
Abstract

Keywords
Introduction
A 30-year-old woman with type 1 diabetes mellitus underwent pancreas transplantation at the age of 18, during which the donor's pancreas's artery supply was connected the recipient's right common iliac artery, and enteric exocrine drainage was connected to the recipient's jejunum. Her pancreas allograft failed 13 months ago due to chronic rejection. The patient's consent for publication was obtained.
Presenting Concern
Eight months after allograft failure, she experienced a massive lower gastrointestinal (GI) bleeding, and a 1.5-cm pseudoaneurysm from the right common iliac artery near the pancreas allograft (
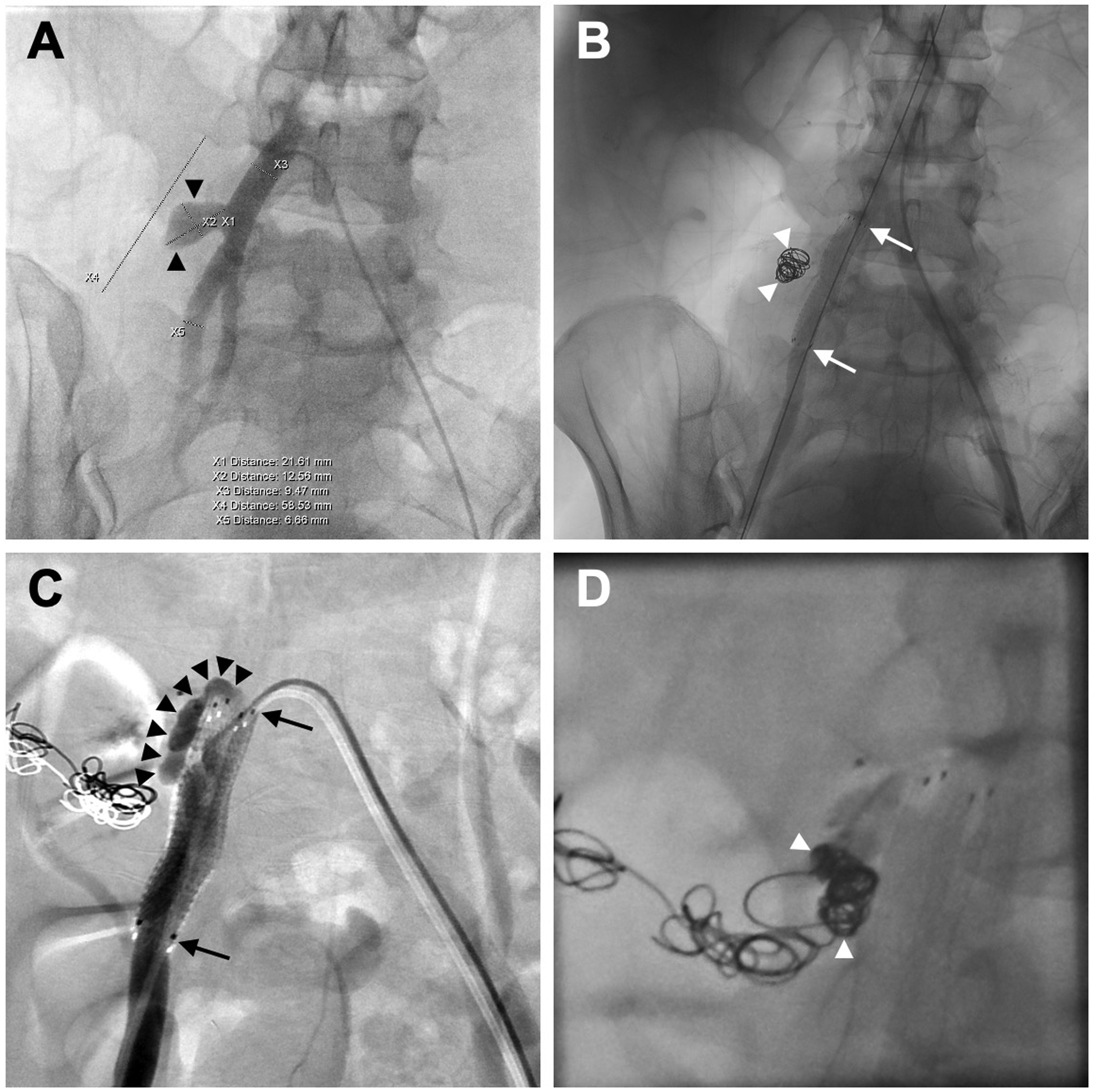
Recurrent bleeding necessitated multiple angiographic interventions of the iliac artery.
