
Abstract

Background
Heart transplant is an established treatment for selected patients with end-stage heart failure. Maximizing long-term survival is a primary focus of posttransplant management and research. Optimal outcomes after transplantation require adherence to a complex therapeutic regimen consisting of immunosuppressants, co-medications and nonpharmacological health-related behaviors, such as sun protection, sufficient physical activity, appropriate diet, smoking cessation, appropriate alcohol use and appointment adherence to follow-up visits.
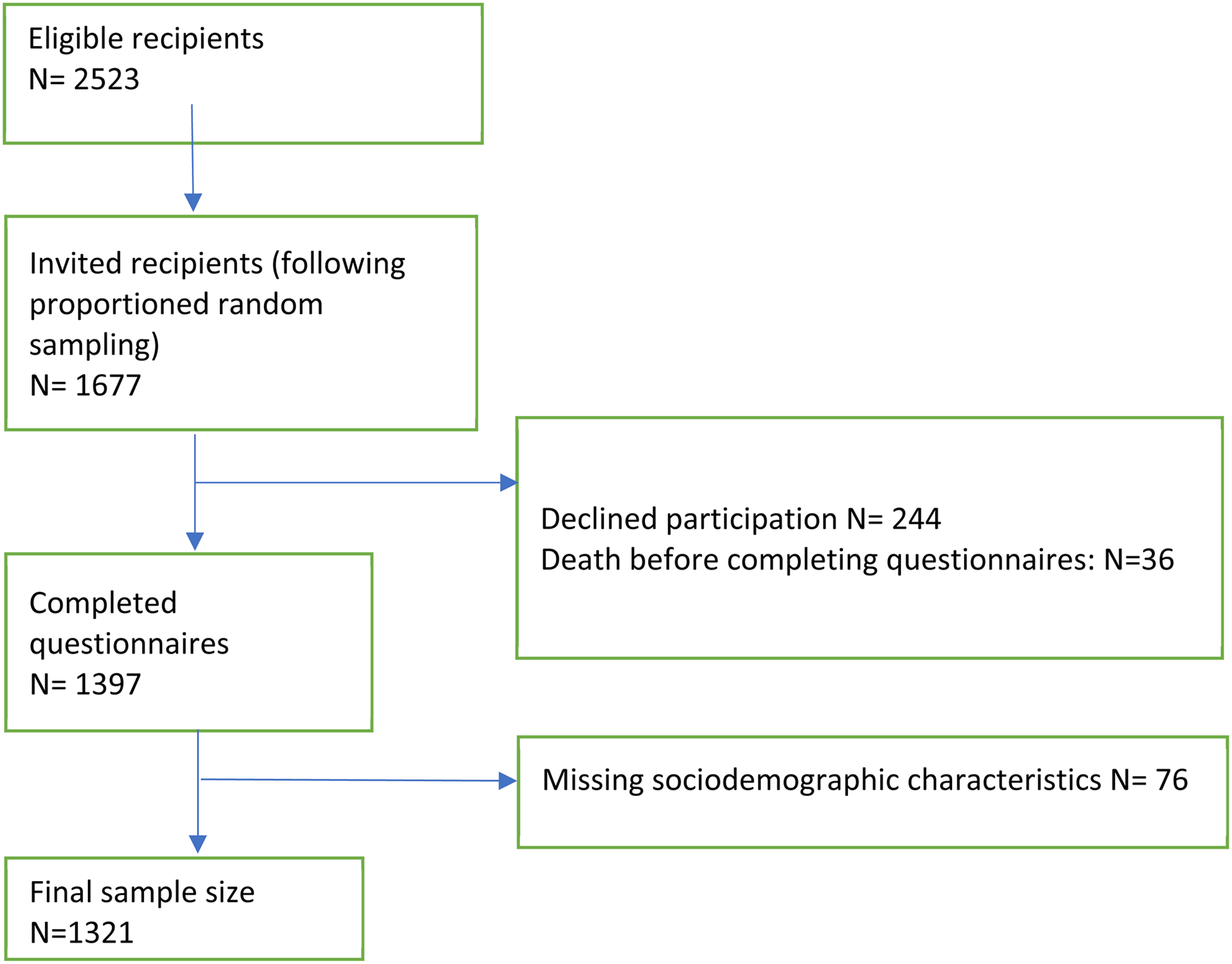
Flowchart of heart transplant recipient sample.
