
Abstract
Introduction
Posttransplant diabetes mellitus (PTDM) can increase morbidity and mortality in liver transplant recipients. Although hepatitis C seropositivity is a known risk factor for PTDM, the impact of viremia versus no viremia at time of transplant is unknown.
Project Aims
This program evaluation sought to compare PTDM in hepatitis C seropositive patients with and without viremia at the time of liver transplant.
Design
This single-center retrospective review included adult hepatitis C seropositive liver transplant recipients transplanted between January 1, 2010 to September 5, 2017 without pretransplant diabetes. Primary outcome was PTDM within 1 year. Secondary outcomes included evaluating 1-year posttransplant death-censored graft loss, mortality, and metabolic outcomes.
Results
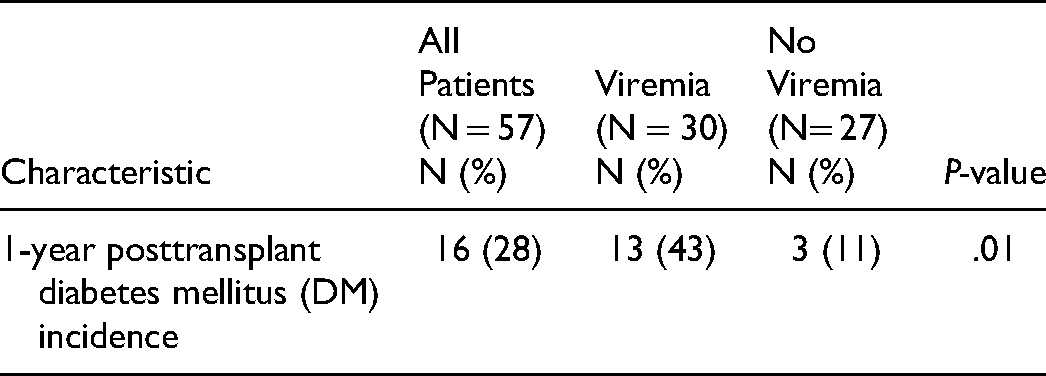
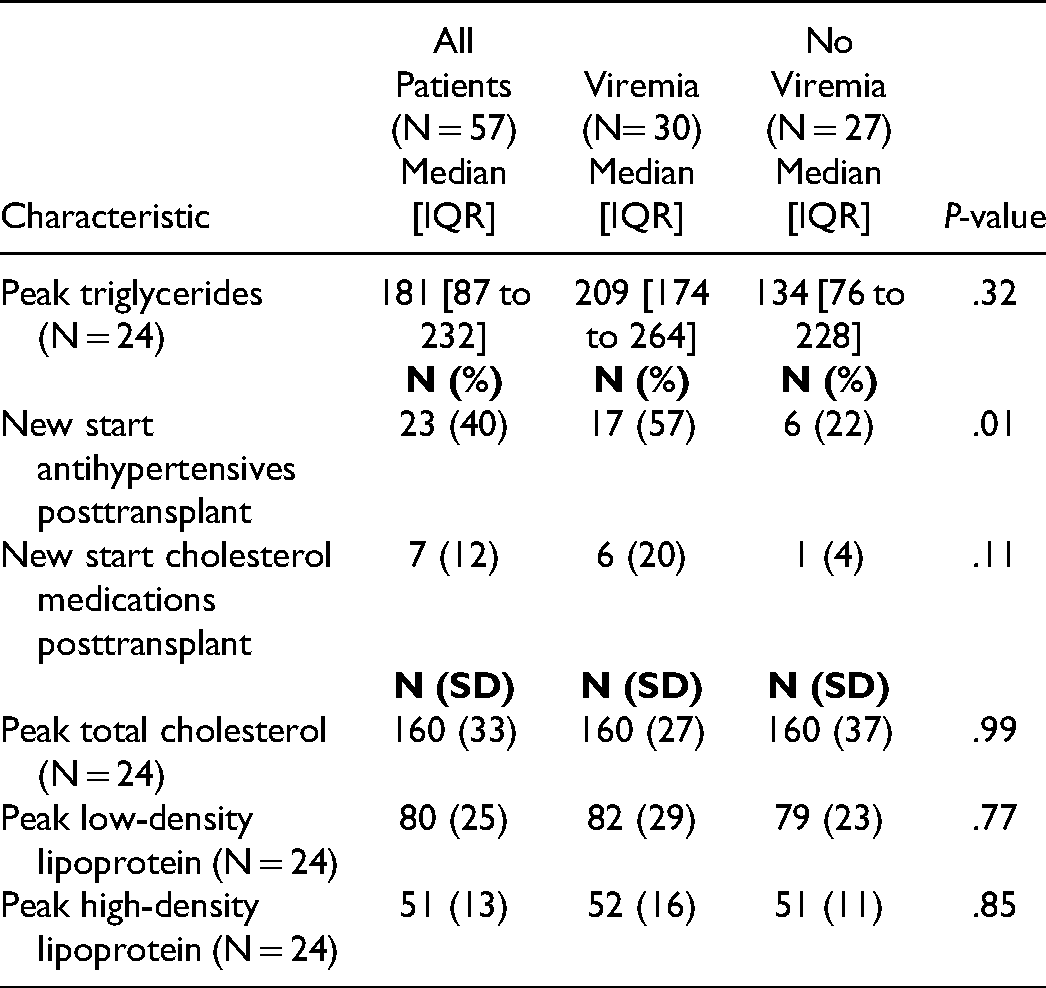
Fifty-seven liver transplant recipients with hepatitis C were included, of which 53% (n = 30) were viremic at transplant. Baseline characteristics were similar between groups. Significantly more patients with pretransplant viremia developed PTDM by 1-year posttransplant compared to the patients without viremia (43% vs 11%, P = 0.01). There were no differences between groups outside of more patients with viremia requiring antihypertensives by 1-year posttransplant compared to patients without viremia (57% vs 22%, P = 0.01).
Conclusion
Liver transplant patients with hepatitis C viremia at transplant were more likely to develop PTDM at 1 year compared to those without pretransplant viremia. This is an added consideration when deciding the timing of direct-acting antiviral (DAA) utilization in the context of liver transplant for hepatitis C seropositive patients.
Keywords
Introduction/Background
Posttransplant diabetes mellitus (PTDM) is recognized as a complication following solid organ transplant, and is a significant source of morbidity and mortality. 1 Incidence of PTDM in liver transplant recipients has been reported to be 12% to 45% within 1-year posttransplant, and as 40% to 50% at both 3- and 5-years posttransplant.2,3 Sequelae include renal failure, infection, and graft loss.2,3 Major cardiovascular events can also occur, which is notable as cardiovascular disease is the leading cause of non-graft-related death in liver transplant recipients. 