
Abstract
Introduction
Kidney transplant education in dialysis facilities could be optimized with internet resources, like videos, but most qualitative research predates widespread availability of online video education about kidney transplantation. To improve understanding of dialysis staff transplant education practices, as well as the potential value of video, we conducted focus groups of dialysis center staff members in Buffalo, NY.
Methods/Approach
Seventeen focus groups (97 participants: 53 nurses, 10 dialysis technicians, 6 social workers, 6 dieticians, 7 administrative personnel, 2 trainees, and 1 insurance coordinator) from 8 dialysis facilities in Buffalo, NY, were conducted, audio-recorded, transcribed, and analyzed. After thematic data analysis, a diverse patient and caregiver community advisory board was invited to comment, and their voices were integrated. Findings: Five key themes were identified that captured barriers to transplant education delivery and how online video could be a facilitator: (1) delivery of transplant education was reliant on one person, (2) other dialysis staff had time to answer transplant questions but felt uninformed, (3) patient lack of interest in existing supplementary transplant education, (4) patient disinterest in transplantation education was due to education timing, feeling overwhelmed, and transplant fear/ambivalence, and (5) video education could be flexible, low effort, and spark transplant interest. Study limitations are potential selection bias and inclusion of English-speaking participants only.
Discussion
Dialysis staff barriers of time, insufficient knowledge, and limited resources to provide education to patients and their care partners may be mitigated with online educational videos without increasing staff workload.
Introduction
High quality education provided at dialysis centers translates to increased transplant access.1,2 However, of 1694 dialysis centers recently surveyed, only 3% used what was considered an intensive education approach. 3 Barriers experienced by dialysis staff to deliver transplant education are extensively documented. Dialysis center staff are short on time,3-5 knowledge,3,5,6 and resources4,7 and have difficulty reaching several communities, including low literacy learners,8,9 non-English speakers, 3 individuals who are afraid or reluctant to learn about transplant, 4 and care partners. 4
Advances in information delivery format, such as streaming video, may make transplant education in dialysis centers easier for staff to deliver and patients to learn. Video education has been successfully deployed at dialysis centers1,2 and has demonstrated effectiveness with minority groups.10-12 A variety of educational videos developed by transplant researchers are available online.10,12-14 Individuals with end-stage kidney disease have indicated a willingness to learn transplant information from videos 15 and have rated educational videos highly.12,16-18 Video education may equip a broader range of dialysis staff with the tools to deliver education. However, dialysis center staff perspectives about using video to enhance patient education about kidney transplantation are unknown.
It is important to note the difficulty of embedding and implementing video-based patient education in dialysis centers without up-to-date information about dialysis staff education practices and barriers. It is also important to learn staff members’ perceptions of online video to enhance their provision of transplant education. The following study was designed with these concerns in mind.
Materials and Methods
Design
A descriptive study using focus group meetings was conducted at dialysis centers in one Eastern city to understand staff experiences delivering transplant education and perceived value of online educational videos in preparation for an interventional study. In parallel, we sought feedback from a community advisory board assembled by the researchers (through a community engagement studio) to corroborate content. Our Institutional Review Board approved the conduct of this study (IRB ID 00002771). Study methods followed the Consolidated Criteria for Reporting Qualitative (COREQ) research.
Data Collection
Setting
Between June 2019 and February 2020, administrators at all freestanding dialysis centers in our local area (n=19) were contacted about conducting focus groups on their premises. One dialysis organization declined participation on behalf of its facilities. The other 2 organizations allowed the proposed research. The first responding centers were chosen. The dialysis centers actively referred patients to the researchers’ transplant center. Facility administrators were informed that the proposed research was to understand transplant education delivery at dialysis centers. Declining (vs participating) centers more frequently offered home hemodialysis (40% vs. 25%) and had a census of > 25 patients (80% vs 75%), respectively.
