
Abstract
For patients with a left ventricular assist device (LVAD) as a bridge to transplant, receiving mental health treatment, particularly inpatient treatment, can be challenging due to their complex medical needs. Unfortunately, patients with LVADs have higher rates of depression, anxiety, and suicidality than the general population, making this restricted access to care more problematic. Limited access to full spectrum mental health treatment may negatively impact patients’ transplant psychosocial candidacy for transplant. In this article, we present a successful case of arranging inpatient psychiatric treatment for a patient with an LVAD on a medical inpatient unit through a collaborative approach that spans multiple services and programs. This article details the strategic interprofessional process involved in devising the plan that allowed for treatment and successful discharge.
Keywords
Introduction
Untreated severe psychiatric illness is commonly considered a contraindication for transplant due to concerns for posttransplant poor treatment adherence and self-care.1–3 Severe psychiatric illnesses such as depression with suicidal ideation can require inpatient psychiatric treatment, which would be crucial to optimizing a potential candidate's psychiatric readiness for transplant. Unfortunately, patients with left ventricular assist devices (LVADs) used as a bridge to transplant encounter barriers to inpatient psychiatric treatment when needed due to their medical complexity. 4 This is challenging since patients with LVADs have higher rates of depression, anxiety and suicide rates than the general population. 5 This article expands upon a case report 6 that supported the feasibility of admitting a patient with an LVAD to inpatient psychiatry. In the following sections, we detail the process of an interprofessional transition plan from inpatient cardiology to inpatient psychiatry based on our patient care experience, as a blueprint for arranging for inpatient psychiatric admission for this patient population at a tertiary academic hospital.
Clinical Relevancy to Practice
Severe, untreated mental illness can pose serious threats to the physical health of transplant recipients. Transplant recipients must adhere to a rigorous, complex medical regimen to maintain their new organ and poorly managed mental illness can impact a recipient's ability to keep to the regimen. For example, psychosis, which warps an individual's sense of reality, can lead to mismanagement of medications and post-operative wound care. Depression may result in social withdrawal, poor self-care, and reduced participation in rehabilitation. Severe depression with suicidal thoughts could result in completed suicide resulting in loss of the recipient's life along with a transplanted organ. Untreated substance use disorder can result in similar complications as well as direct physiological harm to a transplanted organ. As such, well-managed mental illness can not only mitigate psychiatric symptoms, but can both reduce psychosocial barriers to transplantation in patients with LVADs implanted as a bridge-to-transplant and improve the likelihood of success of organ transplant. While patients with active medical illness generally face barriers to inpatient psychiatric treatment, it has been nearly impossible for patients with LVADs due to their complex needs. However, there are potential solutions to the specific barriers.
Practice Issues
The following was a process that guided psychiatric hospitalization at an academic medical center of a 60-year-old man with an LVAD implanted 2.5 years previously, who developed symptoms of major depression and suicidal ideation. The patient provided written permission to share this information. This occurred in the context of multiple psychosocial stressors, including a parent with whom the patient lived and who developed terminal illness, very strained family relationships, a break-up with a significant other, and increased alcohol use. His cardiac status was stable. The patient was in care with an outpatient mental health therapist, who urged psychiatric hospitalization for the suicidal ideation. However, the patient's local hospital could not accommodate that because of the LVAD. This highlights a common obstacle - psychiatric inpatient units lacking preparedness and resources to manage the medical needs of patients with LVADs.
Subsequently, the patient was transported to this medical center where the LVAD had been implanted and followed. For expediency and safety, the patient was admitted to the inpatient cardiology service - a psychiatric hospitalization of such a patient had not previously occurred at this center. The transplant psychiatrist evaluated the patient and identified the need for psychiatric hospitalization due to severe depression and suicidality. Because the medical center housed inpatient psychiatry services, this was an innovative opportunity to coordinate cardiac and psychiatric treatments, and provide the necessary and more comprehensive patient and family-centered care.
Necessary Early Steps
Garnering Support
This was a key early step and involved discussions with directors in the cardiac services including the LVAD service, psychiatry services, and psychiatric nursing leadership. The transplant psychiatrist, a member of the consultation-liaison psychiatry team, was in a unique and invaluable position due to established relationships with both Cardiology and Psychiatry. The transplant psychiatrist initiated these efforts, highlighting the needs of the patient, the value of collaboration, and an opportunity for an innovative approach for this and future such patients.
