
Abstract
Introduction
Eliminating racial inequities in access to kidney transplantation requires multilevel interventions that target both patients and health systems.
Research Question
The aim of this study was to determine whether adding culturally sensitive, web-based patient education to a transplant center-level intervention was associated with increased knowledge, motivation to pursue living donor kidney transplant, and confidence in the behavioral skills to discuss living donation among Black/African American patients with end-stage kidney disease.
Design
A total of 411 transplant candidates were randomized to intervention (N = 222) or control groups (N = 189) and completed measures at baseline and immediate follow-up during the transplant evaluation visit.
Results
Results indicated no significant change in knowledge across time or study condition. At immediate follow-up, participants of both study conditions exhibited a significantly higher motivation to pursue living donation (t = 3.066, P < .01) versus at baseline. Both study conditions demonstrated increased confidence in the behavioral skills to discuss living donation over time (t = 3.580, P < .001). Process evaluation findings demonstrated limited engagement with the online video content across both conditions.
Conclusion
Results suggest that the intervention did not perform better than control but raised important considerations for the delivery of transplant education targeting Black/African American patients in a busy clinical setting.
Keywords
Introduction
Chronic kidney disease is a significant cause of morbidity and mortality in the United States that can progress to end-stage kidney disease (ESKD) if left untreated, particularly among patients with hypertension and diabetes. 1 Racial disparities in ESKD are persistent and profound, where Black patients disproportionately account for over 30% of ESKD patients. 2 Where Black patients have an almost 4-fold increase in adjusted incidence of ESKD compared to White patients, they are 3.5 times less likely than White patients to receive living donor kidney transplantation (LDKT), which offers the greatest quality of life and lowest risk of morbidity and mortality. 2
Patient-level barriers to LDKT include a lack of knowledge and awareness, financial concerns, distrust toward the healthcare system, and religious beliefs that the body needs to remain whole to enter heaven.3–6 Potential kidney recipients’ reluctance to discuss LDKT with family members may be due to historical and current inequities in the healthcare system more broadly.7,8 These patient and system-level barriers converge to produce reduced kidney transplant access, particularly for Black patients. There is a need for improved communication between dialysis facilities and transplant centers throughout referral of these patients; dialysis staff would benefit from greater engagement with transplant centers to help patients at each stage of the evaluation and waitlisting process.
To reduce barriers, technology may be important for educating patients about live donor kidney transplant and strengthening communication between health systems.
9
Stemming from a need for multilevel interventions addressing barriers to LDKT among Black ESKD patients, the investigators adapted a culturally sensitive patient-level learning platform (Living ACTS, or
Specific AIM
This study aimed to evaluate whether adding patient-level education to an existing systems-level intervention would yield improved patient outcomes related to information, motivation, and confidence in the ability to discuss LDKT among Black patients. The investigators hypothesized that from baseline to immediate follow-up during the clinic transplant evaluation visit, patients who received Living ACTS in a transplant program that used T-REX would demonstrate greater: (1) knowledge and understanding of the process of LDKT, including benefits and risks, (2) motivation to pursue LDKT, and (3) confidence to discuss LDKT as a treatment option with friends and family, as compared to participants who received standard education. While results for the primary outcomes of this study have not yet been reported, understanding the effect of the intervention on psychosocial outcomes could inform future analyses of clinical outcomes.
Design/Methods
Design
This study is a 2-arm randomized trial designed to test the effectiveness of the Web-based Living ACTS educational intervention administered to Black patients with ESKD being evaluated at 1 of 2 southeastern US transplant centers. 12 The study protocol was approved by the 2 relevant Institutional Review Boards.
