
Abstract
Introduction
Acknowledging the evolved landscape in thoracic transplantation, professional employment becomes an important outcome measure to quantify the success of this costly procedure.
Objective
We aimed to assess rates of and characterize factors associated with professional employment in patients following thoracic transplantation, and create an evidence-base on the relationship between professional employment and relevant outcome parameters.
Methods
We systematically searched Medline, Cinahl, and GoogleScholar to identify studies published between 1998 and 2021 reporting on professional employment following heart and lung transplantation.
Results
Twenty-two studies from 11 countries with varying sample sizes (N = 27; 10 066) were included. Employment rates ranged from 19.7% to 69.4% for heart, and from 7.4% to 50.8% for lung transplant recipients. Most frequently reported positively associated factors with employment after transplant were younger age, higher education, and history of pretransplant employment. Longer duration of unemployment prior to transplantation and Medicaid coverage were the most frequently reported negatively associated factors. Relationships between professional employment and clinical outcomes included lower rates of acute and chronic rejection, less infection episodes, and better quality of life among working patients; one study reported a lower 5-year-mortality rate. Reasons not to work were “physical or mental health-related,” “employment-related,” “financial reasons,” and “lifestyle choices.”
Discussion
Substantial proportions of patients following thoracic transplantation are not professionally employed, potentially diminishing the success of transplantation on individual and societal levels. Considering adverse clinical outcomes in employed transplant recipients were low, more efforts are needed to identify modifiable factors for employment in these populations.
Introduction
Thoracic transplantation represents an established treatment strategy for patients with end-stage heart or lung-failure. 1 The primary goal for thoracic transplantation seeks to increase life expectancy and quality of life (QoL) for these patients. With marked improvements in surgical, medical, and pharmaceutical treatment strategies, more studies have emphasized secondary outcomes to measure the success of these costly procedures.2,3 This includes return to a professional work-life following transplantation 4 —either into the same or another job. Failure to return to a work-life may form a threat to physical and psychosocial life on the individual level, and may impair QoL perceptions. 5
In the current literature, neither a conceptual definition, nor a consensual terminology for professional employment exists. Thus, for the purposes of this study, professional employment was conceptualized as a meaningful and paid engagement with the purpose of actively partaking in societal life, recognizing educational, functional, and mental capabilities by an individual. This entangles paid employment (full- and part-time), and educational pathways towards paid employment such as vocational traineeship or studying. Professional employment eventually leads to retirement, usually being permanent, with retirement age differing by country and country-related healthcare regulations. Retirement can be age-related, disease-related, or due to other reasons. 6
Professional employment represents a key element of an active social adult life. A professional life can be endangered or even disrupted by serious and end-stage heart or lung diseases and subsequent transplantation. 4 Since transplantation incurs high societal costs, it becomes of utmost importance to target secondary outcomes by understanding and supporting return to work. The societal perspective may consider economic aspects within a climate of fiscal restraints, from an individual's perspective; however, professional employment may improve recipients’ QoL after heart transplantation,6–8 and lung transplantation.6,8–10 This becomes particularly important as neither negative effects nor rejection or infection rates for those recipients, which had deliberately chosen their professional reintegration, have been reported. 10
The most recent review aiming to systematically appraise professional employment after heart transplantation dates back to 1997. 11 A literature review to describe social adaptation for heart, lung, and heart-lung recipients has been performed by Paris and White-Williams in 2005. 12 However, the majority of literature filtered in this review captured transplant outcomes in the early eras of thoracic transplantation. For the lung populations, no systematic critical appraisal of the current literature has been identified.
Objective
Acknowledging the evolved landscape in thoracic transplantation our review aimed to (i) assess average rates of professional employment in heart and lung recipients, (ii) characterize factors associated with professional employment, (iii) create an evidence-base on the relationship between professional employment and relevant outcome parameters including rejection, infection, QoL, and survival, and (iv) identify reasons for not being professionally employed following transplantation.
Methods
We conducted a systematized review of the literature to provide an overview. As reported by Grand and Booth 13 a systematized review as an “attempt to include one or more elements of the systematic review process while stopping short of claiming that the resultant output is a systematic review."(p. 102) According to that definition we used a systematic approach to the literature search, data extraction, and data analysis, but without a formalized assessment of the quality of included studies. Data are reported based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement extension for scoping reviews (PRISMA-ScR). 14
Search Strategy and Study Selection Process
Our search strategy and search terms were developed in collaboration with 2 experts in the field of transplantation. We searched the databases MEDLINE (Ovid and Pubmed) and CINAHL (Ebsco), complemented by citation tracking via GoogleScholar and expert recommendations to identify studies examining professional employment and related concepts after thoracic transplantation. Titles and abstracts were searched using search terms and their synonyms depicted in Figure 1. We included empirical studies published in English or German between January 1998 and March 2021 that focused on professional employment of adults after heart and/or lung transplantation. Studies that focused on retransplantation were purposefully excluded due to differing regulations between different countries and the comparatively poor physical capacity levels of retransplant recipients that would potentially bias the analysis. Full text screening, assessment, and data extraction were conducted by 2 authors independently. Results of this process were checked mutually until consensus was obtained. Ambiguous cases were discussed with a third author. A PRISMA flow diagram of the study selection process 14 is provided in Figure 1.
