
Abstract
The solid organ transplant community is slow to adopt the routine practice of using direct oral anticoagulants. Rivaroxaban and apixaban share common metabolic pathways with tacrolimus. This study aimed to clarify the impact of rivaroxaban/apixaban on tacrolimus troughs. Fifty solid organ transplant recipients with concomitant use of tacrolimus and rivaroxaban/apixaban were retrospectively assessed for changes in tacrolimus troughs and dose. Average dose-adjusted tacrolimus troughs and average tacrolimus total daily doses prior to and after rivaroxaban/apixaban initiation were compared. Subgroup analyses evaluating rivaroxaban and apixaban individually were performed. Rivaroxaban was prescribed to 18 recipients, and apixaban was prescribed to 32 recipients. Transplanted organs included kidney (n = 22), lung (n = 18), liver (n = 7), simultaneous pancreas and kidney (n = 1), and simultaneous kidney and liver (n = 2). The median doseadjusted tacrolimus trough and tacrolimus total daily dose prior to rivaroxaban/apixaban initiation was 2.15 ng/mL/mg (IQR 1.17, 3.37) and 4 mg (IQR 1.88, 6.25), respectively. The median dose-adjusted tacrolimus trough and tacrolimus total daily dose after rivaroxaban/apixaban initiation was 2.16 ng/mL/mg (IQR 1.24, 4.10) and 3.55 mg (IQR 1.5, 6.35), respectively. No significant difference was found between average dose-adjusted tacrolimus troughs or tacrolimus total daily doses before and after rivaroxaban/apixaban initiation or in the individual subgroup analyses for rivaroxaban/apixaban. It is unlikely that initiating rivaroxaban/apixaban affects tacrolimus troughs or requires tacrolimus dose adjustment. This study does not elucidate if tacrolimus affects rivaroxaban/apixaban pharmacokinetics or pharmacodynamics.
Introduction
Incidence of venous thromboembolism (VTE) in solid organ transplant ranges from 2-34% depending on transplanted organ, 1 which is increased compared to the thrombosis incidence of 0.1-0.2% in the general population. 2 Factors that predispose solid organ transplant recipients to thrombosis include their pre-transplant comorbidities (ie, lupus nephropathy, familial amyloid polyneuropathy, heart failure, pulmonary fibrosis), immunosuppressive medications (ie, calcineurin inhibitors and corticosteroids), and post-surgical coagulopathies. 1 Simultaneously, the incidence of atrial fibrillation (AF) in transplant recipients ranges from 0.3-39% depending on transplanted organ, 3 –7 further adding to their thrombotic risk. The hypercoagulable state in this population appears to be multifactorial and lifelong, although thrombosis risk is likely greatest in the initial 6 months after transplant. 1
Warfarin has historically been the oral anticoagulant of choice. However, within the past 5 years, direct oral anticoagulants (DOACs), specifically rivaroxaban (RIVA), apixaban (APIX), dabigatran, and edoxaban, have become recommended first-line agents in national guidelines for the treatment of VTE 8 and stroke prevention in patients with nonvalvular AF in the general population. 9,10 Unfortunately, none of these guidelines provide recommendations specifically for organ transplant recipients leaving a question as to whether this recommendation should be applied in this population. 8 –10 Preference for DOACs is based on their ability to significantly reduce thromboembolic events and decrease the incidence of intracranial hemorrhage compared to warfarin. 9 –12 They offer a more attractive option for both the patient and the healthcare team as they do not require therapeutic drug monitoring and do not have as many dietary, drug-drug, and drug-disease interactions as warfarin. Despite recommendations for their use as first-line agents and their benefits compared to warfarin, there is hesitation to use DOACs.
