
Abstract
Introduction:
Recipient travel distance may be an unrecognized burden in lung transplantation.
Design:
Retrospective single-center cohort study of all adult (≥18 years) first-time lung-only transplants from January 1, 2010, until February 28, 2017. Recipient distance to transplant center was calculated using the linear distance from the recipient’s home zip code to the Cleveland Clinic in Cleveland, Ohio.
Results:
569 recipients met inclusion criteria. Posttransplant graft survival was 85%, 88%, 91%, and 91% at 1 year and 49%, 52%, 57%, and 56% at 5 years posttransplant for recipient travel distances of ≤50, >50 to ≤250, >250 to ≤500, and >500 miles, respectively (P = .10).
Discussion:
We found no significant relationship between recipient travel distance and posttransplant graft survival. In carefully selected recipients, travel distance is not a significant barrier to successful posttransplant outcomes which may be important for patient decision-making and donor allocation policy. These data should be validated in a national cohort.
Keywords
Introduction
Recipient travel distance from home to transplant center may be an unrecognized burden in lung transplant. The continuum of transplant care includes repeated travel for pretransplant evaluation appointments, appointments while wait-listed, travel for the transplant operation, and travel for lifelong posttransplant visits. In 2016, there were 77 lung transplant centers in the United States, with annual center volumes ranging from 3 to 113 transplants per year. 1 As a result, patients with end-stage lung diseases traveled varying distances to reach one of the few lung transplant centers. Additionally, some patients may bypass the nearest center to reach a more distant center with the capacity to offer transplant services for their more complex medical comorbidities.
Considerations are being given to broader geographic sharing of donor allografts to increase patient access in liver, kidney, and heart transplantation. 2 –4 These considerations may be applicable to lung transplant, but with increased patient access, recipient travel may also increase. The impact of travel distance on post–lung transplant graft survival is not fully understood and is the focus of our study. We hypothesized that recipient travel distance did not impact post–lung transplant graft survival.
Methods
We performed a retrospective single-center cohort study of all adult (≥18 years) first-time, lung-only, transplants from January 1, 2010, until February 28, 2017. Clinical data were collected through June 30, 2017, ensuring all patients had at least 4 months of follow-up. Retransplants, multi-organ transplants, and recipients hospitalized at the time of transplant were excluded.
Native lung diseases were grouped according to United Network for Organ Sharing defined categories: restrictive (primarily idiopathic pulmonary fibrosis), obstructive (primarily chronic obstructive pulmonary disease), cystic (primarily cystic fibrosis), and vascular (primarily pulmonary hypertension). The Lung Allocation Score at the time of transplant was used. The primary outcome was posttransplant graft survival, defined as time from lung transplant until patient death or retransplant.
Data Collection
The data were abstracted through the Cleveland Clinic Electronic Data Interface for Transplant, which contains demographic and clinical outcomes data. This study was approved by the institutional review board of Cleveland Clinic.
Recipient Travel Distance
Recipient distance to transplant center was calculated using the linear distance in miles from the recipient’s home zip code to the Cleveland Clinic in Cleveland, Ohio, and categorized either as ≤50 miles, >50 to ≤250 miles, >250 to ≤500 miles, or >500 miles. Our center policy is that nonhospitalized wait-listed patients are seen every 3 months in outpatient clinic in Cleveland, Ohio. Patients may live at home while waitlisted if they live within 1000 nautical miles (1150 miles) of Cleveland, Ohio. For patients who live ≥4-hour driving distance from Cleveland, they travel by air ambulance at the time of transplant. After transplant, recipients must remain within 1-hour driving distance of the Cleveland Clinic for an average of 6 to 8 weeks after hospital discharge prior to returning home. During the first 2 years after transplant, posttransplant outpatient care occurs every 3 to 4 months in Cleveland, Ohio and can be more frequent at the discretion of the clinician. One year after transplant, recipients may transfer care to another transplant center; however, our center continues to follow and record graft survival.
Socioeconomic Status
To capture socioeconomic status, we assessed the median income in US dollars for each zip code using national census data. We also examined the type of insurance recipients reported at the time of transplant.
Statistics
Summary statistics including counts and percentages for categorical variables and means and standard deviations for continuous variables were used to describe the study cohort. Wilcoxon tests were used for comparing continuous variables and χ2 tests for categorical variables. Kaplan Meier and Cox proportional hazard models were used. Two-sided P values of .05 or less were considered significant. Data were analyzed with SAS ( version 9.4; SAS Institute, Cary, North Carolina).
