
Abstract
Verapamil has been used in perfusion solution to improve kidney performance, but evidence was anecdotal, and no research has been reported on recipient outcomes. Our organization began a program to evaluate Verapamil’s effect on pump performance, transplant rate, and recipient outcomes. One kidney in a pair was treated with Verapamil and one with standard perfusion. Donor inclusion criteria were age 18 or older and both kidneys were placed on the pump. The laterality of the treated kidney was changed every month to reduce bias. From January 1, 2020 to June 30, 2020, 88 kidneys were evaluated. Of those, 21 donors had both kidneys transplanted to different recipients, so for those 42 kidneys, recipient outcomes were evaluated. Small improvements in pump performance were observed in the Verapamil-treated kidneys and more were transplanted. No clinical differences were found in recipients between the Verapamil-treated and standard perfused kidneys. A larger cohort is needed to determine whether differences are significant.
Keywords
Background
In 2019, over 20% of kidneys recovered from deceased organ donors went unused. 1 Many of these discarded kidneys came from older donors. There is potential for growth in transplantation if these kidneys could be transplanted, so the need to develop the processes to transplant less-than-ideal kidneys is great. Organ Procurement Organizations (OPOs) have tried various methods to improve kidney function post-recovery, including the use of vasodilator medications to decrease vascular resistance, but these practices are based on anecdotal evidence. Marginal kidneys, especially, could benefit from a method of improving vascular resistance while undergoing hypothermic pulsatile kidney perfusion (HPKP).
Our OPO's historical practice for kidneys undergoing HPKP was for our perfusionist to adjust perfusion pressure based on vascular resistance and flow rate as well as medicate the perfusate with Verapamil based on these parameters. We were interested in evaluating if the addition of Verapamil in the preservation solution affected vascular resistance, flow rate, or recipient outcomes.
There has been some interest in using Verapamil in both recipients and donor kidneys prior to transplant to improve renal function. No studies of Verapamil evaluated it as an additive to the solution in a perfusion device. A 1991 study suggested that Verapamil prevented cyclosporin-A induced decreases in renal function in mice and renal transplant recipients. 2 Compared with the control group, Verapamil recipients had improved renal parenchymal diastolic blood flow velocities on the first day post-surgery. Verapamil recipients also had improved graft function after one year. This study was limited by its small sample size of 59 patients. 2 A 2019 study evaluated the effect of Verapamil in kidney recipients over 10 years. Their cohort included living donors, brain dead donors, and donation after circulatory death donors, and administration did not improve graft function after transplant in any group. 3 A 2008 study that evaluated the effects of Verapamil on recipients, that had their donated grafts flushed with a preservation solution prior to transplant, found that the addition of Verapamil can improve long-term graft function. 4 This study had limitations noted including the fact that it was not designed with a paired kidney framework. Some of the realized differences noted could have been contributed to the donor graft quality, not necessarily the administration of Verapamil. The kidneys were also given a one-time flush of solution with medication rather than being given a continuous positive pressure administration, such as a hypothermic perfusion pump.
Clinical Relevance to Practice
Perfusion parameters are used by transplant centers as a predictor of graft outcomes. 5 Flow and resistance parameters can be used to predict delayed graft function and graft survival, so they are frequently evaluated by transplant centers when making the decision whether to accept the organ. A 6-month sample of 123 kidneys recovered and placed on HPKP at our organization revealed that discard rate decreased as the terminal flow rate increased and significantly decreased once terminal flow rate exceeded 100. Due to this known correlation between terminal flow rate and discard rate, we were interested in evaluating our practice of Verapamil administration to better understand whether administering Verapamil to kidneys placed on HPKP could lead to more kidneys being placed for transplant. The impact of Verapamil in HPKP is not well studied or understood, but many OPOs use it or other vasodilator medications in perfusion solution with the intent of improving kidney perfusion resistance and flow. If OPOs could understand how to improve kidney function when undergoing HPKP, then they may be able to increase the transplant rate of less-than-ideal kidneys.
Practice Issues
To understand the impact of Verapamil, one OPO developed a performance evaluation of Verapamil administration using donated paired kidneys. For each set of paired kidneys that both underwent HPKP, one kidney was pumped with Kidney Perfusion Solution from Organ Recovery System (KPS-1) alone and one kidney had Verapamil added to the KPS-1. For the Verapamil-treated kidneys, the OPO followed its previously established protocol. The protocol required an initial dose of 2.5 mg added to 1 L of perfusion pump solution, followed by an additional 2.5 to 7.5 mg over 4 hours, based on vascular resistance and flow rate. Both kidneys followed the same titration of perfusion pressure with identical initial pressure settings. We alternated the laterality of the kidney to receive Verapamil each month to decrease a laterality bias. No other change in practice was made regarding the selection of donor kidneys that underwent HPKP. We collected data about pump resistance, flow rate, transplant rates, and recipient outcomes from January 1, 2020, through June 30, 2020. The donors included in the data collection had to be over 18 years old at the time of death, both kidneys had to be recovered for transplant and placed on machine perfusion for a minimum of 4 hours and have research authorization. This program assessment was approved by the Medical Advisory Board of the OPO prior to implementation.