Sample
Two sessions were held in each dialysis facility's private conference room on the same day, back-to-back, at lunch time to maximize opportunities for staff participation. Lunch was provided by the research team. Any English-speaking dialysis staff members 18 years or older were eligible to participate for range of perspective, which amounted to 9-13 staff per center. Only researchers and participants were present. Later, narrative sections were shared by one investigator with the community advisory board of 3 kidney failure patients and 2 care partners (2 Black, 2 White, 1 Hispanic; all female); their voices were integrated into the findings. Board members provided written informed consent, and their characteristics were self-reported
Information Collection
All participants provided written consent and completed a demographic questionnaire. The focus groups were conducted by 2 White female researchers: an experienced doctoral-level social scientist (MR) and graduate-level research coordinator (RS), using a guide designed by a transplant surgeon, an epidemiologist, and a researcher with qualitative experience. The guide was informed from the literature and included open-ended questions about (a) dialysis staff delivery/barriers to delivery of transplant education, (b) dialysis patients’ perceived knowledge of and reactions to kidney transplantation, and (c) anticipated benefits of educating patients with web-based videos. The guide also included two structured-response questions posed to social workers to assess patients’ frequency of using a device, like a smart phone or a tablet while receiving dialysis treatment and the center's internet quality.
Focus groups were audio recorded and lasted approximately 45 minutes. Field notes were made after each focus group. Participants were mailed a US $25 check to compensate for their time. Recordings were professionally transcribed verbatim within 1 week and were not checked by participants to minimize participant burden. Focus groups were repeated until reaching saturation.
Data Analysis
Data were analyzed using the framework method of thematic analysis. 19 Transcripts were independently reviewed by two investigators, a social scientist and a transplant surgeon, using Excel. As new data became available, initial codes were compared, revised, and thematically grouped by study aims. Weekly meetings allowed for resolving coding discrepancies and discussing reflexivity. We emphasized depth and exploration, rather than breadth or quantification of responses.
Findings
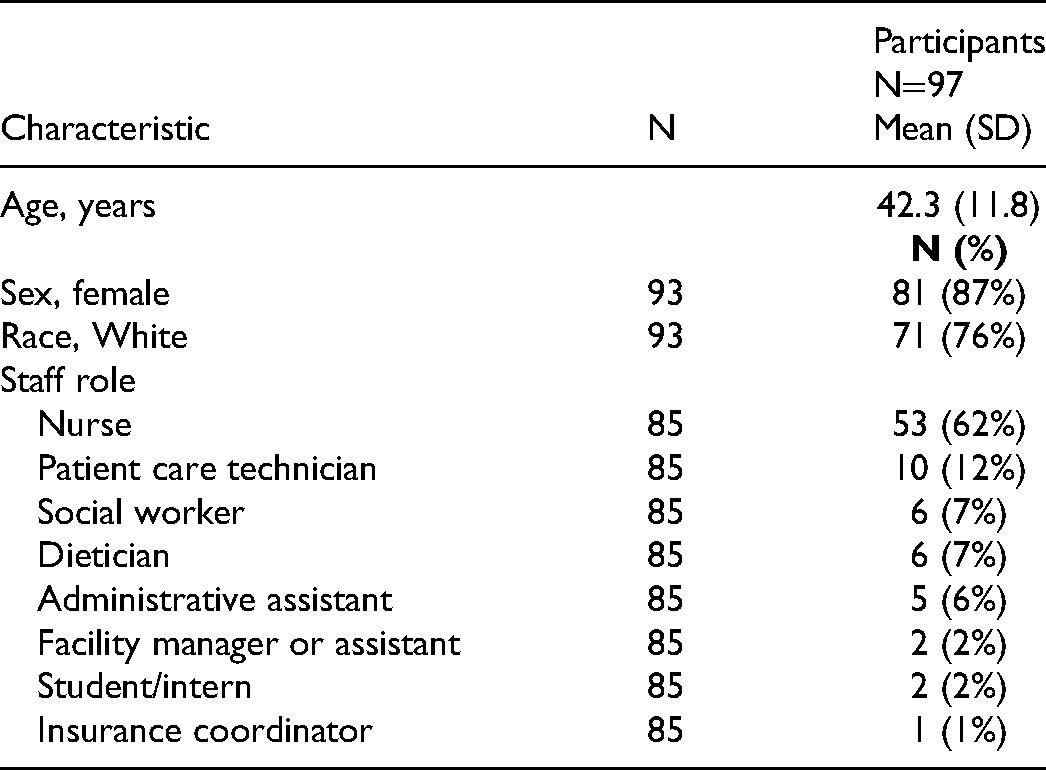
Seventeen focus groups were conducted at 8 dialysis centers with 97 dialysis staff members and characteristics are shown in Table 1. Dialysis centers had a mean of 45 patients served. Dialysis staff averaged 42 years of age and were predominantly nurses (62%), female (86%), and White (75%). Patients were predominantly non-Hispanic White and Black. Wi-Fi quality at the centers and patient technology use were rated highly. The characteristics of the 8 dialysis centers is shown in Table 2. Five themes emerged in the examination of transcripts and are described below along with representative quotations from both dialysis staff and community advisory board members.
