
Abstract
Introduction:
There is debate over whether Apolipoprotein L1 (APOL1) gene risk variants contribute to African American (AA) live donors’ (LD) increased risk of kidney failure. Little is known about factors influencing physicians’ integration of APOL1 genetic testing of AA LDs into donor evaluation.
Design:
We conducted a cross-sectional survey, informed by Roger’s Diffusion of Innovations theory, among nephrology and surgeon members of the American Society of Nephrology, American Society of Transplantation, and American Society of Transplant Surgeons about their practices of and attitudes about APOL1 genetic testing of AA potential LDs. Descriptive statistics and bivariate analyses were performed.
Results:
Of 383 completed surveys, most physicians believed that APOL1 testing can help AA LDs make more informed donation decisions (87%), and the addition of APOL1 testing offers better clinical information about AA LD’s eligibility for donation than existing evaluation approaches (74%). Among respondents who evaluate LDs (n = 345), 63% would definitely or probably begin or continue using APOL1 testing in the next year, however, few use APOL1 testing routinely (4%) or on a case-by-case basis (14%). Most did not know the right clinical scenario to order APOL1 testing (59%), but would use educational materials to counsel AA LDs about APOL1 testing (97%).
Discussion:
Although physicians were highly supportive of APOL1 genetic testing for AA LDs, few physicians use APOL1 testing. As more physicians intend to use APOL1 testing, an ethical framework and clinical decision support are needed presently to assist clinicians in clarifying the proper indication of APOL1 genetic testing.
Keywords
Introduction
African Americans (AAs)/Blacks have disproportionately greater prevalence of chronic kidney disease (CKD) and end-stage renal disease (ESRD) than other racial/ethnic groups. 1 Such disparities extend to AA living kidney donors (donors). The incidence of ESRD and CKD, and their risk factors, is significantly higher in AA donors than in European American donors. 2 –4 The estimated risk of ESRD at 15 years post-donation is higher in AA donors than in European American donors: 74.7 versus 22.7 per 10 000 living donors.
Genetic factors may contribute to these disparities. 5 –7 Apolipoprotein L1 (APOL1) gene risk variants are significantly associated with CKD and ESRD in individuals of African ancestry (such as AAs), 8 but not other populations. 9,10 The Dallas Heart Study found that, among AAs without diabetes, significantly more participants with 2 APOL1 risk variants (6.7%) had CKD (GFR <60 mL/min per 1.73 m2) than those with 0 to 1 risk variants (1.7%). 7 In several large population-based studies, 13% to 15% of AAs without kidney disease have 2 APOL1 risk variants and 39% have one risk variant. 7,11 African Americans with 2 gene risk variants have a 10-fold odds of FSGS-, and 7-fold odds of hypertension-attributed ESRD. 9
Evidence suggesting the contribution of APOL1 risk variants to donor outcomes comes from deceased donors (DD). The APOL1 risk variants in AA DDs significantly increased the risk of graft failure in kidney transplant recipients, regardless of recipients’ race/ethnicity 12 or possessing 2 risk variants. 13 Kidneys from DDs with 2 APOL1 risk variants had significantly worse graft survival (2-fold hazard ratio) than kidneys from DDs with no or one variant. 12,14 The APOL1 risk variant was found in 13% of AA DDs, 15 and virtually all DDs with APOL1 risk variants were of African ancestry. 12 Case reports of living donors developing ESRD suggest APOL1 risk variants as contributing factors. 16,17
These findings have generated heightened ethical concern and uncertainty in the transplant community over whether to use genetic testing to protect donor safety, improve donor informed consent, and reduce disparities. 18,19 The American Society of Transplantation’s (AST) 2015 consensus conference recommended against routine APOL1 testing for AA donors because CKD/ESRD rarely arises in individuals with 2 gene variants; the risk of CKD/ESRD was very low among living donors; and utilizing APOL1 testing may potentially magnify disparities for AAs in access to kidney transplantation. 20 However, the Kidney Disease: Improving Global Outcomes guidelines subsequently recommended “considering APOL1 genotyping” in AA donors. 21(pS76) The National Institutes of Health has since funded the APOL1 Long-term Kidney Transplantation Outcomes Network (APOLLO) in 2017 to assess APOL1 risk variants’ effect on kidney function in kidney transplant recipients receiving kidneys from AA deceased or living donors.
Without professional consensus and definitive outcomes data, transplant physicians must rely on their clinical judgment to determine whether to use APOL1 testing, which could affect donors’ decision making. As proponents posit, APOL1 testing could risk stratify donors; the presence of 2 risk variants should comprise a relative contraindication to donation, requiring careful counseling and consent. 6,22 Opponents contend that APOL1 testing is premature given its lack of specificity in predicting disease, 22 and lack of long-term population-based studies of APOL1 in donors. 23
With the advent of commercial testing for APOL1 risk variants, more transplant centers use APOL1 testing. 6 The AST surveyed 83 AST/American Society of Nephrology (ASN) Transplant Nephrology Fellowship Directors and transplant programs, of which 13% used APOL1 genotyping. 20 Little is known about physicians’ attitudes about APOL1 testing and barriers and facilitators to the adoption of APOL1 testing into clinical practice.
Our national survey aimed to assess transplant and nephrology physicians’ normative attitudes, behavioral intentions, and practices of APOL1 testing. Attitudes and intentions are important to evaluate because, as precursors to actual behaviors, 24 they inform clinical judgment affecting care that donors receive now and in the future. Assessing attitudes before APOLLO study results emerge can illuminate factors that may influence the adoption of APOL1 genetic testing into clinical practice.
Design/Methods
Design
A cross-sectional survey assessed physicians’ attitudes and use of APOL1 testing. Northwestern University’s Institutional Review Board approved this study.