4 Liver transplant recipients seropositive for hepatitis C virus (HCV) have been identified as having an increased risk of developing PTDM compared to recipients without the virus.1,5 The mechanism for this association is unknown, but is theorized to be due to a virus-driven increase in insulin resistance. 6
The advent of the direct-acting antiviral (DAA) agents has drastically improved HCV cure rates from 30% to 40% during the interferon–ribavirin era to greater than 90%. 7 One study in liver transplant recipients discovered sustained virologic response (SVR) was associated with a decreased PTDM risk. 8 A small proportion of patients in their study achieved SVR pretransplant, which was found to decrease PTDM risk further. Limited data exists with a focus on assessing the effect of HCV clearance pretransplant on the subsequent development of PTDM in liver transplant recipients.
Specific Aims
The primary purpose of evaluating our program was to assess the effect of viremia in HCV-seropositive patients at the time of liver transplant on PTDM incidence 1-year posttransplant. Secondary purposes included evaluating 1-year posttransplant death-censored graft loss, mortality, and metabolic outcomes.
Design/Methods
Design
This was a retrospective, single-center, cohort evaluation. It was approved by the center‘s Institutional Review Board.
Setting
The program evaluation took place within an academic medical center.
Population
The OPTN/SRTR 2019 Annual Data Report: Liver showed the majority of liver transplant recipients in the United States that year were middle-aged (48% 50-64 years old) White (70.7%) males (63.7%). 9 Hepatitis C was reported as a common etiology for transplant although rates have decreased since the introduction of DAAs. As noted from the program evaluation center‘s 2020 volume, liver transplants were predominantly performed on middle-aged (41% between 50 and 64 years old) Hispanic/Latino (53%) and White (40%) males (54%).
