
Abstract
Introduction
Worldwide, the need for organs for transplantation continues to be greater than the number of available organs. 1 According to the latest National Health Service Blood and Transplant United Kingdom report, there are currently over 6000 individuals awaiting an organ transplant. 2 Deceased donors are those who have been confirmed as deceased following brainstem or circulatory death 3 and, with consent from either the individual prior to death, a nominated individual, or a next of kin, have their organs removed for transplantation. 4 Following a survey in England, 80% of individuals were found to be willing to donate their organs after death, 5 yet less than half of this figure had actively registered this decision (opted-in) to the organ donor register (ODR).5,6 To increase the number of donors, there have been legislative changes across Scotland, England, and Wales to one of deemed consent or an opt-out system.7,8 Everyone is now considered an organ donor after death for routine transplants unless they have registered their opt-out decision on the ODR, have verbally expressed their opt-out decision to a nominated individual or next of kin, or meet the country's excluded group criteria. In England, this excludes under 18-year-olds, lack of mental capacity, visitors to or less than 12 months residency in England. 7
There is growing interest in the factors that influence an individual's decision to become an organ donor after death in the UK. Four negative affective attitudes have been consistently cited throughout the literature as significant factors in shaping organ donor intention.9–12 These are (a) bodily integrity: a belief that the body must remain intact; (b) medical mistrust: a belief that doctors will not save the life of someone on the ODR; (c) ick factor: feelings of disgust relating to donating organs; (d) jinx factor: superstitious beliefs such as tempting fate. 10 However, literature concerning the positive aspect of becoming an organ donor appears to be limited. Organ donation is considered to be an altruistic act, and therefore the donor would not necessarily receive any direct benefit or positive impact from donating their organs after death.13,14 Morgan et al., 10 offered an understanding of an individuals’ perceived benefits of becoming an organ donor, finding that when attitudes were phrased in support of organ donation, this strongly predicted that an individual would perceive benefits from being a donor. Cohen and Hoffner 15 further examined perceived benefits, dividing this into other benefits and self-benefits, and measuring this against organ donor intention and affective traits, such as empathy. Interestingly, those perceiving a greater self-benefit had significantly higher intentions to donate than those with perceived other-benefits. When assessing the role of empathy, the participants demonstrating greater empathetic concern as well as perceived greater other benefits were also more likely to donate.
With the recent legislative changes, it is crucial for public health campaigns to raise awareness sensitively, while improving attitudes towards organ donation and intentions to donate. Consideration of both positive and negative factors is therefore important. A recent study 1 found that campaigns with high-threatening language and loss-framing messaging (the losses of an opportunity) decreased intentions whereas emphasising the benefits using gain-framing (the gains of an opportunity) increased intentions. Further research is therefore warranted to assess presentation of the language that should be used in campaigns that are raising awareness of the opt-out system.
The current study aimed: (1) to evaluate how negative affective attitudes and positive statements differed depending on anticipated organ donor status (AODS) under an opt-out system; (2) to evaluate how the order in which negative affective attitudes and positive statements were presented to participants impacted organ donor intention across AODS groups. It is important to note that this study was conducted prior to the legislative changes in England.
Design/Method
Design
The study was quasi-experimental, consisting of a mixed between-within design and was approved by the REDACTED ethics committee (SSSBLRECSTUD2536). Participants were randomised into 1 of 2 conditions via a filter question with an anticipated, approximately even distribution – participants were asked to indicate whether they preferred sweet or savoury foods. This decided the order in which participants received the questions. In condition one (C1), sweet foods, participants were presented with negative affective attitudes first then positive statements. In condition two (C2), savoury foods, participants were presented positive statements first then negative affective attitudes. This was designed to reduce the impact of an order effect. Those who did not provide a response to the filter question were automatically assigned to C1 by the survey software.
As in Miller et al., 12 the independent variable was determined following the participant's response to AODS following a legislative change to an opt-out system with four levels: opt-in, opt-out, not sure, and deemed consent. The three dependent variables (DV) were: negative affective attitudes with four subscales (DV1); positive statements with three subscales (DV2); organ donor intention measured at three intervals – baseline, post-positive statements, and post-negative affective attitudes (DV3).
Setting
All participants consenting to take part followed a link to an online participant information sheet and consent form, once completed, this was followed by the online questionnaire to complete.