Adherence to nonpharmacological treatment can reduce the risk after transplant just as in the general population.1,2 Chronic exposure to immunosuppressant medications has potential serious side effects within 10 years of transplantation, including hypertension (70-90%), 1 dyslipidemia (>50%), 2 diabetes (11-38%), 3 osteopenia/osteoporosis (13-17%), 4 cardiac graft vasculopathy (50%), 5 malignancy (7-82%),6,7 and chronic kidney disease (25-68%). 8 Emerging literature has shown that nonadherence to nonpharmacological health-related behaviors posttransplant, negatively impacts morbidity and mortality and the determinants of behaviors.9–19
According to the International Society for Heart and Lung Transplantation's (ISHLT) registry the median survival, conditional on survival to 1 year, for adult recipients overall, is 13.9 years with females surviving longer than males, 14.8 years versus 13.6 years, respectively. 16 A large cohort study of heart recipients reported that females were less likely to have diabetes mellitus, hypertension, peripheral vascular disease, tobacco use, prior cardiovascular surgery and were less supported by an intra-aortic balloon pump or durable ventricular assist device than males but were more likely to have a history of malignancy or require intravenous inotropes. Males had a higher Index for Mortality Prediction After Cardiac Transplantation score. 20
There is a limited and emerging literature on adherence to lifestyle recommendations in transplantation. For example, Brocks et al reported no gender difference in adherence to recommended lifestyle habits in heart transplant recipients. 21 Dew et al found that male gender was protective against home self-care adherence in lung transplant recipients 9 and Fine et al found that females were more adherent that males in solid organ transplant recipients 22 as did Germani. 23 Siwinska et al found that females adhered more with health-related behaviors. 24 In a meta-analysis Duerinckx et al 12 found that males were 1.33 times more likely to engage in smoking post-transplant than females and Dobbels et al noted that male gender was associated with alcohol use post-transplant, 13 while Berben et al found no relationship to low physical activity. 11 In these analyses, the specific gender association with adherence is usually noted as an aside to the primary endpoints, finding varying results.
Geographical data in nonpharmacological health-related behaviors in transplantation is limited, however, a previous global BRIGHT study analysis reported an overall 52.2% adherence to physical activity, 60.1% adherence to sun protection, 61.8% adherence to diet recommendations, 77.1% adherence to alcohol use, 92.6% adherence to not smoking, and 94.3% adherence to follow-up visits. 19
The aims of this secondary analysis of the BRIGHT study were: (a) to describe gender-specific prevalence of nonpharmacological health-related behaviors post-heart transplant (ie, sun protection, diet, physical activity, appointment keeping, alcohol use recommendations and not smoking), and (b) to investigate gender differences of health-related behavior at the continent level.
Methods
Design
This was a secondary analysis of the Building Research Initiative Group: Chronic Illness Management and Adherence in Transplantation (BRIGHT) study, a cross-sectional, multinational, multicenter study that included 1397 adult post-heart transplant patients following a 3-level ecological model of behavioral determinants: the micro level (interpersonal or face-to-face relationships), the meso level (practice patterns or health care organization characteristics) and the macro level (health care system where the patient lives, including local, state and national health laws and policies).
The BRIGHT study was designed to explore the associations of multiple correlates examining the factors linked to medication and nonpharmacological health-related adherence and details of the study methods have been previously published.17–19
Sampling
The BRIGHT study applied a multi-stage sampling approach. A convenience sampling of 36 heart transplant centers from 11 countries in Europe, North America, South America and Asia was used. Centers were included if they had performed at least 50 heart transplants over the 60 months prior to inclusion and the willingness of a heart transplant director and an administrator to participate.
A proportional random sample of patients in the participating centers included adults, 18-years-old at the time of enrollment, transplanted and received care at the participating center, a single organ recipient and recipients of a first heart transplant, 1 to 5 years posttransplant, who could read and understand one of the study materials’ languages, and provide written informed consent. Dual organ recipients, those who had participated in a medication adherence intervention research or drug trials the 6-month period prior to study consent, or if had any type of professional support to enhance medication adherence were excluded.
The BRIGHT study was approved by the University of Leuven (Belgium) Ethics Review Boards as well as by each heart transplant center's Institutional Review Board. The data were collected between March 2012 and October 2015.