Clinical Findings
Emergent angiography revealed extravasation at the right common iliac artery (
Outcome
She underwent exploratory laparotomy, revealing an eroded right common iliac artery, an exposed vascular stent graft, and an eroded jejunum. A transplant pancreatectomy with the removal of a segment of the right common iliac artery along with the vascular stent graft was conducted, followed by a femoral–femoral artery bypass grafting. Postoperatively, she recovered well, and her hemoglobin gradually returned to 11.1 g/dL without any blood transfusion.
Discussion
Pseudoaneurysm and arterio-enteric fistula are uncommon following pancreas transplantation. 1 Despite their infrequency, these conditions account for half of the reported GI bleeding cases. 2 Our patient, with a failed pancreas allograft, experienced ongoing right common iliac artery erosion after vascular stent graft placement, subsequently forming a new arterio-enteric fistula at the upper margin of the vascular stent graft. Given the potential for life-threatening bleeding, the meticulous management of pseudoaneurysm and arterio-enteric fistula was imperative. Traditional surgical interventions, while effective, pose risks such as infection and iatrogenic injury to the allograft or vascular structure. Endovascular interventions, including embolization or stent graft placement, offer alternatives that circumvent major surgery and serve both diagnostic and therapeutic purposes. The decision between surgical or endovascular interventions hinges on the functional status of the allograft. 3 For those with functional pancreas allografts, endovascular intervention is recommended. Embolization demonstrates superior graft function preservation but is associated with a higher incidence of recurrent bleeding.1,3 Conversely, stent graft placement offers enhanced efficacy in halting bleeding, yet it carries the potential to impede the blood supply to the pancreas allograft, resulting in allograft failure or necrosis. 1 Generally, a preference for stent grafts arises because of the risk of life-threatening rebleeding outside the hospital that embolization may bring. For those with failed pancreas allografts, the hemodynamic stability of the patient becomes a critical factor, guiding the choice between transplant pancreatectomy and initial endovascular intervention. 1 Hemodynamically stable patients are recommended to undergo transplant pancreatectomy, whereas those who are hemodynamically unstable are advised to undergo initial endovascular intervention to halt bleeding. 1 Subsequent assessment determines the necessity of further transplant pancreatectomy. Our case was finally managed by a transplant pancreatectomy with stent removal and femoral–femoral bypass. This case report emphasizes that surgical intervention instead of endovascular treatment was likely the ultimate approach for recurrent GI bleeding in patients with a failed pancreas allograft.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported for research purpose by the “Yin Yen-Liang Foundation Development and Construction Plan” of the School of Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan (111Q58502Y, 113Q158505); the National Science and Technology Council, Taiwan (112-2314-B-A49-059-MY3, 112-2811-B-A49A-039, 112-2321-B-A49-020, 112-2634-F-A49-003-3); Taipei Veterans General Hospital, Taiwan (V111D63-003-MY2, V111D60-004-MY3, VGHUST111-G6-7-2); and the “Center for Intelligent Drug Systems and Smart Bio-devices (IDS2B)” from The Featured Areas Research Center Program within the framework of the Higher Education Sprout Project by the Ministry of Education (MOE) in Taiwan.