Population
A brief description of the England population where the sampling was recruited is described in the limitations using comparisons from the 2019 Census data. 16
Sampling
To be eligible to take part in the study participants needed to currently reside in England and be over the age of 18. No other exclusion criteria were applied. Participants were recruited via two methods. The study was advertised online using the social media accounts of the lead researcher and encouraged sharing of the link to reach as wide a sample as possible across England. Additional participants were recruited using the psychology department research repository of a university in the North-East of England where the research team was based. Students recruited via this method were offered course credits. No other incentives were offered. Participants were recruited via opportunistic sampling from May to June 2019 via online advertisements.
Data Collection
The questionnaire was adapted from previous studies9,12,13 to understand differences in characteristics across donor intention as well as attitudes towards organ donation. This questionnaire consisted of demographics, current organ donor status, organ donor intentions, organ donation and knowledge, AODS, negative affective attitudes, and positive statements.
Demographics
Participants were asked about their age, education level, employment status, religious beliefs, racial group, and England region currently residing in (provided their postcode) as part of the demographic information collected.
Current Organ Donor Status
Participants were asked what their current organ donor status with seven additional questions was relating to personal experience of donation, eg, ‘Have you ever donated an organ?’. Optional responses to these were, Yes, No or, Not sure.
Organ Donor Intention
Participants used a Likert scale to rate whether they strongly disagreed (1) to strongly agreed (7) with, I intend to donate my organs after death. This measured organ donor intention at three intervals for the DV: (1) after current organ donor status (baseline), (2) after negative affective attitudes, and (3) after positive statements.
Organ Donation Knowledge and Anticipated Organ Donor Status
Participants were asked three questions based on knowledge and awareness of organ donation and legislation. Participants were presented with information regarding the legislative change and asked, If the organ donation laws in your country change to an opt-out system, what would your choice be?, with four optional responses: (a) I would opt-in [to the ODR] (I want to be an organ donor); (b) I would opt-out [of the ODR] (I do not want to be an organ donor); (c) I have no objection in donating my organs (deemed consent to be an organ donor); (d) not sure. This would determine the four AODS groups.
Negative Affective Attitudes
The negative affective attitude 11-item scale (with four subscales) was adapted from Miller, et al 12-item scale, 12 with one jinx factor statement removed to increase scale reliability. 12 Participants used a 7-point Likert scale, ranging from 11 to 77, with higher scores indicating greater agreement with the statements. The four subscales were: (a) Bodily integrity: two statements (α = .81), eg, The body should be kept whole for burial. (b) Medical mistrust: four statements (α = .67), eg, If I register as an organ donor, doctors might not try so hard to save my life. (c) Ick factor: three statements (α = .79), eg, The idea of organ donation is somewhat disgusting. (d) Jinx factor: two statements (α = .61), eg, People who donate their organs risk displeasing God or nature.
Positive Statements
The positive statements 11-item scale consisted of three independent factors derived from existing scales.9,13 Participants used a 7-point Likert scale, ranging from 7 to 77, with higher scores indicating greater agreement with the statements. The concepts measured were: (a) Perceived benefits: four statements (α = .73), eg, Organ donation allows something positive to come out of a person's death. (b) Cognitive attitudes: four statements (α = .73), eg, I view organ donation as a benefit to humanity. (c) Altruism: three statements (α = .73), eg, Helping others is one of the most important aspects of life.
Data Analysis
A power analysis using GPower3.1 indicated a sample of 756 would be sufficient in detecting a small effect size using three groups, f = .10, α = .05, power = .80. 17 Therefore, this made three AODS groups for comparisons: opt-in (N = 443); opt-out/not sure (N = 71); deemed consent (n = N = 165).
Analyses were carried out using the statistics program R with the WRS and WRS2 packages for robust estimates.18,19 Descriptives, reliabilities, and non-parametric tests of difference were conducted in SPSS Version 26 (IBM Corp., Armonk, NY).
Negative affective attitudes and positive statements were examined using multiple analysis of variance (MANOVA) using the Choi and Marden 20 method, follow-up analysis of variance (ANOVA), and post-hoc tests. Multiple violations of normality of dependent variables and homogeneity of variance required the use of robust MANOVA 19 and ANOVA. Each ANOVA was conducted using the t1waybt() and mcppb20() functions in WRS2 implementing a 20% trimmed mean with a 2000 sample bootstrap, following recommendations by Field and Wilcox. 21 Post hoc tests were adjusted for multiple comparisons to P < .017. As normality assumptions were violated, a series of Wilcoxon Signed Ranks Tests were conducted across AODS groups.