The slow adoption of DOACs by the transplant community is likely due to limited body of literature with small sample sizes evaluating the use of DOACs in this population. 13,14 A systematic review of the use of DOACs only identified 9 full-text studies evaluating the safety and/or efficacy of DOACs in solid organ transplant recipients. The largest of these studies included 99 recipients while the others included 52 recipients or less. 14 Lichvar and colleagues conducted a nationwide survey of adult transplant programs in the United States to assess DOAC utilization. While 94.3% of survey responders allowed DOAC therapy in the posttransplant setting, 73.8% did not preemptively adjust the DOAC dose for recipients receiving tacrolimus (TAC), which demonstrates practice discordance across sites. Nearly 65% of transplant pharmacists who responded to the survey acknowledge the lack of transplant-specific data on DOACs further emphasizing the need for additional research within this population. 15
A concern with the use of the DOACs in is the potential of unmonitored drug-drug interactions given their extensive medication regimens. 16 Tacrolimus, the backbone of immunosuppression therapy, is a well-known substrate for cytochrome P450 3A4 (CPY3A4), cytochrome P450 3A5 (CYP3A5), and permeability glycoprotein (P-gp). 17 Rivaroxaban, APIX, and TAC, share metabolic pathways (Figure 1). RIVA and APIX are also both substrates for CYP3A4/5 and P-gp, generating concern about the safety and efficacy of RIVA/APIX in transplant recipietns. 18,19 Competition for these proteins could lead to increased TAC concentrations, which may lead to an increased risk of adverse effects (ie, neurotoxicity, nephrotoxicity).
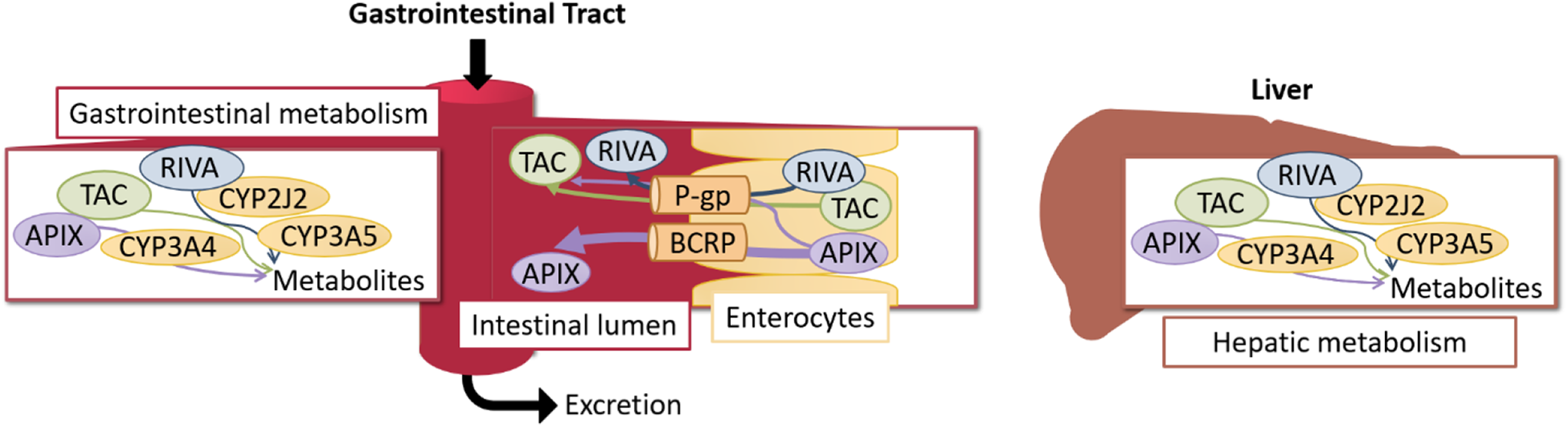
Shared metabolic pathways of RIVA, APIX, and tacrolimus. APIX: apixaban, BCRP: breast cancer resistance protein, CYP: cytochrome P450, P-gp: permeability glycoprotein, RIVA: rivaroxaban, TAC: tacrolimus.
Within the limited available literature, there is conflicting evidence as to whether DOACs alter TAC pharmacokinetics. 20 –24 A 22-patient subgroup analysis of a single-center, retrospective study of solid organ transplant recipients demonstrated that concomitant use of TAC and RIVA significantly increases TAC dose-adjusted trough concentration by 9.2% (P = 0.042). 20 Another study observed a non-statistically significant (P = 0.78) mean increase of 16.5% in TAC troughs in 20 recipients who received DOACs after transplantation. Of the 20 recipients included, 6 had TAC dose adjustments after DOAC initiation complicating the interpretation of these results. 21 Conversely, a prospective study evaluating 11 heart transplant recipients did not find a significant change in TAC (n = 3) or cyclosporine (n = 8) troughs after initiating RIVA. 23
The aim of the current study was to further investigate whether RIVA/APIX affect TAC troughs in solid organ transplant recipients. Clarity of this potential drug-drug interaction is necessary to provide clinicians with the information to make evidence-based decisions regarding TAC dosing and the use of RIVA/APIX in solid organ transplant recipients.