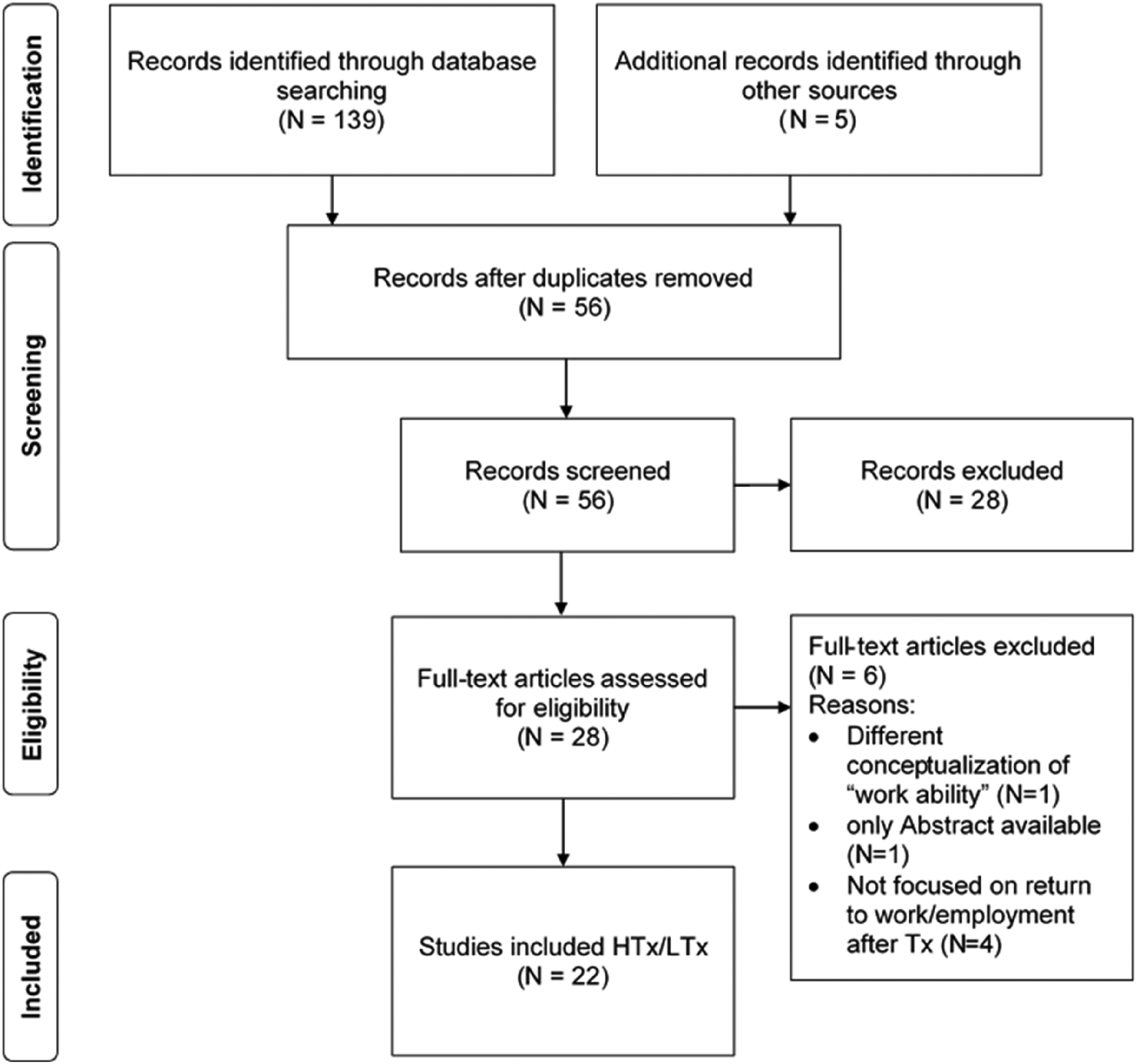
Search terms and PRISMA flow diagram of study selection process.
Bias Assessment
In accordance with the recommendations of the methodological literature for the typology of literature reviews, 13 a formalized quality assessment for this type of review (systematized) was not performed.
Data Extraction and Analysis
Data were extracted and summarized narratively and in tabular form. Whenever possible, extracted data were presented separately for heart and lung transplantation. If the desired data were not explicitly stated, but the data basis made it possible, we calculated and extrapolated these data. Data concerning aims (i), (ii), and (iii) were analyzed descriptively. Data concerning aim (iv) were analyzed thematically using an inductive approach. We further categorized the professional employment concept after thoracic transplant into (1) employment rate, as the amount of individuals that are or have been employed at a certain point of time after transplantation, regardless of pretransplant employment status, and (2) return to work, as the amount of individuals employed after transplantation who had been employed pretransplant (same or a different job), requiring valid intrapersonal data.