Sample Population and Recruitment
United States-based transplant surgeons, transplant nephrologists, and general nephrologists (MD or DO) who were members of the American Society of Transplant Surgeons (ASTS), the ASN, or AST were eligible to participate. Eligible participants were recruited differently depending on how each Society shared their membership lists. The ASTS (900 US physician members) provided members’ e-mail addresses. Members were recruited via e-mail with a URL link to the online survey, with 5 reminder e-mails sent every 1 to 4 weeks.
The ASN (8104 US physician members) provided single use access to members’ mailing addresses. General nephrologists’ perspectives are important because they have expertise in evaluating risk of kidney disease progression, follow many donors post-donation long-term, and provide insight into the risk of kidney disease progression for donors outside the transplant context. Given limited research resources, a random sample stratified by state of 4005 members was recruited once via postal mail and given a URL link to the online survey. The statistician (J.L.) provided a computer-generated random number list with different sample sizes for different strata (ie, states with members <50 were oversampled) to generate the sample.
The AST declined paid access to members’ contact information. Therefore, physician members of AST’s Kidney Pancreas, Transplant Diagnostics, Live Donor, and Psychosocial Communities of Practice were invited to participate via e-mail to each one’s listserv with a URL link to the online survey. Communities of Practice included 147, 146, 212, and 18 US physician members, respectively. Four e-mails to each listserv were sent every 1 to 4 weeks. The online survey, mailed survey, and recruitment letter included a fact sheet describing the current science on APOL1 so that potential participants gained a knowledge base with which to respond to the survey.
To increase response rates, multiple recruitment attempts were used. Participants had an option to enter a drawing to win a $10 Starbucks gift card or an Android or Apple watch. 25 Survey initiation indicated consent to participate in the study.
Theoretical Framework
Roger’s theory of Diffusion of Innovations 26 guided survey question development, as used in another study of adopting genetic testing. 27 Roger’s theory explains how a new behavior (ie, APOL1 testing) spreads through a social system, that is, the transplant field, and gets adopted into practice. 26 Physicians’ adoption of APOL1 testing will depend on perceptions of APOL1 testing as new or innovative. Physicians will vary in their stage of adoption from awareness of the need for the innovation, to deciding to adopt testing, to initial use of APOL1 testing, and to continued use of APOL1 testing. Diffusion of Innovations theory, as it applies to the transplant context, postulates that physicians are more likely to adopt the innovation if they perceive it as: (1) advantageous in conferring benefits to potential donors, based on knowledge of the existence of, indications for, and intended use of APOL1 testing (ie, for decision-making), (2) compatible with organizational and individual norms, attitudes, and needs, (3) simple and readily available to use, (4) usable to try out before committing to adoption, (5) observably conferring benefits to potential donors, that is, awareness of cases of APOL1 testing, and (6) open to modification by providers, that is, integrating genetic services into care. 26
Data Collection
The survey was developed by experts in research methods (E.J.G., R.R.S., and C.W.) and transplant and nephrology (J.F. and E.J.G.) to enhance its content validity. The survey was pilot-tested among 8 transplant surgeons, transplant and general nephrologists at Northwestern Medicine® to refine question clarity, response options, and order. The survey included 56 closed-ended and 4 open-ended questions. Topics covered: current clinical practice of APOL1 testing (n = 10), hypothetical clinical decisions about donors with APOL1 risk variants (n = 6), normative expectations about APOL1 testing (n = 3), attitudes about APOL1 testing (n = 11), barriers and facilitators to adoption and use of APOL1 testing (n = 7), thresholds for adopting APOL1 testing into clinical practice (n = 2), demographics (n = 3), and clinical practice characteristics (n = 14). A copy of the survey is freely available upon request.
Data Analysis
Descriptive statistics (eg, frequencies, percentages, means, standard deviations) assessed the distribution of survey responses across the sample. χ2 or Fisher exact test statistics, as appropriate, were used to assess the relationship between attitudinal variables and physician type; and between physicians’ experience with cases of APOL1 genetic test results and donor decision-making. Likert scale questions were treated as categorical variables. Transplant surgeons were compared to all nephrologists, and transplant physicians (surgeons, nephrologists) were compared to general nephrologists. All tests were 2-sided, performed using SPSS version 24 (Armonk, New York), and P value <.05 was considered statistically significant.
