
Abstract
Purpose:
Living kidney donation is safe and effective, but patients in need of a transplant continue to outnumber donors. Disincentives to living donation include lost income, risk of job loss, perioperative complications, and unreimbursed medical expenses.
Methods:
This study uses US registry and follow-up data on living kidney donors from 2013 to 2015 to identify social predictors of return to work across gender following living kidney donation.
Results:
Using logistic regression, we find that predictors of return to work following living kidney donation differ for women and men. Among women, age, education, smoking status, and procedure type are associated with return to work. Among men, education, procedure type, and hospital readmission within 6 weeks postdonation are associated with return to work. Notably, single and divorced men are less likely to return to work compared to married men (odds ratio [OR] for single men 0.51, 95% confidence interval [CI], 0.37-0.69, P < .001; OR for divorced men 0.51, 95% CI, 0.34-0.75, P = .006). Marital status is not associated with return to work for women. Single and divorced men’s greater odds of not returning to work are robust to controls for relevant pre- and postdonation characteristics.
Conclusions:
Single and divorced men’s lack of social support may present an obstacle to work resumption following living kidney donation.
Introduction
A kidney transplant is an important treatment option for end-stage renal failure. 1 Living kidney donation is a safe and effective alternative to transplanting scarce deceased donor organs. 2 In the United States, 5628 (31%) of 17 878 kidney transplants performed in 2015 involved living donation. 3 Although transplant centers screen living donors for healthy physical status and adequate social support, 4 living donors nevertheless experience significant disruptions to their usual activities in the months following donation. 5,6 One of the most important disruptions is to living donors’ paid work participation. Prior studies find that many previously employed donors return to work between 6 weeks and 3 months following the initial surgery, 7 yet there is also evidence that living donors have higher rates of unemployment than the general population following transplantation. 8,9
An inability to return to work after donation is likely to create financial strain for donors, resulting in difficulty paying for unreimbursed medical costs and lost income in the postdonation period. 5 In turn, these consequences may disincentivize living donation, 10 limiting the number of kidney transplants that can be performed. Men and women differ in their workforce participation, 11 but prior studies have not considered whether predictors of return to employment after donation differ between men and women. The primary goal of this study was to identify social predictors of return to work following living kidney donation, and the secondary goal was to understand whether these predictors were consistent across genders.
Methods
Data and Sample
The study was deemed exempt from review by the local institutional review board. Data were obtained from the United Network for Organ Sharing (UNOS), which manages the registry of all living donors in the United States. Transplant centers report donor registration and follow-up data to the Organ Procurement & Transplant Network (OPTN) via a secure, Internet-based system. 12 Data were obtained at the time of living donor registration as well as from follow-up reports scheduled at 6 months, 1 year, and 2 years after donation. 13 Donor follow-up was censored at June 2016 in the available data. Living donors from 2013 to 2015 were evaluated for inclusion in the analysis. Exclusion criteria, detailed in Figure 1, were age <18 or >64 years at donation, donation to a spouse, anonymous donation, residence in US territories, not working for income at the time of donor registration, widowed marital status at donation (due to small sample size), and lack of follow-up data. 14 Finally, 2 donors were excluded due to postoperative mortality.

Exclusion criteria flow diagram.
Measures and Analysis
The primary outcome was the return to paid employment as reported by transplant centers during the donor’s most recent follow-up (scheduled for 6 months, 1 year, and 2 years posttransplant). As illustrated in Figure 1, all donors in the sample worked for income prior to donation so that all donors could have plausibly returned to a job they held before donation. Logistic regression models stratified by gender were fitted to evaluate the associations between social variables, clinical characteristics, and return to employment following living donation. 15 A fully interacted model was fitted to the pooled sample to test for gender differences in model coefficients. 16 Covariates assessed at the time of donation included marital status (married, divorced, and life partner), age, race/ethnicity (white, black, Latino, and Other), educational attainment (less than high school, high school, some college, and college degree), functional limitation (requiring assistance with daily activities), body mass index (BMI), current or prior smoker, hypertension, estimated glomerular filtration rate (eGFR, a measure of kidney function calculated using Modification of Diet in Renal Disease equations), and surgical technique (open, hand-assisted laparoscopic, non–hand-assisted laparoscopic). 17 Models also controlled for readmission within the 6 weeks after donation. State-level random effects were included to adjust for residual differences in donors’ likelihood of returning to work across the 50 US states and the District of Columbia. Data analysis was performed using Stata/MP 14.2 (StataCorp LP, College Station, Texas), and P < .05 was considered statistically significant.