Procedure
Participants responded to the online advertisements, which provided them with an online link to the participant information sheet and to sign the consent form, confirming their eligibility. Following this, the participants were provided with the online questionnaire, see
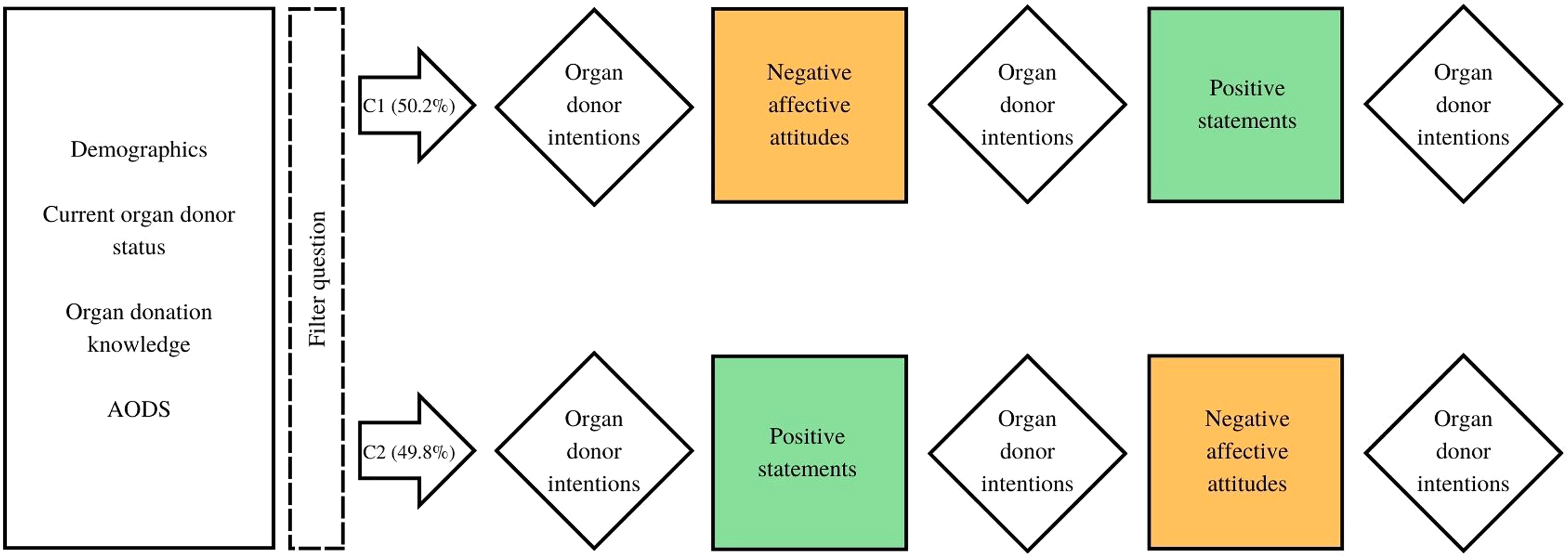
A flow diagram demonstrating the layout of the questionnaire following the filter question.