Methods
Study Design and Population Sampling
This was a single-center, retrospective, before-and-after study comparing average dose-adjusted TAC troughs before and after RIVA/APIX initiation in solid organ transplant recipients. The target population was all patients who received RIVA or APIX while taking immediate-release TAC for solid organ transplant-related immunosuppression. To identify this population, the electronic medical records of a 700-bed academic medical center and affiliated outpatient clinics were retrospectively reviewed to identify adult recipients (18 years of age or greater) that met the target criteria between January 2014 and August 2018. Recipients were excluded if they did not have a TAC trough documented within 6 months before and after RIVA/APIX initiation. Empiric RIVA/APIX and/or TAC dose adjustments at the time of RIVA/APIX initiation was not standard practice at this institution. This study was conducted with approval from the overseeing institutional review boards.
Data Collection
Baseline patient characteristics were assessed at the time of RIVA/APIX initiation. Estimated creatinine clearance (eCrCl) was calculated using the Cockcroft-Gault equation. Adjusted body weight was used rather than actual body weight for the Cockcroft-Gault equation when the adjusted body weight was greater than 130% of the actual body weight.
The primary outcome was the change in average dose-adjusted TAC troughs after RIVA/APIX initiation. Trough blood concentrations of TAC were measured by chemiluminescence microparticle immunoassay. A dose-adjusted TAC trough was calculated by dividing the TAC trough by the TAC total daily dose (TDD) from the previous day. 20 Dose-adjusted TAC troughs were used rather than TAC troughs to account for changes in TAC trough goals and TAC doses. TAC troughs measured within 3 days of RIVA/APIX initiation were excluded from analysis to ensure troughs reflected TAC steady state (half-life approximately 24-48 hours). Each recipient’s dose-adjusted TAC troughs before and after RIVA/APIX initiation were averaged and then compared. The first 5 dose-adjusted TAC troughs within the 6-month period before and after RIVA/APIX initiation were used for analysis. Five dose-adjusted TAC troughs were selected with the assumption that most recipients would have 5 TAC troughs within the 6 months before and after RIVA/APIX initiation.
Secondary outcomes included change in average TAC TDD after RIVA/APIX initiation and incidence of acute kidney injury (AKI) and allograft rejection. Acute kidney injury and allograft rejection were evaluated during the first 6 months after RIVA/APIX initiation or until the oral anticoagulant was discontinued. Acute kidney injury was defined using a modified version of the Kidney Disease: Improving Global Outcomes criteria, which included a serum creatinine increase of greater than 0.3 mg/dL within 48 hours or a serum creatinine increase greater than 50% within 7 days. Data on concomitant drug-drug interactions were recorded for recipients initiating or discontinuing medications known to influence CYP3A or P-gp during the time in which TAC troughs were assessed. Supplementary Table 1 provides a comprehensive list of medications that were considered to be CYP3A and P-gp inhibitors or inducers in this study.
Data Analysis
JMP® version 13 (SAS Institute Inc.) was used for all statistical analyses. The sign test was used to compare outcomes before and after RIVA/APIX initiation. Subgroup analyses evaluating RIVA and APIX individually were conducted for the primary outcome and the TAC TDD. Fisher’s exact test and Pearson’s chi-squared test were used to analyze differences in baseline characteristics between recipients started on RIVA compared to APIX. Subgroup analyses of average dose-adjusted TAC troughs for recipients with and without documented CYP3A and P-gp inducers or inhibitors were conducted. A P-value of < 0.05 was considered statistically significant.
Results
Patient Characteristics
A total of 50 transplant recipients were identified as initiated with RIVA/APIX while taking TAC. Of these 50 recipients, 18 (36%) were started on RIVA and 32 (64%) were started on APIX. The most common indication for anticoagulation was AF (56%). Table 1 summarizes baseline characteristics. The median time since transplant was 2.7 years (IQR 1.1, 7.3) and the median eCrCl at baseline was 52.5 mL/min (IQR 39.9, 68.5). All 5 TAC troughs within 6 months were not available for 12 recipients and 23 recipients before and after RIVA/APIX initiation, respectively. The median number of reported troughs within 6 months before and after RIVA/APIX initiation was 5 (IQR 4.75, 5) and 5 (IQR 3, 5), respectively. No statistical difference in age, kidney function, transplanted organ, or time since transplant was identified between recipients started on RIVA compared to those started on APIX.