Results
Table 1 includes descriptive statistics for all model variables across gender and return to work. For both men and women, return to work was common: 93% were employed by the most recent follow-up. For both men and women, return to work varied by educational attainment, smoking status, and procedure type. Among male donors, return to work also varied by marital status, race ethnicity, eGFR, hypertension, insurance status, and hospital readmission.
Descriptive Statistics for all Variables by Gender and Return to Work Status.a
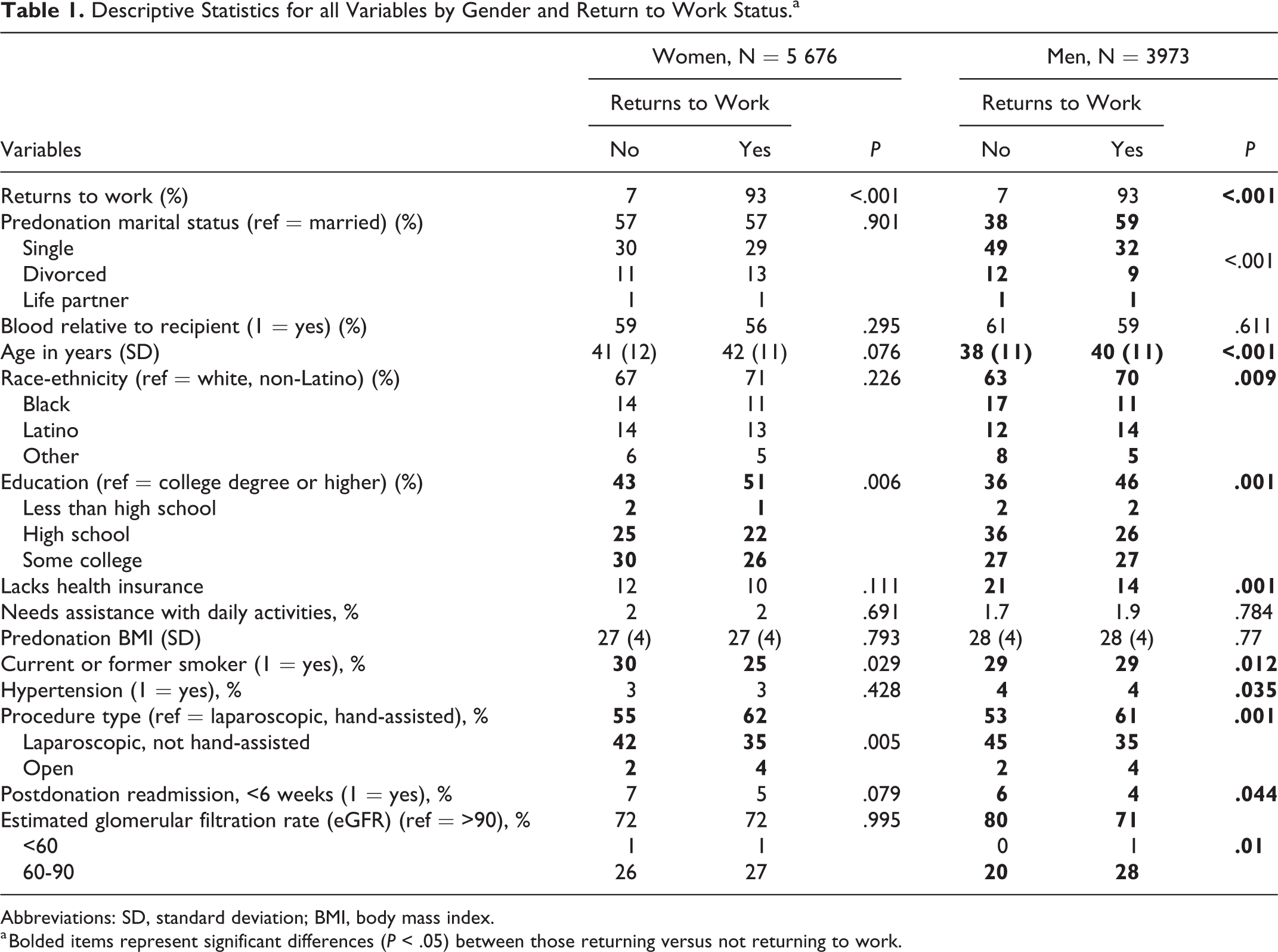
Abbreviations: SD, standard deviation; BMI, body mass index.
a Bolded items represent significant differences (P < .05) between those returning versus not returning to work.