Data Collection
Variables were assessed by chart review and through the BRIGHT questionnaires, completed by patients’ self-report. Questionnaires included self-developed and established measures, as specified in the published BRIGHT protocol17 and previous papers.18,19 The demographic characteristics included patientś age, time since transplantation, race/ethnicity, marital status, education, insurance, employment, and living status. Adherence to nonpharmacological health-related behaviors were assessed as follows:
Health-Related Behaviors
Sun protection. Adherence was measured using a scale based on the Swiss childhood cancer registry and on the Cambridge University Hospitals’ perception of skin cancer in transplant recipients.25,26 Patients were asked how consistently they protected themselves against the sun regarding four protective behaviors: applying sunscreen, wearing a hat or clothes with long sleeves, staying in the shade, and being sensitive to the time of the day and sun exposure. Adherence to these items was assessed using a Likert scale ranging from 1 (never) to 5 (always), from which a total average score was calculated.
Diet. Adherence was assessed using a 5-item instrument specifically developed for the BRIGHT study. Adherence to dietary advice regarding low salt, low calorie, low saturated fat, low sugar and/or any other kind of diet was only assessed in case one or more of these diets had been prescribed and was rated on a 5-points Likert scale ranging from 1 (never) to 5 (always).17 Adherence was defined as the total average score over the scored items (ie, for the prescribed diets). Patients not having prescribed a diet were not included in the analysis.
Sufficient physical activity. Activity was assessed by the Brief Activity Assessment tool, 27 a 2-item validated measure assessing a patient's vigorous and moderate activity performed during an average week. Patients were considered adherent if they had at least 20 minutes of vigorous activity 3 times per week, or if they did moderate physical activity of 30 minutes at least 5 times per week or combinations of both vigorous and moderate activity.
Appointment keeping. Attending appointments were assessed by one self-report item. Patients were considered adherent if they reported not having missed any of the past 5 scheduled outpatient clinic appointments. Nonadherence was scored as having missed 1 or more appointments. 19
Alcohol use. Use was assessed by 2 items asking whether the patient consumed alcohol during a typical week and the number of alcoholic drinks consumed. 19 A gender-specific operational definition differentiated adherence from nonadherence: females were adherent if they did not have more than 1 unit per day while males were adherent if they did not have an intake of more than 2 units per day. One unit was defined in terms of pints of beer (1 pint is 12 oz or 355 mL), glasses of wine (1 glass is 5 oz or 148 mL) or shots of spirits (1.5 oz or 45 mL).
Not smoking. Tobacco use was assessed by a question from the Swiss Health Survey 28 with the following answer options for tobacco use behavior: currently smoking, stopped smoking less than a year ago, stopped more than a year ago, or never smoked (yes/no). Patients were scored as adherent if they had stopped smoking more than one year ago or had never smoked, as not smoking was a heart transplant requirement.
Data Analysis
Descriptive statistics used frequencies, measures of central tendency (means, medians) and variability (standard deviations and IQR), depending on measurement level and distribution of variables. The prevalence of adherence at the continent level were weighted for the size of the transplant population per country based on data from the Global Observatory on Donation and Transplantation covering the same years of patient's transplant dates. 29 Bivariate comparisons of sample characteristics between the genders used two-sample t-tests, Chi-square tests or Mann-Whitney U test and Fisher exact test, as appropriate. Weighted multiple linear regression analyses were used to compare gender differences for continuous variables sun protection and diet keeping. Weighted multiple logistic regression analyses tested for gender differences in the above-defined dichotomous adherence measures of health-related behaviors, sufficient physical activity, appointment keeping, alcohol use recommendations and not smoking. All the regression models were adjusted for patients’ age, race, marital status, education level, employment status, and insurance type. Statistical significance for all statistical tests was set at 0.05. All the data were analyzed using Stata 15.1.
Results
Sample Characteristics
There were 36 participating centers with 2523 post-heart transplant recipients that met inclusion criteria, from which 1677 patients were randomly selected and invited to participate. Of those, 244 declined and 36 died prior to enrollment; 76 had missing data in sociodemographic characteristics, resulting in a final sample size of 1321 for this analysis (Figure 1).
Overall, females were younger and less likely to be employed than their male counterparts (Table 1). Subgroup analysis by continent of residence found European females to be younger, more frequently living alone and less frequently working posttransplantation. In North America, more males were white than females. There was no significant gender difference in marital status, education, or insurance coverage, regardless of the continent.
