
Abstract
Introduction
Solid organ transplant recipients experience greater cardiometabolic risk than the general population. Following a Mediterranean dietary pattern has been shown to reduce cardiometabolic risk. This study aimed to assess multidisciplinary clinician perspectives of routine nutrition care for kidney and liver transplant recipients and barriers and enablers to implementation of the Mediterranean dietary pattern.
Methods
Semi-structured individual interviews were conducted with clinicians in a metropolitan health service at tertiary/quaternary transplant centres involved in longer-term management of kidney and liver transplants recipients. Audio-recorded interviews were transcribed verbatim and analysed using thematic content analysis.
Findings
Nineteen clinicians (9 medical officers, 5 dietitians, 3 nurses and 2 other allied health professionals) were interviewed. Four themes with 11 subthemes were identified: the Mediterranean dietary pattern is not part of routine care (there are competing clinical priorities; healthy eating principles aligned with but not the full dietary pattern are recommended); variation in knowledge and acceptance of this dietary approach (variances in information sources and degree of knowledge of Mediterranean dietary pattern clinical evidence); nutrition advice is influenced by service delivery and culture (there is lack of consistent nutrition advice; limited consultation time; and reliance on existing patient education resources); and patient-centred care influences decisions on nutrition advice (clinicians do not know how to recommend this dietary pattern in a patient-centred manner).
Discussion
The Mediterranean dietary pattern is not considered part of routine post-transplant nutrition care. To be implemented in these services intervention strategies which address the identified barriers and potential enablers need to be considered.
Keywords
Background
Organ transplantation is the clinical intervention most likely to prolong life in patients with end stage kidney and liver diseases. 1 When successful, liver and kidney transplants improve survival and quality of life. 2 However, this population have increased cardiometabolic risk as a result of pre-existing lifestyle related risk factors and metabolic consequences of immunosuppression.3,4
Immunosuppressive medications are required for graft survival but are associated with increased prevalence and severity of cardiovascular risk factors including hypertension, obesity, diabetes and dyslipidaemia. 5 These risk factors impact overall survival and quality of life with cardiovascular disease a leading cause of death for transplant recipients. 1
Many chronic disease practice guidelines have transitioned away from recommending specific macronutrient or calorie restriction to the promotion of overall healthy dietary patterns, which are focused on the variety and combinations of foods in the diet. There is strong evidence to suggest that following the Mediterranean dietary pattern, commonly referred to as the Mediterranean diet (MedDiet), reduces the risk of chronic disease and may improve cardiometabolic risk factors that contribute to this burden in transplantation, including dyslipidaemia, diabetes, hypertension and obesity.6–8 Key principles of the MedDiet are regular intake of plant foods (fruits, vegetables, extra virgin olive oil, wholegrains, legumes and nuts); moderate intake of seafood, poultry and dairy; and low intake of red meat and processed foods.9,10 Although there is limited evidence on the impact of the MedDiet on clinical outcomes for kidney and liver transplant recipients broadly, it has been suggested that following MedDiet principles may lead to decreased risk of new onset diabetes 11 and improved kidney function 12 post-kidney transplant. In liver transplant recipients, there is some evidence that unhealthy eating patterns may have an impact on cardiometabolic risk 13 and recent trial data demonstrated this patient group can adhere to the MedDiet 14 and this contributed to improvement in metabolic health and quality of life. 15
It is unclear to what extent the MedDiet is being implemented in routine nutrition care to this patient group. A recent national survey of dietitians in Australia found that the MedDiet was not routinely recommended to liver or kidney transplant recipients. 16 For effective translation of evidence into routine care, current practice and existing barriers and enablers to the implementation of this evidence in the local setting should be identified. 17 Thus, the aim of this study was to assess clinician perspectives of routine nutrition care within state-wide kidney and liver transplant services with a focus on identifying whether the MedDiet is recommended and barriers and enablers to implementation.
Methods
This study used a qualitative descriptive design and aligned with the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines. 18 The study protocol was approved by the Metro South Health Human Research Ethics Committee (approval number HREC/2019/QMS/52598). Informed consent to participate was obtained either in written format or verbally (whereby the investigator signed on the participant’ behalf and recorded the date and time). All participants were provided with a detailed information sheet explaining the purpose of the interview, which was entirely voluntary, and were given the opportunity to ask questions, prior to consenting.