Results
Participant Characteristics
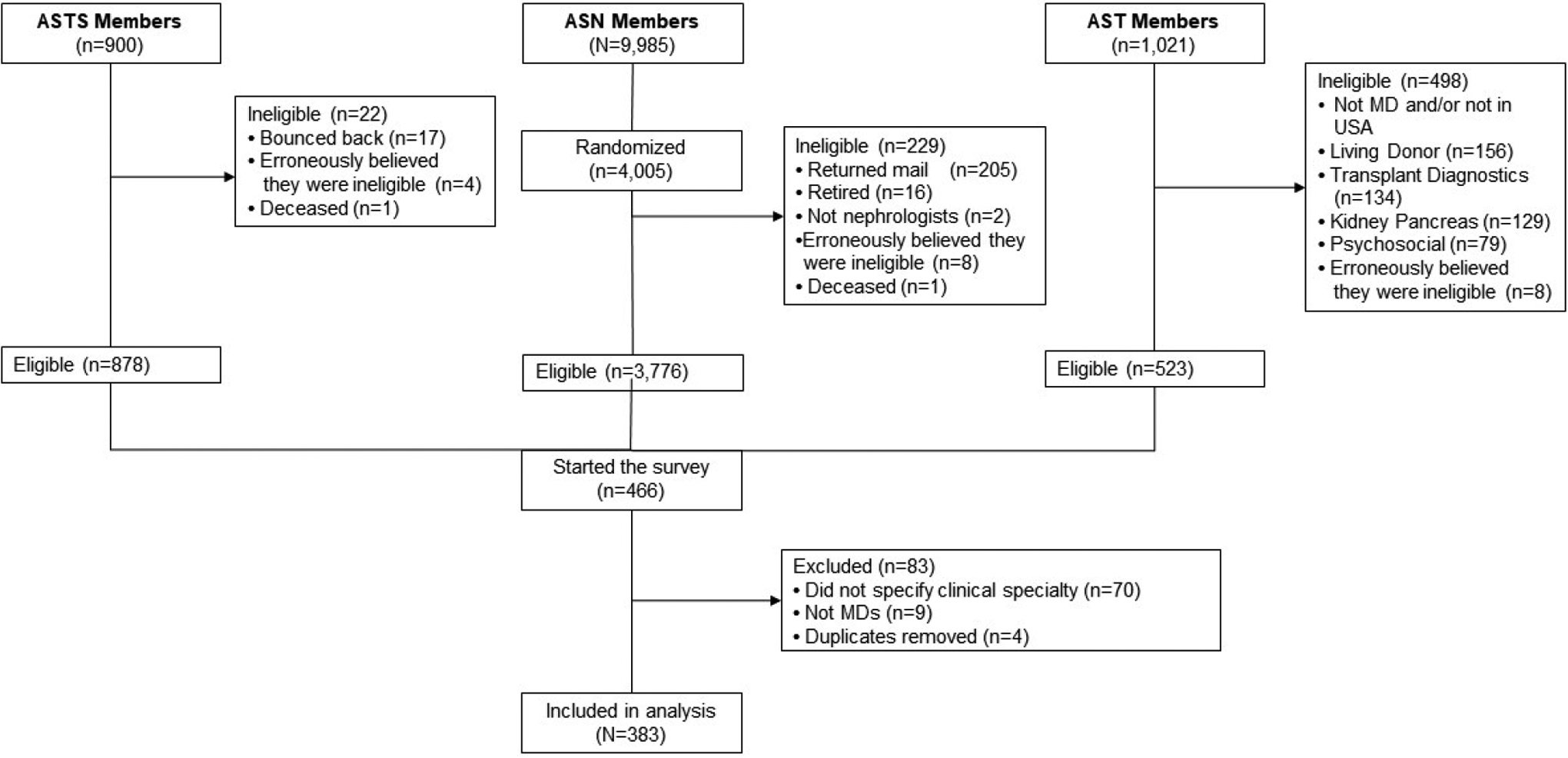
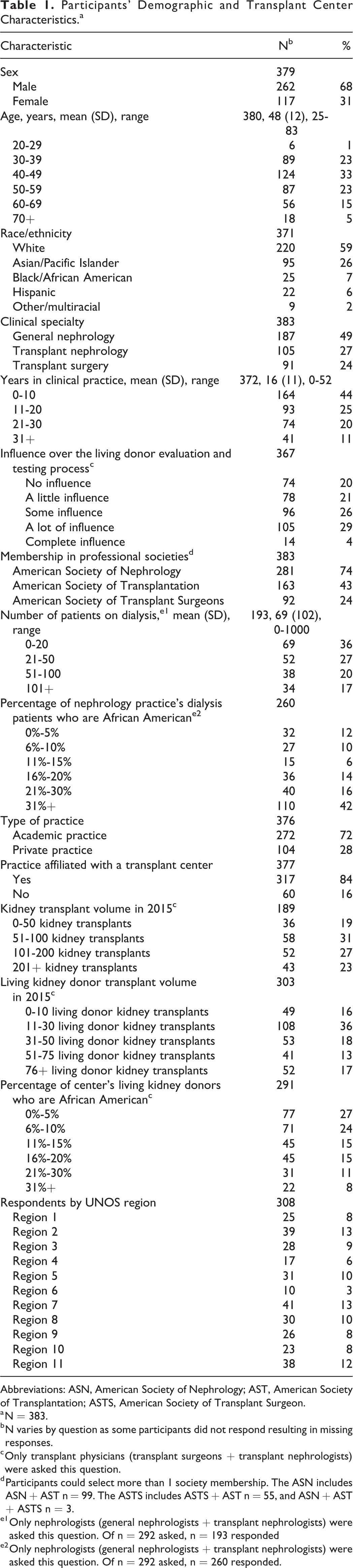
Of 11 906 members, 5177 were eligible to participate or were sampled from the list (ASN only) (Figure 1). Physicians were ineligible (n = 749) due to bounced back e-mails, returned mail, not being US physicians, or self-identified as ineligible given retirement or clinical inactivity. Of the eligible participants, 466 members started the survey, but 83 were excluded due to not specifying clinical specialty, nonphysician status, and duplicate entries. A total of 383 surveys were included in analysis. Table 1 presents participants’ demographic and clinical practice data. Participants were mostly male (68%), white (59%), general nephrologists (49%), transplant nephrologists (27%), and transplant surgeons (24%).
Participation rate.
Participants’ Demographic and Transplant Center Characteristics.a
Abbreviations: ASN, American Society of Nephrology; AST, American Society of Transplantation; ASTS, American Society of Transplant Surgeon.
a N = 383.
b N varies by question as some participants did not respond resulting in missing responses.
c Only transplant physicians (transplant surgeons + transplant nephrologists) were asked this question.
d Participants could select more than 1 society membership. The ASN includes ASN + AST n = 99. The ASTS includes ASTS + AST n = 55, and ASN + AST + ASTS n = 3.
e1 Only nephrologists (general nephrologists + transplant nephrologists) were asked this question. Of n = 292 asked, n = 193 responded
e2 Only nephrologists (general nephrologists + transplant nephrologists) were asked this question. Of n = 292 asked, n = 260 responded.