Sociodemographic Characteristics Stratified by Continent and Gender.
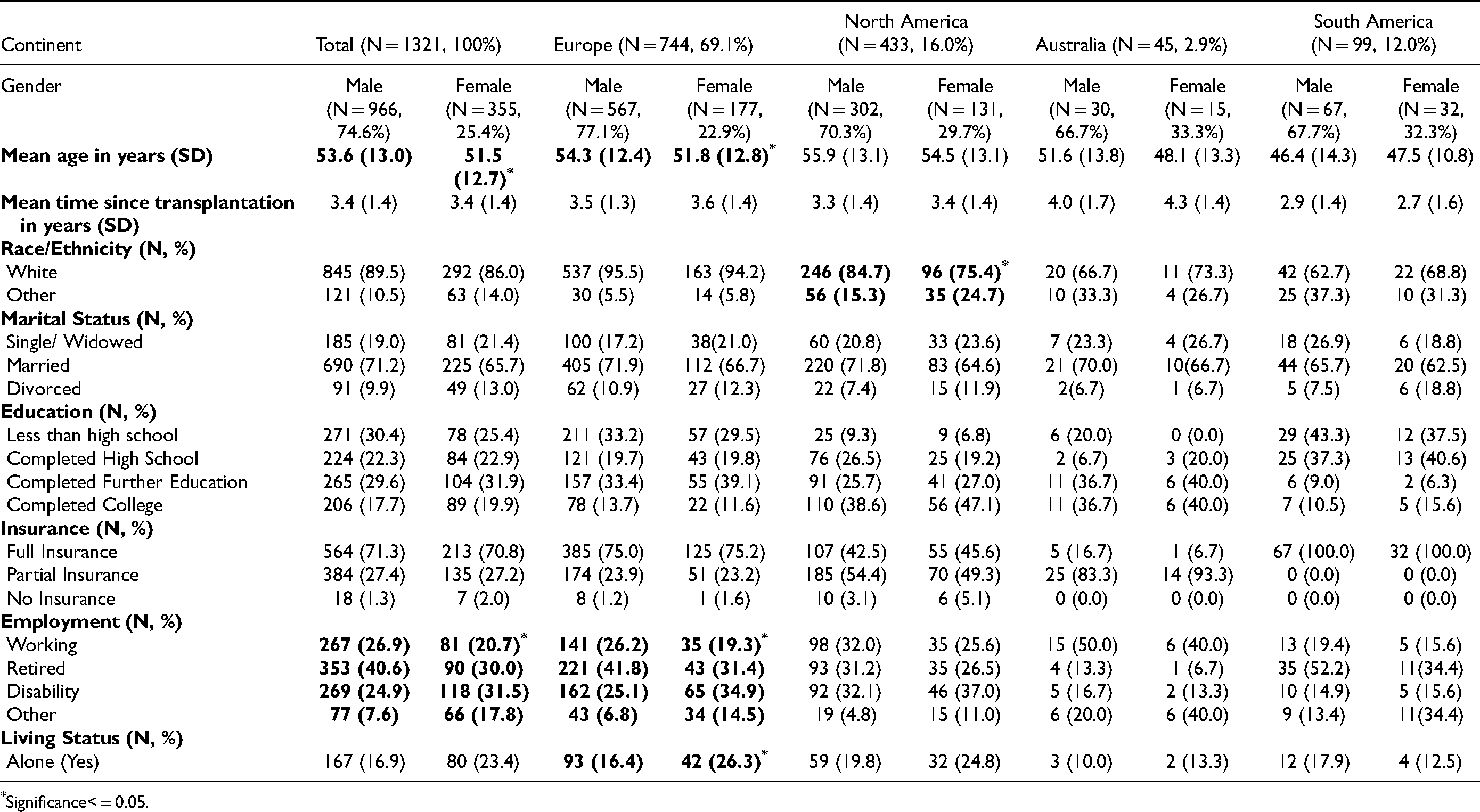
Significance< = 0.05.
Table 2 presents adherence to nonpharmacological health-related behavior comparisons by gender, overall and per continent. Overall, females were more adherent to sun protection (P = 0.00), not smoking (P = 0.00) and alcohol use recommendations (P = 0.00) and less adherent to sufficient physical activity than males in Europe, North America, South America and Australia (P = 0.00 respectively), and to not smoking recommendations in South America (P = 0.01).