Baseline Characteristics Assessed at Time of RIVA/APIX Initiation.
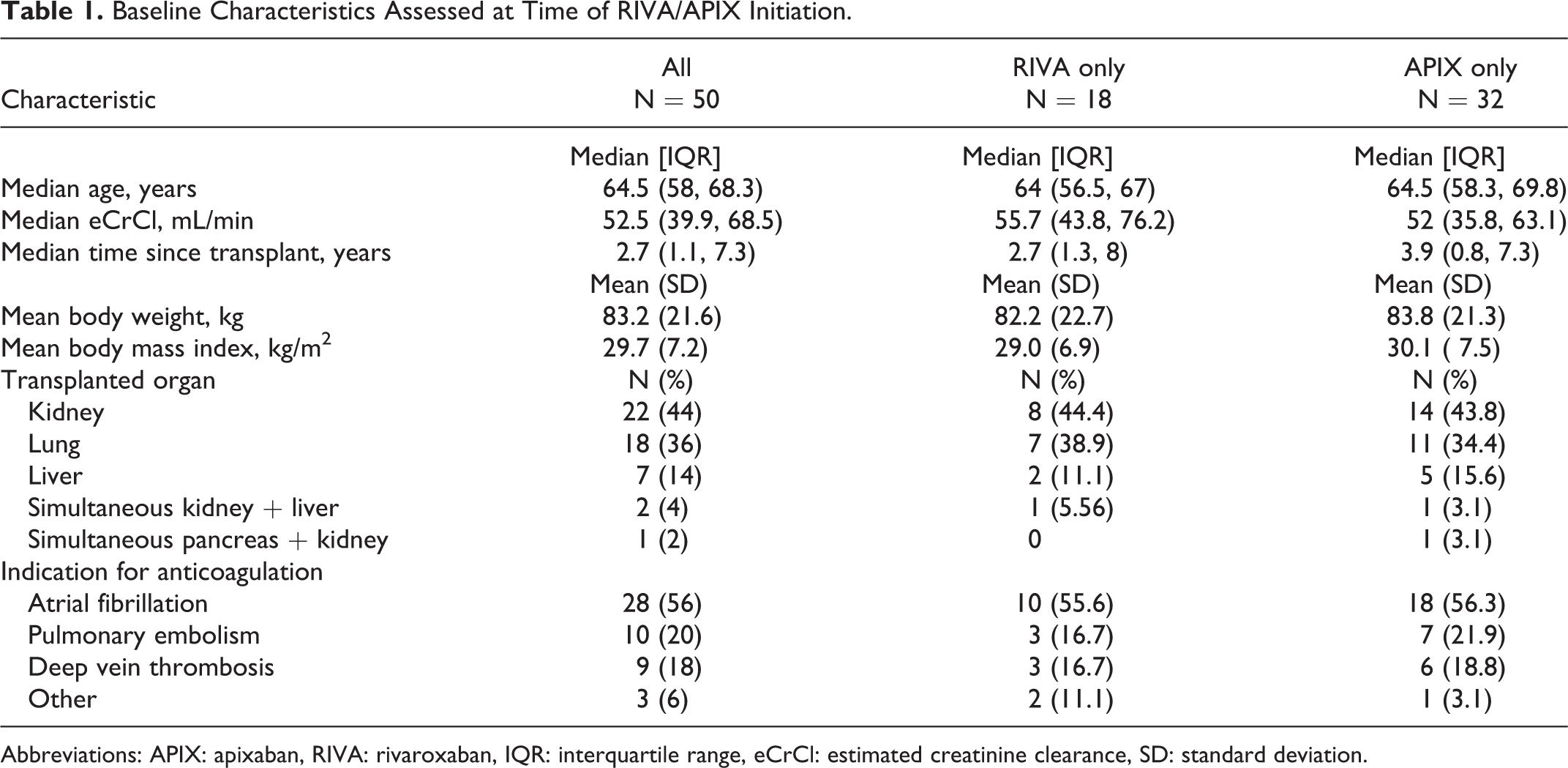
Abbreviations: APIX: apixaban, RIVA: rivaroxaban, IQR: interquartile range, eCrCl: estimated creatinine clearance, SD: standard deviation.