Results
Study Characteristics
We identified 22 studies from 11 countries published between 1998 and March 2021 reporting about the professional employment status after heart and/or lung transplantation. Most studies were cross-sectional (n = 15). Ten studies provide data on heart recipients,9,15–23 7 studies on lung recipients,10,24–29 and 5 studies included both.6,8,30–32 The studies were heterogeneous with regard to several aspects: (i) they differ considerably in sample sizes (N = 27 to N = 10 066), (ii) time since transplant (3 months to 18 years), (iii) age of participants (18-79 years), and (iv) the conceptualization of professional employment after transplantation. Table 1 provides an overview of conceptualizations used in included studies and the interpretation within this review based on the categorization of the professional employment concept as described in the introduction. Few studies provide data differentiated according to both professional employment and return to work.
Description of Study Characteristics (Studies are Sorted in Descending Order by Publication Date).
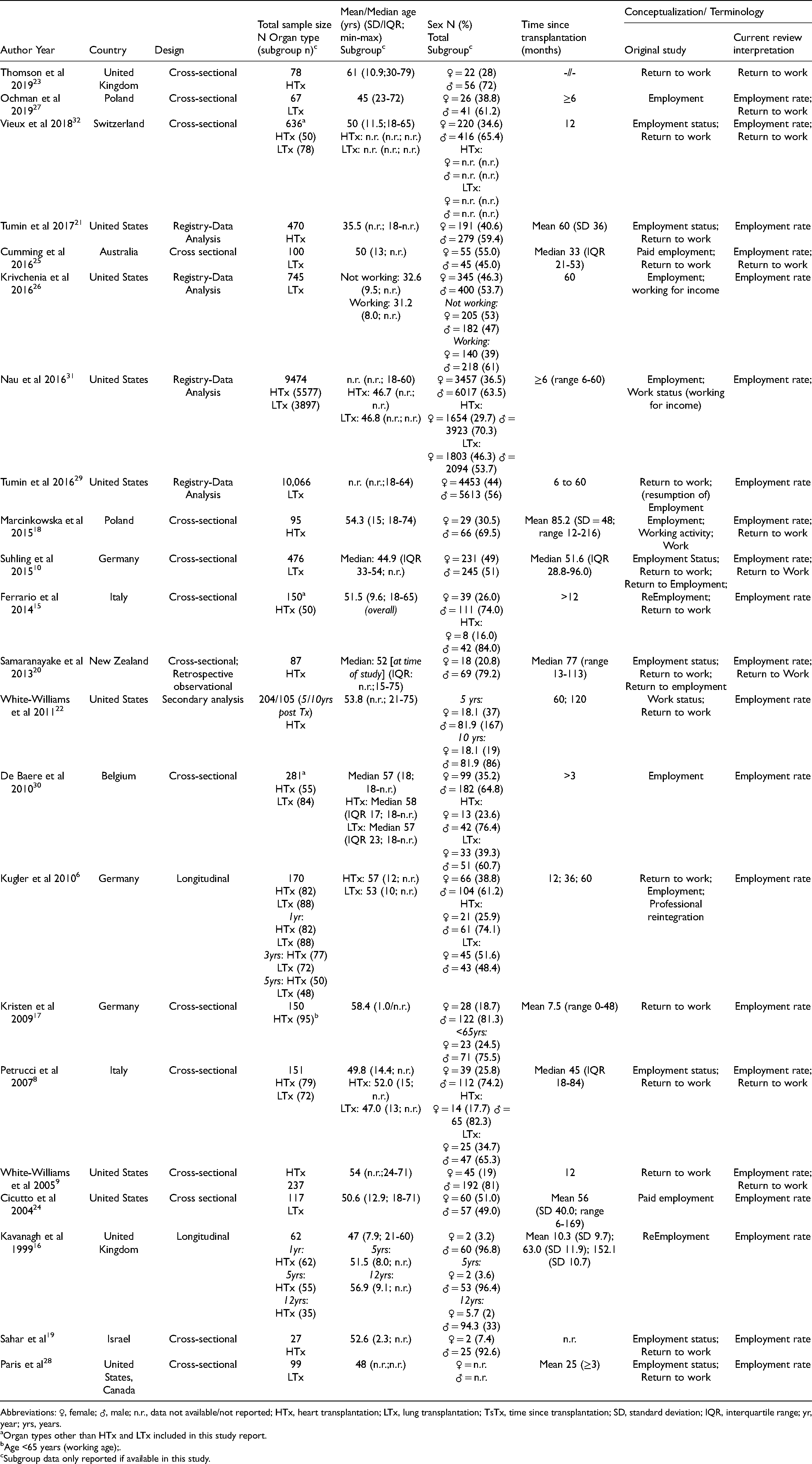
Abbreviations: ♀, female; ♂, male; n.r., data not available/not reported; HTx, heart transplantation; LTx, lung transplantation; TsTx, time since transplantation; SD, standard deviation; IQR, interquartile range; yr, year; yrs, years.
Organ types other than HTx and LTx included in this study report.
Age <65 years (working age);.
Subgroup data only reported if available in this study.