Prior to this study being conducted, both transplant centers implemented a new electronic application called T-REX as a standard of care. 12 Transplant Referral EXchange is a secure, information technology intervention intended on targeting multiple levels of influence (facility leadership, staff, and dialysis patients) to improve the efficiency and communications of the early transplant referral and evaluation process across health systems using a multimodule, HIPAA-compliant, web-enabled software application. The implementation of T-REX occurred in a staggered fashion to run parallel with patient recruitment and data collection. 12
The Living ACTS website was designed to provide culturally sensitive web-based education around LDKT for Black patients in the US Southeast. 12 The Living ACTS website shares evidence-based information from health care providers, personal stories from donor/recipient pairs that emphasized the role of family in LDKT, and practical skills for identifying a living donor from a perspective of cultural sensitivity. 13 The website consists of 5 tabs, each of which includes one video of 2 to 8 min in length: (a) Introduction to LDKT, (b) Benefits and Risks of LDKT to the recipient and donor, (c) The Kidney Transplant Process, (d) Identifying a Potential Kidney Donor, and (e) Act Now, based on the constructs of the information–motivation–behavioral skills (IMB) model. 14
Participants were encouraged to click on the tabs and watch the videos that they were most interested in watching to closely simulate how they might naturally engage with the website. Those who were randomized to the intervention condition across both sites had access to the Living ACTS website. This type of educational intervention that explicitly focuses on Black/African American patients aligns with a recommendation made by Sandal et al 15 in a recent systematic review and meta-analysis of educational interventions that seek to improve measures of LDKT.
Setting
This study was conducted in 2 large kidney transplant centers in the Southeastern United States. Participants completed their study-related tasks either in the transplant center or in their own private spaces (eg, at home).
Population
The target population consists of Black patients who initiated their evaluation for kidney transplantation at 1 of 2 transplant centers in the Southeastern United States. Of the patient population of transplant center A that underwent kidney transplant evaluation between 2019 and 2023, 28%, 69%, and 4% were White, Black/African American, and other racial groups, respectively. For transplant center B, patients who underwent kidney transplant evaluation during that same time period, 27%, 71%, and 2% were White, Black/African American, and of other racial groups, respectively.
Sampling
Patients were deemed eligible for the study if they met the following criteria: (a) self-identified as African American or Black, (b) 18 to 70 years of age, (c) body mass index <35 kg/m2, and (d) English speaking. 12 Patient recruitment was conducted from February 2019 to January 2023. Patients were recruited and screened for enrollment in one of two ways: (a) Flyers detailing the study procedures and components of the inclusion criteria were posted in the lobby and patient rooms of the 2 transplant centers; and (b) A secure, password-protected report from each study site of all patients referred and scheduled for an upcoming evaluation was sent to the project coordinator. This report included those who were recognized as Black/African American in the electronic medical record. A question on the screening form (“Do you consider yourself to be Black or African American?”) further confirmed that participants self-identified as Black or African American. Eligible patients were recruited at the transplant centers during their evaluation appointment or called and offered to participate in the study via Zoom by trained research assistants. This study began with in-person recruitment and switched to a virtual format due to the emergence of COVID-19, which triggered hospital emergency operating procedures. Written informed consent was obtained from each patient before enrollment. 12
Data Collection
Demographic information
Items that assessed participant demographic characteristics included date of birth, gender, ethnicity, education, employment status, income, marital status, health insurance benefits, and length of time on dialysis.
Psychosocial Outcomes
Knowledge and understanding of LDKT were measured using a 13-item instrument comprised of true/false items. The items were adapted from a previous study of the original intervention 11 to align with the content of the website. Total scores were derived from calculating the number of items that were correct. The possible range was 0 to 13, and the actual range was 2 to 13.
Motivation to pursue LDKT was measured with a 9-item instrument from Waterman et al 16 and gauged the respondent's perceptions and attitudes toward LDKT. The possible range of the summed scores (on a 1-5 scale with 5 representing greater motivation) was 9 to 45 points, and the actual range was 11 to 43 (Cronbach α = .63).
Confidence in the behavioral skills to discuss LDKT was a 10-item instrument that was informed by the Waterman et al 16 construct of Situational Self-Efficacy. Items were developed to align with the intervention that captured confidence in the ability to carry out specific behaviors like starting a conversation about living donation with friends or family. Responses ranged from 1 to 5 with higher values relating to a stronger confidence level. The possible range of the summed score was 10 to 50; the actual range was 12 to 50 (Cronbach α = .89).
Data Analysis
Descriptive statistics were used to summarize the baseline characteristics of the study population by group or recruitment type (via Zoom or in-person) and study institutions. Differences in baseline characteristics between the intervention and control groups were compared using χ2 tests or Fisher exact test for categorical variables and t tests for continuous variables.
The scores of all psychosocial outcomes and calculated mean difference scores were described as means (M) with standard deviation (SD) at baseline and follow-up time periods by study group. Two-way analysis of variance was used to test the score change from baseline to follow-up between intervention and control groups. A χ2 test of independence was also performed to examine the relationship between study group and the amount of time participants spent engaging with video content.