Primary and Secondary Outcomes
There was no statistically significant difference in average dose-adjusted TAC troughs before and after RIVA/APIX initiation (Table 2A). Similarly, a subgroup analysis of RIVA only and APIX only showed no difference in average dose-adjusted TAC troughs after initiation for either medication individually (Table 2A). There was no difference in TAC TDD before and after RIVA/APIX initiation (Table 2B).
Comparison of Median Dose-Adjusted Tacrolimus (A) and Total Daily Dose (B) After Initiation of RIVA and APIX.
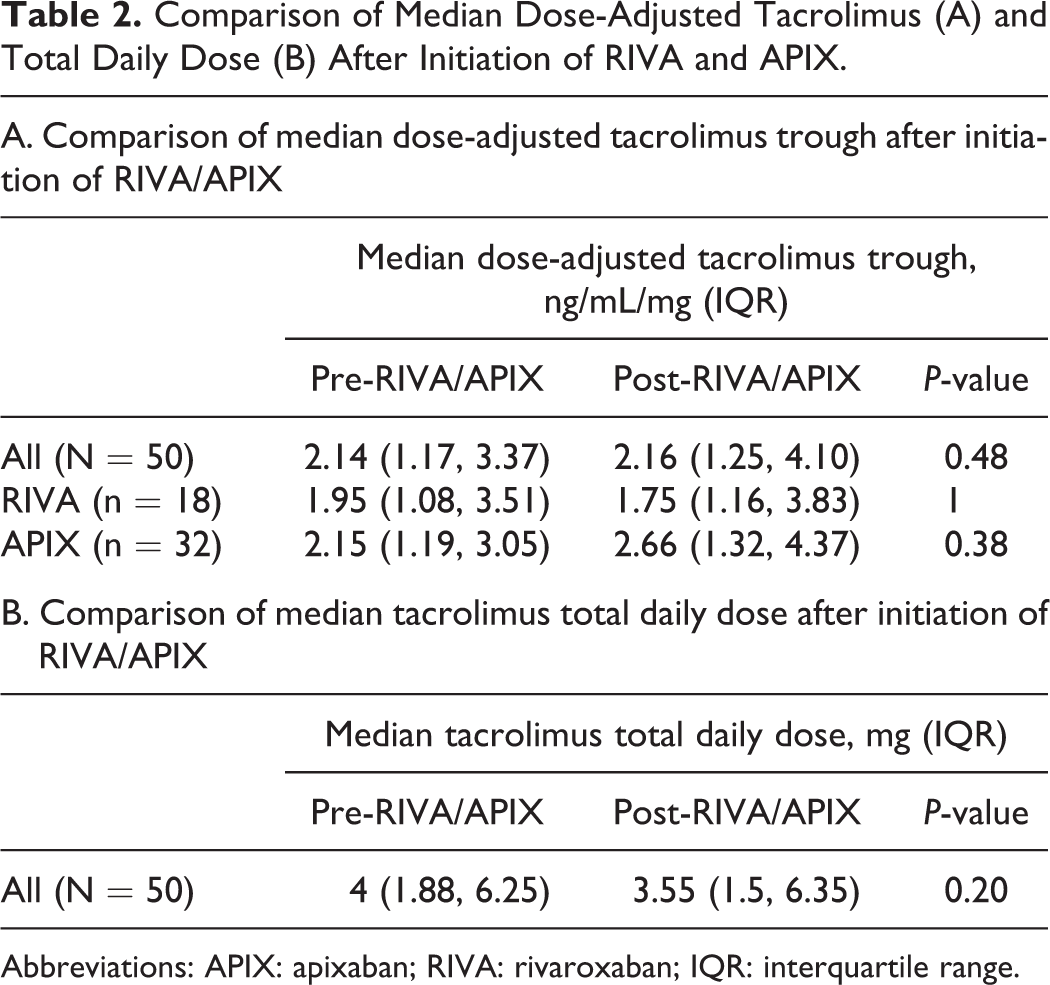
Abbreviations: APIX: apixaban; RIVA: rivaroxaban; IQR: interquartile range.