Program Assessment
To evaluate Verapamil's impact, data was collected related to kidney vascular resistance and flow, whether the kidney was transplanted and recipient outcomes. The HPKP parameters were documented in electronic health record per normal practice. Flow rate and resistance were documented immediately following the placement of the kidneys on the pump and at 2 and 4 hours. Average flow rate and resistance measurements were compared between the Verapamil-treated kidneys and the untreated kidneys. Recipient outcome data was obtained through United Network for Organ Sharing (UNOS), as reported by the transplant centers. It included recipient discharge creatinine and whether they experienced delayed graft function, defined by UNOS as requiring dialysis in the first week following transplant. Creatinine clearance was calculated based on recipient age, discharge creatinine, and weight on the match run. Recipient outcome data compared both the average discharge creatinine and creatinine clearance and the median discharge creatinine and creatinine clearance to reduce the effect of any potential outliers.
Program Analysis and Summary
At the end of June, we had collected data from 44 deceased donor kidney pairs, or 88 kidneys. Of the kidneys that received Verapamil, 62% of those recovered resulted in successful transplantation. Of the kidneys that received preservation solution only, 52% were transplanted. This difference represents an additional 4 kidneys transplanted from the group that received Verapamil during 6 months of data collection. Although this represents a positive difference between the 2 groups in transplantation rate, this was not a statistically significant difference and could be due to chance. A larger data set would be needed to determine whether this is a statistically meaningful observation.
All HPKP kidneys that were enrolled in this program were used to evaluate what, if any, effect the medication may have on perfusion parameters of the kidney undergoing HPKP. The 2 parameters that were evaluated were vascular resistance and perfusion flow rate. Both the flow and resistance for kidneys that were treated with Verapamil had superior performance. Notably, there was an approximate 16% lower resistance and 9% higher flow rate in the Verapamil-treated kidneys at the final time measurement interval. It was also noted that both vascular resistance and flow rate improved as time intervals progressed. Although this was true for both the treated and untreated kidneys, there was a more positive trend in the treated kidneys (see Figure 1). In any future studies, additional time intervals could be included to determine whether improvement trends continue out past the 4-hour mark selected for this program.
