intensive Education (Intervention Arm)
Potential transplant candidates randomized to the intensive education arm underwent the same education and evaluations as the usual care patients. In addition, at the transplant evaluation, study participants in the intensive education arm viewed a video and then had an additional LDKT discussion with the research assistant or nurse (Transplant Educator).
First, study participants viewed “The experiences of living kidney donors,” a 25-minute video that was the third of 4 videos from the Explore Transplant series. 15,16 The video discusses how living donors came to their decision to donate; donors’ motivations and what they learned; facts about the donor evaluation, surgery, and recovery; risks to the living donors; and life after donation. We chose this video because of its relevance to transplant candidates being evaluated for transplant. The 2 earlier videos in Explore Transplant focus upon motivating patients with ESRD to pursue transplant and are less relevant to patients already attending the transplant evaluation. The fourth video in the series covered how to discuss living donation with potential donors, an explicit focus that was not permitted by the funding agency.
Second, after viewing the video, study participants met privately with the transplant educator for approximately 15 minutes to review LDKT fact sheets and brochures from Explore Transplant and ask questions about LDKT. 13 The transplant educator answered any questions that participants may have had based upon what they saw in the video; explored with participants their reasons for wanting a kidney transplant; explored with participants their current situation with chronic kidney disease (CKD) and ESRD; examined how the participants’ CKD/ESRD affects their family and friends; and answered any questions or concerns about transplant that the participant had. The viewing of the video and subsequent LDKT meeting with the transplant educator could occur at any point during the evaluation day after the 90-minute slide presentation seen by all transplant candidates.
Outcomes
This project’s funder, the Health Resources and Services Administration, stated that because of the risks associated with any major surgical procedure, projects could not attempt to increase the number of living donors. 17 Our study met the objective of the grant program by measuring knowledge of the benefits, risks, and process of LDKT (not living donor inquiries or LDKTs). In our study, the primary outcome was knowledge of LDKT, 1 week after the transplant evaluation. We did not measure transplant candidates’ baseline knowledge, prior to arriving at the transplant center and receiving transplant education.
Prespecified and post hoc secondary outcomes included readiness to pursue transplant and LDKT and willingness to take steps toward LDKT.
Measurements
Demographic and clinical characteristics
We collected participants’ demographic and clinical characteristics, including etiology of ESRD and whether the participant had identified a potential living donor prior to the start of the study.
Past education about transplant and LDKT
We also determined participants’ past education about transplant and LDKT. We also asked participants which of 8 educational actions (eg reading brochures about transplant) they had taken.
Health literacy
We measured participants’ health literacy and numeracy using the Newest Vital Sign (NVS), an instrument that requires in-person administration 18 as well as 3 validated single-item questions “How often do you have someone help you read hospital materials?” “How often do you have problems learning about your medical condition because of difficulty understanding written information?” and “How confident are you filling out medical forms by yourself?” 19
The LDKT knowledge
Knowledge of LDKT was measured using a 20-item questionnaire with 12 true-false and 8 multiple-choice questions administered over telephone. These items measured knowledge of key facts, risks, and benefits of transplant and LDKT.
Decision-making variables based upon the transtheoretical model
We collected decision-making variables using validated measures 20,21 that were based upon the transtheoretical model of behavior change. 22 These decision-making variables included stage of readiness and steps toward LDKT. The stages of readiness for LDKT and DDKT (separate measures for each) are precontemplation (not considering living/deceased donation in the next 6 months), contemplation (considering taking actions in the next 6 months to get a living/deceased donor transplant), preparation (preparing to take actions in the next 30 days to get a living/deceased donor transplant), action (LDKT: taking actions to get a living donor transplant, and DDKT: undergoing transplant evaluation to get a deceased donor transplant), and maintenance (DDKT only: listed and waiting to get a deceased donor transplant).
The LDKT-related actions
We assessed at 1 week postevaluation whether participants had asked a family member or friend to consider donating a kidney (yes/no). We also asked whether participants were willing to take any of 6 steps toward LDKT at 1 week (yes/no; eg, Share my need for a living donor with a large community through a general announcement).