Fourteen recipients (28%) developed an AKI during the time in which TAC troughs were assessed. Of these 14 recipients, 4 (28.6%) were taking RIVA and 10 (71.4%) were taking APIX. At the time of AKI, 4 recipients (28.6%, 3 lung transplant recipients and one kidney transplant recipient) had RIVA/APIX doses higher than the FDA approved dosing. One recipient (kidney transplant) taking APIX was diagnosed with T-cell-mediated rejection.
Thirty-one recipients (62%) initiated or discontinued a known CYP3A or P-gp inducer or inhibitor during the time in which TAC troughs were assessed. A subgroup analysis evaluating the 19 recipients without a change in a concomitant CYP3A or P-gp inducers or inhibitors was conducted. No difference was found in average dose-adjusted TAC troughs or TAC TDD after RIVA/APIX initiation (Table 3).
Comparison of Median Dose-Adjusted Tacrolimus Trough and Median Tacrolimus Total Daily Dose After Initiation of RIVA/APIX for Patients Without a Change in a Concomitant CYP3A or P-Gp Inducers or Inhibitors (N = 19).
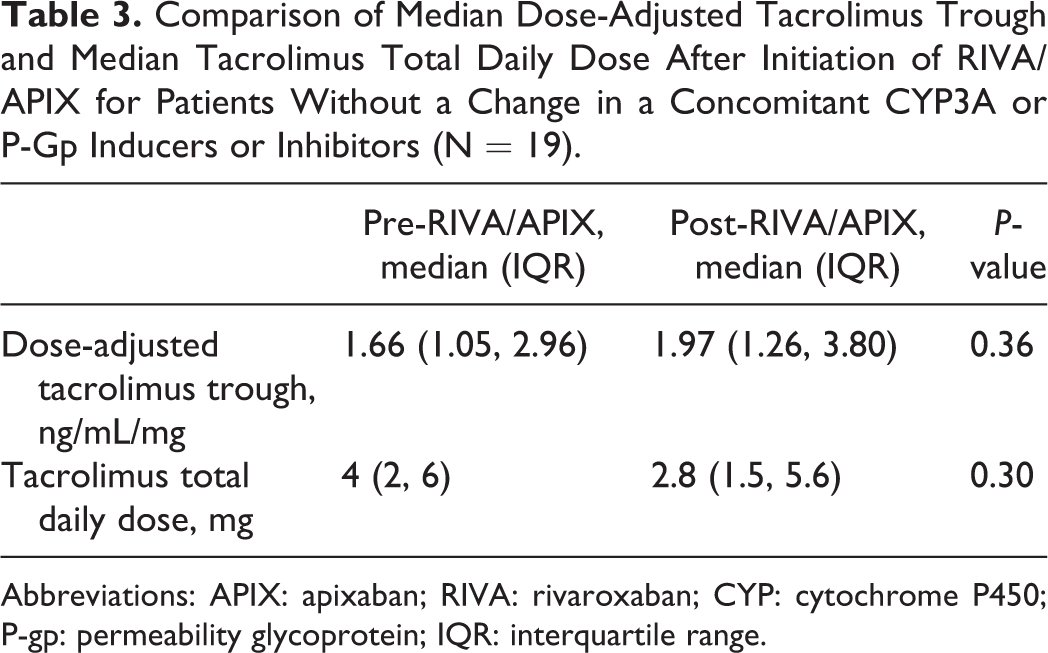
Abbreviations: APIX: apixaban; RIVA: rivaroxaban; CYP: cytochrome P450; P-gp: permeability glycoprotein; IQR: interquartile range.
