
Abstract
Keywords
Introduction
While survival rates after receiving an organ transplant continue to improve for pediatric patients, concerns remain with rates of organ rejection and hospitalization for these patients.1–3 Medication nonadherence is one of the most significant predictors of late acute rejection, number and frequency of hospitalizations, and even mortality.1,2 The challenges with and consequences of medication nonadherence experienced by adolescent transplant patients are well-documented.2,3 Individual studies have reported nonadherence among adolescent transplant recipients as high as 40% to 60%.2,4
Researchers and healthcare providers have increasingly called for greater use of technology and improvement in mHealth approaches with pediatric transplant patients.5,6 Metaanalyses addressing efforts to promote adherence in pediatric care have emphasized the need to tailor intervention efforts to the patient, improve patient engagement, provide interpersonal support, and address multiple identified barriers to adherence.7–10 Critical features facilitate real-time monitoring and observation of medication-taking behavior and include tools for improving patients’ organizational skills, planning, and conscientiousness around the behavior.10,11
Despite the potential of mHealth adherence interventions, low patient engagement continues to be a significant challenge.8,9,12 Engagement is a multidimensional concept including behaviors synonymous with system usage as well as psychological processes such as perceived depth of involvement in the behavior change process. 13 Short et al 14 emphasized microlevel engagement (ie, use of system features and level of user interest and attention when completing activities) as important as macrolevel engagement (ie, motivation for changing behavior) in improving the ability of mHealth interventions to promote behavioral changes. Baysari and Westbrook 15 underlined that mHealth apps must support patients’ active involvement in the coordination of their care. mHealth apps that provide 2-way communication features can improve patients’ reflective motivation, psychological capability, and social opportunities and are, thus, more likely to improve patients’ intentionality to adhere to their regimens. 16
A mobile health application developed by Scene Health Inc. embodies these system requirements to support medication adherence by facilitating an asynchronous mobile video directly observed therapy intervention. 17 This mHealth app also allows patients to record and submit dose-by-dose videos of themselves completing treatment administration at home (eg, taking immunosuppressant medication). Videos are reviewed and approved by a healthcare professional (eg, transplant nurse) through a centralized platform asynchronously. Patients can review and track their progress over time, report any symptoms of illness or side effects, message the reviewing nurse, or communicate with their transplant team. Study staff and nurses can use the app to contact patients, caregivers, and the patient's transplant care team with concerns. The app includes features to support a higher level of engagement via 2-way communication features that, in turn, can improve patient participation in her/his care coordination, and increase their self-efficacy with their treatment regimen.
The directly observed mHealth intervention was successfully implemented and piloted with adolescent heart transplant patients from a children's hospital in the southeastern United States, wherein patients and their caregivers reported high levels of intervention acceptability18,19 Ten adolescent transplant recipients recruited from a large pediatric heart transplant program received the mHealth intervention with 8 completing the 12-week protocol. Specifically, the study involved adolescent heart transplant recipients who exhibited poor medication adherence. The current study was a secondary qualitative analysis that sought to explore the nature and degree of interactions between adolescent heart transplant recipients and nursing staff during the intervention.
Methods
Design
The study was a content analysis of adolescent heart transplant recipients’ and nursing staff's engagement during the prospective, single-group pilot of the 12-week asynchronous directly observed mHealth intervention. 19 The University Institutional Review Board reviewed and approved the study (Study #IRB202000695).
Setting
The study took place in a large pediatric heart transplant program in the southeastern United States. Participants made no research-specific clinic visits during recruitment or enrollment due to concerns with COVID-19 and conducting in-person contact with immunosuppressed patients. All study procedures with patients were accomplished virtually or by telephone. When beginning the intervention and setup of the mobile application, staff from Scene Health Inc. assisted patients with download, installation, and feature demonstration on their mobile devices. Patients and parents completed pre and postintervention interviews including completing measures of key study outcomes. A flow chart detailing the enrollment, training, measurement points, and staff responsibilities during the intervention has been previously published. 18
Sampling
A convenience sampling strategy was used to recruit adolescents ages 11 to 21 years from the transplant clinic that had documented evidence or concern for medication nonadherence during routine, outpatient clinic visits. Recipients who had received a heart transplant more than 6 months prior and were otherwise deemed medically stable by the pediatric transplant team were eligible to participate. Problems with medication adherence were defined as medication level variability index 1 values ≥ 2.0 or by reported concerns by the pediatric transplant care team. Non-English-speaking participants were not included due to the communicative features of the directly observed mHealth app and the availability of only English-speaking nursing staff.