Statistical Analysis
Power analysis and sample size determination
With 250 participants in each study arm, using a 2-sample t test with type 1 error of .05, and a conservative intraclass correlation (ICC) of 0.40, the study had over 95% power to detect 10% to 20% higher transplant knowledge between study arms at 1 week.
Outcomes analyses
To determine whether randomization resulted in equal distributions in the 2 study arms, we compared frequencies, means, and medians for baseline variables, between the usual care and intensive education arms. We calculated the ICC to determine the extent of clustering within date of the evaluation day.
We compared knowledge (the primary outcome) for LDKT and DDKT, at 1 week between the usual care and intensive education arms, using the analysis of covariance models that adjusted for out-of-balance baseline measures. The independent variable was the assigned study arm (usual care or intensive education). We also examined this outcome stratified by race to determine whether there was heterogeneity of treatment effect. For transplant knowledge, the observed ICC was small at .05, so primary analyses did not account for clustering, although sensitivity analyses using multilevel regression models with a random intercept for class date were examined. Our main analysis used an intent-to-treat approach. To permit inclusion of all enrolled study participants, even those with missing data, we also used multiple imputation for sensitivity analyses. 23 We also compared the odds of being in later stages of LDKT and DDKT readiness between the control and intervention arms and of willingness to take LDKT-related actions at 1 week, using multivariable logistic regression models adjusting for out-of-balance baseline measures. To determine whether willingness to take these actions was greater among participants who were earlier in the process of pursuing LDKT, we conducted a subanalysis of differences in these steps between study arms only among participants who had no previous matching living donor.
Results
Participant Screening
From December 2010 to June 2012, during 211 separate evaluation days (clusters), 766 patients appeared for transplant evaluation at our center (Figure 1), of whom 99 (12.9%) were ineligible and 168 (21.9%) refused participation in the study, leaving 499 (65.1%) patients who consented to participate. The participation rate was 68.5% in the usual care arm versus 62.1% in the intensive education arm (P = .06).
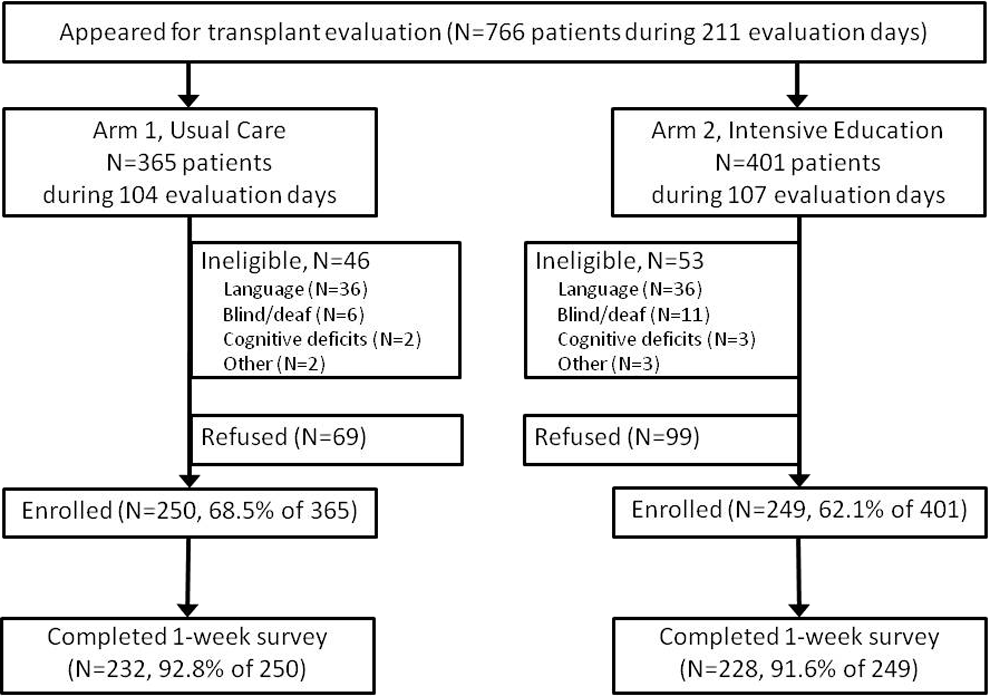
Patient flow through screening and enrollment.