Professional Employment Rates
Posttransplant employment rates for professional employment were differentiated by organ type and ranged from 19.7% to 69.4% for heart, and from 7.4% to 50.8% for lung recipients, respectively (Figure 2). In addition, in 9 of the included studies,8–10,18,20,23,25,27,32 return to work rates (same or different job) for recipients posttransplant were provided. These rates ranged from 37.1% to 88.3% for heart recipients,8,9,18,20,23,32 and from 27.0% to 51.6% for lung recipients,8,10,25,27,32 respectively (Figure 2).
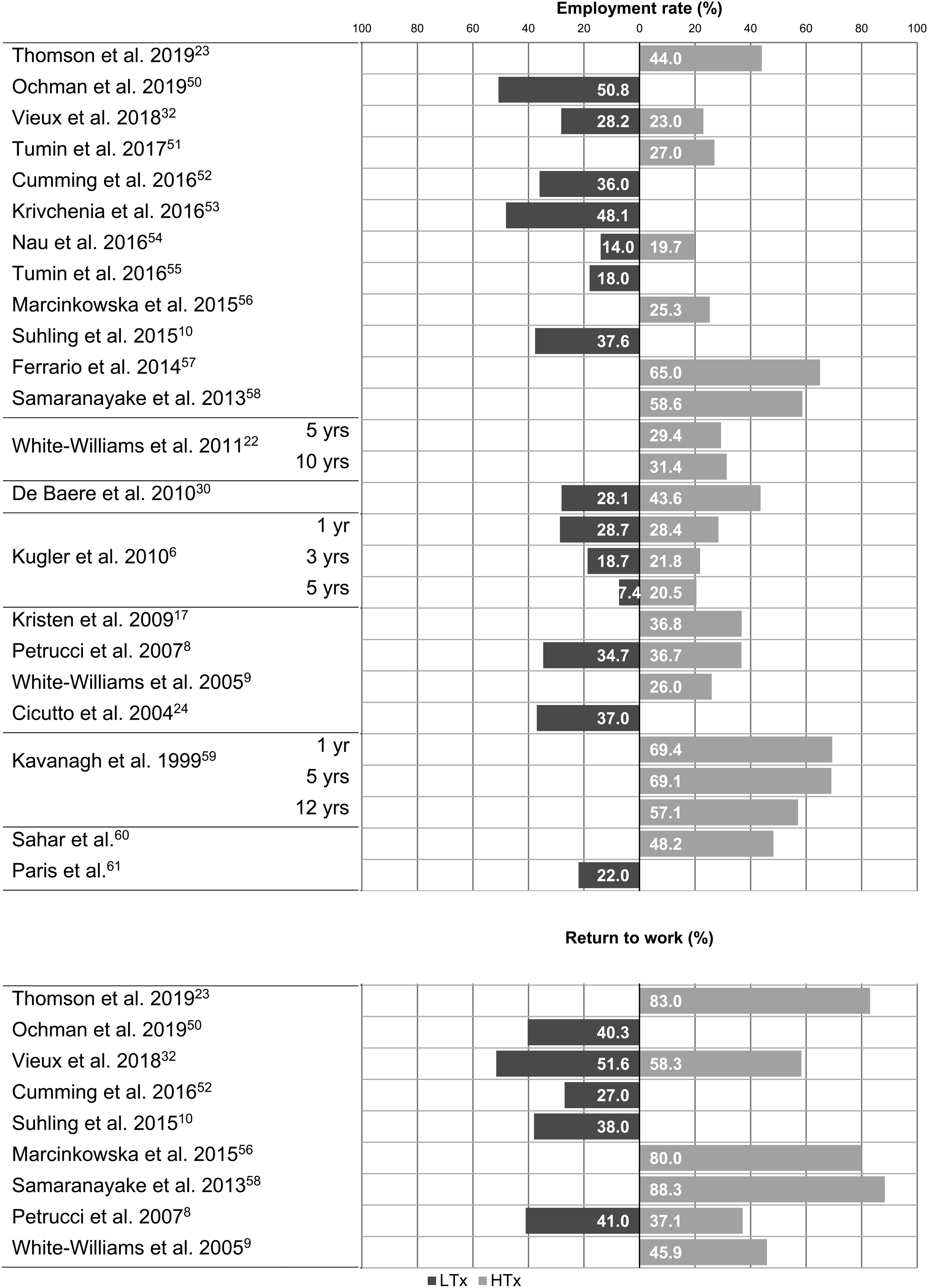
Rates of professional employment and return to work after heart and lung transplantation.
Factors Associated With Professional Employment
Correlates of professional employment that were investigated in these studies included demographic characteristics, employment-related factors, physical functioning (self-rated or objectively assessed), healthcare insurance status, and psychological aspects (mental health and/or social support). Factors statistically significant associated with professional employment for heart and lung transplantation and the numbers of studies that reported those factors are depicted in Figure 3. The most frequently reported positively associated factors were younger age (n = 12), followed by a higher level of educational attainment (n = 9), and a history of employment pretransplant (n = 7). In comparison, the number of studies reporting factors negatively associated with professional employment was lower, with the duration of unemployment prior to transplantation (n = 3), and Medicaid coverage (n = 3) being the most frequent.