Results
Demographic Characteristics
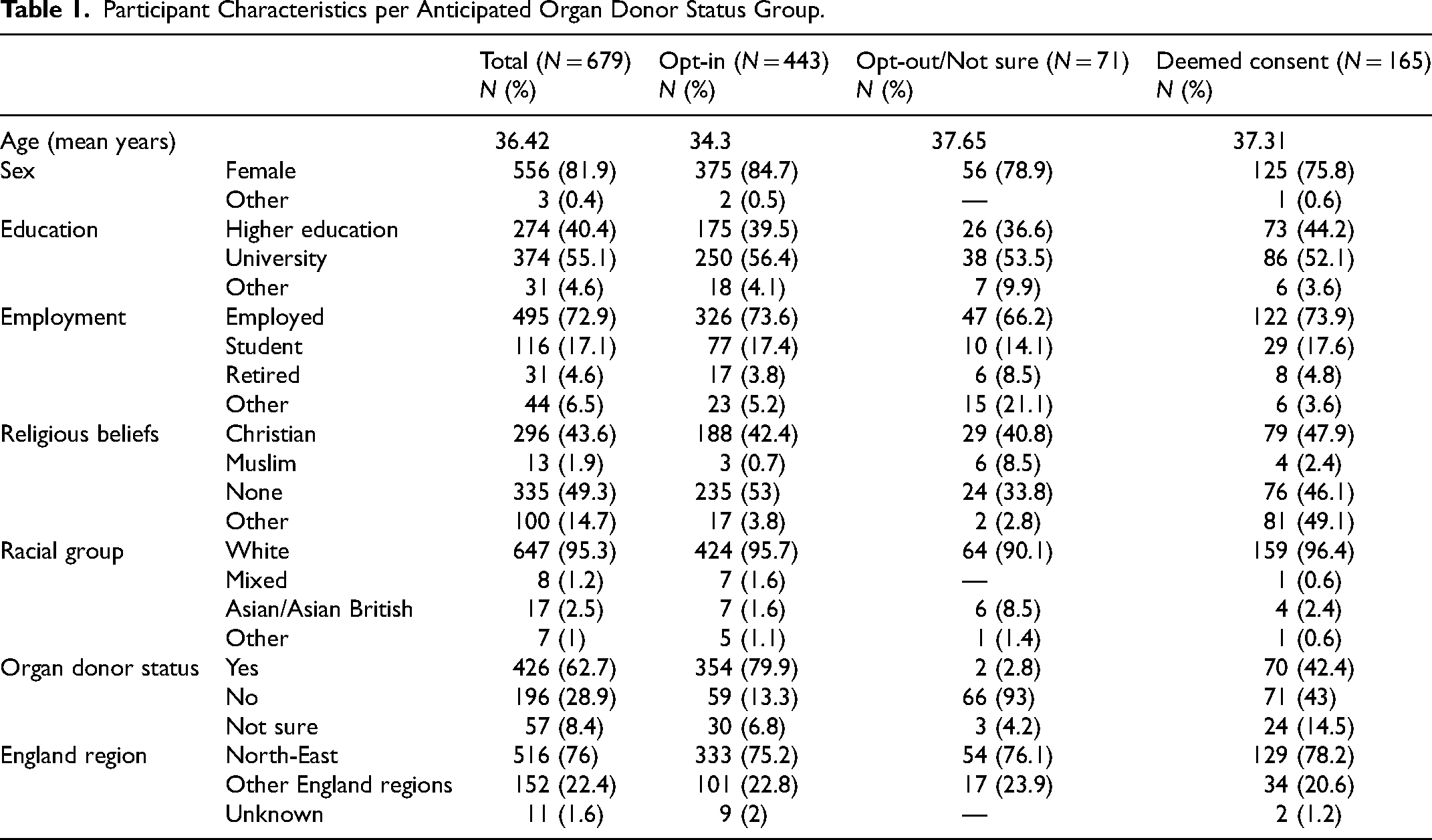
In total, 778 participants responded to the online survey; 99 were excluded due to not meeting the inclusion criteria or incomplete online consent forms. Therefore, 679 participants were included in the final sample, 556 (81.8%) identified as female, 516 (76%) self-reported as residing in the North-East of England and 647 (95.3%) were White.
Participant demographics can be seen in
Participant Characteristics per Anticipated Organ Donor Status Group.