Adherence Comparisons To Nonpharmacological Health-Related Behavior By Gender Globally And Per Continent.
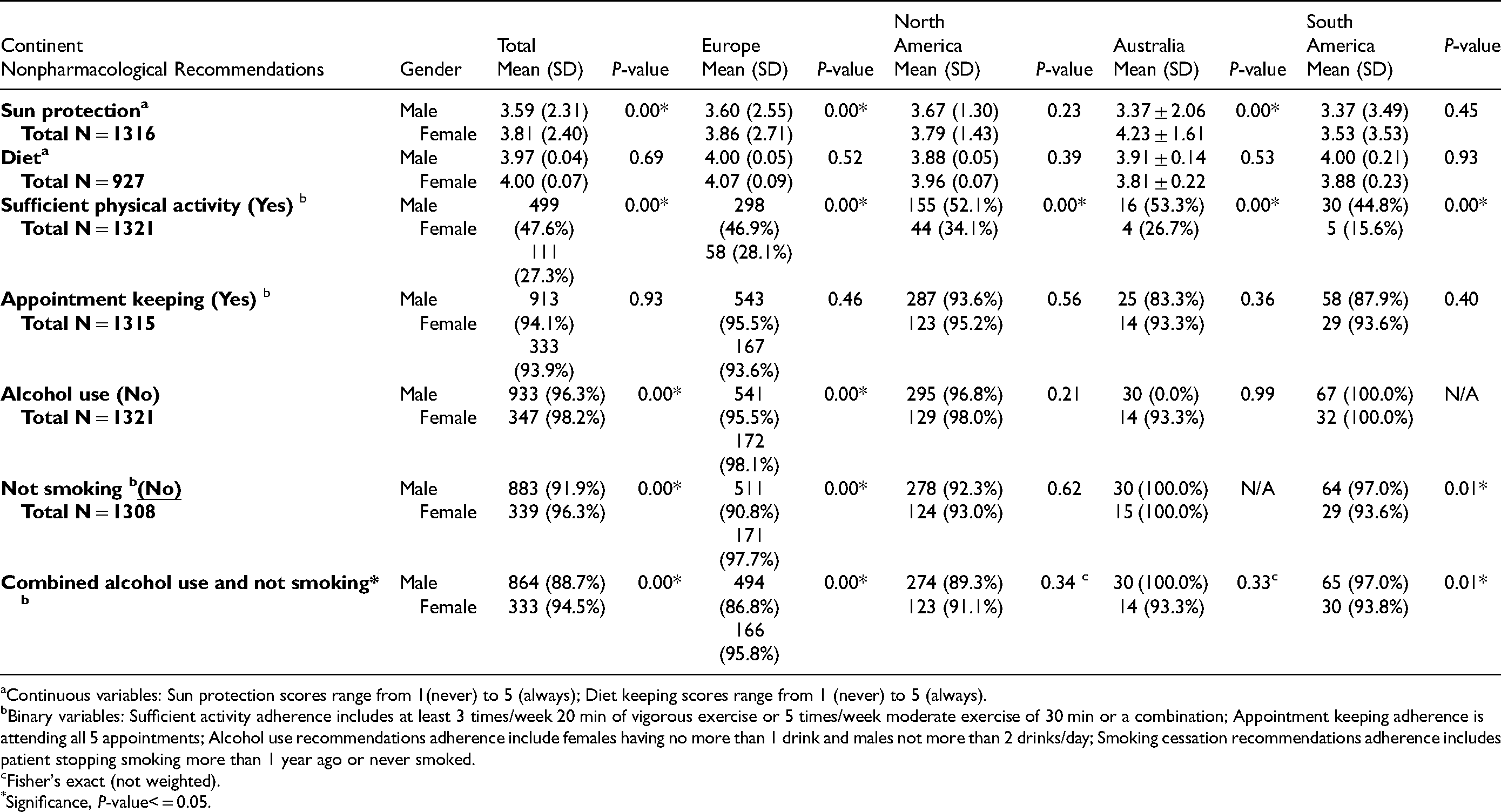
Continuous variables: Sun protection scores range from 1(never) to 5 (always); Diet keeping scores range from 1 (never) to 5 (always).