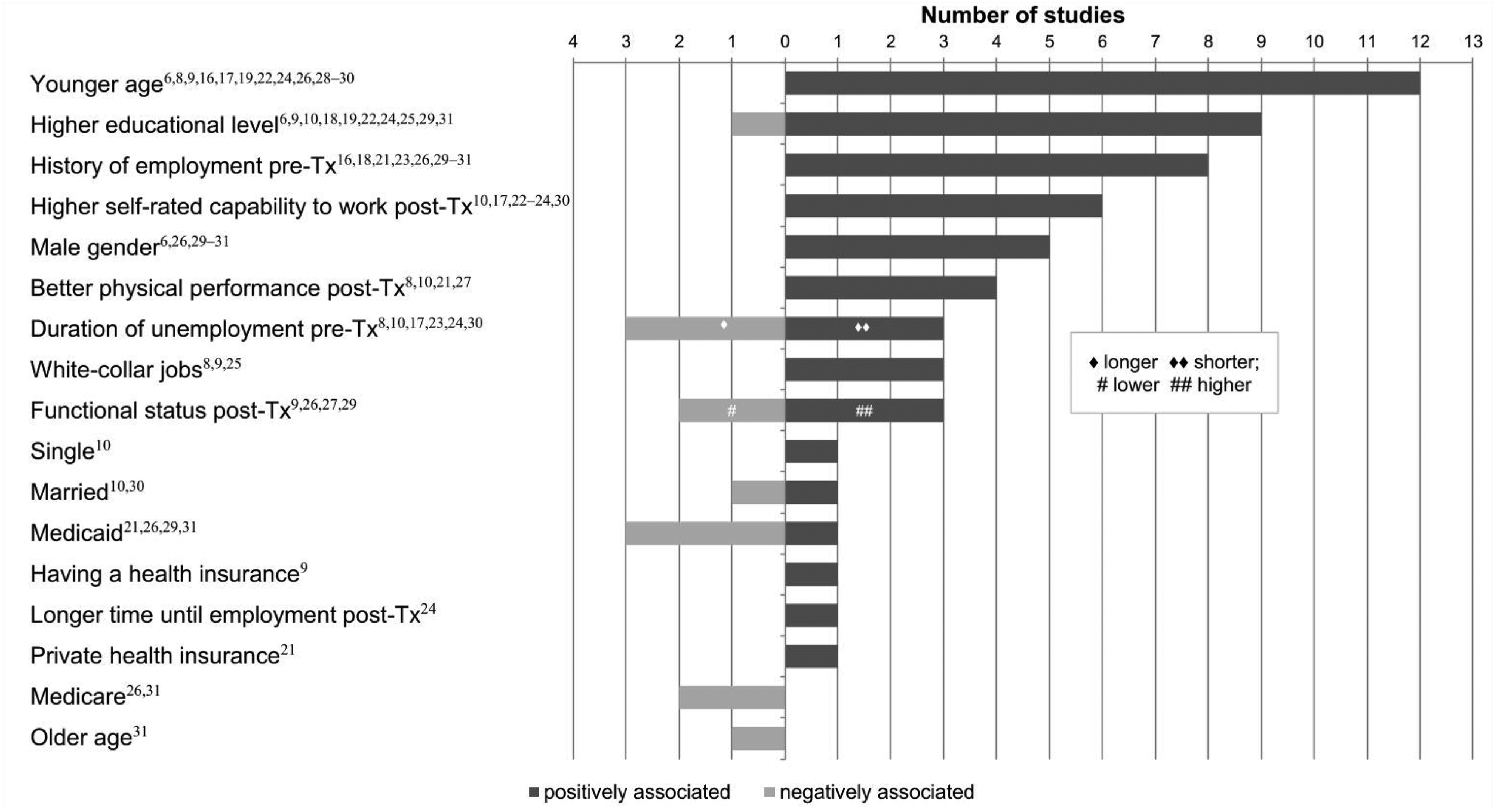
Statistically significant key factors associated with employment after heart and lung transplantation.
An analysis subdivided by organ type showed the following results. Most often reported factors positively associated with employment after heart transplantation were younger age (n = 6), higher level of education (n = 5), and a history of employment pretransplant (n = 5). Similarly for lung transplantation, positively associated factors were higher level of education (n = 7), younger age (n = 6), and male gender (n = 4). Negatively associated factors showed a larger spectrum in both groups, and none of these factors was reported remarkably often. The most frequently reported factors were health insurance related with Medicaid (n = 2) post heart transplant, and Medicare (n = 2) post lung transplant. A detailed overview of the respective factors is shown in Supplemental file 1 for heart transplantation and Supplemental file 2 for lung transplantation. Two studies could not be included in the subdivided analysis due to missing subgroup data.8,30
Financial and psychological factors have been reported, but were not included in graphical presentation due to their heterogeneity. For heart recipients the financial need for paid employment was positively associated with employment after transplantation, 17 whereas “governmental social assistance” for lung recipients 10 (p. 214) or “government benefits” for heart 23 (p. 255) recipients was negatively associated. With respect to psychological factors, those positively associated with employment among heart recipients were better mental health (eg, less depression, 22 better coping effectiveness, 9 ) less psychosocial disability, 9 and better perceived social support (social and economic satisfaction and family satisfaction). 22 None of the studies reported factors related to mental health or social support solely for lung recipients except Petrucci et al 8 reporting better mental health to be positively associated with employment after transplantation.