Results
There were 569 recipients who met inclusion criteria. Sixty-eight patients were inpatient at the time of transplant and were excluded. Table 1 shows baseline categorical and continuous results, respectively. No significant differences among the 4 distance categories were identified by gender, age, race, single versus bilateral transplant, body mass index, insurance type, or blood type. The most common indication for lung transplant was restrictive lung disease. Wait-list time, hospital length of stay after transplant, episodes of acute rejection, and number of posttransplant readmissions were also not impacted by recipient travel distance. The number of recipients with prior heart valve surgery pretransplant or who transferred their care to another transplant center increased significantly with increased travel distance. The allocation score at the time of transplant and posttransplant intensive care unit (ICU) length of stay was significantly different between the 4 different distance categories. Donor characteristics were similar across the 4 recipient distance groups, though we note a trend toward decreasing use of donation after cardiac death donors with increasing recipient travel distance. In assessing socioeconomic status, recipients traveling >500 miles were signficantly more likely to have private insurance and live in a zip code with a higher median income than recipients traveling ≤50 miles.
Clinical Characteristics.
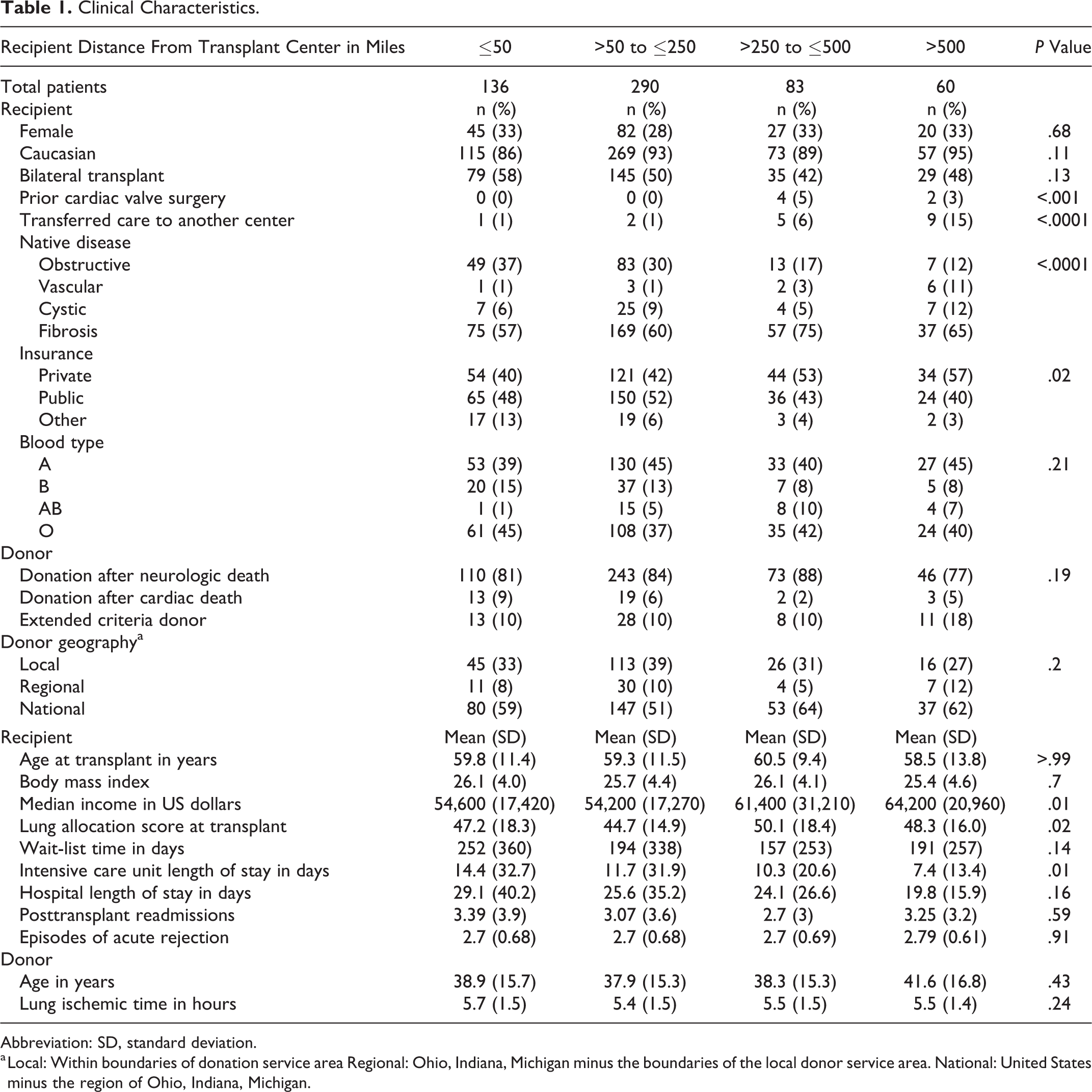
Abbreviation: SD, standard deviation.