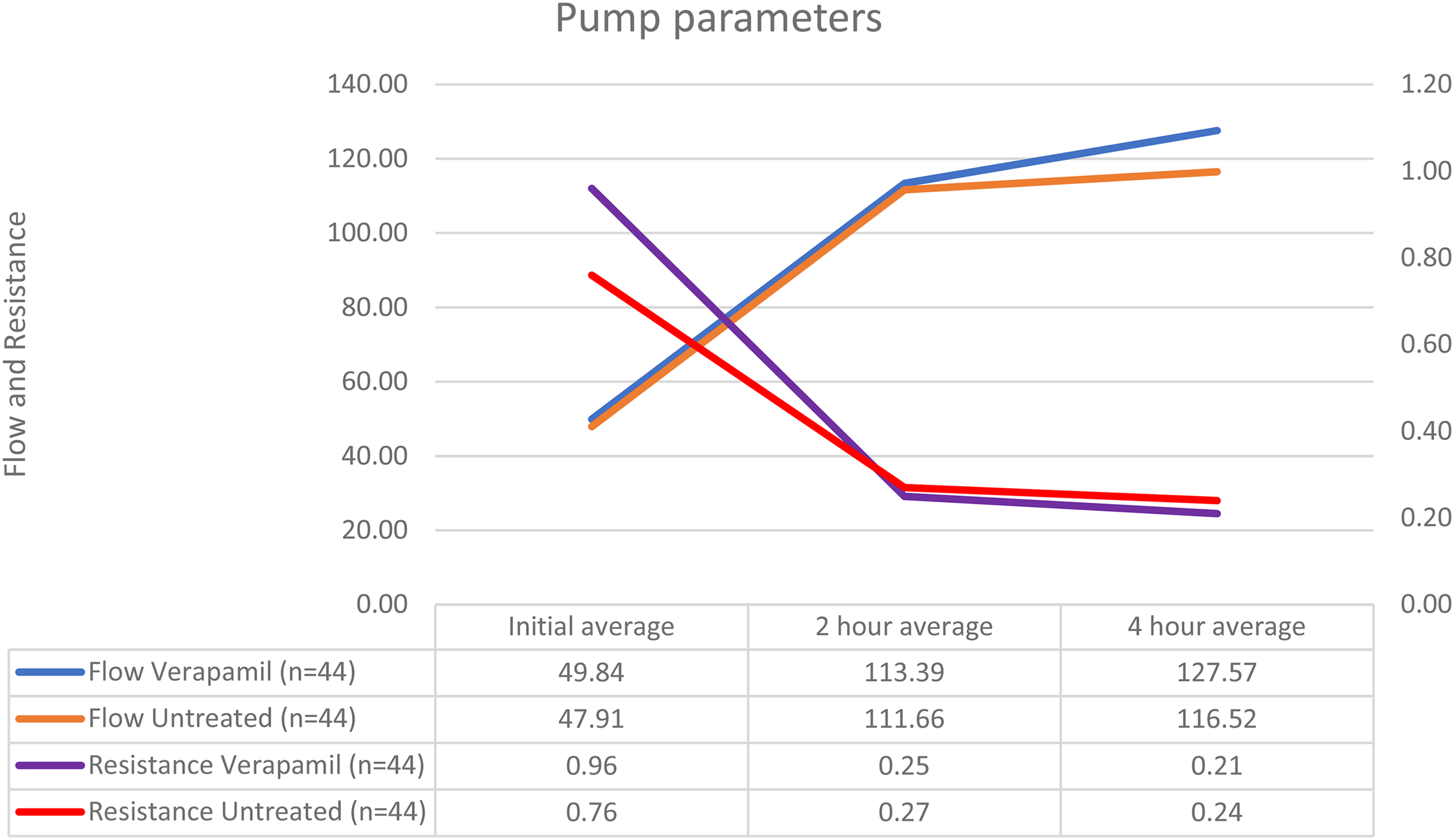
Evaluation of flow and resistance of Verapamil-treated kidneys and untreated kidneys.
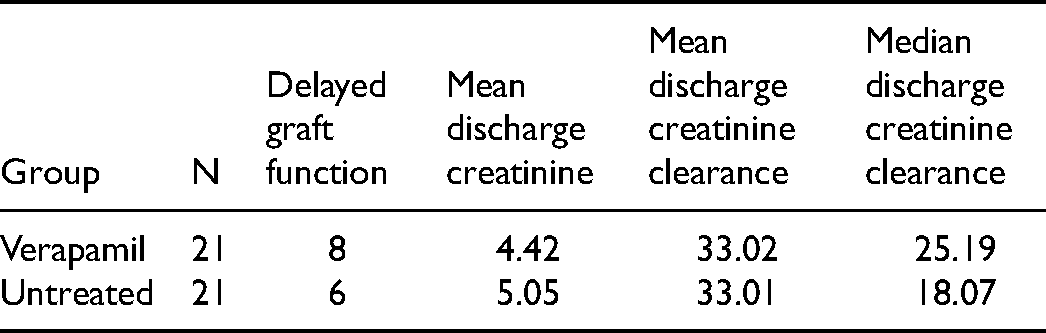
To examine the recipient outcomes, the only kidneys that were included in this analysis were those from donors where both kidneys were transplanted to different recipients. This was done to eliminate any potential bias associated with a more optimal donor kidney being used for comparison, where the difference could have been impacted by the donor quality disparities. There was a total of 42 kidneys transplanted from donors where both kidneys were transplanted (21 in the Verapamil-treated group and 21 in the untreated group). Recipients who received kidneys from donors that were treated with Verapamil performed similarly to kidneys from donors that were not treated with Verapamil. Delayed graft function was experienced by 8 recipients in the treatment group and 6 recipients in the untreated group (38% vs 30%, respectively). Discharge creatinine clearance was similar as well, with an average of 33 in both the treatment group and the untreated group (Table 1).
Comparison of Recipient Outcomes From Recipients Who Received Verapamil-Treated Kidneys and Those Who Received Untreated Kidneys
Implications for Practice
The early recipient outcomes were similar between those who received kidneys that were medicated compared to those who received pump solution only. Both the kidney perfusion parameters and the kidney transplantation rates were greater for the treated kidneys compared to the untreated kidneys though not to a level that meets statistical significance. These findings need further study and larger sample size to understand the significance and impact on recipients. Limitations of our evaluation include the sample size and lack of long-term recipient graft function data availability at the time of this publication. As a result of this pilot program, the OPO will continue to medicate kidney pump solution while working to facilitate a larger study to further evaluate the effect of Verapamil on kidney transplantation rate and graft performance over time. Additionally, recipient follow-up data at year one will be tracked. Lastly, future studies should consider more time intervals and examine donor demographics such as donation after circulatory death, age, and kidney donor profile index (KDPI) in the analysis of the impact of Verapamil.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.