The effectiveness of the Living ACTS intervention in changing knowledge, motivation, and confidence was assessed using generalized linear mixed models (GLMM) after controlling for study site, private insurance, and interview modality. Study group (intervention vs control) and time (baseline vs follow-up) were included as fixed effects in the model, along with an interaction term to assess whether the intervention effect differed from baseline to follow-up, and a random effect was included to account for clustering within the 2 institutions. The baseline characteristics were included in the adjusted GLMM if they were significantly different between the intervention and control groups. The level of significance for all statistical tests was set at α = .05. All analyses were conducted using R 4.2.3 with package lme4. 17
Procedure
Patients completed a baseline questionnaire via iPad addressing theoretical constructs in the IMB model (see Figure 1), and then were randomized to condition by a research coordinator using a smartphone application. Patients randomized to the control arm were provided an iPad to watch one 12-min National Kidney Foundation video and explore the website content; those assigned to the intervention group received the Living ACTS intervention. Upon completion of a follow-up questionnaire, patients were given a $30 gift card. 12 Study coordinators completed a process evaluation survey that included an item assessing how long participants interacted with the website.
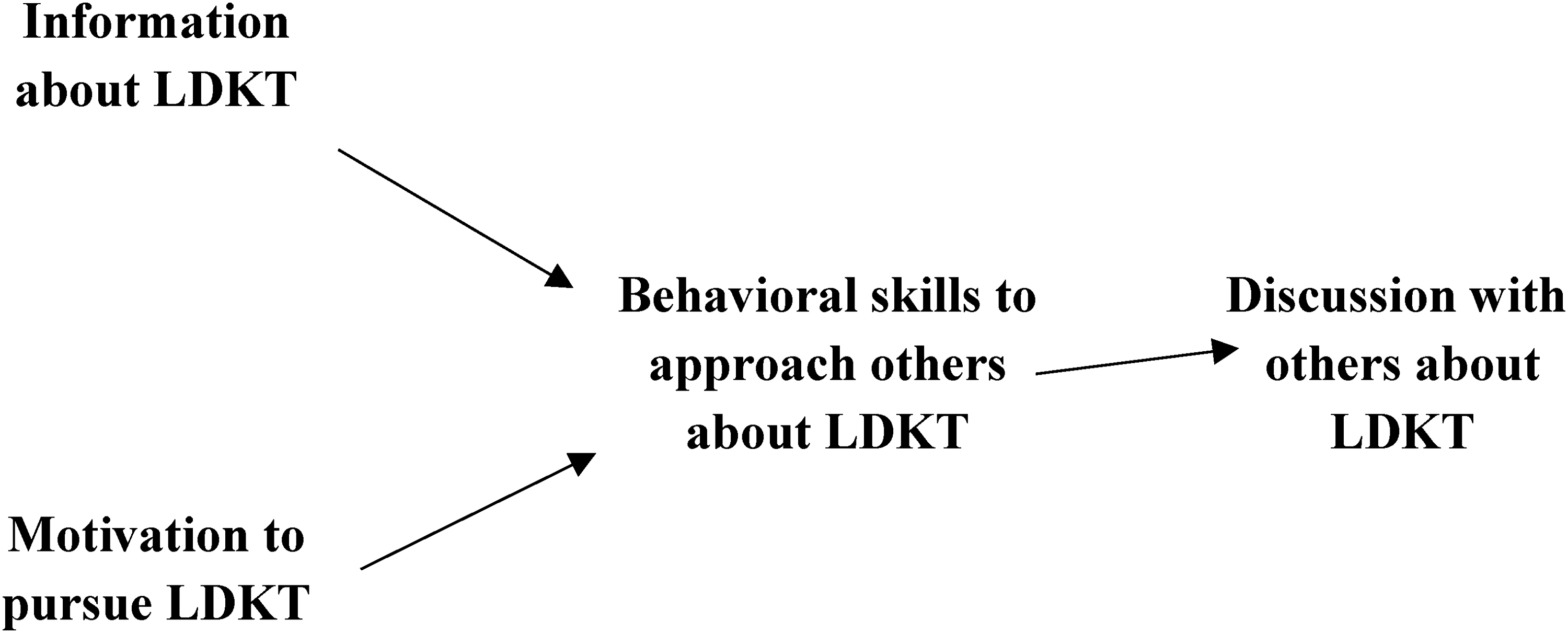
Information, motivation, behavioral skills Model 14 for living donor kidney transplantation. LDKT, living donor kidney transplantation.