Sampling
Adult HCV-seropositive patients who received a liver transplant at the transplant center between January 1, 2010 and September 5, 2017 were reviewed for inclusion in the evaluation. Patients were excluded if they had a pretransplant diabetes diagnosis, underwent a multi-organ transplant, were lost to follow-up, or had documentation of antihyperglycemic medication use pretransplant, regardless of indication.
Data Collection
Patients were identified through the center‘s internal transplant database. Data collected included recipient demographics, model for end-stage liver disease (MELD) score, body mass index (BMI), pretransplant comorbid conditions, DAA use pretransplant, HCV genotype, SVR, graft steatosis, diabetes mellitus (DM) family history, immunosuppression regimens, steroid or anti-lymphocyte antibodies received, pertinent diabetic and liver function laboratory results, and antihyperglycemic, antihypertensive or antihyperlipidemic medication use posttransplant. Biological MELD and listed MELD-Na scores were collected. Biological MELD was defined as calculated MELD-Na score excluding exception points. MELD scores were converted to MELD-Na scores for patients transplanted before 2016.
Hepatitis C seropositive patients without viremia at the time of transplant (no viremia group) were compared to those with quantifiable viremia (viremia group). All non-viremic patients were included, and a comparable number of viremic patients were selected for analysis via computer-generated randomization. The primary outcome was PTDM within 1 year. To meet PTDM criteria, patients had to be on a steroid-equivalent dose of prednisone ≤ 5 mg daily and at least 45 days posttransplant. PTDM was defined as any one of the following occurring after 45 days posttransplant: two fasting blood glucose (FBG) ≥ 126 mg/dL, random plasma glucose (RPG) ≥ 200 mg/dL, two-hour plasma glucose ≥ 200 mg/dL after 75 gm oral glucose tolerance test, hemoglobin A1c ≥ 6.5%, new diabetes diagnosis from an outside provider, or new start of antihyperglycemic medications.
Death-censored graft loss and mortality at 1-year posttransplant were evaluated. The use of DAAs, antihypertensives, or antihyperlipidemic treatment within 1-year posttransplant was also collected.
Data Analysis
JMP® Pro, version 14.0 (SAS Institute Inc.) was used for statistical analyses. Baseline characteristics were compared between the viremia group and the no viremia group. Incidence of PTDM was calculated by the number of patients in each group who met the criteria for PTDM by 1-year posttransplant divided by the total number of patients in each group. Graft loss and mortality were each calculated by the number of patients who experienced that outcome in each group divided by the total number of patients in each group. Metabolic outcomes were evaluated by the number of patients who were started on an antihypertensive or antihyperlipidemic divided by the total number of patients in each group.
All continuous variables were analyzed using a goodness of fit test to assess normality. Chi-squared or Fisher‘s exact test was performed for categorical data and t-test or Wilcoxon rank-sum test were performed for continuous data where appropriate.
Procedure
Data were extracted manually from electronic medical records and documented in Microsoft Excel using numerical coding.
Results
Baseline characteristics were relatively balanced between groups (Table 1). Patients were mostly middle-aged, Hispanic, or Caucasian males with a median biological MELD-Na score of 16 and a BMI of 30 or greater. Significantly more patients in the no viremia group had hypertension at transplant (47% vs 13%, respectively; P = .03) and used DAAs pretransplant (59% vs 6.7%, respectively; P = .001). Most patients were HCV genotype 1. Documentation of SVR was identified in 15% of the no viremia patients at the time of transplant. No differences were identified between groups for DM family history. Considering donor characteristics, a majority were deceased. Steatosis was present on zero-hour biopsy in 16% of grafts with no differences between groups.
Baseline Characteristics of Recipients With and Without Pretransplant Hepatitis C Viremia.