Baseline Characteristics
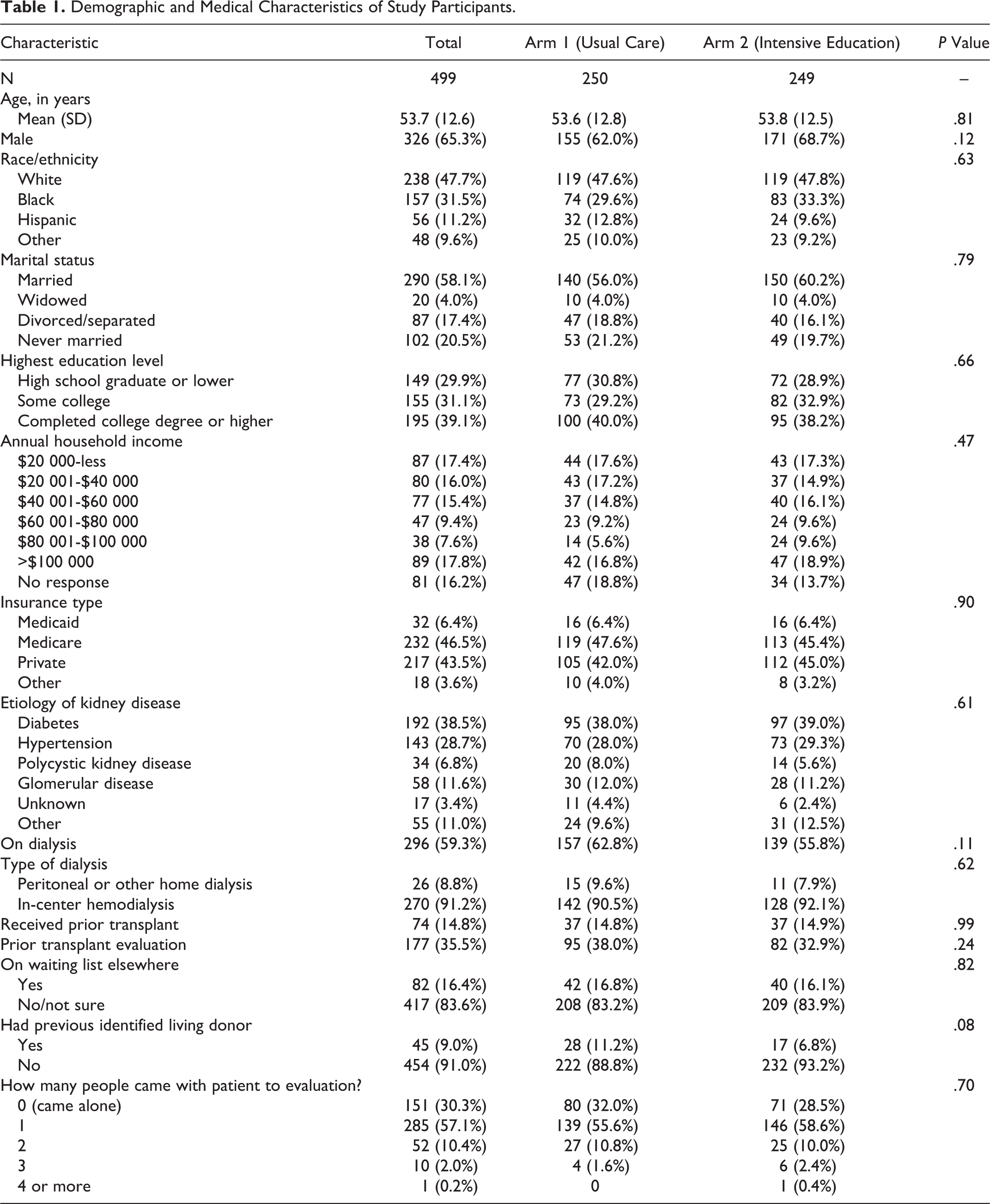
No significant differences in baseline demographic and medical characteristics were observed between the study arms (Table 1). Among the full sample, the largest proportion of participants identified diabetes as their etiology of kidney disease (38.5%), were on dialysis (59.3%), and had not received a transplant in the past (85.2%; Table 1). Most had not previously identified a potential living donor (91.0%), and most attended the evaluation with one other person (57.1%).