Clinical Practice of Using APOL1 Testing
Most respondents were aware of APOL1 testing as an option for AA potential donors (78%). Among respondents who evaluate donors (n = 345), few currently use APOL1 testing for AA potential donors routinely (4%), or on a case-by-case basis (14%), or did not know (16%).
Experience With APOL1 Testing
Forty-nine (13%) of 380 respondents knew of or had participated in the care of an AA potential donor for whom APOL1 testing was used. Among 48 of these respondents, more genetic test results were positive (i.e., 2 risk variants were found) (n = 26, 54%) than negative (n = 22, 46%). Among 47 cases, the results strongly or slightly dissuaded donors from donating (40%), strongly or slightly encouraged donors to donate (19%), or had no effect (40%). Bivariate analysis revealed a significant relationship between test results and donors’ decision making (P < .001). Positive test results were related to donors being strongly or slightly dissuaded from donating (79.2%), while negative results were related to donors being strongly or slightly encouraged to donate (33.3%). In a few cases, positive results had no effect on donors’ decision (23.1%), and negative results had no effect on donors’ decision (61.9%).
Figure 2 identifies clinicians who provided counseling/education to AA potential donors before and after APOL1 genetic testing. On both occasions, leading clinicians were the respondent, another physician, and nurse or nurse practitioner. Leading topics discussed before APOL1 testing included: medical (51/63, 81%), donor candidacy (48/63, 76%), family/social (29/63, 46%), insurance (22/63, 35%), and financial (18/63, 29%) implications of positive test results.
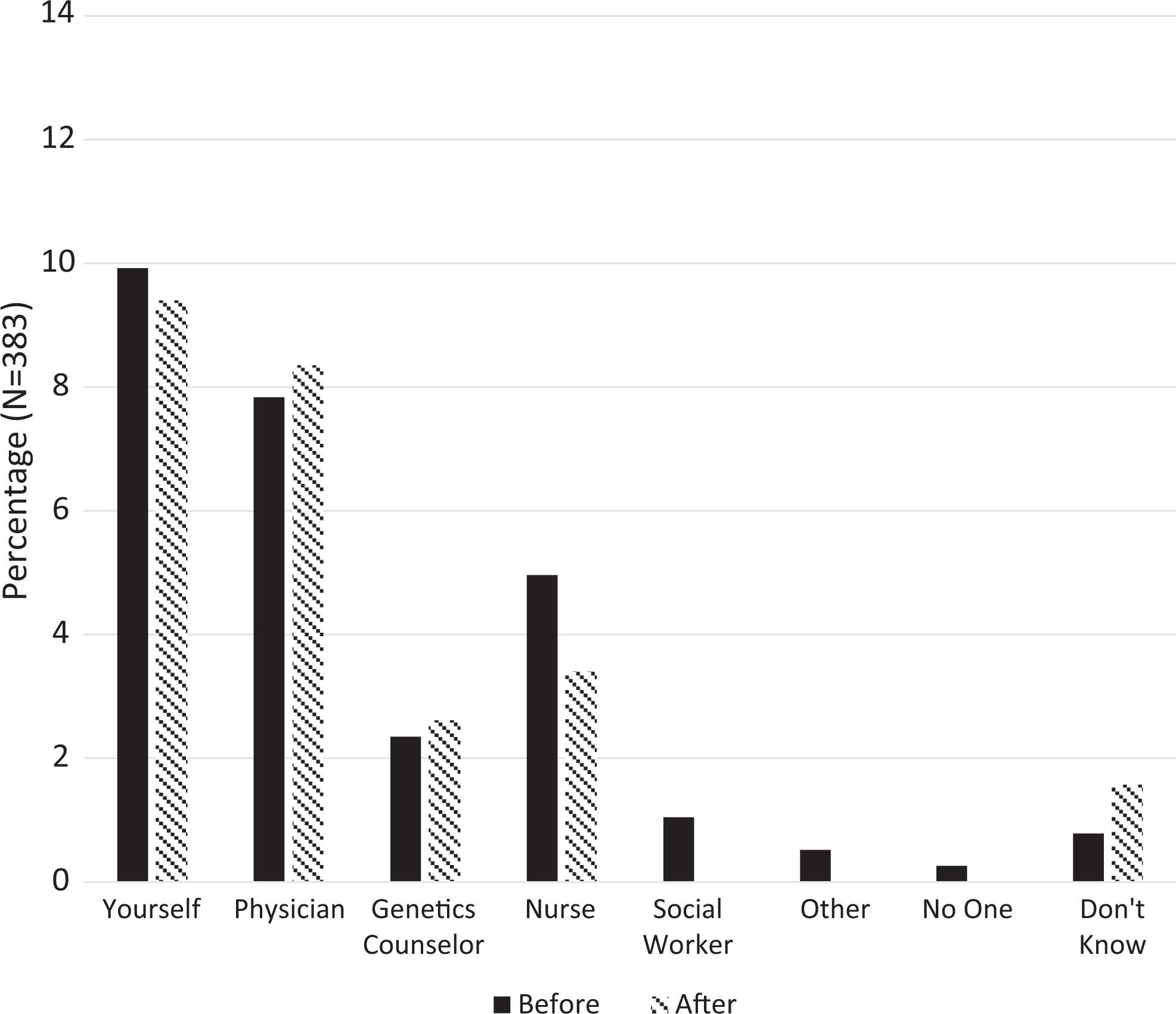
Clinicians providing counseling before and after using Apolipoprotein L1 (APOL1) genetic testing.