Results
There were 2690 participants who were referred to the study via weekly reports of patients with upcoming appointments. Of these, 965 were invited to participate based on further eligibility screening (see Figure 2). The final study sample consisted of 416 participants, with 68% enrolled at study site 1% and 32% at study site 2 (Table 1). Of these, 411 patients completed follow-up measures (189 and 222 randomized to the control and intervention groups, respectively). The mean age for participants was 49.5 years, with most patients consisting of men (55%). The greatest proportion of participants had completed high school or equivalent (48%), was unemployed (30%), had household incomes of $10k to $29k (27%), and did not have private health insurance (64%).
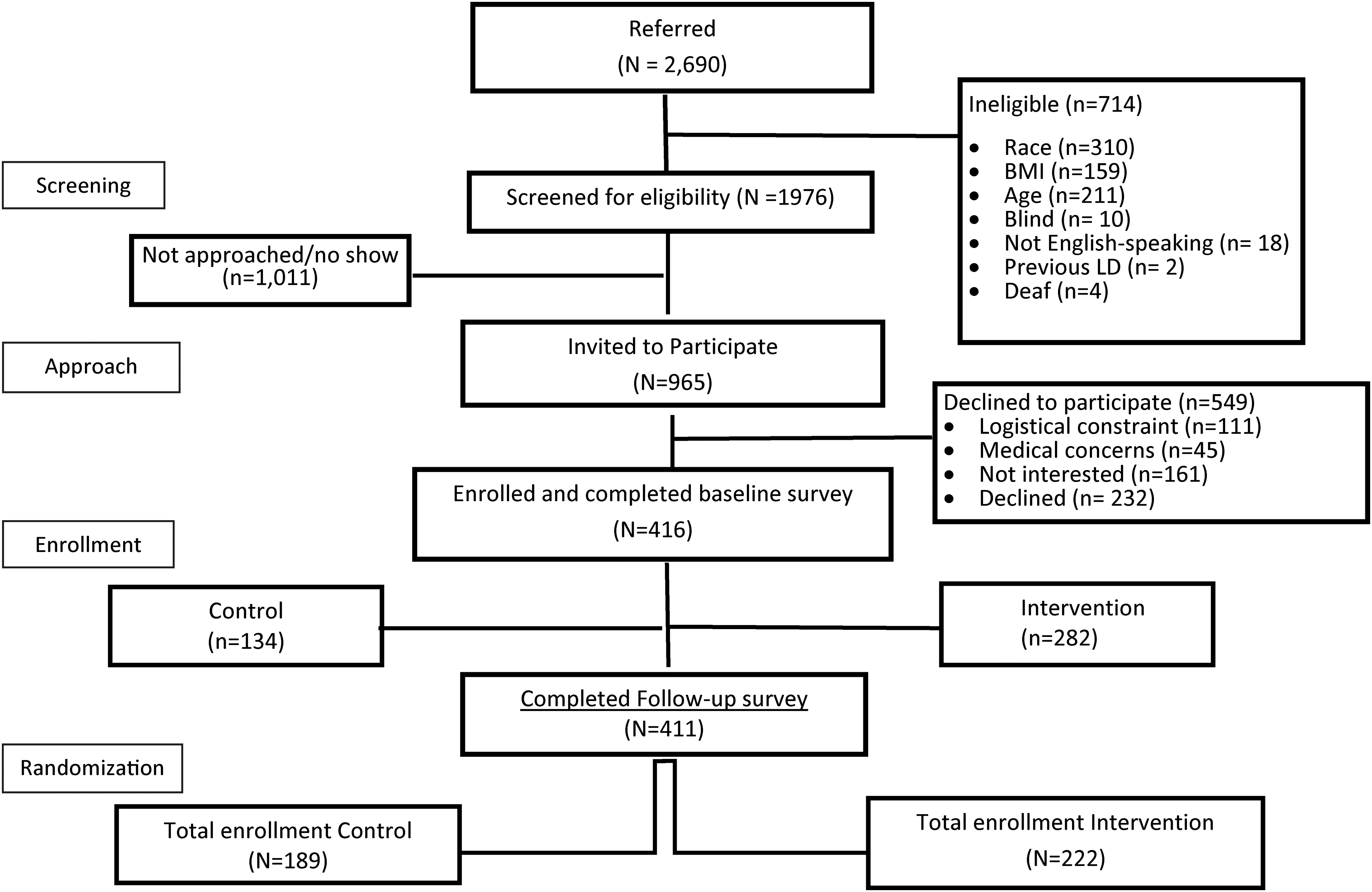
Study participant enrollment and randomization.