Baseline Characteristics of Focus Group Participants.
Dialysis Center Characteristics.
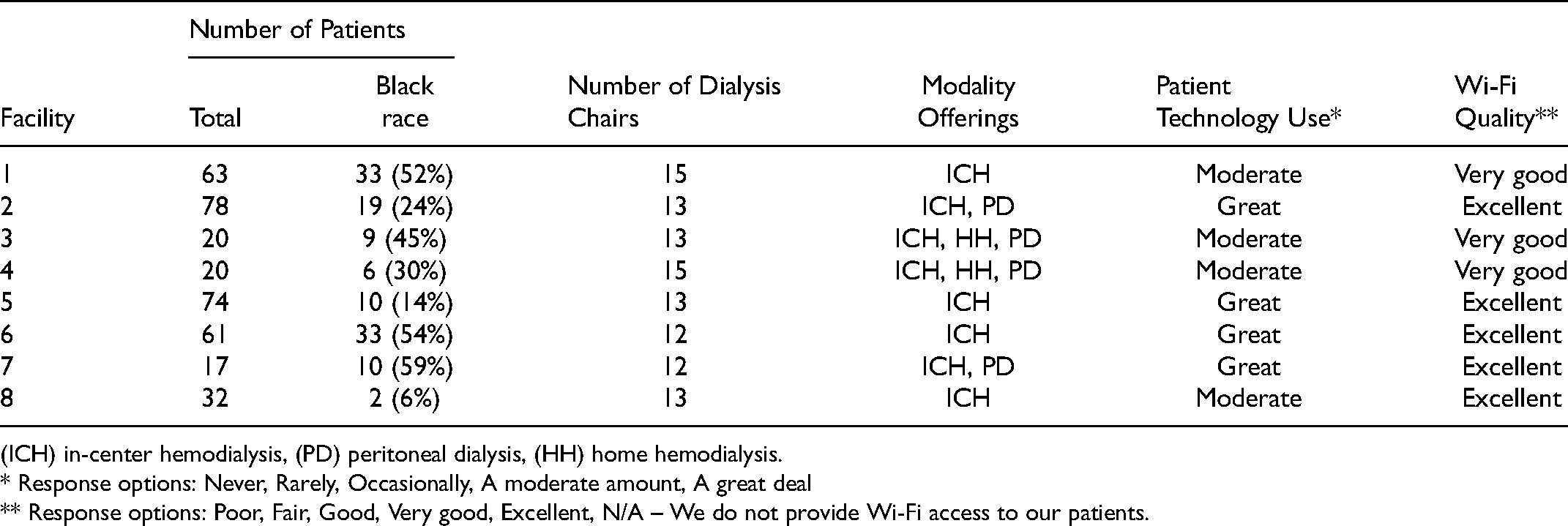
(ICH) in-center hemodialysis, (PD) peritoneal dialysis, (HH) home hemodialysis.
* Response options: Never, Rarely, Occasionally, A moderate amount, A great deal
** Response options: Poor, Fair, Good, Very good, Excellent, N/A – We do not provide Wi-Fi access to our patients.
Delivery of transplant education was reliant on one person.
Dialysis centers relied on a designated educator, usually a social worker, for transplant education. Social worker availability to deliver education was limited because of part-time scheduling, multiple facility assignments, the requirement to cover numerous topics in addition to transplantation, and intensive patient and family member educational needs, such as individuals who were unable to read or understand English. Inadequate time and reliance on one person to provide quality education was encapsulated by participants from 4 centers: As much as we all wish we could just sit there and like go over things, we just don't have the time… It's hard to stay focused when someone is asking you seven different things and a whole pod of patients coming around. By the time you’ve done everything that you needed to do, that person is either sleeping, gone, or you forget.