Demographic and Medical Characteristics of Study Participants.
Regarding baseline health literacy and previous transplant education, most participants were extremely confident filling out medical forms by themselves (58.6%) and had the highest score category (4-6) on the NVS (75.2%; Table 2). Most participants recalled receiving previous recommendations from a kidney doctor to call a transplant center to be evaluated (78.2%) and to talk to family or friends to see if someone might be a living donor (67.8%). Prior to evaluation, most participants had read brochures about transplant (72.3%) and living donation (53.7%) and talked to family and friends about getting a transplant (60.7%;Table 2). The study arms did not differ on these characteristics except for their scores on the NVS and their confidence in filling out medical forms (Table 2). In subsequent analyses, all P values and odds ratios were adjusted for these 2 health literacy variables.
Baseline Health Literacy and Past Learning Behaviors.
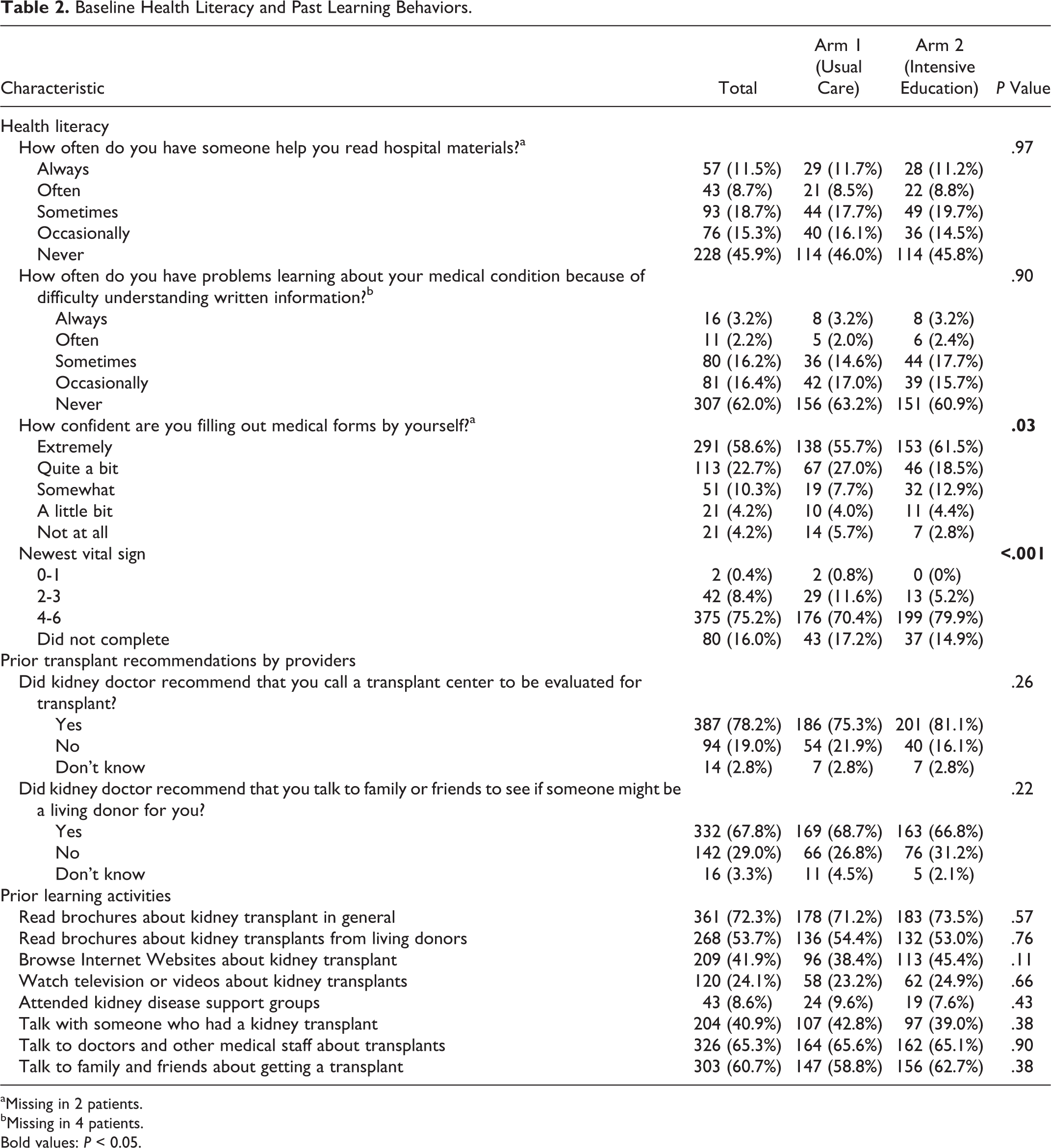
aMissing in 2 patients.