Binary variables: Sufficient activity adherence includes at least 3 times/week 20 min of vigorous exercise or 5 times/week moderate exercise of 30 min or a combination; Appointment keeping adherence is attending all 5 appointments; Alcohol use recommendations adherence include females having no more than 1 drink and males not more than 2 drinks/day; Smoking cessation recommendations adherence includes patient stopping smoking more than 1 year ago or never smoked.
Fisher's exact (not weighted).
Significance, P-value< = 0.05.
Table 3 presents multivariable gender analysis of the assessed nonpharmacological health-related behaviors. When controlling for age, race, marital status, educational level, employment status and insurance type, females were more adherent to sun protection (β = −0.24, P = 0.00) and to not smoking (β = 0.37, P = 0.00) compared to males. Overall, the odds of male adherence to sufficient physical activity were higher compared to females (AOR = 2.39, P = 0.00). At the continent level, in Europe and in Australia, females were more adherent than males to sun protection (β = −0.27, P = 0.00 and β = −0.86, P = 0.00, respectively), and in Europe to not smoking (β = 0.20, P = 0.00). Males were more adherent than females to sufficient physical activity in Europe (AOR = 2.27, p = 0.00), North America (AOR = 2.08), Australia (AOR = 3.44, P = 0.00) and South America (AOR = 7.54, P = 0.00).
Multivariable Analysis of Adherence to Nonpharmacological Health-Related Behaviors by Gender Globally and Per Continent.
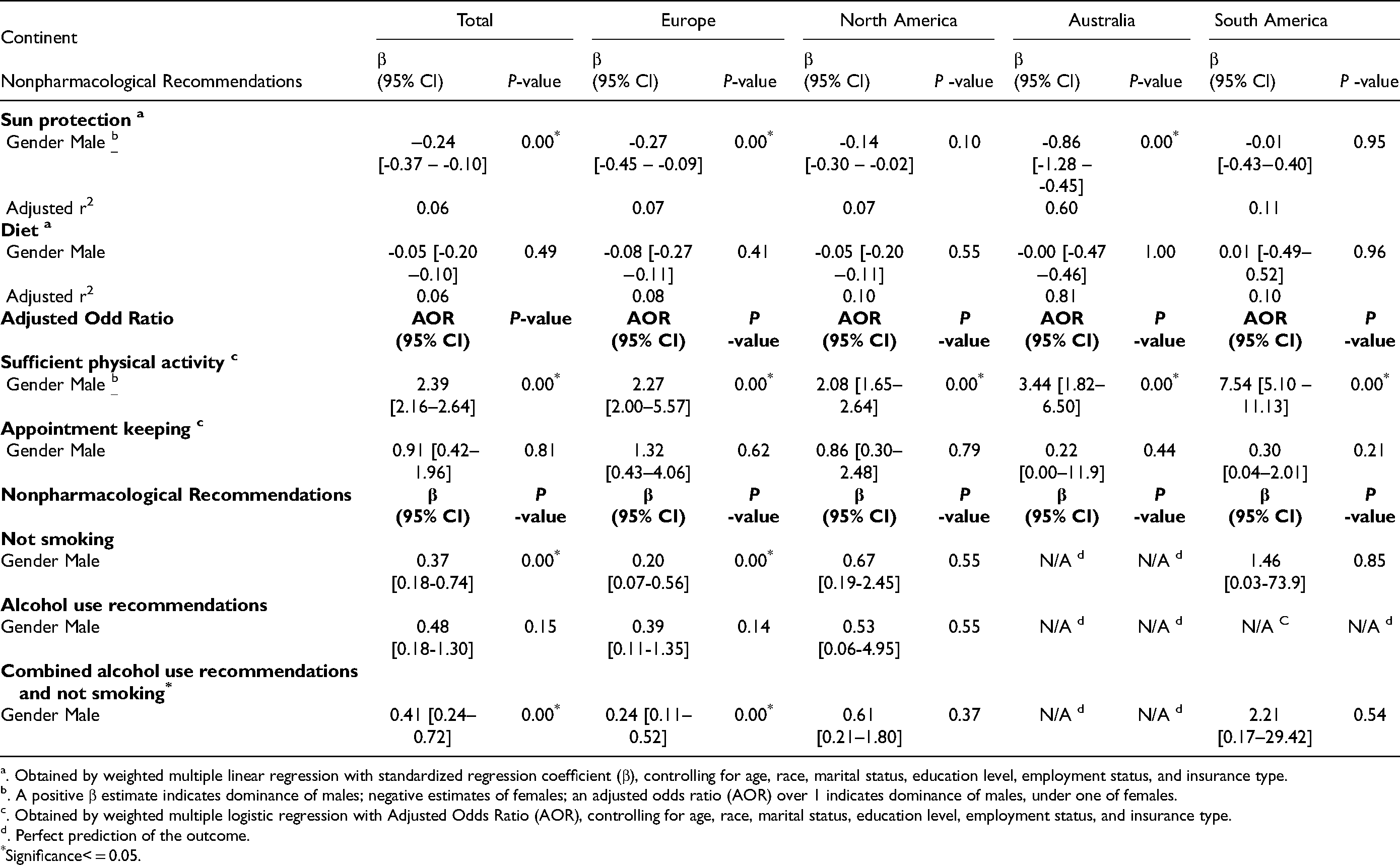
. Obtained by weighted multiple linear regression with standardized regression coefficient (β), controlling for age, race, marital status, education level, employment status, and insurance type.