Setting and Sampling
Eligible participants were dietitians and other clinicians (medical officers, nurses, and other allied health professionals) who were routinely treating kidney or liver transplant recipients in a subacute or outpatient setting of two hospitals within the metropolitan public service Metro South Health, Queensland, Australia, and had a role related to providing nutrition care or dietetics referrals. One of these hospitals hosts state-wide kidney and liver transplant centres, including specialist outpatient clinics, and the other hospital services patients post-transplant as outpatients in broader hepatology and renal clinics. At the time of recruitment, it is estimated that across the two hospitals there were a total of 5 dietitians and 25 non-dietetic clinicians routinely managing relevant transplant patients who would have been eligible to participate.
Dietitians were identified purposively by the research team and recruited first. In interviews, dietitians suggested relevant other clinicians and this initiated a snowball method. Invitation to participate was via email from the principal investigator. Each participant was deidentified with a code and ID with “D” for dietitian and “C” for non-dietetic clinicians.
Data Collection
Semi-structured interview schedules were developed by the principal investigator with consultation from the research team. These included planned open questions and potential prompts with separate versions for dietitians and other clinicians, modified following pilot testing with a dietitian and medical officer. Interview questions explored clinicians’ current roles and priorities in nutrition care, their understanding of the MedDiet, and perceived barriers and enablers to implementation of the MedDiet in routine care. All interviews were conducted by the principal investigator who had undertaken theoretical training and received guidance from experienced qualitative researchers. Interviews were in the participant's workplace either face-to-face or via telephone based on convenience for the participant. Because the interviewer worked as a researcher at one of the hospital recruitment sites, professional interactions had occurred with six of the participants prior to the interviews. Interviews were audio-recorded then transcribed verbatim through an audio to text automatic transcription online service (Temi, 2020, CA USA). The texts were checked for the accuracy of each interview transcript prior to analysis. The semi-structured interview schedules have been published elsewhere. 19
Data Analysis
Descriptive analysis was utilised to summarise participant characteristics. Transcripts from each interview were coded and analysed for themes using thematic content analysis. 20 Microsoft Excel version 16.30 was used to manage the data. Both deductive and inductive analysis approaches were utilised simultaneously. A deductive approach was employed through use of a coding framework that included key research questions as categories for managing the coding, as well as application of the Theoretical Domains Framework in the theming process. The Theoretical Domains Framework summarises known influences on health professional practices, with a focus on implementing evidence into routine care, and has 14 domains. 21 An inductive approach was used in that coding was derived from line-by-line analysis of the participant responses, with the key research questions and theoretical framework providing a lens, but no pre-determined codes were applied. Two investigators (TMH and HLM) each independently coded 40% of transcripts. The remaining 60% of transcripts were coded by TMH and reviewed by HLM. Preliminary findings were discussed and compared to identify points of difference and generate further analysis. Once completed, triangulation was done by reviewing coding and participating in consensus discussions with the broader research team. Through this process and ongoing review of the transcripts and codes by the lead investigator, understanding of themes and subthemes was developed and consolidated. For presentation of results, themes were also mapped to illustrative quotes, theoretical domains, and barriers and enablers to practicing the MedDiet. Consideration of the clinicians’ MedDiet knowledge and whether principles were practiced was guided by George et al. (2018). 22 We used the authors’ descriptions of nutrient composition profile and key food-based components of the MedDiet to identify similarities, differences and gaps when comparing to the clinicians’ descriptions of the MedDiet as well as their key dietary priorities with patients, to identify similarities, differences, and gaps.