a Local: Within boundaries of donation service area Regional: Ohio, Indiana, Michigan minus the boundaries of the local donor service area. National: United States minus the region of Ohio, Indiana, Michigan.
Posttransplant graft survival was 85%, 88%, 91%, and 91% at 1 year and 49%, 52%, 57%, and 56% at 5 years posttransplant for travel distances of ≤50, >50 to ≤250, >250 to ≤500, and >500 miles, respectively (Figure 1). In the multivariable Cox model, travel distance to transplant center was not associated with 1 year posttransplant graft survival (Table 2).
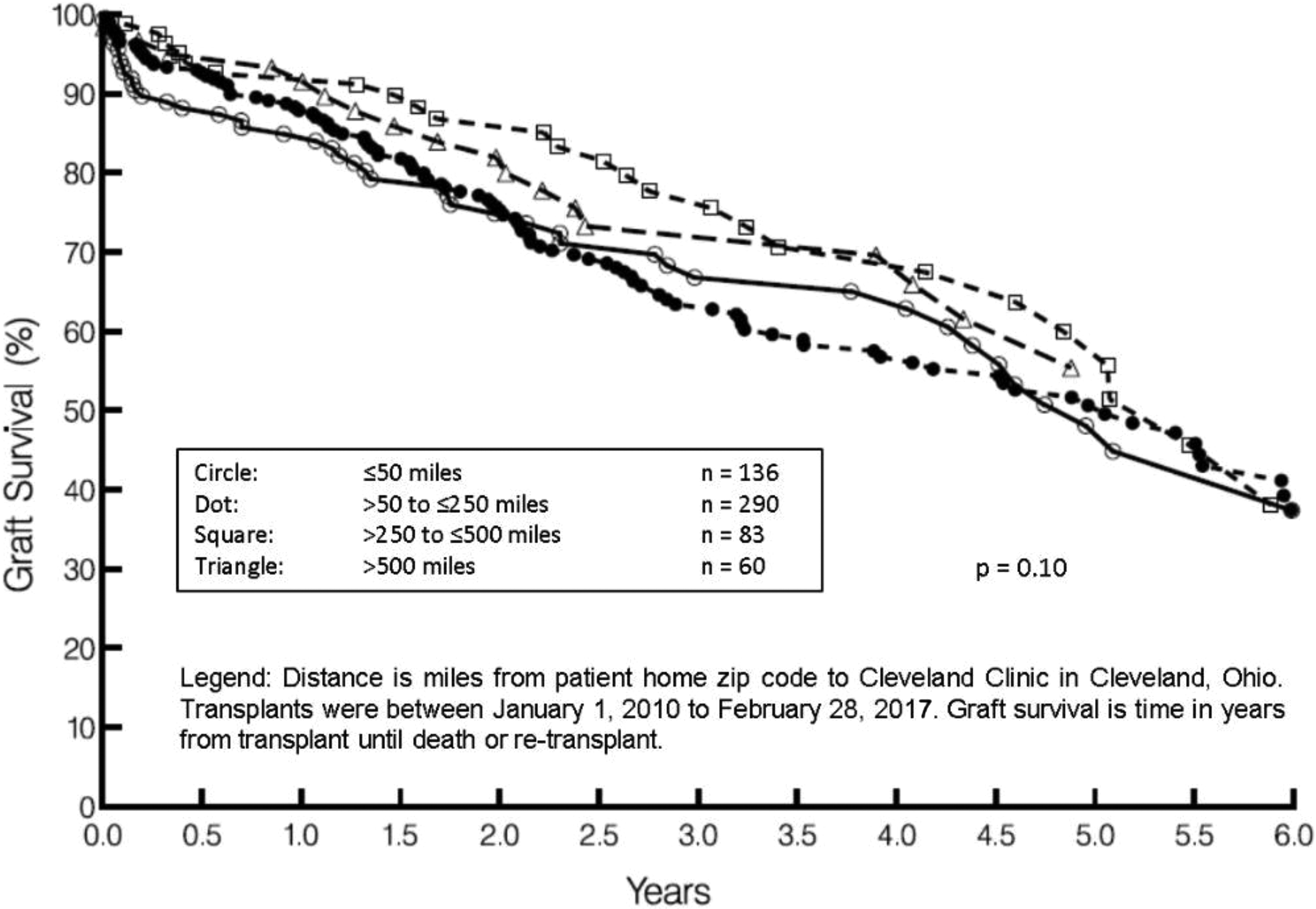
Kaplan-Meier posttransplant graft survival by distance (miles) from transplant center.