Baseline Participant Characteristics of the Study Population by Study Group at Time of Enrollment, 2019 to 2023 (N = 416).
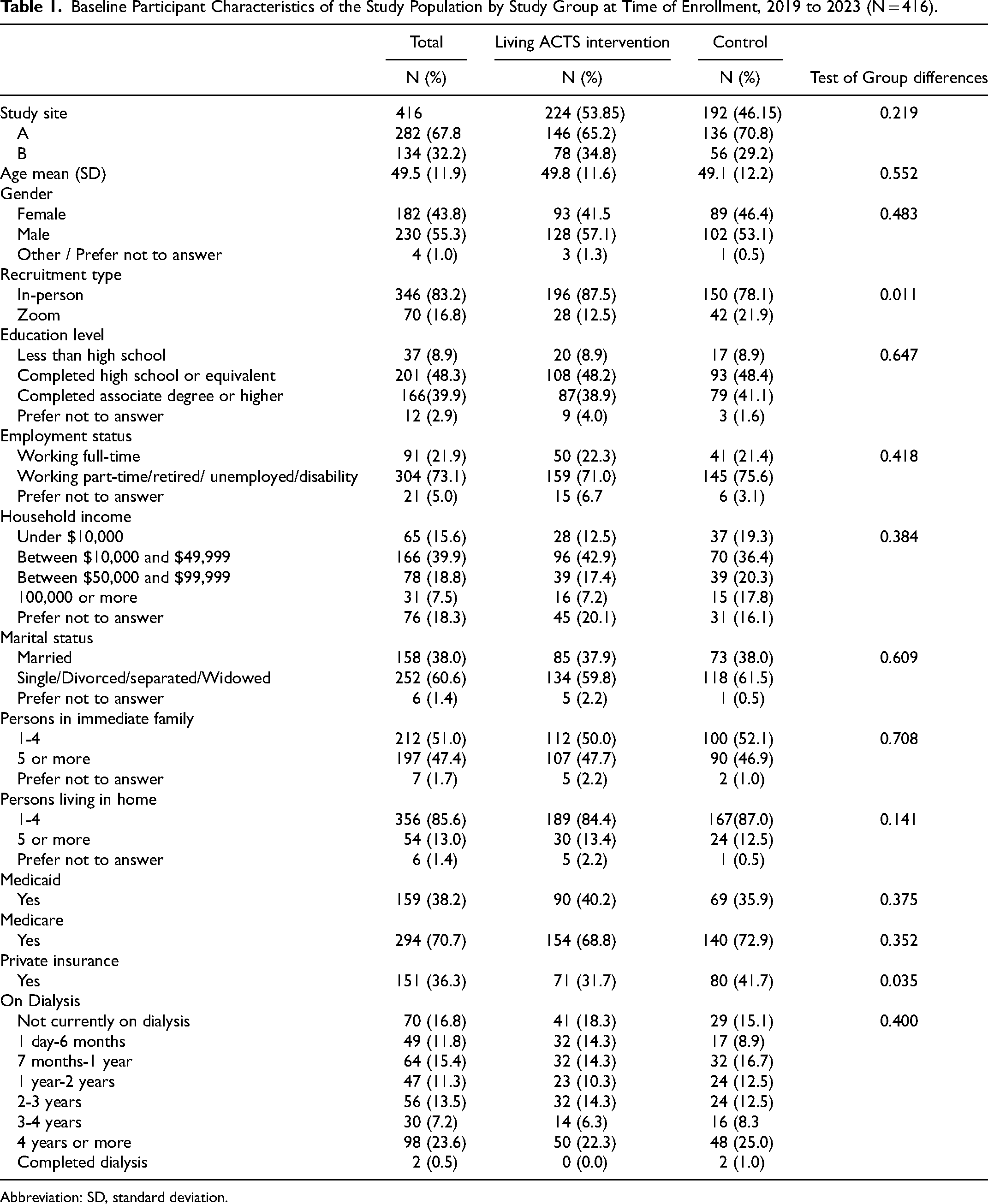
Abbreviation: SD, standard deviation.