Anticipated Organ Donor Status Groups
There were four responses to AODS, opt-in, opt-out, deemed consent, and not sure. Due to the low number of participant responses to I would opt-out and not sure, this was collapsed into one group, as per Miller et al. 12
Negative Affective Attitudes by Anticipated Organ Donor Status Groups
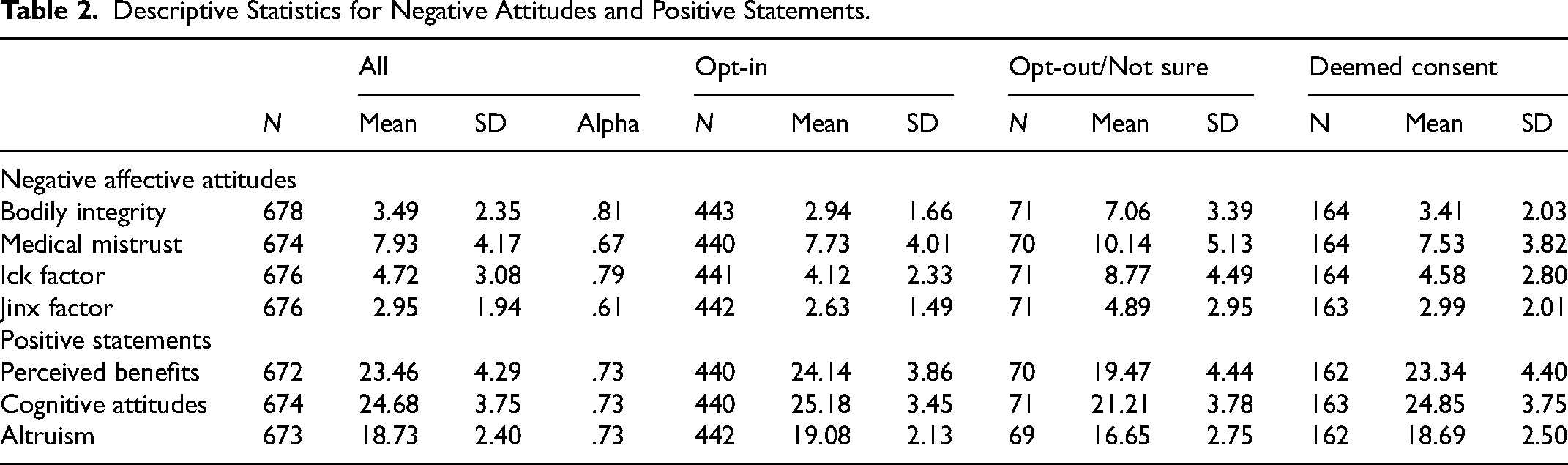
There was a statistically significant main effect of group on negative affective attitudes overall, H (8) = 102.99, P < .001, opt-in (N = 439), opt-out/not sure (N = 70), and deemed consent (N = 163). Additionally, there were statistically significant differences between AODS and mean scores for bodily integrity (Ft(2, 87.47) = 54.176, P < .000; r² = .23), medical mistrust (Ft(2, 99.63) = 7.60, P < .001; r² = .12), ick factor (Ft(2, 85.77) = 31.38, P < .001; r² = .32), and jinx factor (Ft(2, 84.67) = 14.19, P < .001; r² = .21). Post-hoc analysis further revealed statistically significant differences across all AODS group comparisons, for bodily integrity (P < .017) and ick factor (P < .017); opt-in versus opt-out/not sure groups for medical mistrust (=−2.77 [−4.67, −.93]; P < .017) and jinx factor (=−2.51 [−3.78, −1.40]; P < .017); opt-out/not sure versus deemed consent groups for medical mistrust (=−2.95 [.96, .4.96]; P < .017) and jinx factor (=2.36 [1.13, 3.59]: P < .017). All four negative affective attitudes were highest in the opt-out/not sure group compared to opt-in and deemed consent groups, with medical mistrust as the greatest concern across all AODS groups and jinx factor as the least, see
Descriptive Statistics for Negative Attitudes and Positive Statements.
Positive Statements by Anticipated Organ Donor Status Groups
There was a statistically significant main effect of group on positive statements overall, H (6) = 60.39, P < .001, opt-in (N = 436); opt-out/not sure (N = 68); deemed consent (N = 161). Additionally, there was statistically significant differences between AODS and mean scores for perceived benefits (Ft(2, 103.01) = 35.90, P < .001; r² = .10), cognitive attitudes (Ft(2, 105.55) = 45.84, P < .001; r² = .10) and altruism (Ft(2, 95.52) = 25.55, P < .001; r² = .08). Post-hoc analysis further revealed statistically significant differences between opt-in versus opt-out/not sure groups and opt-out/not sure versus deemed consent respectively for perceived benefits (=5.06 [3.67, 6.49] P < .017 and =−4.20 [−5.74, −2.65] P < .017), cognitive attitudes (=4.89 [3.61, 6.17] P < .017 and =−4.56 [−5.88, −3.18] P < .017), and altruism (=2.91 [1.77, 3.97] p < .017 and =−2.51 [−3.58, −1.36] P < .017); no significant differences were found between opt-in versus deemed consent groups. All 3 positive statements were highest in the opt-in group compared to deemed consent and opt-out/not sure groups, with cognitive attitudes as the greatest across all AODS groups and altruism as the least, see
Presentation of Negative Affective Attitudes and Positive Statements on Organ Donor Intentions by Organ Donor Status Groups
For participants assigned to C1, organ donor intentions were measured at baseline, post-negative scale, post-positive scale, whereas for those assigned to C2 organ donor intentions were measured at baseline, post-positive scale, post-negative scale. See
Mean Scores and Standard Deviations of Organ Donor Intentions.