Hazard Ratios of Distance From Transplant Center and Clinical Characteristics.
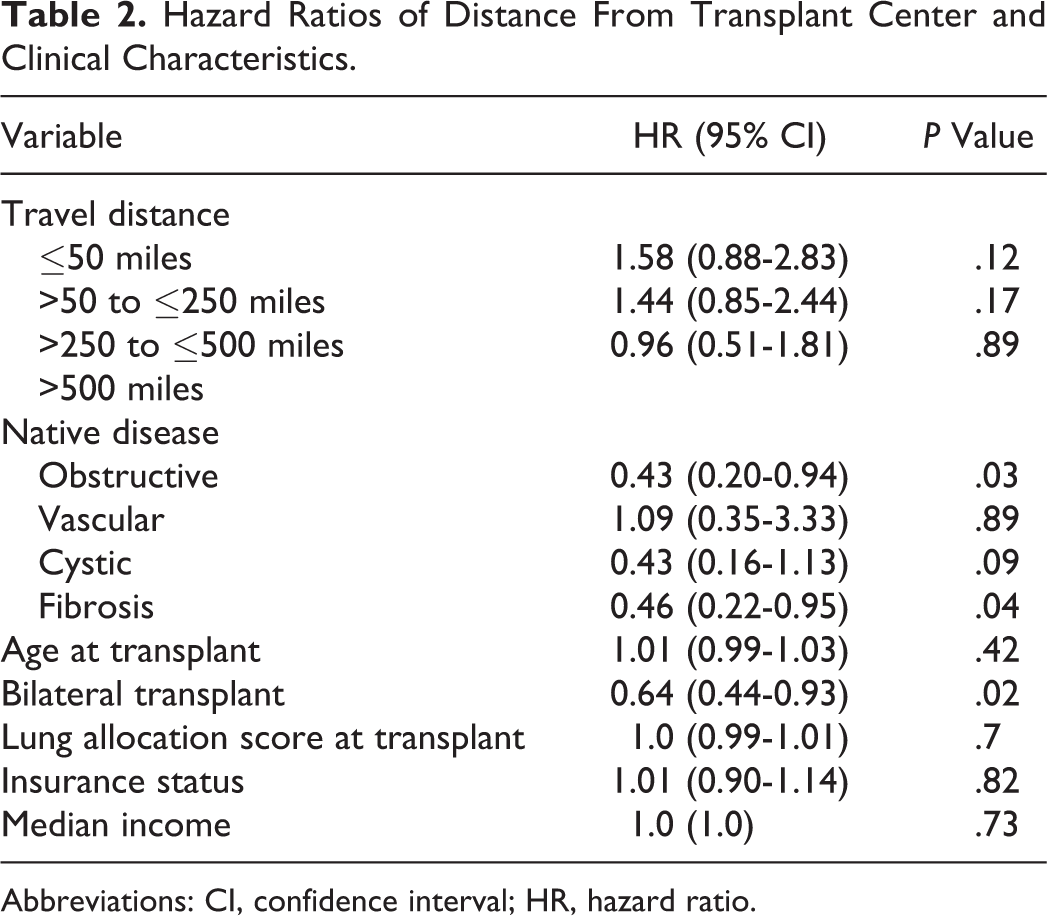
Abbreviations: CI, confidence interval; HR, hazard ratio.
Conclusions
We found no statistically significant relationship between posttransplant graft survival and recipient travel distance. There was a trend toward poorer graft survival with shorter travel distance, which may be from factors not captured in our data set or in the allocation score. There were fewer donation after cardiac death donors with increasing recipient distance from the transplant center, which likely reflects the transplant team weighing the likelihood of procuring organs from a donor after cardiac death against the burden of long distance recipient travel. There was a significant relationship between having prior cardiac valve surgery and travel distance. As prior cardiac valve surgery is a relative contraindication to lung transplant, patients are likely bypassing the nearest transplant center to seek care at our center.