Information Collection
The content, purpose, and context of 894 in-app messages exchanged between 10 patients and reviewing nurses were analyzed using content analysis. 20 The first 2 authors developed a codebook a priori that included initial codes based on the Persuasive Systems Design model and other relevant theories and research. They coded the data independently, selecting up to 3 codes for each text since messages between patients and nurses could contain several sentences and sentiments. The authors used an inductive, iterative process for coding the data and creating additional codes to guide a thematic analysis of the full dataset of 894 in-app messages. Disagreements in coding were resolved through iterative discussions. The percentage of agreement was calculated after the coding period with interrater reliability ranging from 81.5% to 100%.
Data Analysis
After finalizing the coding, thematic patterns in the data were examined using SPSS v27.0 (IBM Corp Armonk, NY). Additionally, descriptive statistics were calculated for the number and frequency of messages and resulting content categories. Tests of association were conducted between message sources and content code (Fisher’s exact test and effect size phi, ϕ) and associations between message content categories and intervention outcomes (Spearman's rho, ρ).
Findings
Ten patients initiated the mobile directly observed therapy (
Patient and Parent Characteristics.
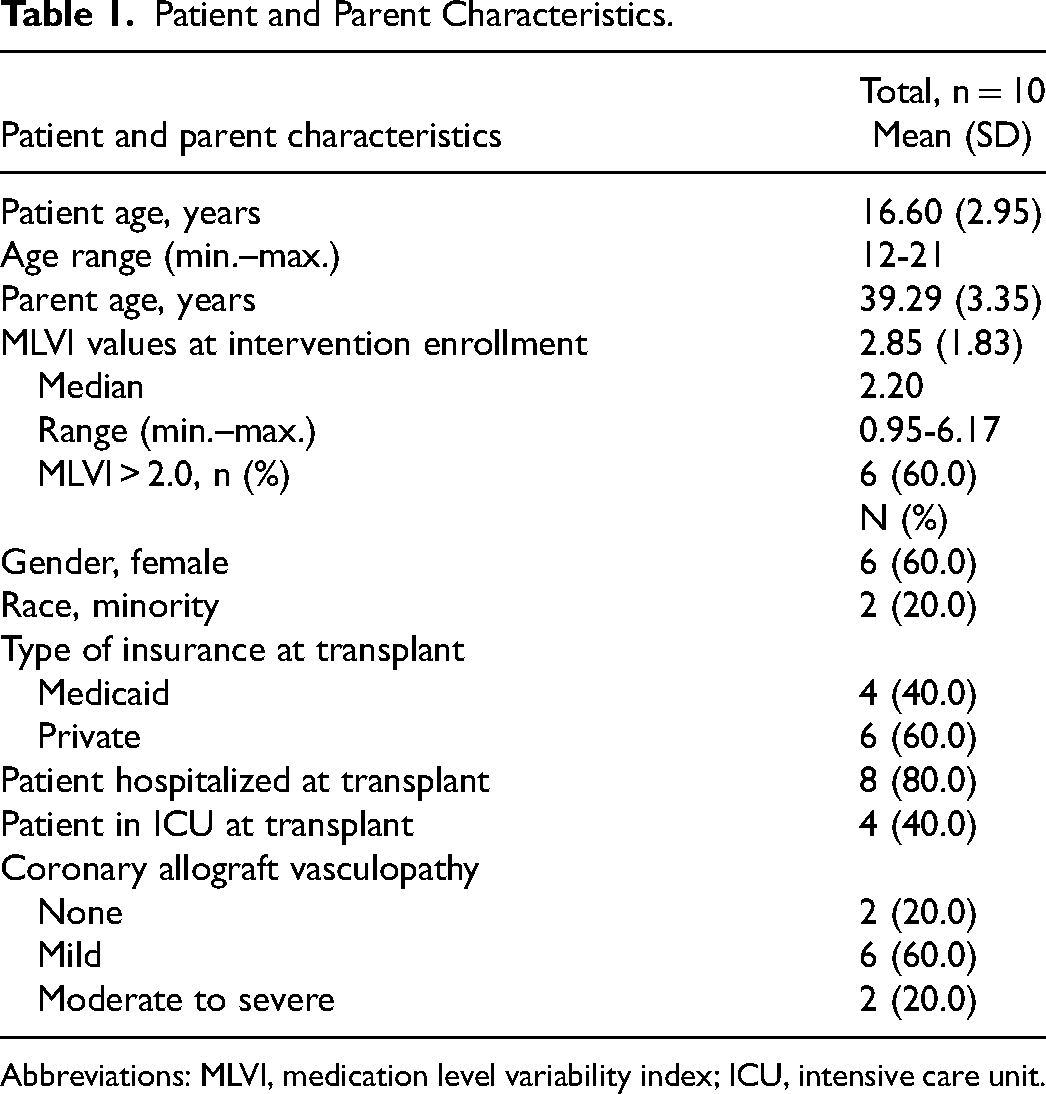
Abbreviations: MLVI, medication level variability index; ICU, intensive care unit.