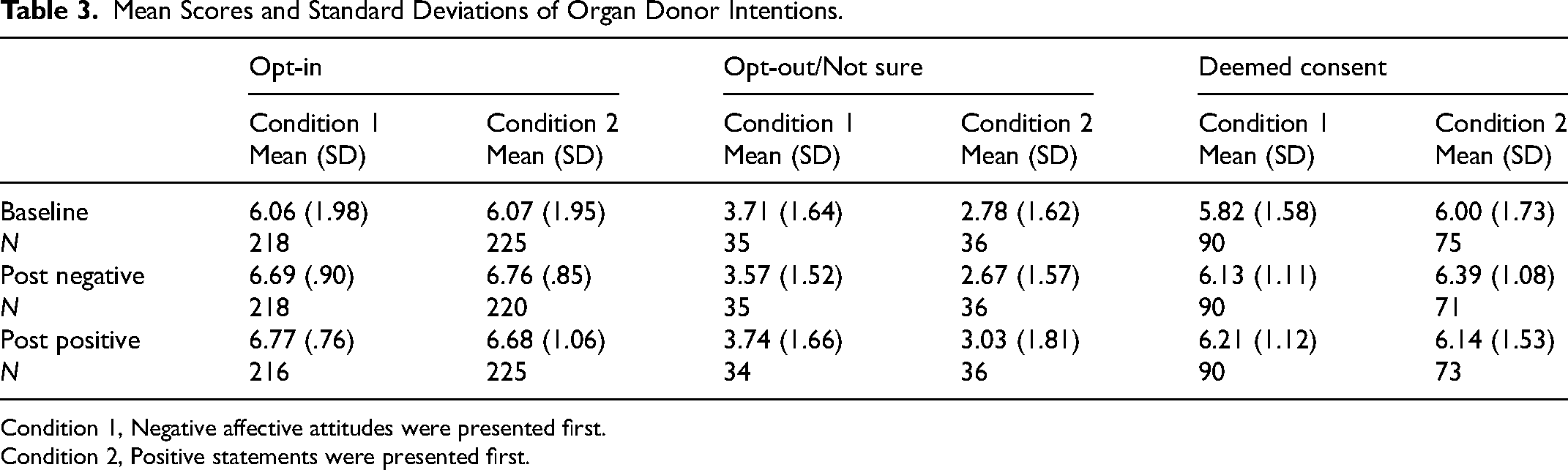
Condition 1, Negative affective attitudes were presented first.
Condition 2, Positive statements were presented first.
Presenting the negative affective attitudes scale first (C1) significantly increased intentions of the opt-in (N = 218), z = −4.17, P < .001, r = .20, and deemed consent groups (N = 90), z = −2.23, P < .05, r = .17, in comparison with baseline. Intentions of the opt-out/not sure group did not significantly change, (N = 35) z = −.910, P = .363, r = .11.
Presenting the positive statements second significantly increased intentions of the opt-in (N = 216), z = −4.76, P < .001, r = .23, and deemed consent groups (N = 90), z = −3.34, P < .05, r = .25, in comparison with baseline. Intentions of the opt-out/not sure group did not significantly change, (N = 34) z = −.322, P = .747, r = .04.
Presenting the positive statements first (C2) significantly increased intentions of the opt-in group (N = 225), z = −4.31, P < .001, r = .19. in comparison with baseline. There was no significant change in intentions of the opt-out/not sure (N = 36), z = −.815, P = .415, r = .10, and deemed consent group (N = 73), z = −.76, P = .446, r = .06, compared with baseline intentions. Presenting the negative affective attitudes scale second significantly increased intentions of the opt-in (N = 220), z = −4.84, P = <.001, r = .23 and deemed consent groups (N = 71), z = −2.24, P = <.05, r = .19, in comparison with baseline. There was no significant effect on intentions within the opt-out/not sure group (N = 36), z = −.579, P = .563, r = .07.