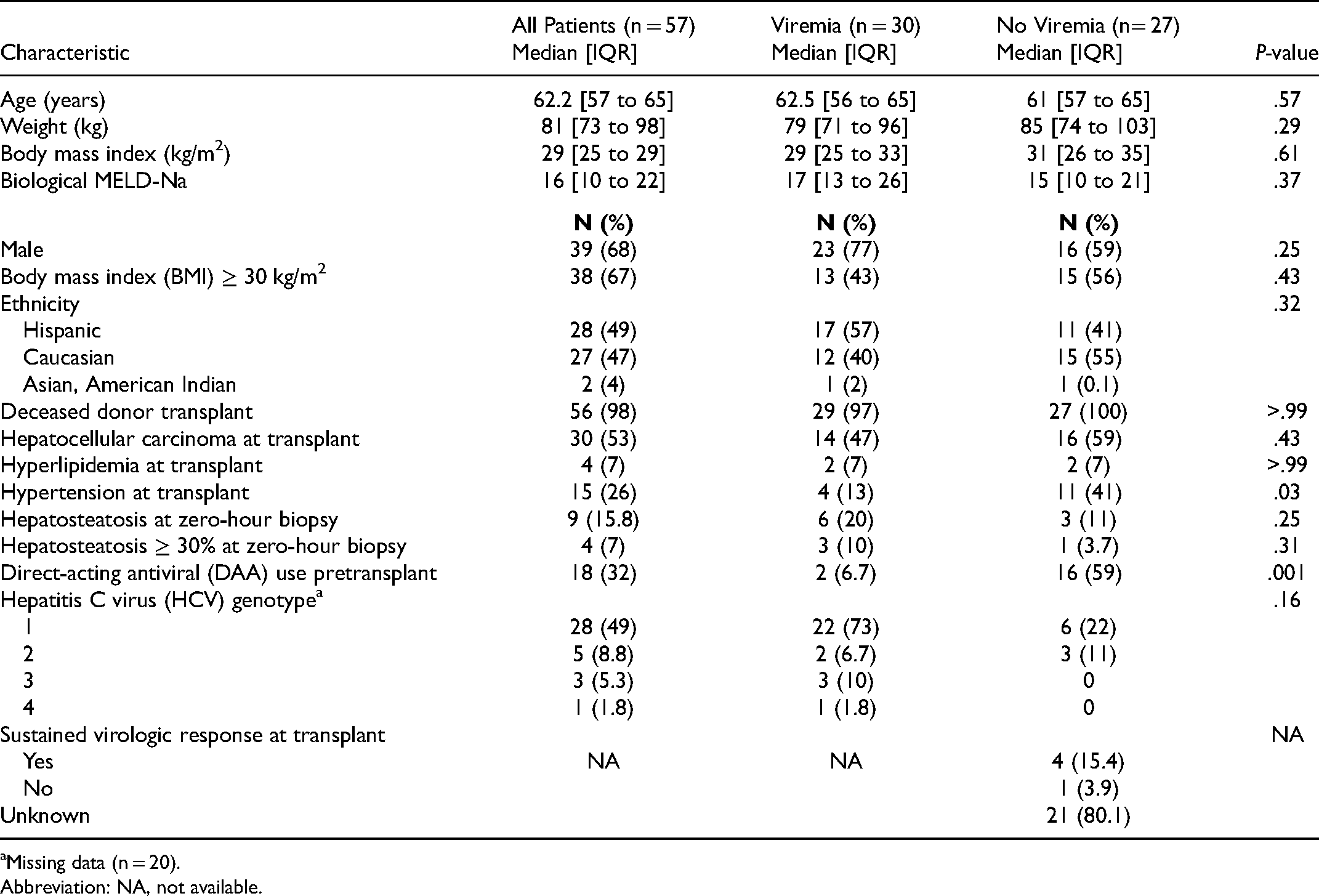
Missing data (n = 20).
Abbreviation: NA, not available.
No patients received antibody-depleting induction. Most patients used tacrolimus for maintenance immunosuppression, with the rest receiving cyclosporine (5%) or sirolimus (2%). All patients received mycophenolate mofetil and steroid taper as part of their maintenance immunosuppressive regimen. Mycophenolate mofetil and prednisone were tapered off and discontinued between 3 and 6 months, and 1 year, respectively, posttransplant. The tacrolimus goal was typically 8 to 10 ng/mL for the first month, then 6 to 8 ng/mL for the first year, followed by 4 to 6 ng/mL, and adjusted for patient-specific factors such as infection or rejection occurrence. Treatment for rejection was infrequent and similar between groups. See Supplementary Table 1 for more information on immunosuppression regimens.