Interpersonal Engagement via In-App Messaging
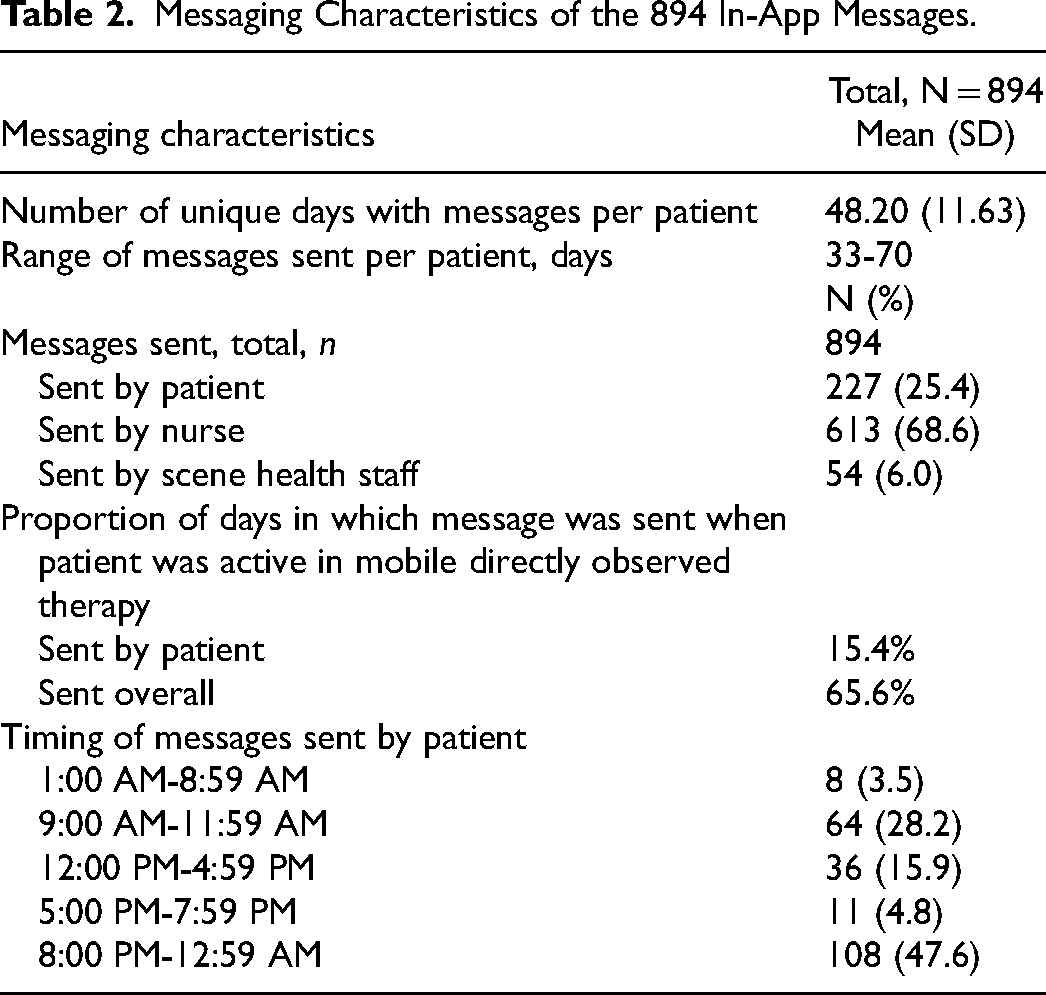
Ten patients and reviewing nurses sent or received 894 unique messages during the 12-week mHealth intervention (see
Messaging Characteristics of the 894 In-App Messages.