Findings
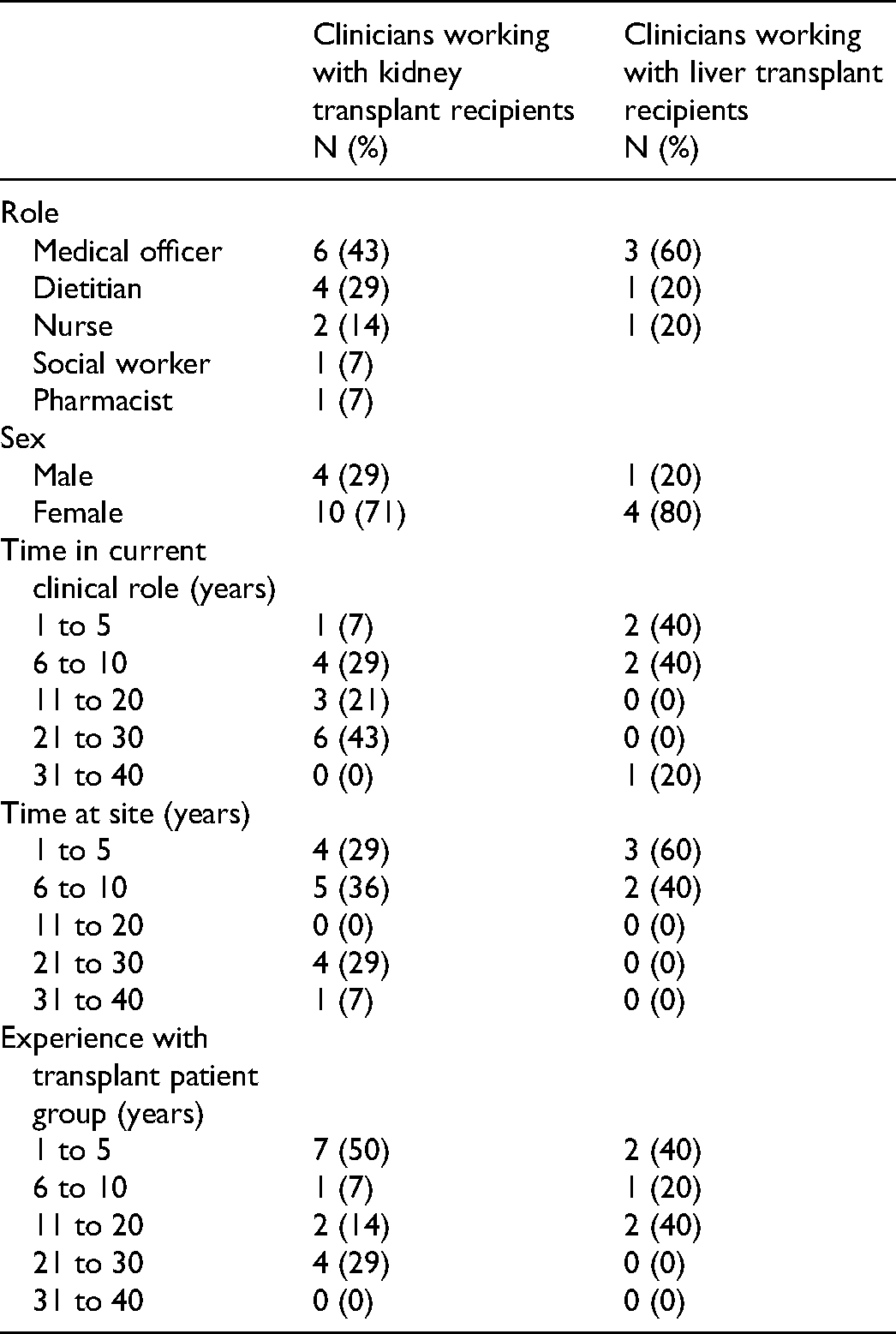
Twenty-five eligible clinicians were invited to participant, of which 5 dietitians and 14 non-dietetic clinicians (9 medical officers, 3 nurses, 1 pharmacist and 1 social worker) were recruited and interviewed (
Characteristics of Multidisciplinary Kidney or Liver Transplant Clinicians Participating in Qualitative Interviews.