Training the Psychiatric Treatment Team
Once administrative support for hospitalization was obtained, there was discussion with leadership of the various psychiatric inpatient units, about which inpatient unit might be best. The geriatric psychiatry unit was chosen, because many team members had medical in addition to psychiatric experience. Unit leadership, providers and staff were supportive of the opportunity. Concomitantly, the transplant psychiatrist inquired if the LVAD team could both train inpatient psychiatric staff and monitor the patient on the unit. Because the LVAD team had experience in training others (ie local emergency services), this proved no barrier.
The LVAD team established training sessions for psychiatry unit nursing, tech support staff, and the medical providers nested in psychiatric units. The training totaled 6 h and was given to staff members across shifts. It included topics on LVAD management guidelines, preparation for LVAD and cardiac emergencies, and coverage for routine and after-hours LVAD care. There was a concise overview provided for the psychiatric social workers. A reference binder was prepared and kept on the psychiatric unit.
Addressing the Uneasiness of the Psychiatric Inpatient Team
Two important elements included establishing commitment for ongoing involvement of the LVAD team and designing a template for collaboration between LVAD and Psychiatry teams. Face-to-face meetings between the teams commenced with clarification of team member roles/responsibilities, and methods of ongoing communication. This information was compiled in the reference binder, including which team members to call for which issues and a list of contact information. The inpatient nurse managers and the social workers in cardiology and psychiatry coordinated their roles and collaborated throughout the hospitalization. The transplant psychiatrist collaborated with the inpatient team as they managed the psychiatric illness in this medically complex patient. Table 1 outlines the areas of learning.