Across the four pairs, there were significant increases in intentions in the opt-in group only, with significant increases in three pairs for the deemed consent group and no significant differences in the opt-out/not sure. Presenting positive statements does improve intentions in the opt-out/not sure group with a detrimental impact on intentions when presented with negative affective attitudes, as seen in
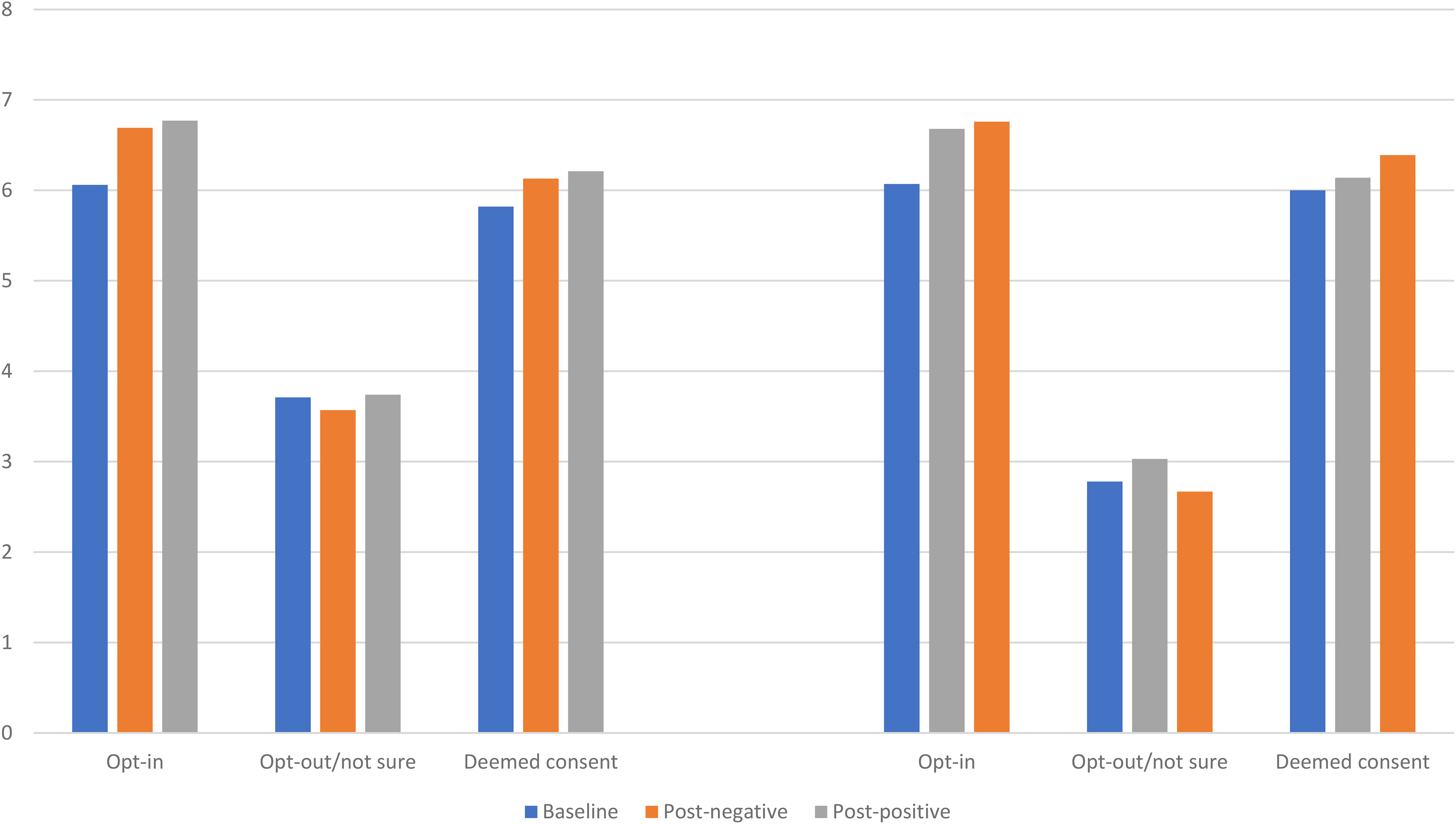
Mean scores of organ donor intentions in condition 1 (left) and condition 2 (right) by anticipated organ donor status.