Likelihood of Using APOL1 Genetic Testing
Among respondents who evaluate donors, 63% would definitely or probably begin or continue using APOL1 testing in the next year, while 21% would definitely or probably not, and 16% did not know. More nephrologists than surgeons/transplant physicians would definitely or probably begin or continue using APOL1 testing in the next year (P < .002, P < .006). Of the general nephrologists surveyed, most (83%) evaluate donors, and of these, 63% would definitely or probably begin or continue using APOL1 testing in the next year.
Hypothetical Clinical Decisions About Donors With APOL1 Risk Variants
In a hypothetical scenario in which an AA potential donor had 2 APOL1 risk variants, half of respondents involved in evaluating donors reported they would not proceed with the living donation or would strongly recommend against it (50%), the rest would either proceed with donation or discuss the pros and cons and let the potential donor decide (40%), or were unsure (10%). When the scenario changed to the donor having one APOL1 risk variant, few would not proceed with the donation or would strongly recommend against it (9%), most would recommend proceeding with donation or discuss the pros and cons and let the potential donor decide (80%), or were unsure (12%). Respondents reported that the decision whether AA donors with 2 APOL1 risk variants should donate resided in the multidisciplinary team (51%), donor (30%), transplant nephrologist (12%), or others.
Ethical Perspectives and Attitudes About APOL1 Testing
Potential donor considerations
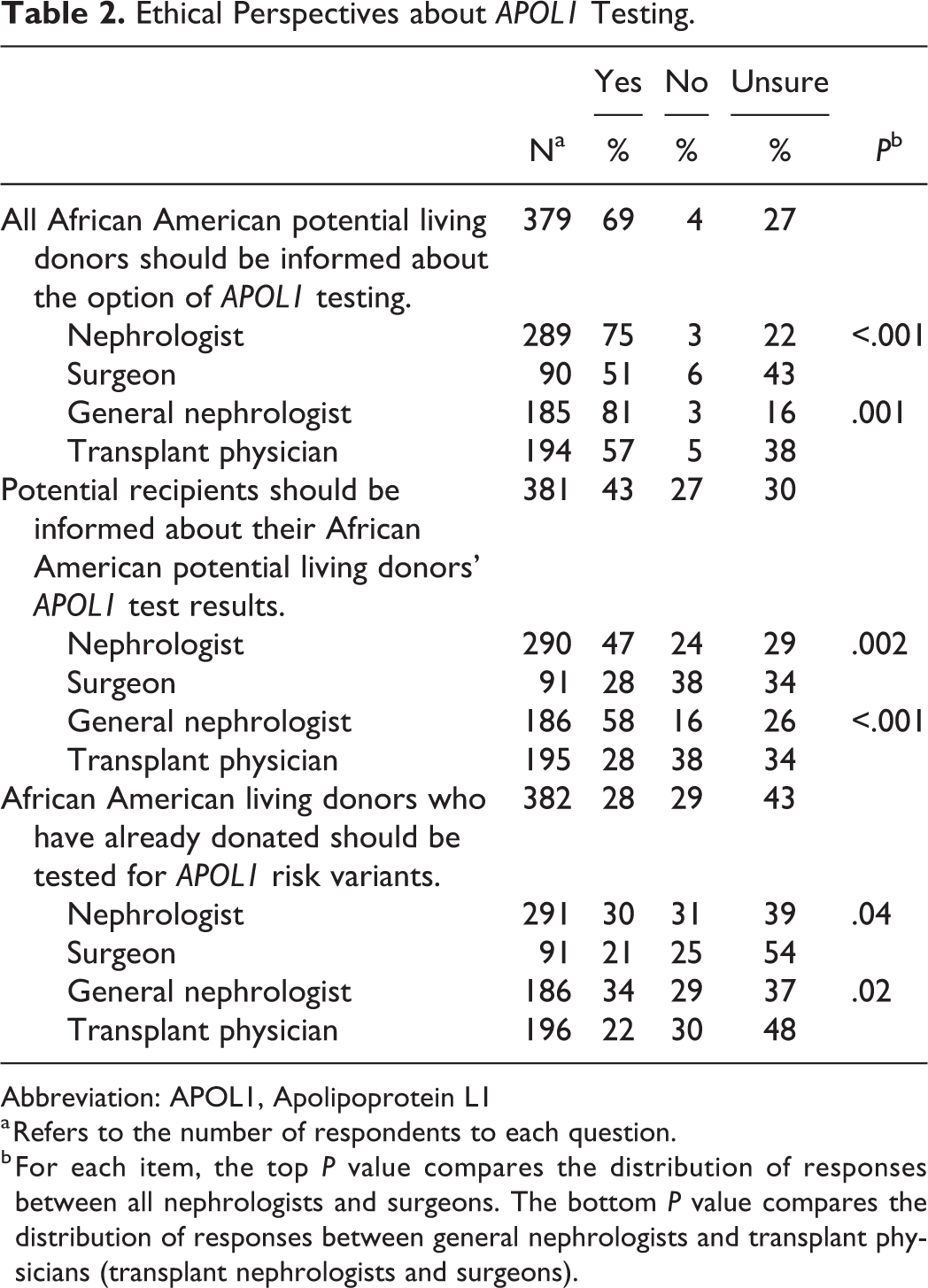
Most respondents believed that all AA potential donors should be informed about the option of APOL1 testing (69%) than were against it (4%) or were unsure (27%); significantly more nephrologists agreed than surgeons (P < .001) (Table 2). Most strongly or slightly agreed that APOL1 testing can help donors make more informed donation decisions (87%) and is beneficial for AA donors (74%), but it would reduce the number of AA donors (73%). Significantly more nephrologists expressed agreement with these attitudes than surgeons/transplant physicians (Table 3).