It's mostly the job of the social worker.
He [tech] goes let me get the social worker for you. The social worker will actually sit down with them.
They don't want to hear the social worker will be here next week.
Advisory board members perceived dialysis social workers to be overwhelmed with other responsibilities, leaving little time to deliver transplant information: They cover so many different aspects of social work but very little about transplantation. I have not really heard anything in my time at dialysis.
Other dialysis staff had time to answer transplant questions but felt uninformed.
Nurses and technicians were in patient rooms more often than social workers and were regularly approached by patients with questions about transplantation. These staff felt unprepared to answer patients’ questions, such as who was eligible for a transplant, the process for a referral, tests required for transplant evaluation, why patients could not be listed at multiple transplant centers in New York State, and transplant recovery and follow up. Inability to answer patients’ questions made staff feel incompetent. They were frustrated by having to defer to the social worker and voiced concern that waiting for information may deter patients from seeking referral to a transplant center. A majority reported receiving no formal transplant training and had a desire for more education to be able to answer patients’ transplant questions. Participants from different centers shared their experiences fielding patient questions about transplantation: They ask a lot of questions that I really seriously don't know.
It's hard to say to your patients, wait until the [social worker is in]. It's this person's job. I mean they’re basic questions. We should know the answer to that. It makes us look incompetent.
I had one guy ask me the other day about the after care. Like, I don't know. They’ll explain all that to you when you go there, but that's not really helpful to make that transition.
An advisory board member was reluctant to discuss transplantation with her dialysis nurse due to perceived lack of knowledge:
When the nurse didn't know, I didn't want to ask. That was a huge deterrent.
Patient lack of interest in existing supplementary transplant education.
Dialysis staff provided verbal transplant education one-on-one, supplemented with print materials, group classes, and DVDs, but patients lacked interest in the supplementary education provided. After distributing print materials, staff observed patients not reading or sharing it with others and indicated that large packets and booklets gave too much information at once. Some staff held group classes, but sessions were not well attended by patients due to fatigue after treatment. Others had shown transplant DVDs in the lobby, but the videos did not hold patients’ attention. There were differences in access to educational materials among facilities; however, all facilities lacked educational materials for patients who were unable to read or did not speak English. Limitations of current educational materials are illustrated in these staff comments: A pamphlet is too much information, they are not going to go through it. Yes, you can always have that, but have something a little more simple, like short and sweet, so they can get their foot through the door.
After dialysis, the patients are feeling low because there's so much energy from your body that they go home and they go to sleep for hours for the rest of the evening and they don't have energy or they don't feel like doing it [classes].
We tried a [DVD] before. Remember the one time we tried, and they’re like okay not for this. We want our Price is Right. They were getting all fussy about it.
Some people can't read, but they won't tell you that.
An advisory board member voiced the following about supplemental transplant education:
It can't be too lengthy and it needs to be easy to understand. You gotta engage people.
Patient disinterest in transplantation discussions due to education timing, feeling overwhelmed, and transplant fear/ambivalence.
Staff observed patient disinterest in transplant education at different points in time. Newly dialyzed patients were not open to discussing transplant, overwhelmed with receiving a diagnosis of kidney disease and embarking on dialysis. Instead, staff reported the optimal time was the third or fourth treatment, when patients were better at managing their dialysis and open to further education. If education was delayed too long, many patients became unreceptive to education, which was attributed to transplant fear or ambivalence.
Feeling fearful or ambivalent about transplantation deterred interest in receiving education about transplantation. Some patients were against transplant after hearing negative stories from peers. Many were fearful of undergoing surgery, having negative outcomes, and the financial impact of transplant. Others worried about the lengthy transplant evaluation process and not knowing how long they would wait for a kidney. When patients were not open to conversations about transplantation, staff voiced the need to use a conversational approach that subtly introduced the topic. Dialysis provider comments about the challenges in providing transplant education are encapsulated in these quotes: They tend not to ask questions after receiving the diagnosis of ESRD [sic] and losing the function of their kidneys and what all that means. They have to try to get that part down first before they even think about a transplant.
They are scared of the unknown. Is it gonna reject as soon as I get it?