Associations between patient characteristics and message codes and frequencies were examined. The total number of messages and the number sent by patients did not significantly correlate with patient age, preintervention medication level variability index, and time since transplant (all P > .05). The number of messages exchanged and those sent by patients did not significantly differ by patient gender, minority status, insurance status at the time of transplant (public vs private medical insurance), and both hospitalization and ICU medical statuses at time of transplant (all P > .05).
Nature and Content of In-App Messages
The content analysis identified 3 broad categories: (1) interpersonal support and rapport-building, (2) medically related questions and information, or (3) supportive information about the mHealth intervention and functional aspects of the Scene Health app. Descriptions of the text exchanges and examples are presented in
Message Content Codes per Category With Examples.
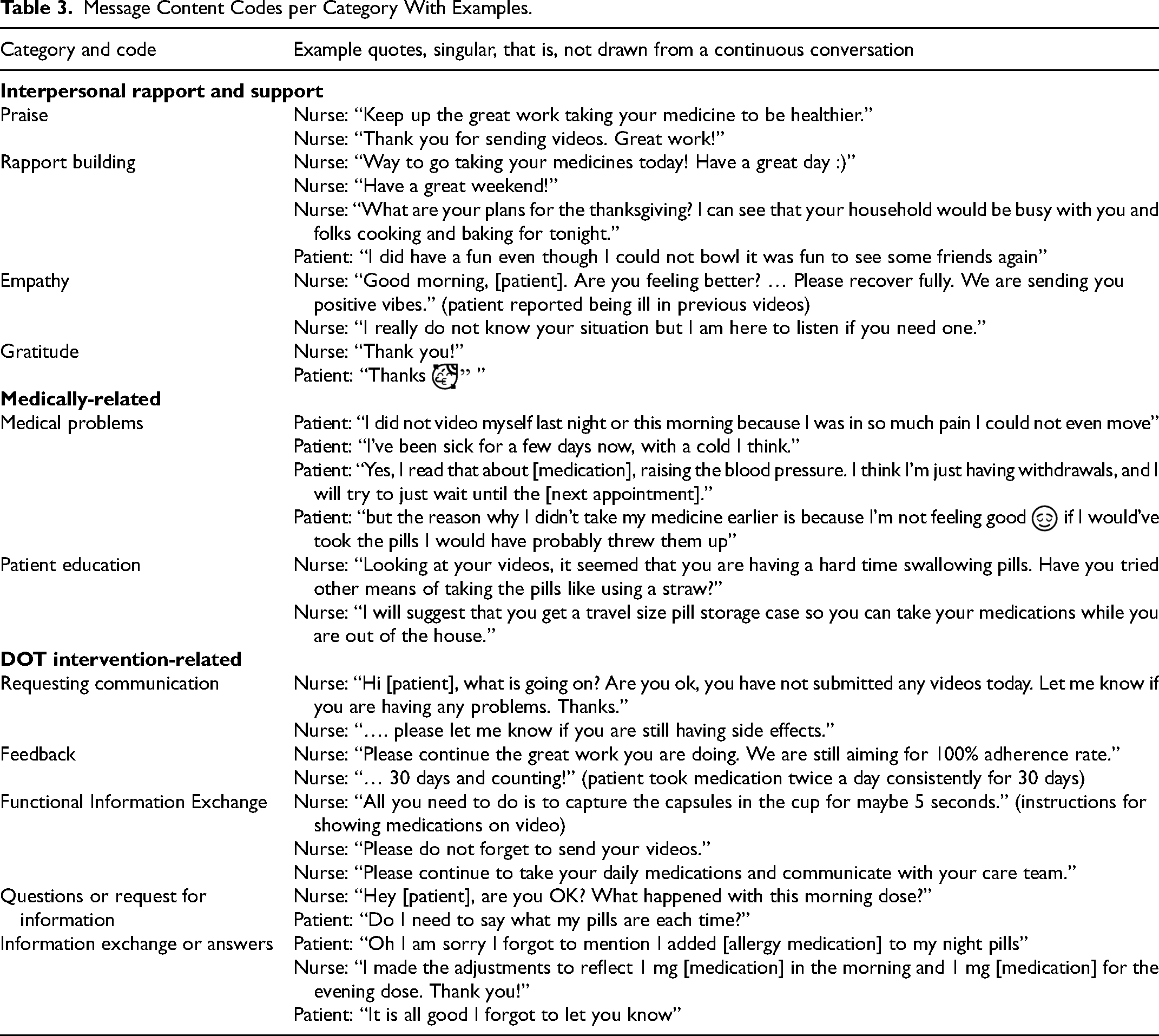
Interpersonal support and rapport-building messages included Praise or complimentary statements for something done well. Rapport Building referred to friendly, medically unrelated messages such as jokes, or stories about family members and plans around holidays and weekends. These also included messages from nurses expressing empathy in response to patients’ sharing personal challenges or medical difficulties. These messages were coded as Empathy. Lastly, simple messages like those acknowledging a prior message or a simple thank you were coded as messages of Gratitude.