In Table 2, logistic regressions estimated odds ratios (ORs) of return to work across social and clinical characteristics. Notably, among women, return to work did not vary by marital status. Among women, older donors were more likely to return to work (OR = 1.01, confidence interval [CI], 1.00-1.02, P = .007), and women with less than a high school degree (OR = 0.40, CI, 0.20-0.81, P = .011) or some college (OR = 0.77, CI, 0.60-0.97, P = .025) were less likely to return to work than the college educated. Also, female smokers were less likely to return to work (OR = 0.78, CI, 0.62-0.98, P = .033) as were women undergoing an open surgical procedure relative to a non–hand-assisted laparoscopic procedure (OR = 0.73, CI, 0.56-0.95, P = .018).
Multivariate Logistic Regressions of Return to Work by Gender.
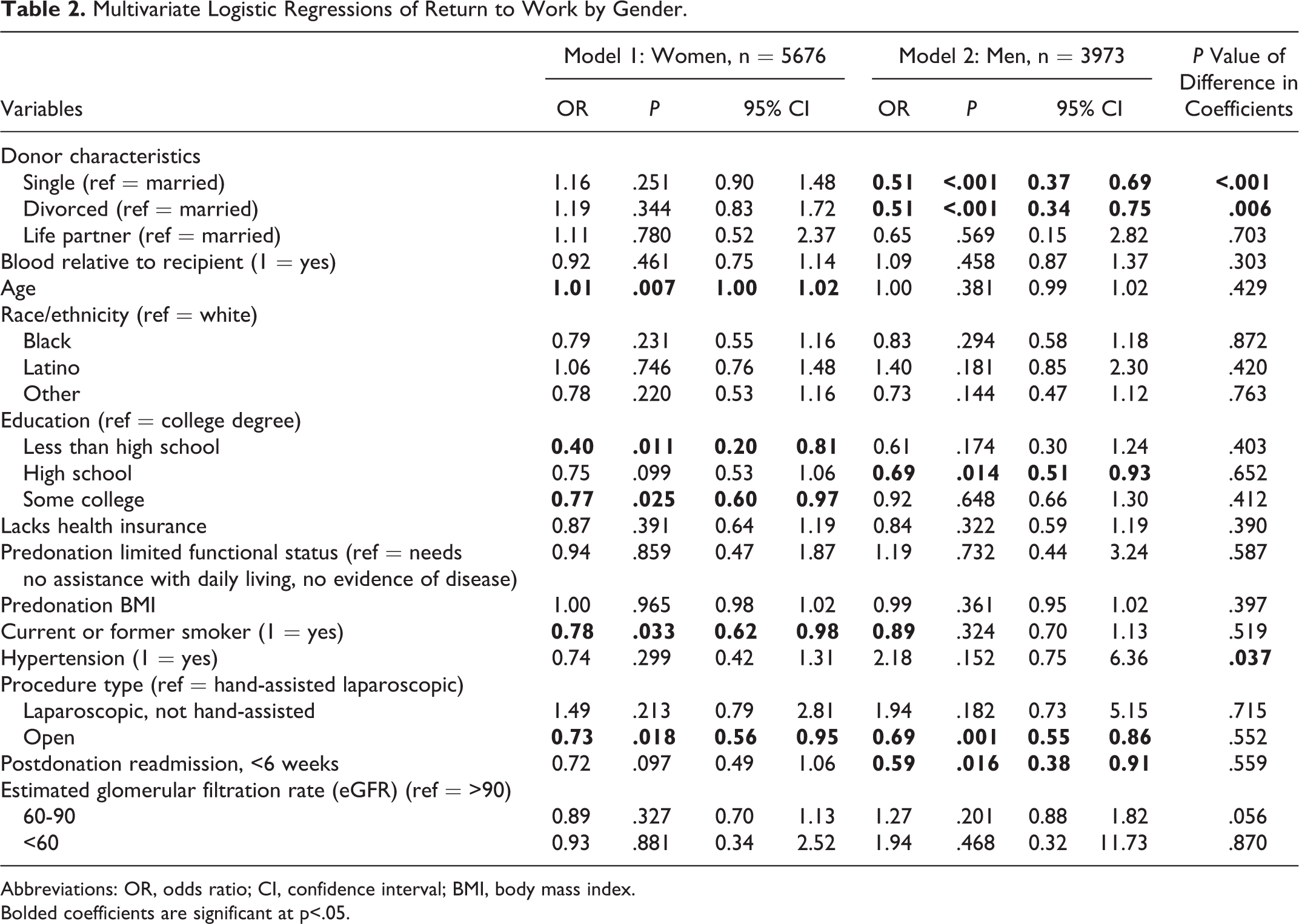
Abbreviations: OR, odds ratio; CI, confidence interval; BMI, body mass index.