Four studies determined 6 facilitators for professional employment including the availability of the previous job, 24 better self-reported health, 24 physician encouragement to work, 24 a desire to enter the paid workforce, 24 higher physical activity levels,8,27 and living in cities. 18
Professional Employment and Relevant Outcome Parameters
Several studies reported on the relationships between professional employment and relevant outcome parameters, including episodes of acute (n = 7)8–10,17,22,29,32 and chronic (n = 4)6,10,22,29 rejection, infection (n = 5),8,9,22,29,30 QoL (n = 6),6,8–10,22,27 and survival (n = 2)10,29 (Table 2).
Statistically Significant Relationships Between Professional Employment and Relevant Outcome Parameters After Thoracic Transplantation (Studies are Sorted in Descending Order by Publication Date).
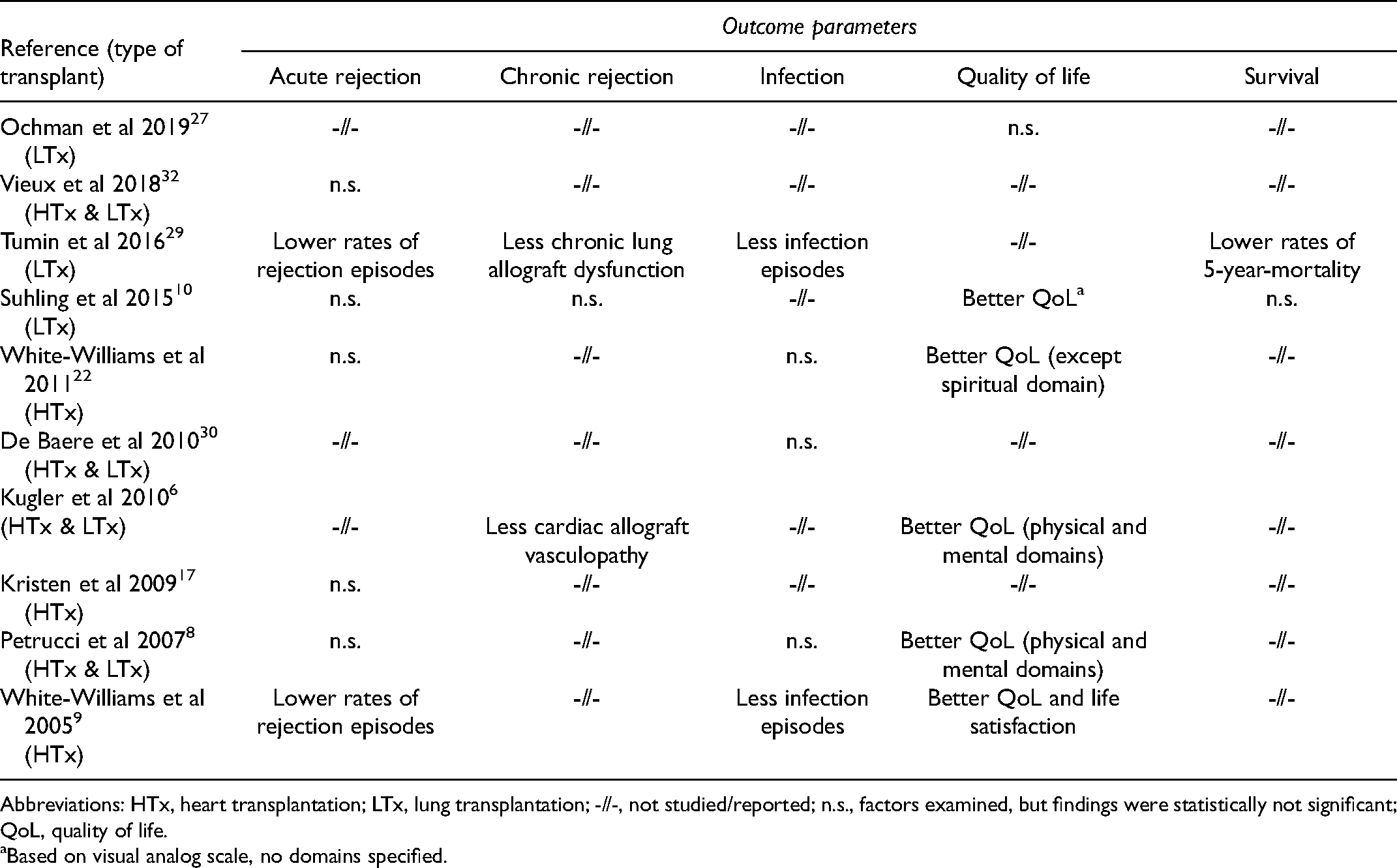
Abbreviations: HTx, heart transplantation; LTx, lung transplantation; -//-, not studied/reported; n.s., factors examined, but findings were statistically not significant; QoL, quality of life.