Ethical Perspectives about APOL1 Testing.
Abbreviation: APOL1, Apolipoprotein L1
a Refers to the number of respondents to each question.
b For each item, the top P value compares the distribution of responses between all nephrologists and surgeons. The bottom P value compares the distribution of responses between general nephrologists and transplant physicians (transplant nephrologists and surgeons).
Attitudes about APOL1 Genetic Testing.
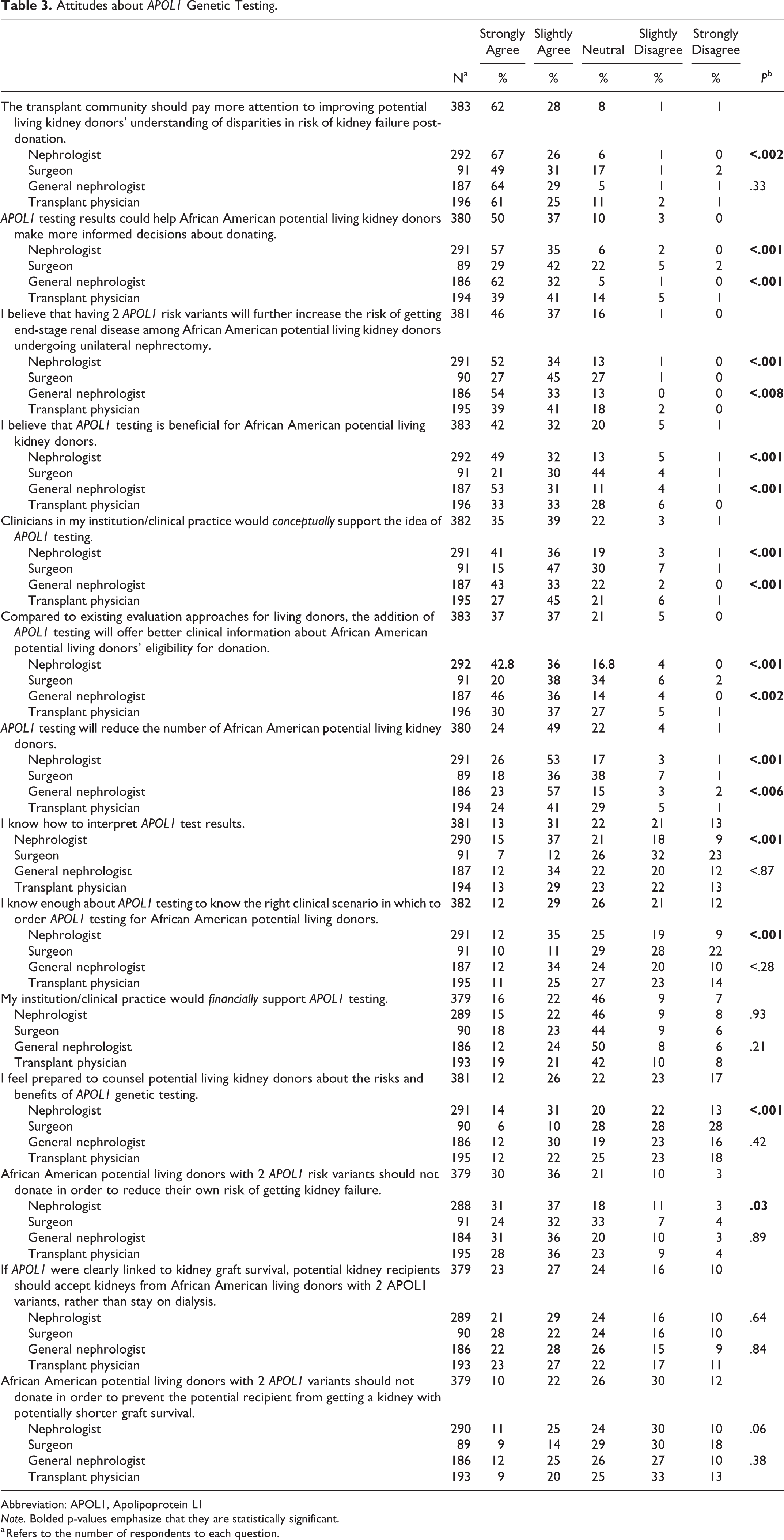
Abbreviation: APOL1, Apolipoprotein L1
Note. Bolded p-values emphasize that they are statistically significant.
a Refers to the number of respondents to each question.
Most reported that the addition of APOL1 testing to donor evaluation would offer better clinical information about AA donor’s eligibility for donation than existing evaluation approaches (74%). Significantly more nephrologists expressed agreement with these attitudes than surgeons/transplant physicians (Table 2).
More agreed (66%) than disagreed (13%) or were neutral (21%) that AA potential donors with 2 APOL1 risk variants should not donate to reduce their own risk of kidney failure; significantly more nephrologists agreed than surgeons (P = .03) (Table 3). One-third agreed that AA potential donors with 2 APOL1 risk variants should not donate to prevent potential recipients from getting a kidney with potentially shorter graft survival (32%) (Table 3). More respondents were unsure (43%) than opposed (29%) or supported (28%) AA donors who have already donated getting tested for APOL1 risk variants; significantly more surgeons/transplant physicians expressed uncertainty than nephrologists (P = .04, P = .02) (Table 3).
Potential recipient considerations
Half reported that, if APOL1 risk variants were clearly linked to kidney graft survival, potential kidney recipients should accept kidneys from AA donors with 2 APOL1 risk variants rather than stay on dialysis (50%) (Table 3). More respondents believed that potential recipients should be informed about their donors’ APOL1 test results (43%) than were against it (27%) or unsure (30%); significantly more nephrologists expressed agreement than surgeons/transplant physicians (P = .002, P < .001) (Table 2).