Discussion
This is the largest study to date evaluating the effects of RIVA/APIX on TAC troughs in solid organ transplant recipients. No significant difference in average dose-adjusted TAC troughs after RIVA/APIX initiation was found in the combined or subgroup analyses. A previously published retrospective study identified a total of 29 recipients that were started on RIVA/APIX while taking TAC. Like the current study, their analysis found no difference in average dose-adjusted TAC troughs after RIVA/APIX initiation in the combined analysis and the APIX only sub-group analysis. 20 Their conclusion that APIX does not influence TAC troughs was strengthened by the current study’s larger sample taking APIX (n = 32 versus n = 7). However, their subgroup analysis of recipients taking RIVA (n = 22) revealed a statistically significant increase of 9.2% in the dose-adjusted TAC trough after RIVA initiation. 20 In contrast to the current study, a 100-day average of dose-adjusted TAC troughs rather than an average of the first 5 dose-adjusted TAC troughs within 6 months was used. The study found no difference in outcomes when the 100-day average was compared to the average of the first 3 dose-adjusted TAC troughs. 20 Therefore, it is unlikely the selection of dose-adjusted TAC troughs in the current study led to the observed differences.
Information on allograft rejection and AKI was collected as surrogate outcomes of altered TAC exposure. If RIVA/APIX reduced TAC exposure, a large proportion of recipients developing rejection may have been identified, however, this was not the case. Only one recipient developed T cell-mediated rejection that was diagnosed less than 3 weeks after starting APIX. Given the short time frame after starting APIX, it is unlikely the rejection was caused by APIX.
The incidence of AKI was collected as a surrogate outcome associated with increased TAC exposure. Acute kidney injury was chosen as a clinical outcome of potential TAC toxicity rather than other signs or symptoms, such as neurotoxicity, because AKI could be collected objectively. Just over one fourth (n = 14, 28%) of the studied sample developed an AKI while on RIVA/APIX. The reported incidence of AKI in solid organ transplant recipients varies widely. One retrospective analysis reported a range of 11-58% in adult kidney transplant recipients, 25 while another study reported a 36% incidence of AKI within first year in a non-kidney transplant pediatric population. 26 As there was no control group in the current study, it is difficult to discern if the AKI rate was directly related to the initiation of RIVA/APIX. However, given the previously reported incidence, it is unlikely initiating RIVA/APIX led to the observed AKI rate.
There are limitations to the present study. First, this was a retrospective analysis which limited the ability to control for concomitant medications that influence CYP3A4/5 or P-gp. To help quantify the impact of concomitant medications on the primary outcome, a subgroup analysis of recipients without these drug interactions (n = 19, 38%) was conducted and revealed no difference in outcomes. Although this was a smaller population, it supports the results of the larger analysis. Additionally, it is well known that CYP3A4/5 is a highly polymorphic enzyme. Differences in the genes encoding the CYP3A4/5 proteins have been shown to influence the metabolism of TAC. 20 Pharmacogenomic data were not available transplant recipients in this study; therefore, the phenotype of CYP3A4/5 could not be predicted.
Lastly, the present study did not assess effects of TAC on the safety and efficacy of RIVA/APIX as drug-specific anti-Xa levels (anti-Xa for RIVA or APIX) and thrombosis and bleed rates were not collected. Drug-specific anti-Xa levels were not routinely collected at this study’s site and finding a difference in thrombosis and bleeding events would have likely required a much larger sample size than the population accessible to the study.
Based on these results, it was unlikely that RIVA/APIX had a clinically significant impact on TAC troughs. A change in average dose-adjusted TAC troughs or average TAC TDD after RIVA/APIX initiation was not found. It is doubtful the 0.02 mg/dL difference between the before and after RIVA/APIX dose-adjust TAC troughs would be clinically significant if a larger population had been reviewed. Therefore, the results of this study contribute to the growing body of evidence suggesting that preemptive TAC dose adjustments are likely unnecessary when starting RIVA/APIX for solid organ transplant recipients. Due to the incidence of AKI observed in this study’s population, careful monitoring of renal function is recommended for transplant recipients started on RIVA/APIX while taking TAC to assess the necessity of RIVA/APIX dose adjustments or discontinuation based on renal function. Additional studies are required to evaluate the impact of TAC on RIVA/APIX pharmacokinetics and pharmacodynamics.
Supplemental Material
Supplemental Material, sj-pdf-1-pit-10.1177_15269248211024601 - The Impact of Rivaroxaban and Apixaban on Tacrolimus Trough Levels
Supplemental Material, sj-pdf-1-pit-10.1177_15269248211024601 for The Impact of Rivaroxaban and Apixaban on Tacrolimus Trough Levels by Aileen C. Scheibner, Crystal Franco-Martinez, Elisabeth Kincaide, Reed Hall and Christina Long in Progress in Transplantation
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.