bMissing in 4 patients.
Bold values: P < 0.05.
Transplant Knowledge and Readiness at 1 Week
One week postevaluation, in the full sample, the mean level of knowledge was 12.1 questions correct of 20 total questions, ranging from 3 to 20 correct. Sixty percent of participants were in later stages of readiness for DDKT and 82.4% reported being willing to accept a DDKT. Regarding LDKT, 45.5% were in later stages of readiness, 89.2% said they would be willing to accept an LDKT, and 46.3% had asked a friend or family member to consider donating a kidney.
One week after evaluation, the level of transplant knowledge was greater for participants in the intensive education arm versus the usual care arm (12.7 vs 11.7 questions answered correctly; P = .002; Table 3). The P value is adjusted for differences in the NVS and confidence in filling out medical forms. Regarding DDKT attitudes, there were no differences between the study arms in DDKT readiness or willingness to accept a DDKT. Regarding LDKT attitudes, there were no differences between the study arms in LDKT readiness, willingness to accept a LDKT, or readiness to ask a family member or friend to donate a kidney (Table 3).
Differences in Transplant Knowledge, Readiness, and Attitudes at 1 Week Post Baseline by Educational Condition.
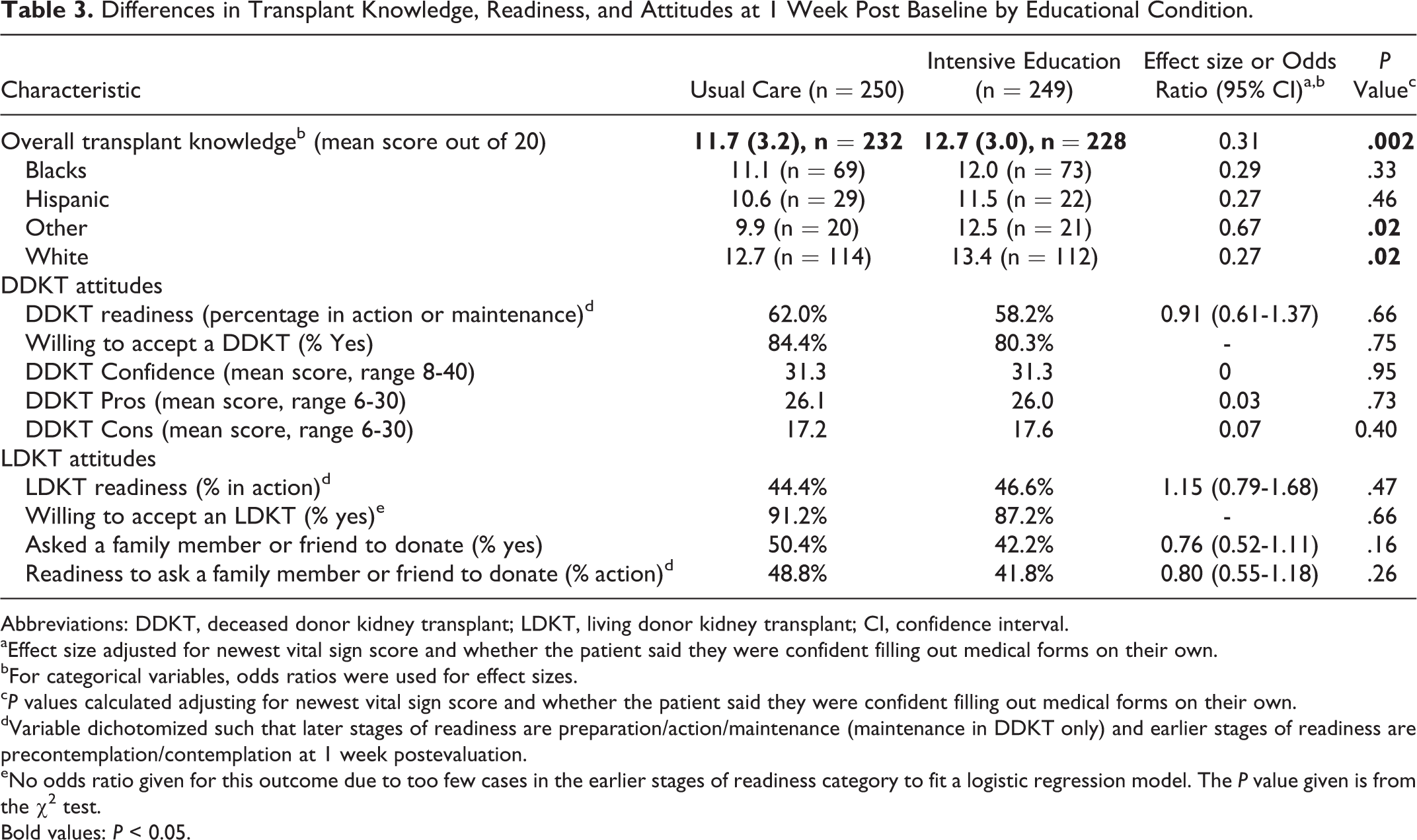
Abbreviations: DDKT, deceased donor kidney transplant; LDKT, living donor kidney transplant; CI, confidence interval.
aEffect size adjusted for newest vital sign score and whether the patient said they were confident filling out medical forms on their own.
bFor categorical variables, odds ratios were used for effect sizes.
c P values calculated adjusting for newest vital sign score and whether the patient said they were confident filling out medical forms on their own.
dVariable dichotomized such that later stages of readiness are preparation/action/maintenance (maintenance in DDKT only) and earlier stages of readiness are precontemplation/contemplation at 1 week postevaluation.
eNo odds ratio given for this outcome due to too few cases in the earlier stages of readiness category to fit a logistic regression model. The P value given is from the χ2 test.
Bold values: P < 0.05.
Actions Toward LDKT at 1 Week
At 1 week postevaluation, the steps that participants were willing to take toward getting an LDKT varied, with 84.2% willing to accept someone’s offer to donate, 74.5% willing to allow others to tell people that they would be willing to pursue living donation, and 64.7% willing to generally talk to people about their interest in transplant to see if living donor volunteers come forward. However, only 37.1% were willing to send a letter or e-mail to explore potential interest in living donation to important people in their life. Intensive education participants were more likely to be willing to share their need for a living donor through a general announcement (P = .03) but less likely to ask potential donors to be tested (P = .03).