We note that median income and use of private insurance significantly increased with increasing travel distance. These resources likely helped recipients traveling long distances with travel costs and adhere to outpatient follow-up schedules. Thus, the lack of difference between recipients based on travel may in part be affected by noncodified risks including increased resources among longer travel distance recipients.
Posttransplant ICU length of stay significantly decreased with increasing distance from our center, though overall hospital length of stay, readmissions, and episodes of acute rejection were not significantly different. Patients having to travel longer distances are presenting at the time of transplant in a clinical state that lends toward faster recovery immediately posttransplant, and there was a trend toward but a nonsignificant shorter overall hospital stay. The clinical factors behind this finding require further study.
We excluded recipients hospitalized at the time of transplant. The intent was to capture recipients who endure travel back and forth for pretransplant and wait-listed visits and upon receiving a phone call regarding a potential transplant immediately traveling to our center and then identifying local housing for several weeks afterward. One year after transplant, recipients may transfer their care to another lung transplant center, and we noted that this occurred with longer travel distances to Cleveland, Ohio. This practice of recipients seeking local follow-up likely minimized the impact of long travel distance to our center.
Our research extends prior work on the relationship between recipient travel distance and lung transplant outcomes. Thabut et al demonstrated the further a patient lived from a lung transplant center, the less likely that patient would be wait-listed. 5 And no relationship was identified between recipient distance to the nearest transplant center and posttransplant survival. However, Thabut et al included patients up until 2009 in a national cohort, while our study investigated a more recent transplant era (2010-2017) and examined more covariates hypothesized to impact recipient travel distance and posttransplant graft survival.
Recipient travel distance has also been explored in patients undergoing hematopoietic stem cell transplant and liver transplant. In patients undergoing stem cell transplant, those driving ≥160 minutes compared to those driving ≤40 minutes had worse survival. This was attributed to a lower frequency of posttransplant visits due to challenges associated with long distance driving. 6 Pediatric patients seeking liver transplant traveling >200 miles from home to transplant center had the same chance at receiving a transplant but a 75% higher risk of wait-list death compared to patients traveling ≤200 miles. 7 The disparity in wait-list death was attributed to a delay in referral as patients turned down at a local center had to travel farther to another transplant center, delaying time to wait-listing. The authors did not examine posttransplant survival. Finally, in a large study of Veterans Affairs (VA) patients, Goldberg et al showed that greater distance between a local VA center and the nearest VA liver transplant center was associated with a lower likelihood of being wait-listed, receiving a liver transplant, and increased risk of wait-list mortality. Posttransplant survival was not studied. 8
Our study has limitations. First, its small sample size from a single-center limits the power to detect differences in survival outcomes and the generalizability of our findings. Therefore, further study is needed to replicate our methods in a larger national cohort. Second, recipients may have moved to Cleveland, Ohio while wait-listed, and therefore, the shorter travel distance would not have been captured as we used the recipient’s permanent home zip code to calculate travel distance. However, we expect this number of recipients to be low based on our clinical experience. In addition, there may be other outcome measures including complication burden, quality of life, and social and financial burdens that may be directly impacted by travel distance and require further study. Finally, calculating linear travel distance using home zip code may be less informative than asking recipients to report travel mileage or minutes driven in the context of transport access, which may reflect travel burden and could be used in future study.
Our study examined a modern cohort of lung transplant recipients to assess the impact of travel distance on posttransplant graft survival. On November 24, 2017, donor lung allocation in the United States shifted toward broader geographic sharing in order to increase access to lung transplant. Donor lungs that were preferentially allocated locally are now allocated to the highest acuity patient across a broader region. 9 Donor allografts may be preferentially directed toward high-volume transplant centers with high-acuity patients. Therefore, with potentially fewer but higher volume transplant centers, consideration should be given to recipient travel burdens and its impact before and after transplant.
Footnotes
Authors' Note
Belinda L. Udeh is now affiliated to Department of Quantitative Health Sciences; Neurology Institute; and Quality and Patient Safety Institute, Cleveland Clinic, Cleveland, OH, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: W.M.T. receives funding from the American Society of Transplantation Faculty Career Development Award.