. A positive β estimate indicates dominance of males; negative estimates of females; an adjusted odds ratio (AOR) over 1 indicates dominance of males, under one of females.
. Obtained by weighted multiple logistic regression with Adjusted Odds Ratio (AOR), controlling for age, race, marital status, education level, employment status, and insurance type.
. Perfect prediction of the outcome.
Significance< = 0.05.
Discussion
Using the BRIGHT study dataset we found gender differences in nonpharmacological health-related behaviors with females being more adherent to sun protection and to not smoking while males were more adherent to sufficient physical activity, overall. Continent-specific analysis confirmed these findings. Our findings are in line with previous evidence.30–33
Our findings suggest a less favorable behavioral phenotype of male transplant recipients for 2 of the 6 assessed nonpharmacological health-related behaviors: not smoking and sun protection. The less favorable behavioral phenotype might contribute to risks against male survival post-heart transplant, even though a favorable factor for positive transplant outcomes in the male behavioral phenotype was the higher adherence to sufficient physical activity.16,34
The female behavioral phenotype in our study highlighted a better profile in view of sun protection and not smoking, potentially contributing to the lower observed incidence of malignancies and lower incidence of graft vasculopathy compared to males over an observation period of 10 to 15 years posttransplant in the ISHLT registry. 16 Our study did not examine the link between health-related nonpharmacological behaviors to transplant outcome due to the cross-sectional design.
Despite the increasing evidence that health-related behaviors are independent risk factors for poor transplant outcome,12–16 the behavioral pathway in the development of transplant complications is seldom studied and interventional approaches to improve transplant outcomes generally focus on medication adherence, and the gender perspective is absent in explaining nonpharmacological health-related behaviors. 35
Sun protection is crucial for the prevention of skin cancer, as malignancy continues to be a major contributor to post-heart transplant morbidity, with an incidence of 28% at 10 years posttransplant. 16 Adherence to sun protection overall was 61.8% in a previous analysis of the BRIGHT study. 19 Our analysis showed that females were more adherent overall, in Europe and in Australia. A recent systematic review evaluating interventions for the prevention of skin cancers in solid organ transplant recipients concluded that the quality of evidence was low, 36 suggesting that more behavioral and or pharmaceutical interventional studies could improve gender sun protecting behaviors. Studies could focus on gender sun protection differences at the continent level to compare and to contrast them.
Diet may decrease the risk for obesity, diabetes mellitus, and hypertension, all risk factors posttransplantation. 16 The overall prevalence of adherence to diet in a previous BRIGHT study was 61,8%, 19 and our data did not show a gender difference in diet adherence behaviors posttransplant overall or at the continent level. More studies about gender differences in diet keeping after heart transplant may provide further insight into optimal diets.
Physical activity was associated with success after transplantation. 11 Overall, adherence to sufficient physical activity posttransplantation was 52.2% in a previous BRIGHT study. 19 In our study males were more adherent than females globally, in Europe, North America, Australia and South America. Lower female adherence may be explained by a combination of household and child rearing in addition to professional duties outside of the home, 22 and this needs to be tested. Physical activity was associated with better prognosis and healthy aging, and studies should focus on gender differences in physical activity adherence and habits posttransplantation to close the male-female gap.
