
Abstract
Introduction
Liver transplantation is the most reliable treatment strategy for hepatocellular carcinoma (HCC) within certain selected criteria. 1 Patients with HCC may not have access to liver donation at the appropriate time and this may result in fall out from the transplant list. To avoid this, bridging therapy has been recommended for patients with HCC to prevent progression of the tumor and to ensure that patients remain within the criteria of transplantation when the organ finally becomes available. Transcatheter arterial chemoembolization (TACE) is a commonly used bridging therapy in patients with HCC awaiting transplantation. 2
Presenting Concern
Our patient was a 64-year-old man who was been managed for cryptogenic cirrhosis. Consent was obtained from the patient before submission of this report for publication.
Routine follow-up revealed 4.6 cm single nodule in the liver. A decision to proceed to liver transplantation was taken but there was no donor at the time so it was decided to use TACE as a bridging therapy. He received 2 cycles of TACE with full response. The TACE was complicated by liver abscess that was drained with percutaneous catheter drainage.
Clinical Findings
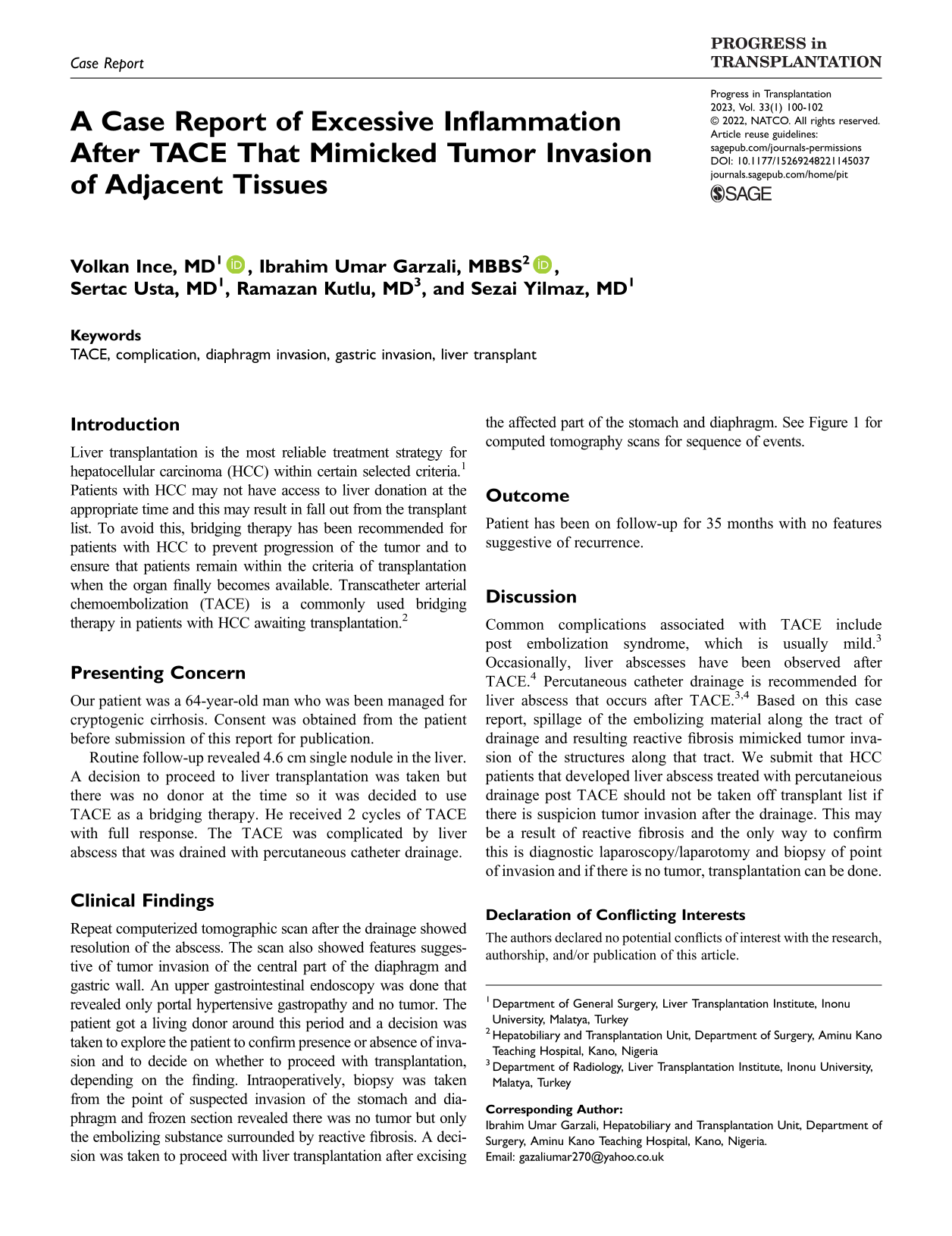
Repeat computerized tomographic scan after the drainage showed resolution of the abscess. The scan also showed features suggestive of tumor invasion of the central part of the diaphragm and gastric wall. An upper gastrointestinal endoscopy was done that revealed only portal hypertensive gastropathy and no tumor. The patient got a living donor around this period and a decision was taken to explore the patient to confirm presence or absence of invasion and to decide on whether to proceed with transplantation, depending on the finding. Intraoperatively, biopsy was taken from the point of suspected invasion of the stomach and diaphragm and frozen section revealed there was no tumor but only the embolizing substance surrounded by reactive fibrosis. A decision was taken to proceed with liver transplantation after excising the affected part of the stomach and diaphragm. See Figure 1 for computed tomography scans for sequence of events.