Discussion
The present study found that 10.46% of participants anticipate opting out of the ODR or were unsure of their decision following implementation of an opt-out system in England, as supported by previous research. 12 Unsurprisingly, this group of participants reported significantly higher levels of negative attitudes, with greater concerns towards bodily integrity, medical mistrust, ick factor, and jinx factor. The greatest concern of participants in this study was medical mistrust, whereas bodily integrity has been previously cited.11,22,23 An increase in medical mistrust, has been recorded in countries that have implemented opt-out systems, leading the Organ Donation Taskforce to fear this occurring in England. 24 Individuals predominantly reported to have a fear of declaration of premature death, despite there being no evidence documenting such practice. 25 Evidence from Wales demonstrated an increase in consent to donate following the change to opt-out consent from 58% in 2015% to 77% in 2019, 26 suggesting this should be replicable in England.
The order of negative affective attitudes and positive statements was manipulated 12 to provoke an effect upon organ donor intentions. Irrespective of the order negative affective attitudes were presented, organ donor intentions in the opt-out/not sure group decreased from baseline. Previous research 1 has suggested that those who plan to opt-out or are unsure of their decision were likely to experience a more heightened emotional response (eg, threat to freedom and anger) to the legislative changes compared with those who plan to actively opt-in or have no objection (deemed consent). It has been further argued that introducing an opt-out system takes away an individual's choice, 8 this belief can contribute to the individual feeling a threat to their freedom. 1 The present study evidenced that less than 10% of individuals may still decide to actively opt-out. Public health campaigns would benefit from emphasising that individuals still have a choice to become an organ donor, this would help to reduce emotional reactance, thus increasing intentions. 1
When presented with positive statements, intentions increased from baseline across all AODS groups in both conditions, despite the lack of significance in some. Those actively opting into the ODR demonstrated greater perceived benefits, cognitive attitudes, and levels of altruism. Given the influence the positive statements had on those who planned to opt-out or were unsure, these statements should be considered by those designing the messaging public health campaigns. Methods such as gain-framing within campaigns can be used to promote the positive impact. 1 Additional support from patient and public representatives in qualitative research highlighted the need to promote the positive impact of receiving a transplant and giving that individual a second opportunity. 27 This described the perceived benefits (self and other) of organ donation as well as suggesting it is an altruistic act that enables individuals to fulfil an innate desire to help others while beholding the potential to promote the same desire across communities. 28 An individual's altruistic behaviour could be further targeted by incorporating reciprocity primes, such as asking individuals if they would accept a donated organ. 14 Altruism, however, would benefit from further research as these results indicated a weak correlation with organ donor intentions.
Most of the limitations within the study derive from the sample. Firstly, it was slightly underpowered due to several exclusions. Secondly, there are certain participant demographic characteristics that were not representative of the population of England, such as the respondents being predominantly female and from the North-East of England. For instance, while 81.8% of the sample were female, compared to 50.9% from the North-East of England, and 50.6% from England as a whole. 16 In addition, 95.3% of the sample were White, compared to 84.3% in the North-East of England, and 94.8% in England. 16 Therefore, while the sample was not representative of sex, it was broadly representative in terms of ethnicity. Evidence suggests that there is a complex relationship between sex and organ donation 29 and that ethnicity and culture are important factors in organ donation 30 Additionally, a considerable proportion of the participants were already registered as an organ donor (opt-in 52.1%; deemed consent 10.3%; opt-out/not sure 0.3%). Generalisability beyond the current sample for these reasons may therefore be limited. Therefore, it has not been possible to draw conclusions on the relationship between participant demographics and AODS. Future research should adopt a purposive sampling approach in order to assess any such relationships.
Conclusions
This study demonstrated the complexity of organ donation attitudes and how they can influence intention to become an organ donor, supporting that content and presentation are important factors to consider when developing public health campaigns. Further exploration of the order organ donation messages, positive or negative, are presented is required given these findings and potential valuable applicability to public health campaigns.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with the research, authorship, and/or publication of this article.