A Summary of Training Provided and Received by Psychiatric and Cardiac Staff.
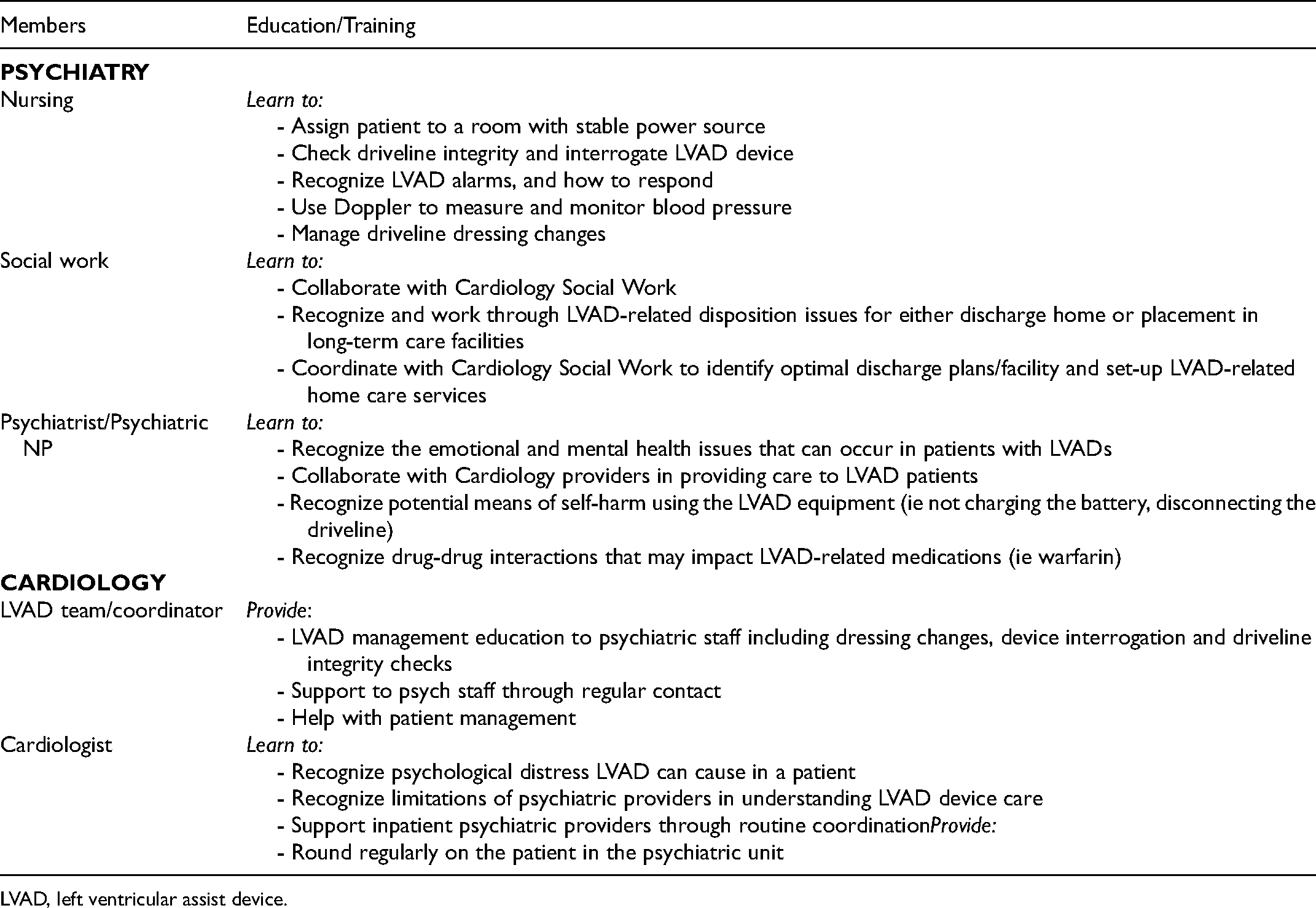
LVAD, left ventricular assist device.
Arranging the Inpatient Environment
The patient's room was arranged across from the nursing station for close observation. Additionally, it was necessary to ensure an uninterrupted electricity source for the LVAD, a necessity in the event of a power outage.
The Psychiatric Admission/Discharge
Preparations for psychiatric admission were completed in 10 days, while the patient remained on the cardiology unit with 1:1 supervision and care by the transplant psychiatrist. Psychiatry and LVAD providers met face-to-face to enact the admission. After admission, the LVAD coordinator came to the psychiatry unit 3 times weekly to assess the patient, provide staff support, answer questions, and supervise the psychiatric nurses on dressing changes and LVAD interrogation. The patient's suicidal ideation, depression, and increased alcohol use were treated through therapeutic discussions, mindfulness training and medication management. The psychiatric team addressed the complex social circumstances including family dysfunction deeply rooted in a history of neglect and physical abuse that contributed to the siblings having little consideration for each other, in turn leading to limited patient support. As family members were supported by the team, they began calling and visiting the patient. The social workers in cardiology and psychiatry collaborated on transportation and housing issues for this patient, whose house had been sold by the siblings during the admission. A suitable senior living facility was arranged; the LVAD team provided training to that facility and to emergency service providers in that locale. An outpatient follow-up plan was arranged, including coordinated cardiology and psychiatry care. There were no LVAD alarms or emergent issues. Figure 1 overviews the timeline of patient care.