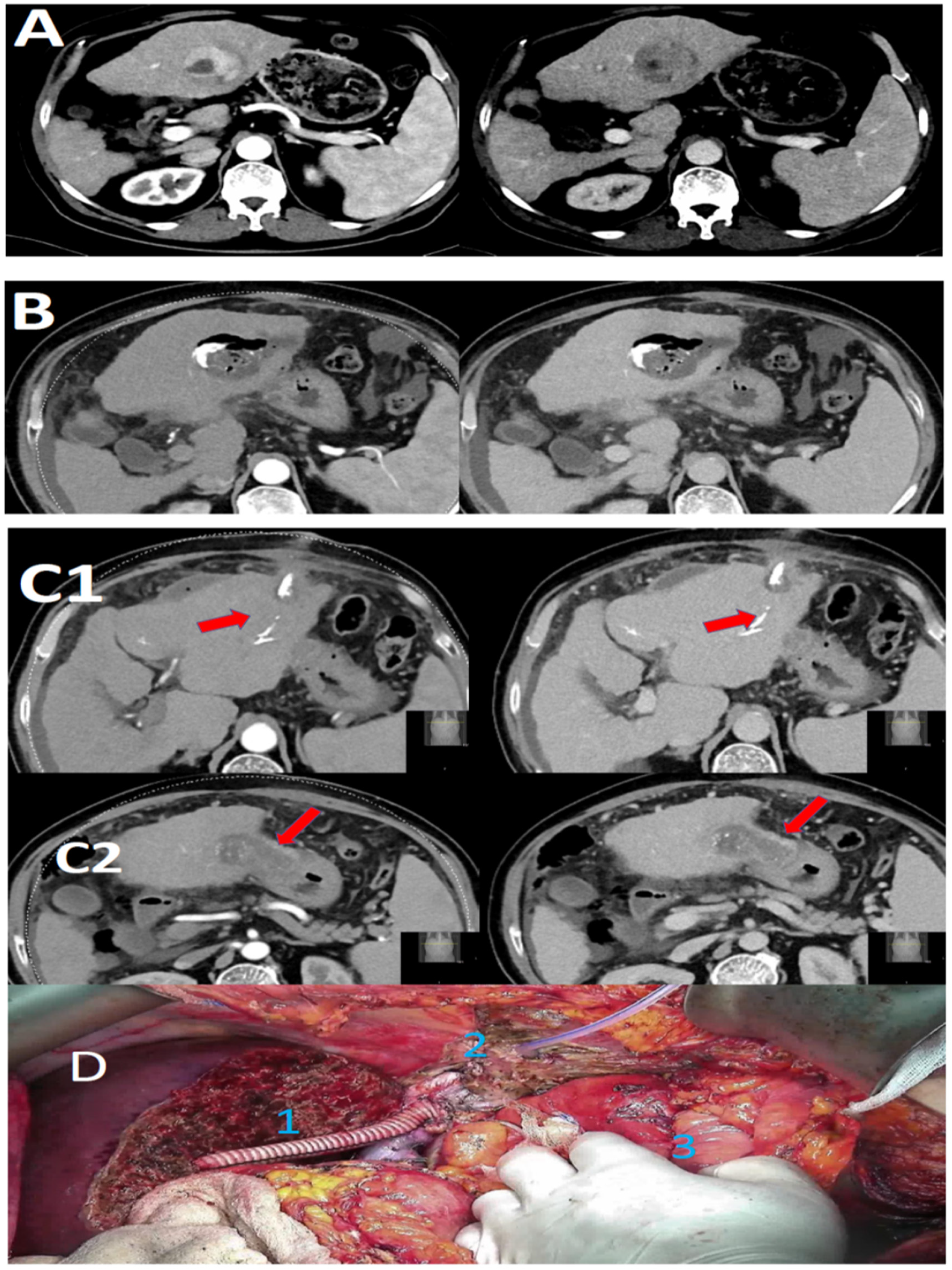
Diagnostic and intraoperative findings. (A) Computed tomography scan showing a single nodule 4.6 cm in size free from the stomach and diaphragm showing no invasion of gastric or diaphragmatic invasion. (B) Computed tomography scan findings of hepatic abscess 6 months after the first cycle of TACE. (C) Computed tomography scan after 8 months of TACE: Abscess has been treated. C1 shows suspected diaphragmatic invasion along the percutaneous tract. C2 shows suspected gastric invasion. (D) Intraoperative image after liver transplantation (1) and excision of affected part of diaphragm (2) and stomach (3).
Outcome
Patient has been on follow-up for 35 months with no features suggestive of recurrence.
Discussion
Common complications associated with TACE include post embolization syndrome, which is usually mild. 3 Occasionally, liver abscesses have been observed after TACE. 4 Percutaneous catheter drainage is recommended for liver abscess that occurs after TACE.3,4 Based on this case report, spillage of the embolizing material along the tract of drainage and resulting reactive fibrosis mimicked tumor invasion of the structures along that tract. We submit that HCC patients that developed liver abscess treated with percutaneious drainage post TACE should not be taken off transplant list if there is suspicion tumor invasion after the drainage. This may be a result of reactive fibrosis and the only way to confirm this is diagnostic laparoscopy/laparotomy and biopsy of point of invasion and if there is no tumor, transplantation can be done.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.