Based on visual analog scale, no domains specified.
Significant relationships between professional employment and relevant outcomes were lower rates of acute rejection and infection episodes,9,29 and 2 studies reported lower rates of chronic rejection namely less cardiac allograft vasculopathy in heart recipients, 6 and chronic lung allograft dysfunction in lung recipients. 29 Five studies reported better QoL among working recipients;6,8–10,22 one study showed a lower rate of 5-year-mortality. 29
Reasons not to Work or not to Return to Work
In 8 studies,6,10,15–17,20,24,30 a total of 27 reasons were identified based on quantitative and qualitative data as to why people did not work or did not return to work after transplantation. These reasons were inductively summarized into 4 categories (Supplemental file 3). The majority of reasons (n = 20) were allocated in the categories physical or mental health related reasons,6,10,15,16,20,24,30 and employment-related reasons.10,15,16,24 Physical or mental health-related reasons were for example concerns about contracting infections or side effects of transplant-related medications, lack of energy, dizziness, or lack of confidence and worries about discrimination. Examples for employment-related reasons were inappropriately adapted workplaces or lack of flexibility in job hours and duties. Financial reasons (n = 4),10,17,24,30 and lifestyle choices (n = 2)20,24 were stated less commonly. One reason (family reasons) 10 could not be allocated because of its nonspecificity.
Discussion
In this systematized review, professional employment of heart and lung recipients was synthesized and revealed employment rates between 19.7% and 69.4% for heart-, and 7.3% and 50.8% for lung recipients. Key factors positively associated with professional employment and most frequently reported for both organ types included younger age, higher educational level, a history of employment before transplant, and higher self-rated capability to work posttransplant. Specifically, age may have been associated with employment as older recipients may have decided to retire if they had reached the retiring age.
Few studies focused on the relationship between professional employment and relevant clinical outcome parameters. Promising findings were reported with respect to lower rates of acute and chronic rejection, less infection episodes, and better QoL among those working after transplantation. One retrospective study indicated a lower rate of 5-year-mortality in employed recipients. Reasons for no professional employment included health-related reasons, employment-related and financial reasons, and lifestyle choices as reported by the recipients.
Most studies included in the review assessed professional employment using retrospective, cross-sectional study designs. Three out of 21 studies however, used a more systematic approach and assessed professional employment rates of heart recipient cohorts at several time-points posttransplant16,22 or applied a prospective, longitudinal study design. 6 Findings from those studies show somewhat conflicting findings. Two studies report that professional employment rates decreased over time posttransplant,6,16 whereas White-Williams and associates 22 observed a slightly increased employment rate in heart recipients at 10 years in comparison to those 5 years posttransplant. Interestingly, in the study by White-Williams and associates 22 no clinical differences in those working versus not working were identified at 10 years posttransplant and the authors assume that having fewer clinical problems immediately posttransplant may facilitate professional employment. In contrast, in the 2 other studies6,16 in which professional employment declined over time, this was associated with decreases in QoL. 6 It might be argued, albeit with caution, that clinical conditions including the increased risk to develop chronic rejection, and other physically limiting co-morbidities, might limit or preclude recipients’ capability to keep up with professional work-life demands with advancing age posttransplant. Thus, these findings might be in line with the declining employment rates in the general population, with advanced age, due to the onset and progression of physical and mental limitations due to chronic conditions. 33
Despite advancements in both lifespan and QoL following thoracic transplantation, substantial proportions of recipients being in employable age ranges do not seek professional reemployment.21,29,31,32 Given the perspective that the transplant procedure is associated with high costs and a potential return in investment for the society, 9 current societal strategies to support recipients in this regard need to be questioned. Employment rates may, at least in part, relate to healthcare system-related differences, for example, in some of the European welfare systems disability benefits and unemployment insurances may provide a safer and more predictable income than reengagement into the active labor market.10,17,30,34 This becomes particularly important as professional employment was not related with an increased risk for infections, and acute or chronic rejection episodes, but instead carries an opportunity to further increase recipients’ QoL, an important parameter to measure the success of this costly procedure. 35 Ivarsson and associates 36 point towards the perceived needs of recipients during the first 6 months following transplantation to returning to a relatively normal life. Their recipients expressed gratitude when their health improved markedly, but they also expressed resignation due to a lack of information and support received which might result in recipients not returning to a professional work-life and remaining dependent on disability funds.10,17 Thus, candidates for thoracic transplantation should (1) be assessed regarding opportunities to remain/reengage into a professional employment before and after transplantation, (2) for those in medically stable conditions, transplant candidates should be encouraged to remain in the professional workforce as long as possible, and at least with a part-time position throughout the waitlist period, (3) assessment and counseling should include working conditions, financial resources, physical and mental health, and expectations of both recipients and relatives before and following transplantation to support an adjustment to normal life and reengagement into the society posttransplant.