Factors Affecting Adoption of APOL1 Testing
Leading barriers to using APOL1 testing were lack of professional guidelines on APOL1 testing (52%), prospective population data on donors (47%), randomized controlled trials on living donor outcomes associated with APOL1 risk variants (46%), and insurance coverage for APOL1 testing (42%) (Figure 3). Of 382 respondents, most (93%) would feel more comfortable offering APOL1 testing to AA potential donors if professional guidelines on APOL1 testing were available.
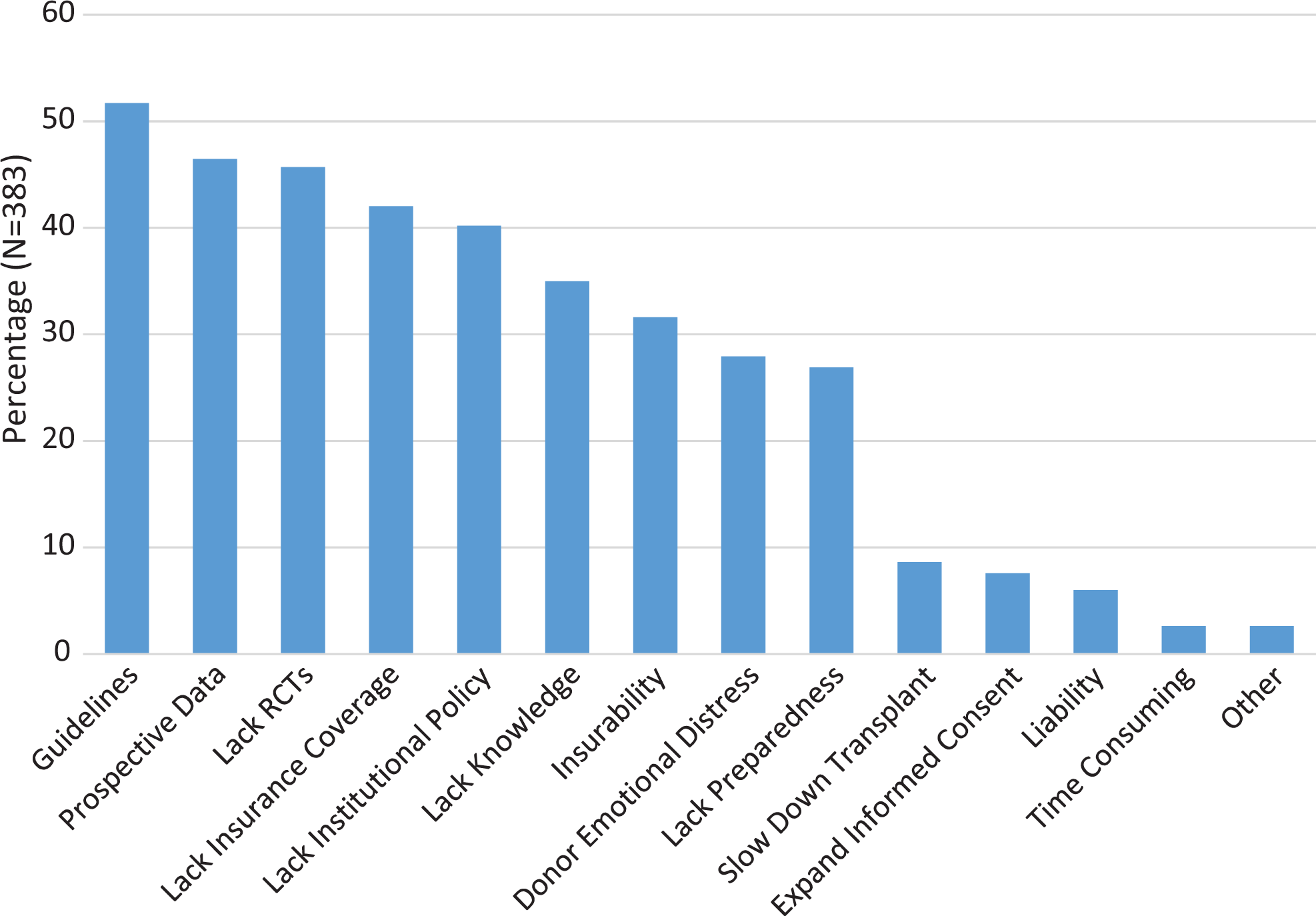
Barriers to using Apolipoprotein L1 (APOL1) genetic testing.
More were neutral or did not know enough about APOL1 testing to know the right clinical scenario to order APOL1 testing (59%). Significantly more nephrologists than surgeons reported knowing the clinical scenario (P < .001) (Table 3). Of 382 respondents, most (97%) would use educational materials to counsel AA donors about APOL1 testing.
To adopt APOL1 testing into clinical practice, most of the 367 (56%) respondents minimally needed a 2-fold increase in relative risk of kidney failure attributed to APOL1 risk variants. To integrate APOL1 testing into routine donor evaluation, most of the 362 (61%) respondents required a minimum of 5% or 10% of the AA population to have 2 APOL1 risk variants.
Discussion
This is the first theoretically driven study assessing transplant and nephrology physicians’ attitudes toward and practices of integrating APOL1 genetic testing into clinical practice for AA potential donors. A key finding was the discrepancy between physicians’ attitudes and practices. Although physicians were highly supportive of APOL1 genetic testing for AA donors, few physicians use APOL1 testing routinely (4%) or on a case-by-case basis (14%). These rates correspond with innovators (3%) and early adopters (14%), respectively, who, according to Diffusion of Innovation theory, are more apt to adopt the innovation. Most physicians identified barriers to adopting APOL1 testing that appear to supersede their ethical norms in favor of APOL1 testing.