Four overarching themes (
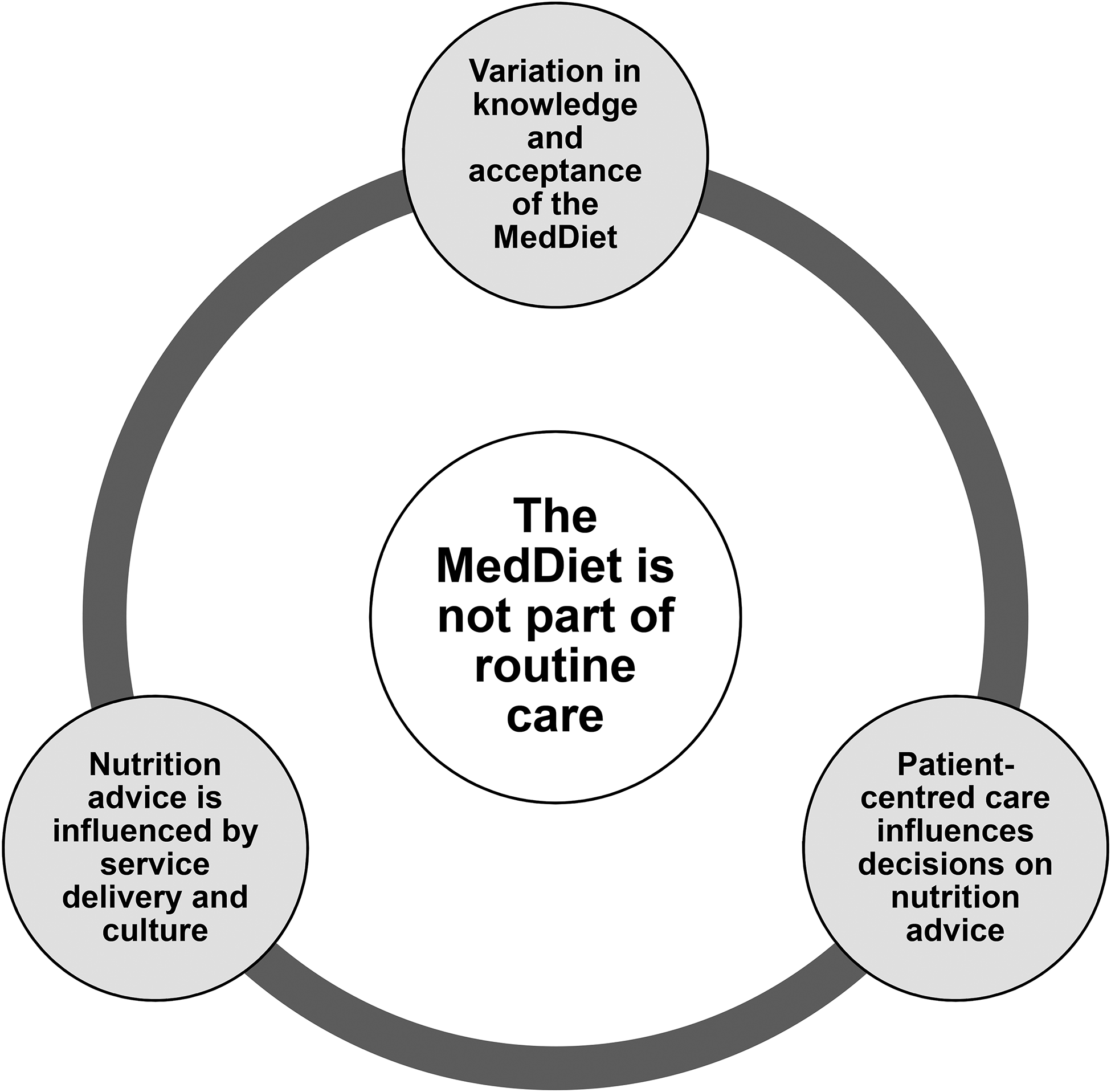
Schematic of four major themes, including one central theme, generated from interviews with multidisciplinary clinicians managing kidney and liver transplant recipients. MedDiet: Mediterranean dietary pattern.
Major Themes Mapped to Barriers and Enablers to Implementing the Mediterranean Dietary Pattern in Routine Care of Liver and Kidney Transplant Recipients and the Theoretical Domains Framework.