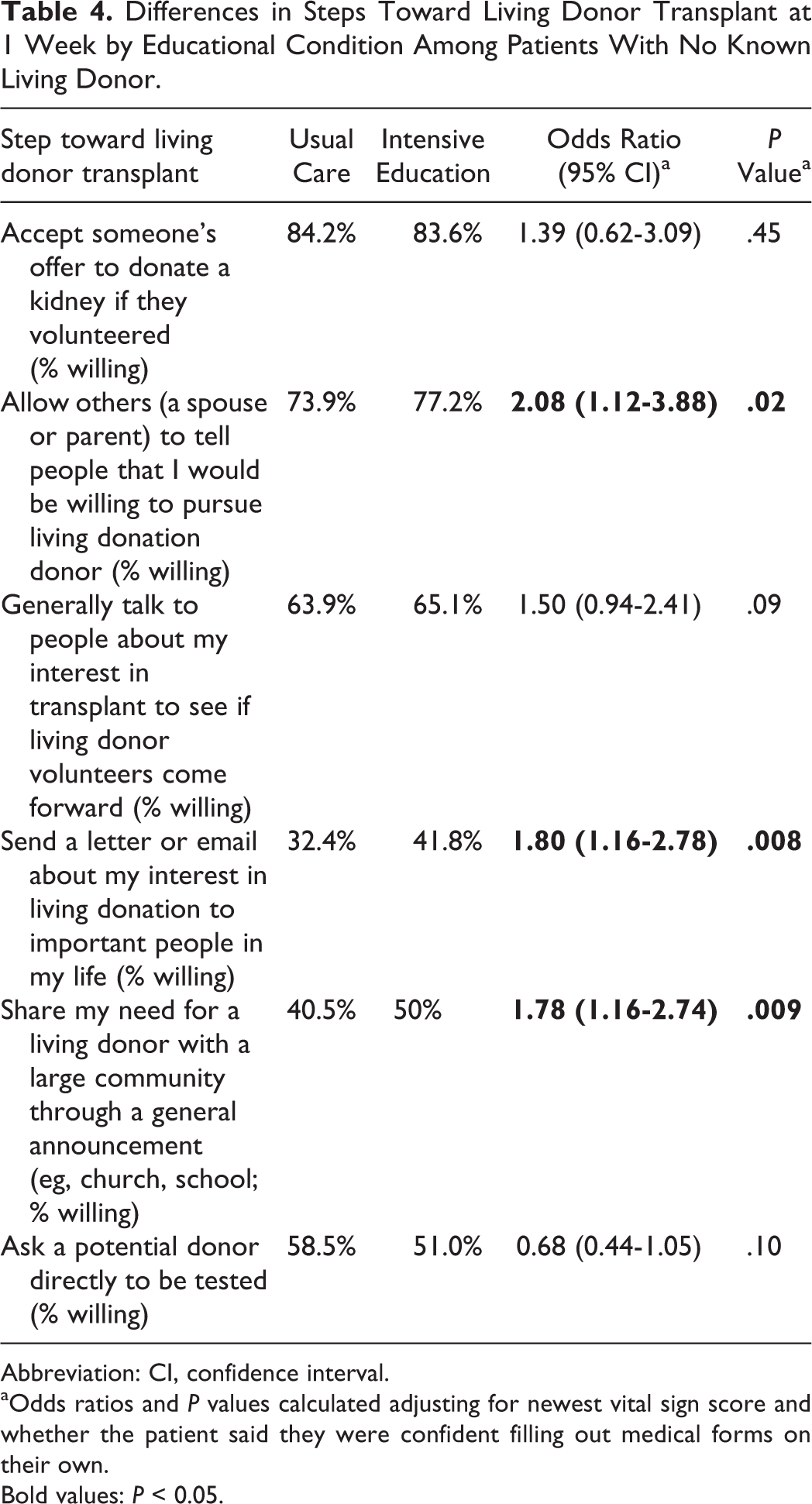
In the subset of study participants who had not previously identified a living donor (n = 454), participants in the intensive education were 1.75 to 2 times more likely to be willing to allow others to tell people the participant would pursue living donation, send a letter or e-mail about their interest in living donation to important people in their life, and share their need for a living donor with a large community (Table 4).
Differences in Steps Toward Living Donor Transplant at 1 Week by Educational Condition Among Patients With No Known Living Donor.
Abbreviation: CI, confidence interval.
aOdds ratios and P values calculated adjusting for newest vital sign score and whether the patient said they were confident filling out medical forms on their own.
Bold values: P < 0.05.
Conclusions
In this single-center, cluster randomized trial, we found that compared to usual care, intensive education, consisting of viewing a video and discussing LDKT with an educator, was associated with higher transplant knowledge 1 week later. The expanded LDKT education in intensive education helped study participants who had not recruited a living donor to increase their willingness to take steps toward LDKT, including allowing others to tell people the patients would be willing to pursue living donation, sending a letter or e-mail to others about their interest in living donation, and sharing their need for a living donor with a large community. However, participants receiving intensive education, versus usual care, were not significantly different in their readiness regarding LDKT at this time.