Unlike AST’s findings in which 13% of physicians use APOL1 testing, we found high levels of support for APOL1 testing, as most (63%) physicians plan to begin or continue using APOL1 testing in the next year. According to Roger’s theory, physicians are more likely to adopt APOL1 testing if they perceive it as advantageous. Most physicians reported that APOL1 testing conferred ethical and clinical benefits: improving donors’ informed consent, reducing donors’ risk of kidney failure, and providing physicians with more clinically relevant information for donor evaluation than is currently available. Nephrologists’ stronger perceptions of APOL1 testing than surgeons may derive from their long-term patient care and being more likely to see transplantations’ impact on patients and families.
Despite their support for APOL1, few physicians currently use APOL1 testing due to various barriers, including absence of professional guidelines, prospective data, and randomized controlled trials on APOL1 in AA donors, which coincide with theoretical requirements for innovations to be compatible with organizational needs. Although genetics guidelines address ethical issues in other clinical conditions, 28 available consensus guidelines on APOL1 are limited in scope due to lack of evidence providing insight into long-term outcomes. 20,21 Consequently, physicians are unclear as to how to use APOL1 test results in the context of living donation.
Perceptions about APOL1 may also affect physicians’ use of APOL1 testing. The majority of physicians (56%) believed the relative risk of kidney failure attributed to APOL1 risk variants would need to increase by at least 2 times to adopt APOL1 testing into clinical practice. Even though 13% of the AA general population has 2 APOL1 risk variants, most (61%) reported that a minimum of 5% or 10% of the AA population would need to have 2 risk variants to warrant integrating APOL1 testing into routine donor evaluation. Thus, one might expect higher rates of APOL1 testing.
Physicians shared an ethical concern that APOL1 testing would reduce the number of potential donors. Some physicians (13%) knew of or had participated in the care of an AA potential donor for whom APOL1 genetic testing was used. Positive test results dissuaded some donors from donating, as expected. Negative test results had little effect on donors’ decisions as most pursued donation.
Despite AST’s recommendations against APOL1 testing, some physicians are still using, and most intend to use APOL1 testing. Thus, education is necessary to guide physicians’ clinical practice. Almost all physicians reported they would use educational materials to counsel AA donors about APOL1 testing (97%). We are currently developing culturally targeted educational materials about APOL1 genetic testing for AA donors. Future research should assess whether educational materials increase physicians’ knowledge of APOL1 testing, and donor comprehension of APOL1 testing for informed consent.
The inconsistency between physicians’ attitudes and practices may highlight a moral tension between promoting donors’ informed decision-making and promoting living donation to help potential recipients, which can ameliorate disparities in AAs’ access to transplantation. Our finding that more physicians intend to use APOL1 testing than currently do suggests that other motivators affect adopting APOL1 testing, for example, ethical concerns about protecting donors from risk.
If APOL1 genetic testing becomes a more routine part of donors’ clinical care, addressing these moral tensions may become difficult to do and contribute to uneven care for potential donors. Therefore, broader professional debate about evaluating donors that addresses the ethical considerations of APOL1 testing is presently needed to proactively protect potential donors and potential recipients.
Our study’s strengths include a theoretically driven approach. Study limitations include a low participation rate. However, low participation rates may be less disconcerting in physician surveys than general public surveys because physicians are usually more homogenous in knowledge, attitudes, and practices. 29 Findings may not be generalizable to all AST, ASTS, and ASN physician members. Nonresponse bias may have affected the results: physicians with greater knowledge of APOL1 testing may have been more inclined to respond to the survey than those who did not. If applicable, this bias would partly explain differences between our and AST’s findings. The survey may have enabled cognitive biases through anchoring effects. A limitation may be physician’s lack of familiarity with and/or use of APOL1 genetic testing. Most general nephrologists surveyed evaluate donors, though the few (17%) who were not involved in evaluating donors might have affected the results. Providing a fact sheet may have skewed participants’ familiarity with APOL1 testing. Participants’ responses to questions may have differed according to their donor program’s volume, influence over evaluating donors, and patients’ and donors’ racial demographics.
APOL1 testing is at the early stages of diffusion. Although available circumstantial data are compelling, it is unclear how much APOL1 testing may provide useful prognostic information for evaluating AA potential donors. 15 Genotyping may potentially personalize medical care through genetic assessment of ESRD risk for potential donors. 30 Physicians’ current and intended use of APOL1 testing highlights the need for an ethical framework and training on APOL1 testing. Professional guidelines and clinical decision support may assist physicians evaluating AA donors to clarify the proper use of APOL1 genetic testing.
Footnotes
Authors’ Note
All persons listed as authors must have (1) participated sufficiently in the work to take public responsibility for the content; or (2) made substantial contributions to the conception and design or analysis and interpretation of data; or (3) participated in drafting of the article or revising it critically for important intellectual content; and (4) given final approval of the version of the manuscript to be published. The manuscript consists of original work and does not copy or otherwise infringe on the copyright or other proprietary rights of others.
Acknowledgments
Thanks go to Elida Romo, Crystal Johnson, and Daniela Amortegui for their research assistance. An earlier draft of this paper was presented at the American Transplant Congress; April 30, 2017; Chicago, IL. REDCap is supported at Feinberg School of Medicine by the Northwestern University Clinical and Translational Science (NUCATS) Institute.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by the NIAID (Grant No. 1 R03 AI126090-01 to E.J.G.). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Research reported in this publication was supported, in part, by the National Institutes of Health’s National Center for Advancing Translational Sciences, Grant Number UL1TR001422.