Medically related messages referred to the exchange of medical information or nurses’ attempts to promote overall healthy behaviors or increase patient knowledge of their medication condition. Medical Problems were evident in messages containing reporting of symptoms or other medically related patient experiences including side-effects of medications. Nurses also offered information or advice about beneficial health behaviors and ways to reduce specific barriers to medication adherence. Patient Education messages included suggestions that patients monitor when they needed a prescription refill, and consider different medication organization tools or practice methods to reduce ingestion issues when taking medication.
In-app messages were also sent to assist the patients through the mHealth intervention and to provide functional information about the intervention. Requesting Information were messages containing requests for information directly. Feedback included messages acknowledging when patients completed directly observed therapy-related intervention activities. Examples included the nurses telling patients their adherence rate or that a specific medication was seen in the video and counted. Functional Information were messages informing the patient about the intervention process including the use of the app, intervention procedures, and reminders to continue taking the medication and demonstrate this behavior via video. Messages sometimes contained questions about procedures, the app, and the intervention that were coded as Questions. The messages that followed answers to these questions were considered Information Exchange.
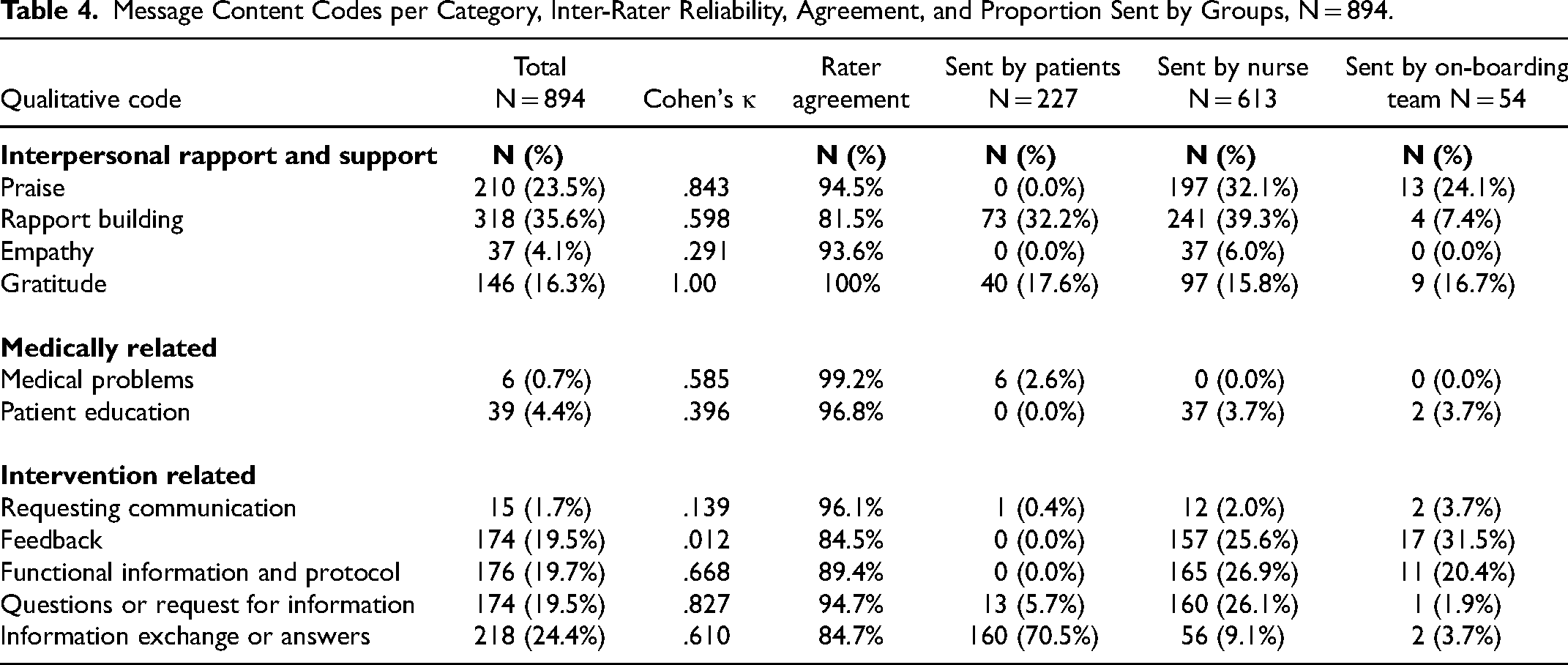
When coding messages, initial interrater reliability was determined through agreement and Cohen's κ (
Message Content Codes per Category, Inter-Rater Reliability, Agreement, and Proportion Sent by Groups, N = 894.