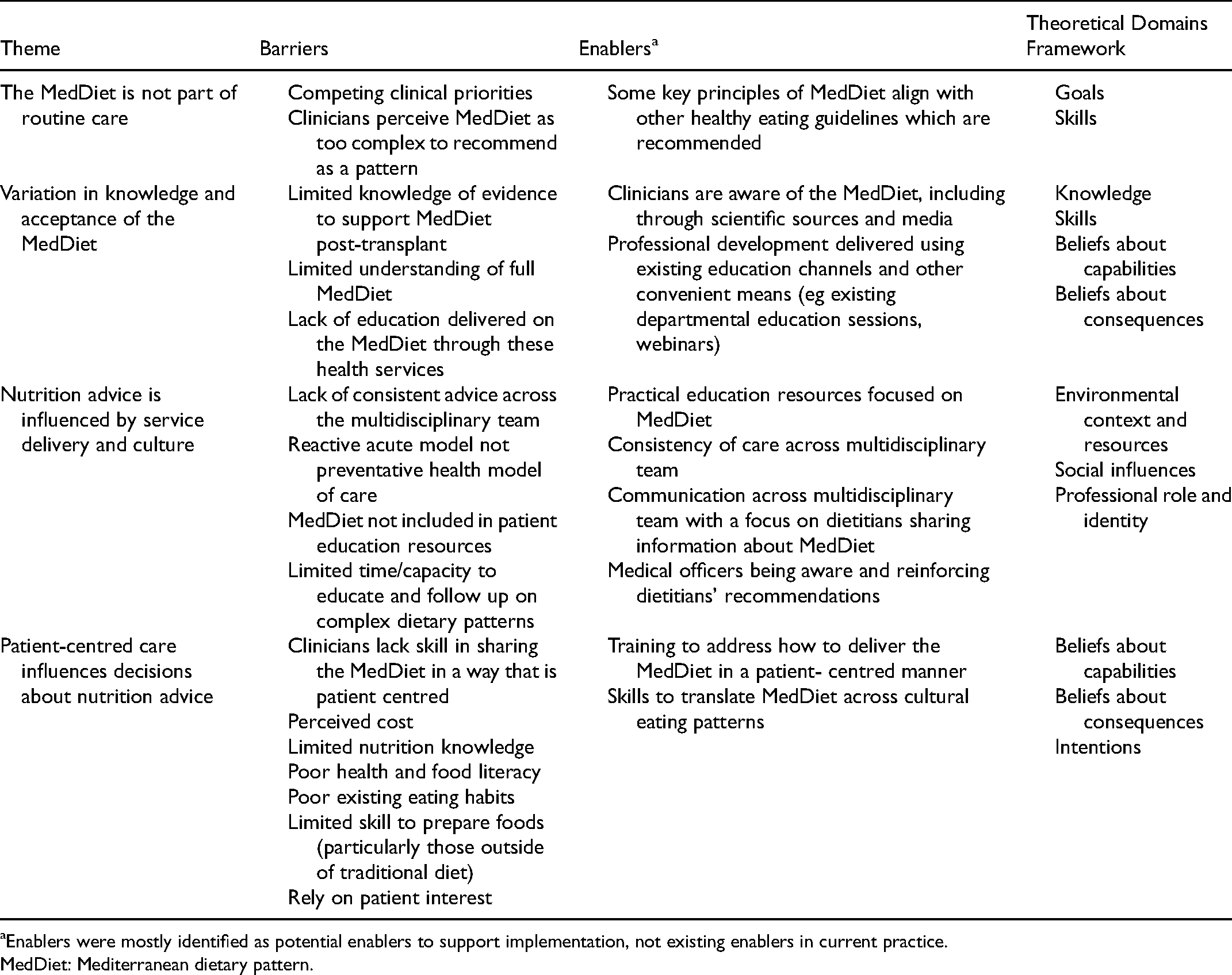
Enablers were mostly identified as potential enablers to support implementation, not existing enablers in current practice.
MedDiet: Mediterranean dietary pattern.
The Mediterranean Dietary Pattern Is Not Part of Routine Care
Aligned Healthy Eating Principles but Not the Mediterranean Dietary Pattern are Recommended
Though some key principles of the MedDiet were being recommended to patients, the dietary pattern itself was not. Clinicians did not recommend the MedDiet outright, though they acknowledged utilising general healthy eating principles that do align with the MedDiet. Dietitians indicated they draw on MedDiet principles, including increasing fruit and vegetable consumption and limiting red meat intake, however they do not present this to patients as a Mediterranean diet. As one dietitian said: “I don't ever specifically go into like a full Mediterranean diet education” (D05)
Non-dietetic clinicians also acknowledged awareness of healthy elements of the MedDiet, but they didn't consider recommending the MedDiet. A perceived lack of value in recommending the MedDiet was also highlighted. As one clinician suggested: If you have a diet where you have a mix of… some red meat but fish and chicken and mix it with vegetables and reasonable amounts of fruit and all that sort of stuff, I’m not sure that suddenly going from that to Mediterranean necessarily is going to make some earth-shattering difference (C11)
Competing Clinical Priorities
The need to manage competing clinical priorities emerged as a barrier to the MedDiet being part of routine care. One non-dietetic clinician stated: “A lot of it with transplant patients is food hygiene, making sure they don't put on weight after transplant, managing their diabetes post-transplant” (C04)
Clinicians indicated their priorities to consider were food safety, weight management (both weight gain and malnutrition) and diabetes management. No clinician spoke of using the MedDiet to address these factors.