This review suggests higher employment rates for heart in comparison to lung transplant recipients, although lung recipients tend to be of younger age at the time of transplantation.6,37,38 Multiorgan comparison studies with emphasis on QoL outcomes following different types of organ transplantation suggest that heart versus lung recipients differ with respect to their physical,6,38–41 and their mental39,40 status posttransplant. Differences in this demographic variable might also be explained, albeit with caution, by the disease severity before transplantation and the risk for infections posttransplant. The higher immunosuppressive maintenance regimen following lung versus heart transplantation might cause more frequent and more distressing immunosuppression related side-effects, specifically fatigue and concentration difficulties,42–45 and more muscle-related physical limitations. 27 Further research is necessary to determine the associations between the physical and mental status of recipients after transplantation and their professional employment posttransplant.
Determinants for professional employment may be subdivided into those factors being modifiable by clinical interventions versus those being nonmodifiable factors, for example, age, and education. While the majority of determinants investigated in the studies included in this review are nonmodifiable, they can be used for a systematic assessment and for clinical consultations, to provide recipients with realistic expectations for their life following transplantation. In association with employment, only 2 studies examined mental health8,22 and only one study reported on perceived social support. 22 Considering that depression- and anxiety-related symptoms are common in thoracic transplantation populations, and that these factors together with social isolation also affect clinical outcomes,46,47 these potential determinants of (un-)employment deserve further attention. Physical and mental status are prone to interventions by the multidisciplinary transplant team and may include physical exercise training, concentration-increasing exercises and/or mind-body relaxation techniques.48,49 In addition, higher education implies other, often less physically demanding occupational fields. Thus, for some cases careful and targeted interventions may include counseling on opportunities regarding the educational path for patients before and following transplantation. This is in line with the recommendations of D’Egidio at al. 50 concerning kidney transplant recipients underlining the importance of social and psychological support within multidisciplinary programs focusing on self-management support and of involving employers to facilitate employment. The same principles are suggested for recipients of stem cell transplants. 51
The current evidence on professional employment is limited due to conceptual, methodological, and measurement-related shortcomings that clearly need to be addressed in future studies. First and foremost, the definition of professional employment lacks a common consensus and standardization, which leads to a limited generalizability of available data. Thus, different and nonstandardized concepts of professional employment status/return to work, limit the comparability of prevalence rates across studies. Second, most data have been drawn from self-developed, nonstandardized, nonpsychometrically tested questionnaires or unstructured interview techniques further limiting the existing evidence to date. Third, the majority of the studies report employment rates from single-sites resulting in small sample sizes and potential center-policy related biases. Finally, most reports applied cross-sectional study designs, preventing causal relationships between employment and potential associations and determinants to be drawn, and do not allow to draw conclusions on whether employment was associated with improved outcomes or the other way around.
Strengths and Limitations
This review provides a descriptive overview of the literature on professional employment after thoracic transplantation that can be used by researchers as a starting point to develop new research questions or for problem identification, and by clinicians to widen their point of view to the occupational situation after transplantation enabling them to develop supporting interventions.
This systematized review of the literature is limited by methodological considerations. Despite being systematic in searching and analyzing the data we only searched 2 bibliographic databases and did not assess risk of bias or performed further critical appraisal. In addition, studies available were heterogeneous in their methodological quality of presenting their findings (eg, inconsistency in the terminology used, outlining the time since transplant at the time-point of their data collection), thus limiting the capacity for firm conclusions. The results of this study need to be interpreted with caution.
Conclusions
Despite marked improvements in overall survival and QoL, a substantial proportion of heart and lung recipients are not professionally employed, potentially diminishing the success on individual and on societal levels. Among the factors positively associated with professional employment, some are modifiable by targeted interventions from healthcare professionals: these include functional and mental status, and physical performance. Acknowledging the few occupational restrictions, mainly due to infectious susceptibility, professional employment may lead to better QoL and should be considered for counseling for future candidates both before and after thoracic transplantation.
Supplemental Material
sj-docx-1-pit-10.1177_15269248211064883 - Supplemental material for A Systematized Review of Professional Employment Following Thoracic Transplantation
Supplemental material, sj-docx-1-pit-10.1177_15269248211064883 for A Systematized Review of Professional Employment Following Thoracic Transplantation by Stefan Jobst, Jonas Schaefer, Christina Kleiser and Christiane Kugler in Progress in Transplantation
Supplemental Material
sj-docx-2-pit-10.1177_15269248211064883 - Supplemental material for A Systematized Review of Professional Employment Following Thoracic Transplantation
Supplemental material, sj-docx-2-pit-10.1177_15269248211064883 for A Systematized Review of Professional Employment Following Thoracic Transplantation by Stefan Jobst, Jonas Schaefer, Christina Kleiser and Christiane Kugler in Progress in Transplantation
Supplemental Material
sj-docx-3-pit-10.1177_15269248211064883 - Supplemental material for A Systematized Review of Professional Employment Following Thoracic Transplantation
Supplemental material, sj-docx-3-pit-10.1177_15269248211064883 for A Systematized Review of Professional Employment Following Thoracic Transplantation by Stefan Jobst, Jonas Schaefer, Christina Kleiser and Christiane Kugler in Progress in Transplantation
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.