He was like not just like tears, he was sobbing. He was so upset. He was scared about his job. He was scared about his family. He was scared about what's he going to do. You know most of it was his financial concerns.
We try to counsel like on transplant, but they, they get very reluctant of all the tests beforehand and cause like it's such a long list. They get daunted by that huge list of things.
Sometimes I’ll mention transplant and they will be like, meh. I think it's because they become content with where they are.
A member of the advisory board discussed her initial response to transplant: In the beginning, they were talking to me and trying to get me to know what was going on but I was in such a state that I wasn't hearing anything.
Online video education could be flexible, low effort, and spark transplant interest.
Staff imagined that online educational videos could be seen by patients on their own devices or by using tablets available at the dialysis facility. Staff anticipated that video education would be easy for any staff member to deliver or initiated by the patients themselves, including at home, thereby reducing staff burden. Staff suggested that a short video about transplant could be helpful to initiate conversations with reluctant patients to pique their curiosity about kidney transplant and interest in learning more. Staff also felt videos could be a resource to boost their own knowledge about transplantation. Staff perceptions of online video education are articulated in these comments: Anyone can refer them to the web site and just say there's a video uploaded where you can watch. That would be real easy, cause most of them have their phones.
They could watch it and [we would] not even have to make a big production about it.
I think a video at first might be nice. A video-- spark the interest and then someone come in and talk to them.
I think it would be good for me, I mean, I would love to watch the videos. There's a lot I can learn.
Advisory board members believed that video education would increase the capacity of dialysis staff to answer questions: I think they need to see it. It would give them the explanation of kidney transplantation and how to suggest this info to patients.
Discussion
This descriptive study of dialysis staff perspectives considered in tandem with experiences from a small group of patients and care partners provides several useful insights about the challenges of delivering kidney transplant education at dialysis centers and the potential facilitating aspects of online video education. Although many prior studies have reported dialysis staff perceptions about education delivery obtained through surveys,3,5,6,8,20 few researchers have conducted interviews to more deeply understand dialysis staff practices and barriers to delivering transplant education, 4 and none have explored staff perceptions of the potential value of online video as a learning channel.
The first theme was that delivery of transplant education by dialysis staff was reliant on one person, typically a social worker, who emphasized time and clinical duty pressures as barriers to providing transplant education. They also cited low patient literacy and English language fluency as patient barriers to receiving education. Barriers of time and patient fluency are consistent with previous research.3,4 However, our study highlights that transplant education by dialysis center staff (excluding physicians/nephrologists) may predominantly rely on the social worker, which is in contrast to some other research that reports transplant education being conducted by multiple staff members, most commonly nurses and social workers. 6 Given the limited resources available at some dialysis centers, 4 innovative methods may be needed to support designated educators to carry out transplant education using less supervision. Proposed solutions have included peer educators4,8,21 or dedicated liaisons between the dialysis and transplant center.4,21 Implementation of in-person strategies may be limited by logistic barriers, including those currently brought on by the COVID-19 pandemic, which increases the importance of strategies that support remote access to patients for peer navigators 22 and transplant educators.3,11
The second theme was that dialysis staff who are not the designated educators have the time and desire to provide transplant information but lack sufficient knowledge to do so. Previous studies have reported gaps in transplant-related knowledge among dialysis providers as a group3,4,6 and among dialysis administrators, 6 but have not described the atmosphere we found of missed opportunities for education from a wide range of dialysis staff with frequent patient contact who are often queried by patients but unable to provide transplant education. Improved educational outreach by transplant centers to dialysis centers was recommended by a recent consensus statement from the American Society of Transplantation. 21 Training and materials could also be provided by national and local community organization, including online approaches. 21 To reach the goal of 80% new patients with home dialysis or transplant within the 2019 Advancing American Kidney Health initiative, transformative changes in transplant education practices within dialysis will be important. 23
The third theme was that existing supplementary education about transplantation in dialysis centers has limited impact. Specifically, available methods of information provision were overwhelming (e.g. booklets, classes) or not engaging (e.g. DVDs), and problematic for reaching the broader transplant population (e.g. non-readers) and their family members. Other researchers have also reported that dialysis staff lack access to optimal education resources,4,6 sometimes due to limited facility finances for education. 4 Online resources have the potential to be widely accessible; however, the level of readability of available online transplant-specific information is at a college level compared with the recommended sixth-or seventh-grade level. 24 The need for culturally tailored materials for use with Black and Hispanic populations has also been addressed by researchers with culturally-sensitive online education,11,25 but only 3.7% of transplant program websites in 2018 had any evidence of a culturally targeted initiative. 26 Efforts to improve provision of transplant-related information, particularly using online methods, are likely to have universal benefits.