Variation in Knowledge and Acceptance of the Mediterranean Dietary Pattern
Discrepancies in Knowledge of the Mediterranean Dietary Pattern Across Clinicians
Though all clinicians had heard about the MedDiet, knowledge of its features and evidence for benefits varied. Some non-dietetic clinicians had very limited understanding of the pattern and could only identify a few key foods. For instance, one such clinician asked about understanding of the MedDiet responded: “It's a clean diet, more so, than anything else, but that's really all.” (C01)
Dietitians and some non-dietetic clinicians identified most key foods and how key food groups are distributed in the MedDiet, however no clinician described a comprehensive understanding of specific or practical features of the pattern. This lack of in-depth knowledge was identified as a barrier to recommending the MedDiet to patients. When discussing potential enablers to implementing the MedDiet in practice one dietitian identified: “Probably just my knowledge and confidence in giving those sorts of recommendations … being able to answer some of the questions a bit more specifically for the patients… more specific advice around meal types.” (D01)
Clinicians that had experience working with other chronic disease groups where MedDiet may be utilised, for example non-alcoholic fatty liver disease, generally had better understanding of the pattern, and how it may be implemented with patients.
Dietary Information Sources Vary
There was clear variation across professions in terms of where knowledge about the MedDiet had been sourced. Dietitians had accessed information about the MedDiet from a range of sources, including conferences, professional development events, scientific literature and communication with other clinicians. One dietitian suggested: “I’ve actually been to a few conferences, and PD [professional development] dinners and things where they’ve discussed quite a bit of evidence about it [the MedDiet] actually” (D03)
Some non-dietetic clinicians indicated they also had gained knowledge from a range of sources including popular media, meetings and less frequently scientific literature.
For example, one non-dietetic clinician indicated: “At meetings and in talks, hear about them [the MedDiet] occasionally referred to in, in papers…You read a lot about it in the lay press” (C11)
Other clinicians reported having accessed fewer sources of information with the lay press and non-scientific literature highlighted. For example, one such clinician when asked about sources of information about the MedDiet stated: “Oh, like cookbooks. We’ve got a cookbook at home.” (C08)
Overall Acceptance of the Mediterranean Dietary Pattern as Healthy, but Evidence Linking to Transplant Less Clear
Dietitians and specific non-dietetic clinicians were generally aware of evidence that the MedDiet may be beneficial for chronic conditions such as diabetes, hypertension, and cardiovascular disease. In contrast, other non-dietetic clinicians had almost no awareness of evidence for the MedDiet. In the context of transplant recipients, clinicians with awareness of evidence did not consider the potential for the MedDiet to address these comorbidities that are known to be common post-transplant. As one non-dietetic clinician indicated: “In terms of the transplant patients, I’m not necessarily aware that Mediterranean diet has any evidence in terms of their health long term, aside from those heart disease [sic], diabetes risk factors, which they’re obviously at higher risk for.” (C06)
In addition, non-dietetic clinicians perceived that the evidence for the MedDiet, and dietary interventions more broadly, is weak and this appeared to impact their likelihood of recommending the pattern. One non-dietetic clinician, speaking about their understanding of the evidence for the MedDiet expressed: “Well …unfortunately the evidence is all observational predominantly… it's low certainty evidence” (C10)
Nutrition Advice Is Influenced by Service Delivery and Culture
Perceived Limited Capacity to Follow Up on Complex Dietary Patterns
Clinicians broadly indicated there is a lack of time to recommend the MedDiet. Delivering detailed dietary recommendations was generally not prioritised. One non-dietetic clinician expressed: “Really, we, we don't have time to cover that. It's just something that you just identify it's an issue and then have to on refer… I think you need other people to step into that space to be able to provide that information” (C09)
The perception of dietitians was that the MedDiet was complex and similarly, they find it challenging to adequately explain and recommend in a single appointment. There was an acknowledgement that structured review appointments are rare or ad hoc. There was the suggestion that priorities for nutrition care are more so based on general healthy eating principles that are more familiar to the patient and simpler to recommend with limited time. One dietitian explained: “There's so much information to run through with these patients… we kind of cover everything all in one. So potentially then introducing a new concept that doesn't directly influence their transplant at the time might not be well accepted” (D01)
Reactive Acute Model Not Preventative Model of Nutrition Care
In the transplant services, the model of nutrition care appears to be reactive and focused on acute concerns as opposed to preventative health education. Several clinicians indicated that for chronic management post-transplant, they could only refer to dietitians if a problem arose. This was linked to a perceived lack of dietitian resourcing. The priorities of some clinicians also seem to be more reactive than preventative, indicating that in long term care they manage issues as they arise.