This study provides useful data on transplant candidates’ prior education and learning about transplant before their evaluation, along with their knowledge and readiness, regarding transplant and LDKT after their evaluation. Before the evaluation, most of the candidates in our study had already read brochures, talked to doctors, or talked to family and friends about transplants. This finding contrasts other studies which have found that dialysis and other pretransplant patients with CKD receive very little education about transplant before they arrive at the transplant center. 4,24,25 The participants enrolled in this trial may have been more prepared for transplant and LDKT than most patients starting the transplant evaluation process.
Despite our participants’ prior education about transplant, there were nevertheless important opportunities to improve their knowledge of transplant and LDKT. The intensive education arm had a significantly higher mean knowledge score at 1 week postevaluation when compared to the usual care arm. The effect size of this increase, however, was modest at 0.31 and likely had little clinical significance, despite being statistically significant. Future interventions should aim to elicit even larger increases in transplant and LDKT knowledge.
Other interventions among transplant candidates have also resulted in increases in transplant knowledge. Rodrigue et al reported that a house call by a transplant educator, a group-based session, and individual counseling each increased transplant knowledge, 1 week later, by 3.0 points or less on a 16-point scale. 26 In another study, a culturally sensitive video and booklet that were implemented at the transplant evaluation increased transplant knowledge, when compared to baseline, by <0.5 points on an 18-item, true-false index of knowledge. 27 A recent study found that Hispanic and Latino patients with CKD who viewed, on the day of their transplant evaluation, a culturally targeted Website for 30 minutes had 10% greater knowledge versus a control arm 3 weeks after the intervention, based upon a 31-item test. 28
Our findings and the results of other trials suggest that learning about LDKT can be improved through expansion of LDKT education within transplant centers. However, interventions that create larger and lasting increases in transplant knowledge may require more tailored interventions based on patients’ stage of readiness to pursue transplant, participation by family and friends (as with home-based interventions), repeated contacts between the transplant candidate and transplant center (rather than a 1-time intervention), use of other providers such as social workers, 29 and interactions with actual transplant recipients and living donors (rather than viewing a static video). Future studies should continue to examine interventions in other settings (eg, dialysis centers and nephrologists’ offices) and at other times (eg, after placement on the waiting list), using different educational delivery methods (eg, online, by telephone).
Our study has several limitations. First, although knowledge and readiness regarding LDKT are important, outcomes such as LDKT and living donor inquiries are likely more relevant and have been measured in other intervention studies. 26,30 Restrictions by this study’s funding agency, however, preclude us from reporting these clinically relevant outcomes. 17
Second, we lacked baseline measurements of transplant knowledge and attitudes, made prior to the start of the transplant evaluation day. Logistically, we were unable to obtain informed consent and administer a baseline questionnaire prior to the start of our transplant education on evaluation days. Future studies should include baseline measurements of patient-reported outcomes as well as relevant outcomes that are not patient reported (eg, receipt of LDKT and living donor inquiries).
Finally, this trial occurred at a single, high-volume, suburban kidney transplant center in the northeastern United States that may differ from lower-volume centers in its practices and processes. These intercenter differences may conceivably impact the effectiveness of an educational intervention.
In conclusion, a 1-time intervention consisting of a video and meeting with a transplant educator was associated with slightly increased knowledge about LDKT versus a comparison control condition. These results, together with the results from other similar interventions and recommendations from the recent Consensus Conference on Best Practices in Living Kidney Donation, suggest that repeated education in multiple settings outside the transplant center may be required to ensure that patients and their prospective living donors are fully informed about LDKT and living donation.
Footnotes
Authors’ Note
This manuscript’s contents are solely the responsibility of the authors and do not necessarily represent the official views of the Division of Transplantation, Health Resources and Services Administration, US Department of Health and Human Services. Preliminary results were presented in part at the World Transplant Congress, July 2014, in San Francisco, California.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described was supported by grant R39-OT15059 from the Division of Transplantation, Health Resources and Services Administration, US Department of Health and Human Services.