The fourth theme was patient disinterest in transplantation education due to timing of education, feeling overwhelmed, and transplant fear/ambivalence. We are the first to report that the optimal timing of transplant education may be after the dialysis initiation period, but within a few weeks. A short delay still complies with Centers for Medicare and Medicaid Services mandates that dialysis centers inform their patients of the option of transplant within the first 45 days of dialysis initiation (CMS573). Fear and ambivalence experienced by dialysis patients about transplantation have been detailed elsewhere. 4 Our findings highlight that fearful and reluctant learners may not respond to traditional education. These individuals, some of whom have prior knowledge that attenuates learning interest, may require different approaches such as persuasion for learning, which considers the emotional impact of communication, visual design, length of message, relevance of content, expanded repertoire, and continuous messaging. 27
The fifth theme was the opportunity of online video education to be flexible and to require low effort and spark transplant interest. A picture of short, accessible online video education emerged whereby videos could be delivered by any staff member or accessed by learners themselves, without additional workload burden. The self-sustaining nature of interventions that accommodate staff capacity and workloads has been recommended previously, 8 including use of themed videos to support providers with less transplant expertise or comfort with education. 13 We shed light on the importance of a short introductory video to enable dialysis staff to engage reluctant learners. Previous research has also suggested the utility of video for those less ready to pursue kidney transplantation. 13 Despite positive comments on the value of online video, dialysis staff in our study had not utilized available online videos and had only reported historic use of DVDs. In other studies, educational video showing at dialysis centers has also been low, between 11% and 20%.3-5 Further research is needed to determine if patients will view videos once available and to inform strategies to successfully deliver video education.
The main limitations of this research relate to its transferability to other practice settings and potential biases. Participants were from dialysis centers staffed by 2 dialysis organizations in one Eastern city and may not represent dialysis staff practices and perceptions at other local centers, national dialysis centers, or centers operated by different dialysis organizations. Physicians were intentionally not involved to facilitate staff comfort in speaking freely. Nevertheless, some interviewees might have been unwilling to raise challenges in front of their colleagues due to the group interview format. Focus groups included a mixture of staff roles within a limited interview duration, potentially limiting clarity and depth of perspective. The study took place in a majority-minority city, with the predominant minority being Black. Therefore, topics relating to cultural barriers may not have been elicited. We concluded the study after no new themes emerged from the last 3 focus groups, but other perspectives may exist. The perspectives of patients were drawn from dialysis staff, rather than the patients themselves. The inclusion of advisory board members helped to substantiate providers’ impressions of patient experiences; however, future work with patients will be needed to fully include patient voice.
Conclusion
Our participants’ perspectives suggest that dialysis facility staff have little time for transplant education, low knowledge about transplantation, and insufficient educational strategies. Innovative methods are needed to support dialysis staff to deliver transplant education using less supervision. Providing transplant-specific information within videos might help to ameliorate current dialysis center staff challenges to deliver transplant education both to patients and their social networks. Our findings could be used to inform the design of a video-based education intervention to enhance transplant education at dialysis centers and suggest the need for videos that are short, engaging and mobile friendly and that provide progressive information.
Footnotes
Acknowledgements
We thank Rachel Seibert MBA, MPH for data collection, and the members of our community advisory board for their time and expertise: Barbara Breckenridge AAS, Sherry Brinser-Day BA, Anna McCarthy LCAT, ATR-BC, and Cheryl Thomas.
Conflict of Interest
The authors declare no conflicts of interest.
Funding Acknowledgements
This work was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under award number UL1TR001412.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Authorship
LK led the conceptualization, data curation, formal analysis, writing, and reviewing of the manuscript. MR contributed to the data curation, formal analysis, writing, and reviewing of the manuscript. MK, BD, and TF contributed to reviewing and editing the manuscript.