One non-dietetic clinician expressed: “They have access to [dietary] advice when referred …if they have a problem” (C08)
One clinician described their perceived priorities in nutrition care: “[to] keep them on track with their diet, addressing anything that is changing or is becoming more severe, which is usually their diabetes.” (C01)
Consistent Nutrition Advice Is Valued but Not Facilitated
The importance of clinicians of different disciplines that see the same patients having an awareness of each other's dietary recommendations was acknowledged. Consistency in dietary advice across clinicians was valued. As one dietitian suggested: “I think it's really important that… we have the support from the consultants… it actually does make a difference having consultants who are enforcing those types of things with the patients because obviously patients respect what their doctors say.” (D05)
However, in general non-dietetic clinicians were not aware of what dietitians were recommending. One indicated: “I’m not sure. I haven't read enough of the dietitian entries recently, to be able to say if that's [the MedDiet] something that's being recommended” (C03)
This was echoed by another who, when asked if dietitians recommend the MedDiet, stated: “Oh, I, I wouldn't, I don't know.” (C04)
However, this same non-dietetic clinician did suggest there was benefit in receiving education from dietitians as to what they were recommending. As they stated: “In-services [workforce education sessions] are always good to make sure that everyone's up to date.” (C04)
Patient Education Materials Guide Practice
Most clinicians indicated they provided patients with handouts containing information relevant to their condition. Patient handouts or pamphlets were suggested by dietitians to guide consults with patients, however existing handouts were not MedDiet focused. As a consequence, counselling about the MedDiet was difficult as it required deviating from content within the accepted handout. One dietitian expressed: “I am going through this handout that kind of has the Australian Guide to Healthy Eating in it. So, it doesn't contradict that at all, but I guess it's [the MedDiet] not clearly written either in there for them to kind of follow.” (D01)
Non-dietetic clinicians also indicated they refer to handouts as a way of sharing nutrition information. Several indicated that, other than referring on to dietitians, this was the basis of their nutrition recommendations. For example, one suggested: “Nutrition related care… Um, we can give out generalized patient information, handout[s]” (C08)
It was also identified that clinicians perceived practical recommendations within handouts as a potential enabler. Some clinicians perceived that the MedDiet was largely foreign to patients and hence overwhelming to implement. There was the suggestion that more practical handouts that included components such as recipes or meal ideas may support patients in implementing the MedDiet. As a dietitian suggested, the absence of a practical MedDiet resource was a barrier to recommending this: “A lot of the… education material that we use around trying to improve dietary quality, is not very specific in terms of that practicality… it doesn't actually give you a lot of ideas on how to do it.” (D03)
This was further supported by a non-dietetic clinician who suggested that uptake of the MedDiet may be enabled if services were able to: “Provide recipes to patients, plastic models of what a Mediterranean diet looks like in the wait room with information, workshops on how to cook these meals” (C12)
Patient-Centred Care Influences Decisions on Nutrition Advice
Perceived Barriers for Patients to Implement the Mediterranean Dietary Pattern
Clinicians broadly acknowledged several perceived barriers which limit patient's ability to implement the MedDiet. This included the perception that cost would be greater than participants usual dietary intake. Another barrier identified was that traditional Australian eating patterns are very different to the MedDiet and that patients would have trouble accepting a Mediterranean-style diet. Finally, patient food literacy, skills and knowledge were considered barriers with clinicians purporting that most patients did not have the ability to buy and prepare meals in line with the MedDiet.
In general, these perceived barriers were seen by clinicians as insurmountable and this perception acts as a barrier to clinicians recommending the MedDiet. As one non-dietetic clinician suggested when asked about barriers to recommending MedDiet routinely: “Probably the same reasons, cause the, the cost, time, resources that patients will have to uptake with it” (C02)
A dietitian echoed this when asked about barriers to recommending the MedDiet: “Possibly, just what I mentioned there to being barriers for the patient. Maybe that would probably limit… how much or how… far the dietitians might go with their advice on, on the Mediterranean diet” (D02)
Dietitians and other clinicians seem to struggle to develop interventions whereby the MedDiet could be implemented while still considering feasible patient-centred care approaches to nutrition advice.