Bolded coefficients are significant at p<.05.
Among male donors, the single (OR = .51, CI, 0.37-0.69, P < .001) and the divorced (OR = 0.51, CI, 0.34-0.75, P < .001) were less likely to return to work than married men. These ORs were significantly different from the corresponding estimates in the subsample of women as determined in the fully interacted model (P < .001 and P = .006, respectively). Men with a high school degree were less likely to return to work relative to college educated men (OR = 0.69, CI, 0.51-0.93, P = .016) as were men undergoing an open surgical procedure (OR = 0.69, CI, 0.55-0.86, P = .001) and men readmitted to the hospital within 6 weeks following donation (OR = 0.59, CI, 0.38-0.91, P = .016). However, apart from marital status, no statistically significant correlates of return to work exhibited different magnitudes of association with this outcome according to gender.
Discussion
Living donation is essential for increasing the availability of donor kidneys but disruptive to the donor’s usual activities, particularly employment. To understand what clinical and social characteristics put donors at risk of delaying or foregoing work after donation, we examined return to work among donors who had been working at the time of donation. Many of our findings were consistent with prior research. The high rate of return to work in this sample was consistent with studies showing few or no long-term impacts of living donation on donors’ health and social lives. 18,19 We also found that undergoing an open surgical procedure was associated with a reduced likelihood to return to work, consistent with prior studies noting differences in recovery rates by surgical technique. 7,17 We advanced existing literature on this topic by showing that for men and not for women marital status was an important predictor of postdonation employment. Specifically, male donors who were single or divorced returned to work less often than men who were married, even after controlling for race, educational attainment, baseline health status, and postdonation readmissions.
Our findings suggest that being single or divorced presents obstacles to resuming usual activities (particularly employment) that are unique to male donors. Prior research shows that men’s social networks tend to be smaller than women’s, especially in the absence of a spouse. 20 For men, the lower likelihood to return to work among the single and divorced may also be a reflection of men’s lack of health literacy, 21 general lack of healthy behaviors, or an increase in postoperative depressive symptoms that may lead to harmful gender-specific coping (eg, substance abuse). 22 As such, single and divorced men may lack both emotional support postsurgery and instrumental help with daily activities, compared to their married peers. This may be exacerbated by a higher rate of perioperative complications among male when compared to female donors as described in a recent study. 17 Unfortunately, the UNOS registry lacks sufficiently detailed data to compare coping behaviors and use of social support across gender and marital status in order to evaluate whether these factors mediate marital status differences in return to work after donation.
Despite the strengths of using a national transplant registry in this study, our conclusions are limited by some aspects of the data and analysis. First, follow-up data could not be obtained for 16.3% of living donors. 13 Second, little detail was available about the donor’s employment, so we could not differentiate return to work according to pretransplant occupation, work hours, or income. Third, the measure of marital status was only available at the time of donation. Fourth, we cannot make precise estimates of the timing of return to work. Most donors able to return to work after living donation do so within 3 months 23 ; by comparison, UNOS follow-ups of living donors were scheduled for 6, 12, and 24 months following surgery.
The present study describes social and clinical predictors of return to work among living kidney donors. Given the disruption that living donation presents to a donor’s employment, family, and health status, and given the significant need for living kidney donors, it is imperative to implement best practices to optimize postoperative clinical and social outcomes for donors. Previously recommended interventions for minority donors 24 —including increasing donors’ health literacy, assisting eligible donors in applying for financial assistance, ensuring longer term follow-up care for donors, and strengthening the ties between transplant centers and donors’ local community organizations—may also offer important benefits to unmarried donors and other donors with limited sources of social support. Single and divorced men may be a previously unidentified group in need of greater support following living kidney donation, and meeting these needs can help to improve postsurgical outcomes and increase the pool of living donors.
Footnotes
Authors’ Note
The data reported here have been supplied by the United Network for Organ Sharing as the contractor for the Organ Procurement and Transplantation Network (OPTN). The interpretation and reporting of these data are the responsibility of the authors and in no way should be seen as an official policy of or interpretation by the OPTN or the U.S. Government.
Authorship
AF designed the study, acquired the data, performed the analysis, and drafted the manuscript. VN and DH interpreted the results and critically revised the manuscript. DT participated in study design and data acquisition, interpreted the results, and critically revised the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.