Incidence of Posttransplant Diabetes Mellitus (PTDM) for Recipients With and Without Pretransplant Hepatitis C Viremia.
Metabolic Outcomes of Recipients With and Without Pretransplant Hepatitis C Viremia.
Discussion
Incidence of PTDM within 1-year posttransplant ranges from 40% to 64% in HCV-seropositive patients compared to 20% to 30% in HCV-negative patients. 10 One study evaluating 24,956 liver transplant recipients demonstrated a higher PTDM risk at 1-year posttransplant in HCV-seropositive recipients compared to HCV-seronegative recipients (HR 1.17 [1.09-1.27], P = .001). 5 Hepatitis C seropositivity has been repeatedly identified as an independent risk factor for PTDM.2–4 In the setting of DAAs for the treatment of HCV, however, viremia at the time of transplant‘s effect on PTDM development has not been thoroughly investigated. A single-center study by Roccaro et al. found that SVR was associated with decreased PTDM incidence in liver transplant recipients (HR 0.40, P = .048). 8 They noted that 12% of their study population achieved SVR pretransplant, and this was associated with a reduced risk of PTDM (HR 0.30, P = .046).
This program evaluation primarily investigated the effect of pretransplant viremia on PTDM incidence in HCV-seropositive liver transplant recipients compared to those who were HCV-seropositive but without viremia. It was found that the viremia group had a higher incidence of 1-year PTDM compared to the no viremia group. Interestingly, most of the viremia group were treated posttransplant with DAAs, yet still had a higher incidence of 1-year PTDM, suggesting that the timing of pretransplant viremia may be important. No differences were identified between groups for 1-year graft loss or mortality. However, a difference was not expected with this study design and size. Most patients in the no viremia group did not have a documented SVR. Most of these patients were followed at an outside institution for HCV treatment, thus it is possible SVR was recorded elsewhere.
To investigate whether patients in the viremia group had other metabolic sequelae outside of PTDM we evaluated lipid panels, and whether antihypertensives or antihyperlipidemics were newly initiated posttransplant. There were no differences between groups concerning lipid panels. More patients in the viremia group were started on antihyperlipidemics and antihypertensives, with the difference being statistically significant for antihypertensives. The clinical significance of this is unknown as laboratory and vitals data needed for hypertension confirmation were unavailable. No recent studies have identified metabolic sequelae as risk factors for PTDM, besides one study identifying weight gain as a risk factor.2–4 Although we are unable to draw conclusions regarding other metabolic diseases, the effect of HCV on overall metabolic disease may require further exploration.
There were several limitations to this program evaluation. Data were collected via retrospective chart review, which inherently has limitations. This evaluation was conducted within a single-center and in a small population, thus external validity is limited. The population was similar to the OPTN/SRTR 2019 Annual Data Report on liver transplant patients, which does support the generalizability of the findings to other centers. 9 Lastly, this evaluation was conducted with a 1-year follow-up period. It is unknown whether outcomes would persist during a longer period.
Conclusions
The results of this program evaluation bring to light the risk for PTDM when HCV-positive patients are transplanted with viremia. Because of the impact that PTDM has on the morbidity and mortality of liver transplant recipients, the identified risk difference in PTDM is a variable to be considered when determining the optimal timing of HCV treatment in a cirrhotic patient population.
Supplemental Material
sj-docx-1-pit-10.1177_15269248211064879 - Supplemental material for Effect of Hepatitis C Viremia on Posttransplant Diabetes Mellitus in Liver Transplant Recipients
Supplemental material, sj-docx-1-pit-10.1177_15269248211064879 for Effect of Hepatitis C Viremia on Posttransplant Diabetes Mellitus in Liver Transplant Recipients by Kelsey Klein, Joelle Nelson, Christina Long, Kermit Speeg, Naim Alkhouri and Reed Hall in Progress in Transplantation
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.