Patient Interest
Dietitians and other clinicians also identified they may only discuss the MedDiet with patients who specifically indicate an interest in or raise the MedDiet themselves and this was therefore a barrier to it being routinely recommended. One dietitian stated: “It's [MedDiet] not often something that I’ve brought up without the patient already kind of indicating that they’re interested in that style of eating.” (D01)
Discussion
This study explored the current practice for nutrition care of liver and kidney transplant recipients and identified that the MedDiet was not part of routine care, though some clinicians do recommend key principles. Several key themes and sub-themes emerged that related to the lack of use of MedDiet in practice and captured clinician-perceived barriers and enablers to the routine recommendation of the MedDiet.
Though some clinicians considered healthy eating principles aligned with MedDiet principles, recommendation of the pattern was not routine. These findings are in line with existing literature that suggests dietitians in Australia only sometimes or rarely recommend the MedDiet to post-transplant patients; even though recommendations may align with MedDiet principles, they did not label it as a Mediterranean diet. 16 It was also recognised that transplant recipients can be complex patients with multi-morbidities, thus there was often a need to address competing clinical priorities. This was identified as a barrier to recommending the MedDiet, tied with a lack of time and dietetic resources to manage nutrition care more broadly. Arguably, the MedDiet may indeed aid in the management of several competing priorities such as diabetes and weight gain. 8
Though clinicians generally agreed the MedDiet was healthy, there was variation in both knowledge and acceptance of its principles and supporting evidence. Notably, some non-dietetic clinicians accepted the benefit of MedDiet on cardiovascular risk factors and the presence of cardiovascular morbidity in transplant recipients. However, they also identified a lack of high-quality evidence for the benefit of the MedDiet specifically in transplant populations with this a barrier to implementing it into their standard practice. Indeed, the lack of randomised dietary trials specifically in transplant populations is an important consideration and there may be value in investing in further research in these specific target groups.
Despite a general understanding of what constitutes the MedDiet, dietitians had an apparent lack of confidence in translating this knowledge into specific MedDiet recommendations for transplant recipients. This suggests there is a need for further clinician education that is specific and practical and offers clinicians support in how to recommend principles of the MedDiet to these patients. Furthermore, building the clinical workforce knowledge, skills and confidence in MedDiet, may assist with individualising the MedDiet to align with patient-centred care while still maintaining the fidelity of the dietary approach.23–25
The influence of service delivery and culture on nutrition advice was identified as a major theme. Across the multidisciplinary teams, a lack of understanding of nutrition advice offered by other clinicians was noted. Consistent health messaging was valued, allowing for key messages to be reinforced by others, but it was acknowledged that there is no mechanism within the service delivery model to facilitate this. Literature has established how a lack of consistency is problematic, leading to confusion and overall acting as a barrier to patient implementation of nutrition advice. 26 Strategies to improve communication across clinical disciplines may enable more consistent dietary advice and uptake of this. As limited consultation time was suggested as a barrier by many clinicians, there is also a need to address inefficiencies in traditional service models. This may include considering more innovative strategies to providing nutrition care such as utilising technology, group education modalities and providing information online.14,27,28
The role of patient handouts within services was highlighted. Some clinicians identified that they follow the structure of these handouts in practice, using the resource to support their education. If the MedDiet were to be referred to explicitly in these handouts it may facilitate incorporation into education sessions. As existing literature has supported, practical support such as information about cooking and shopping is important in delivering dietary education to this group. 29 As has been suggested by clinicians in this study, the development and dissemination of targeted and practical patient education resources may facilitate patient adherence to the MedDiet. This may include utilisation or adaptation of existing MedDiet-focused resources, for example Oldways. 30
To our knowledge, this is the first qualitative study of kidney and liver transplant recipients examining routine nutrition care, including use of the MedDiet and identifying barriers and enablers to its implementation. The current perspectives were limited to those of clinicians in metropolitan hospitals within the targeted Australian services. The interviewer was a research dietitian with MedDiet expertise, which was known by some participants, and may have influenced participants' responses.
Conclusion
The MedDiet was not part of routine nutrition care post-kidney and liver transplant. Key barriers to recommending the MedDiet were competing clinical priorities; variation in knowledge and acceptance of the MedDiet; inconsistent multidisciplinary nutrition advice; lack of practical MedDiet education resources; limited consultation time and perceived challenges for patients. Strategies should be developed to overcome these barriers for MedDiet to be integrated into routine care.
Footnotes
Acknowledgments
We thank Dr Michelle Palmer and Dr Shelley Keating for support in conceptualising the project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Metro South Health Study Education and Research Trust Account (SERTA) Early Career Research Grant.