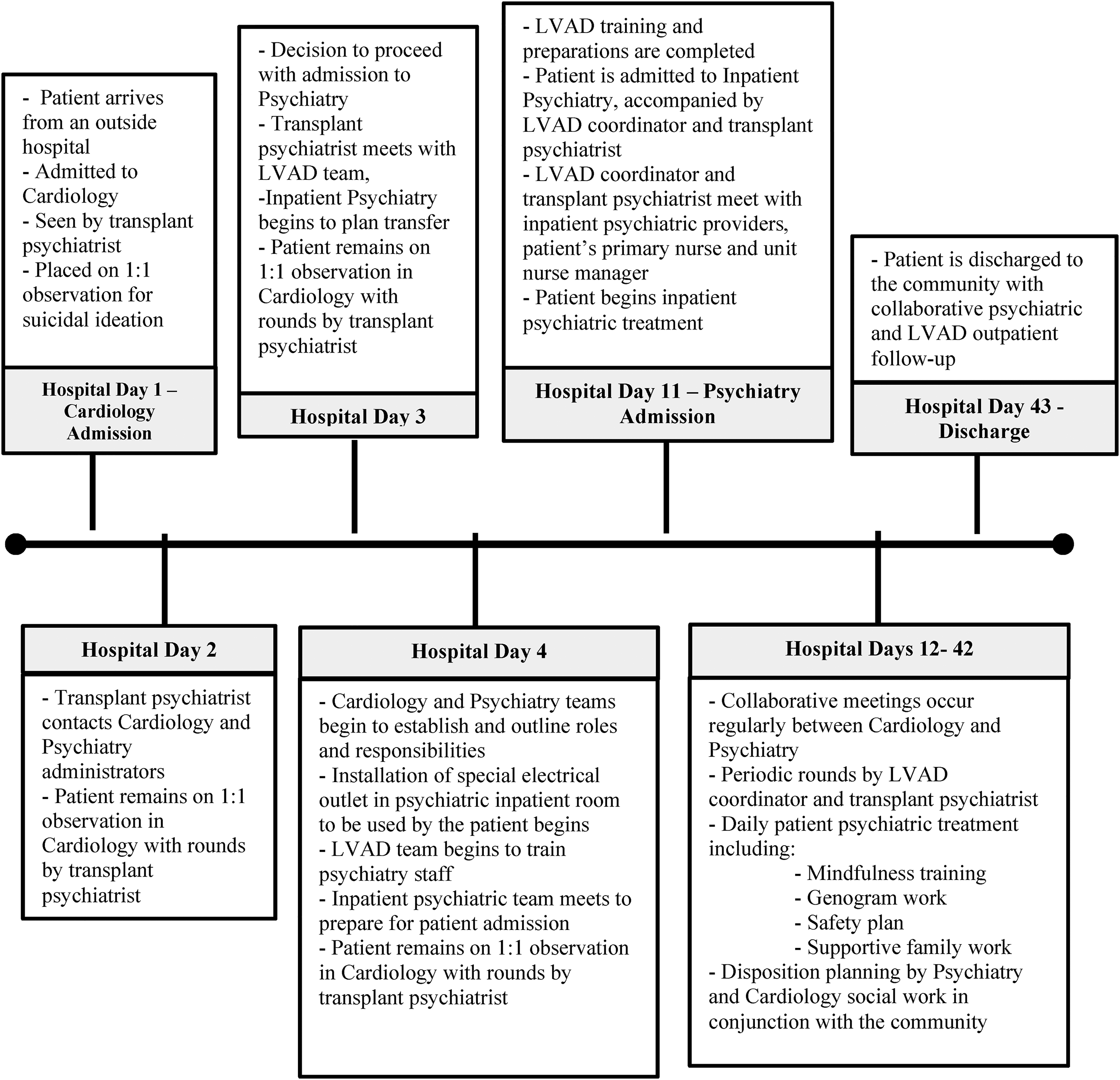
A timeline of patient care on cardiology and psychiatry units. LVAD = left ventricular assist device.
The care teams interacted regularly and often during the hospitalization, both about patient care and how the process was working. There were no suggestions for major improvements to the process flow; no need was perceived for debriefing after discharge. The inpatient psychiatry team highlighted the significant value of ongoing LVAD team involvement. They felt proud of their ability to have treated this patient.
Summary
Patients with LVADs suffer from a high prevalence of mental illness. While it is worthwhile to bolster the psychiatric care of patients with LVADs on medial units, 7 as in this case psychiatric hospitalization will be necessary at times. It is important to prepare for this occurrence and the inherent challenges, as failure to manage severe mental illness in these patients may result not only in undertreatment but also in loss of opportunity to pursue future transplant. This article highlighted an innovative interdisciplinary and inter-specialty approach to such care. It was pivotal to first garner conceptual, administrative and operational support. Once established, it was necessary to secure buy-in from the LVAD team for training and ongoing clinical support of psychiatric providers. It was important to address psychiatric team concerns through meetings and ongoing interdisciplinary and inter-specialty contacts. Clear delineation of team member roles and establishing parameters for ongoing communication between the teams was invaluable. In this case, the process was facilitated by the transplant psychiatrist by virtue of having credible connections with team members of both specialties. We encourage psychiatric and cardiac providers who care for such patients to proactively prepare, through use of these strategies, for the eventual psychiatric hospitalizations of patients with such complex biopsychosocial issues.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.