Message Content by Patients and Nursing Staff
The most common themes identified in messages (N = 894) across the patients and nurses were rapport-building (N = 318, 35.6%), praise (N = 210, 23.5%), and information exchange (N = 218, 24.4%). Patients most often sent messages providing answers to questions or information (N = 160, 70.5%), rapport-building messages (N = 73, 32.2%), and messages of gratitude (N = 40, 17.6%). Patients were significantly more likely to send messages about medical problems (P < .001, ϕ = .139), and to provide information (P < .001, ϕ = .632). Importantly, patients and nurses were similarly likely to send messages coded as requesting communication (P = .204, ϕ = .055), expressing gratitude (P = .529, ϕ = .022), and building rapport (P = .065, ϕ = .066).
The nature of messages from nurses (N = 613) were most often related to rapport-building (N = 241, 39.3%), giving praise (N = 197, 32.1%), providing functional information (N = 165, 26.9%), asking questions or requesting information (N = 160, 26.1%), and providing feedback to patients (N = 157, 25.6%). Results from Fisher's exact tests indicated that nurses were significantly more likely to send the following types of messages: praise (P < .001, ϕ = .337), feedback (P < .001, ϕ = .292), education (P < .001, ϕ = .131), functional information (P < .001, ϕ = .301), questions (P <.001, ϕ = .224), and expressions of empathy (P < .001, ϕ = .131).
Mobile Directly Observed Therapy Adherence and In-App Message Content
The proportion of messages containing each coded theme was calculated as patients varied in the number of messages sent and received. Among the 10 patients, the number of escalations per the protocol were significantly associated with the proportion of the messages that were requests for information (ρ = .632, P = .05) and questions (ρ = 855, P = .002). Both types of messages were required by the escalation protocols, including reminders sent to patients when multiple video submissions demonstrating medication taking were not completed. Conversely, greater medication adherence observed during the intervention was associated with greater exchange of praise (ρ = .604, P = .065, moderate effect size although not statistically significant) and gratitude messages (ρ = .728, P = .017). Adherence rates as observed in the videos were also negatively correlated with the proportion of messages related to requests for communication (ρ = −.824, P = .003), functional information (ρ = −.742, P = .014), questions (ρ = −.884, P < .001). Given the very small sample of patients, no other correlations were significant or had only a moderate effect size (ρ < 0.500, P > .10).
Discussion
The content analysis of in-app messages exchanged between patients and nursing staff offers an in-depth and rich exploration of an innovative 2-way communication feature of the intervention and demonstrated the degree to which interpersonal engagement occurred during the intervention, the nature of these exchanges, and its relationship to medication adherence.