Appointment keeping post-heart transplant is important for medical education and successful follow-up. Gender differences in adherence to medical appointments are scarcely studied, however one study reported the global rate of adherence of 94.3%. 19 Our data did not show significant gender differences overall or at the continent level. Appointment keeping nonadherence was an independent risk factor for graft loss. 15 Studies should explore gender-specific factors associated with gender adherence to appointment keeping.
Other important health-related behaviors pertain to the use of substances, such as alcohol. Even though an alcohol use disorder pretransplant is a contraindication, a meta-analysis including liver, kidney and heart studies calculated an alcohol relapse rate after transplant of 5.6 cases per 100 patients per year. 37 A previous BRIGHT study report found an overall heavy alcohol use after heart transplant of 22.9%. 19 Our data showed higher female adherence to alcohol use recommendations globally and in Europe, however multivariable calculations controlling for confounders did not support these findings. According to the World Health Organization per capita in the general population alcohol consumption was almost four times higher in males compared to females and the largest consumption was in Europe with the lowest consumption in the eastern Mediterranean and low-income countries. 21
Tobacco smoke exposure before and after transplantation increases cardiac allograft rejection, vascular inflammation and graft loss, and despite contraindication in solid-organ transplant, 11% to 40% of all heart transplant recipients resume smoking after solid organ-transplant with the odds being higher in males (OR = 1.33) and in those with hypertension (OR = 1.16). 12 In our data, females were more adherent than males to not smoking overall and in Europe.
Our data also shows that females are more adherent than males overall and in Europe to combined alcohol use and smoking recommendations. Health studies confirm that males participate in risky behaviors at a greater rate than females, however, the gender gap in alcohol use and smoking has been narrowing in the latter part of the 20th century as the result of declining male consumption and increasing female consumption of both. 23 Studies addressing gender-specific prevention and intervention of alcohol use and smoking post-heart transplant are needed to improve survival.
Taking these gender-specific behavioral phenotypes into consideration, our findings point towards a need for gender-specific preventive and restorative behavioral interventions in transplant management. Gender has been understudied in transplantation, and a call for more studies exploring these themes has been recently made by the transplant´s scientific community. 38 Our study contributes to addressing this literature shortage.
Strengths and Limitations
Study limitations include the use of self-report questionnaires. Recruitment and data collection were done during routine clinic visits skewing the data due to adherence focus. The study was cross-sectional supplying data at only one point in time. Body Mass Index information was not collected, which may have added significance when weighting the data for variables. The requirements for participation in the study limited the cohort to between 1- and 5- years post-heart transplant and was reported as any average, which could not account for changes in adherence with distance from the transplant surgery. Our dataset was predominantly male. The lower female transplant rates may have biased the female sample with the inclusion of more adherent patients.
Strengths of this study included the large international sample. The random sampling, clear adherence measures and weighting of the data provided this study with an accurate initial representation of gender differences in adherence. This was a good first step in addressing the gender adherence differences to nonpharmacological health-related post-heart transplant.
Future Research
There are potential implications for future research that can be drawn from the findings regarding gender gaps in nonpharmacological health-related behaviors, which add to the risk of morbidity and mortality posttransplantation.
Questions for future consideration in heart transplant research in adherence to: (1) sun protection intervention include “What are the gender sun protection behaviors in North America and in South America?”; (2) diet, include: “What diets might best support gender healthy eating habits?”; (3) sufficient physical activity, include: “What barriers contribute to femalés lower physical activity adherence at the continent level?”; (4) appointment keeping, include: “What factors might positively influence gender appointment keeping behaviors?”; (5) alcohol use, include: “What gender differences in alcohol use may be observed at the continent level ?”; (6) not smoking include: “What interventions may improve male smoking cessation globally and in Europe?”
Conclusions
Our findings provide strong evidence of international variation in gender health-related behavior post-heart transplant. Globally females were more adherent to sun protection and to not smoking, while males were more adherent to sufficient physical activity. At the continent level, females were more adherent to sun protection in Europe and Australia, and not smoking in Europe, while males were more adherent to sufficient physical activity at all continents. Our findings provide specific information to inform future research and clinical practice. Future studies should focus on further understanding health-related gender-specific behaviors and to develop interventions that could close the existing gaps in post-heart transplant gender adherence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the International Society for Heart and Lung Transplants (2008), Schweizerische Akademie der Medizinischen Wissenschaften (2013), ClinicalTrials.gov, International Transplant Nurses Society, European Union Regional Development Fund, Astellas Pharma (National Institute of Health (grant number: NCT01608477).