This mHealth intervention18,19 was unique because it included features and functionalities that target multiple and modifiable risk factors for nonadherence and promote sustained behavioral change.9,12,21 Previous studies involving mHealth interventions for pediatric transplant patients have mainly focused on the delivery of notifications as reminders to take medications, often in the form of an alarm on a mobile phone or other smart device. 21 These interventions offer limited engagement and produce little to promote health behaviors and medication adherence. Unlike 1-way notification-based interventions that narrowly focus on reminding patients to take their medications, apps that provide 2-way communication can improve patients’ motivations, self-efficacy, and intentionality in adhering to their medication regimens. 16 Previous research has identified difficulties with or anxiety around communication with transplant teams as a possible barrier to medication adherence for adolescent transplant recipients. 22 In line with this, other research has shown that providing patients with a means to communicate with their care team, leads to better perceptions of and better satisfaction with doctor communication, and, consequently, improved adherence. 16 Research has also shown that interventions that facilitate patient–provider communication can enhance patients’ perceptions of collaboration, empathy, and therapeutic alliance and, thus, help strengthen medication adherence. 23
The mobile directly observed therapy mHealth app provides system features that constitute key dimensions in the Persuasive Systems Design model 24 that are critical for improving engagement, and for facilitating behavior change. In addition to primary task and credibility support, the mHealth app includes interactive dialog and social support features that motivate users to engage in and monitor their medication-taking behavior. Combined with direct observation of medication-taking behaviors, in-app messaging facilitated greater patient interaction with transplant care team members, enabled the exchange of more personalized feedback to patients, provided an active path for encouraging positive behaviors, and was possibly key in helping patients improve organizational skills and conscientiousness around their medication. Patients often reported medical problems through the app as they experienced them, indicating a level of comfort in communicating with their medical staff. A significant proportion of the in-app messages contained instances of rapport-building language, praise, and exchanges of medically important information. Nurses often provided praise, and feedback, and asked important questions to patients as prompts for taking their medication.
The volume of and popularity of in-app messaging implies positive perceptions about the 2-way communication and support features of the mHealth app. This finding was further bolstered by the previously reported results of the pilot study 19 that showed patients who completed the 12-week protocol submitted 1211 videos of a possible 1344—demonstrating a 90.1% adherence rate. This adherence rate would have been approximately 82.9% if the videos not submitted by the 2 patients who dropped out from the study prematurely in the third week had been counted.
Limitations in this content analysis, the data, and the overall study should also be considered. Given the purpose of the original pilot study, the sample of patients was small and from a single pediatric transplant center, thus leaving open the possibility of considerable sampling error and lack of generalizability of results. Much communication from the patient to the nurses occurred within videos submitted as evidence of medication adherence, and these were not coded. Many of the messages from the nurses may have been in response to patient communication contained in these videos. There was no control group so comparisons with patients not provided messaging could not be made. The current analysis focused on messaging via the mHealth app and potential causal relationships between in-app messaging and adherence, video submission rates, and patient factors were not examined. Future research should and will include a more robust trial of mobile directly observed therapy that would include a control group to further explore the role of 2-way messaging in adherence outcomes among adolescent heart transplant recipients.
Conclusions
The current study has a number of implications for research on the promotion of adherence health behaviors and engagement of adolescent heart transplant recipients within mHealth interventions. The mobile directly observed therapy intervention and mHealth app included features and functionalities fostering patient engagement and interpersonal support while addressing multiple risk factors for nonadherence potentially improving clinical outcomes. In-app messages and exchanges demonstrated this and the ability of a transplant care team to implement a mHealth intervention that facilitated patient engagement, interaction, and encouragement. To improve scalability, content identified in the messages and exchanges can be used to create a database of predeveloped messages. Medical staff using the provider-facing platform to review patient-submitted videos can respond using prerecorded messages from the patient's own transplant team or other individuals within the patient's social support system. Asynchronous and centralized review can thus reduce providers’ time and effort in engaging and encouraging patient adherence and health behaviors. Continued research and clinical focus on patient engagement and impactful aspects of interpersonal communication could aid in the translation of this intervention into standard clinical care at pediatric transplant centers. Future mixed-methods research should examine specific patient engagement factors and patient perceptions within the mHealth approaches. All these efforts may lead to a positive impact on medication nonadherence especially among high-risk adolescent populations. Overall, this content analysis and exploration of patient engagement in a mHealth intervention provided insights regarding patient engagement and promotion of medication adherence in a sample of high-risk adolescent heart transplant recipients.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Florida State University Office of the Vice President of Research COVID-19 Pandemic Funding.
Declaration of Conflicting of Interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Drs Gupta and Killian serve on the Scientific Advisory Board for Scene Health Inc. The other authors declared no potential conflicts of interest with the research, authorship, and/or publication of this article.