Among the 411 participants with follow-up data, pre-post analyses using 2 sample t tests show that of the three outcomes (knowledge of LDKT, motivation to pursue LDKT, and confidence in the behavioral skills to discuss LDKT), only knowledge produced a significant difference between the 2 groups in the change from baseline to follow-up (see Table 2). Knowledge of LDKT slightly increased among the intervention group (M = 0.117, SD = 1.30) and slightly decreased for the control group (M = −0.159, SD = 1.43) (P = .04). For motivation and confidence, there were no significant group differences in change from baseline to follow-up (Table 2).
Two-Sample T Test Mean Baseline and Follow-Up Scores by Study Condition (N = 411).
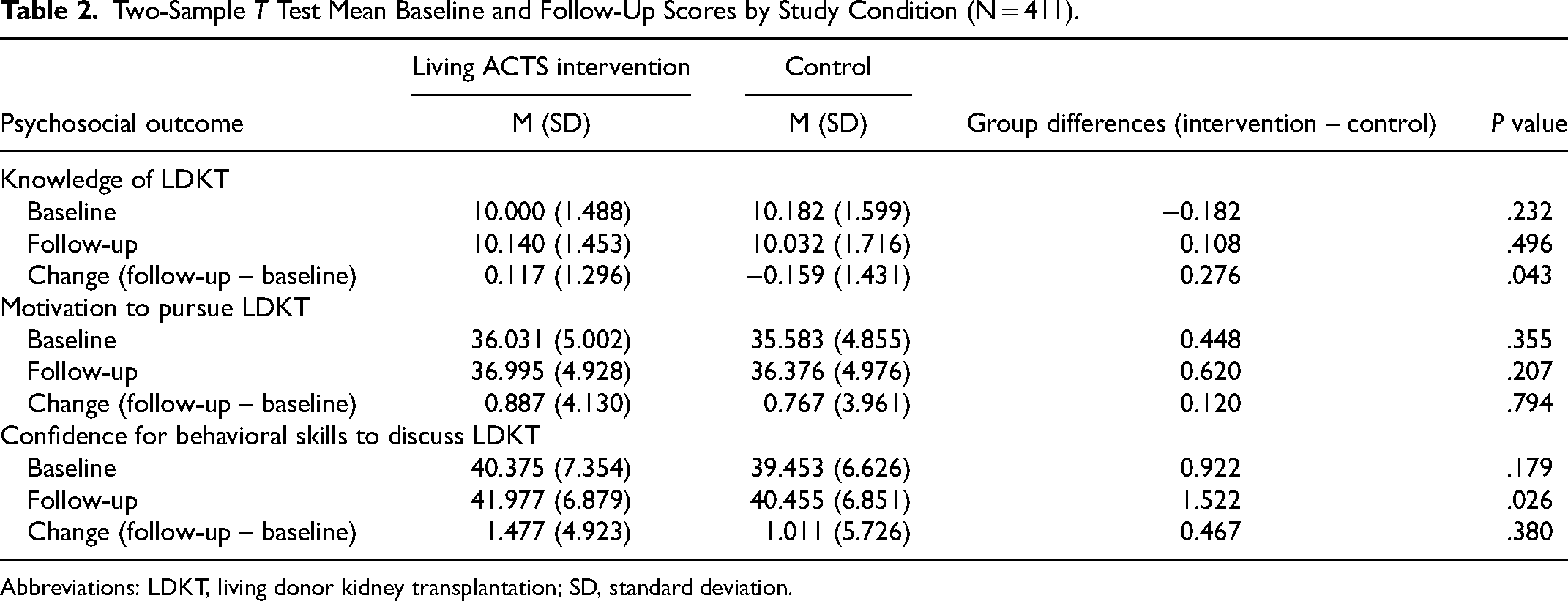
Abbreviations: LDKT, living donor kidney transplantation; SD, standard deviation.
Results based on multivariable analyses examined the effect of condition, time, and condition by time, controlling for private health insurance, interview mode, and study site (Table 3). For knowledge, there were no significant effects. For motivation, there was a significant effect of time (t = 3.066, P ≤ .01), such that intervention and control participants increased in motivation for pursuing LDKT from baseline to follow-up, based on adjusted mean increases of .9 and .8, respectively.
Analysis of Variance Testing Knowledge, Motivation, and Confidence in Relation to Study Condition, Time, and Their Interactions (N = 411). a
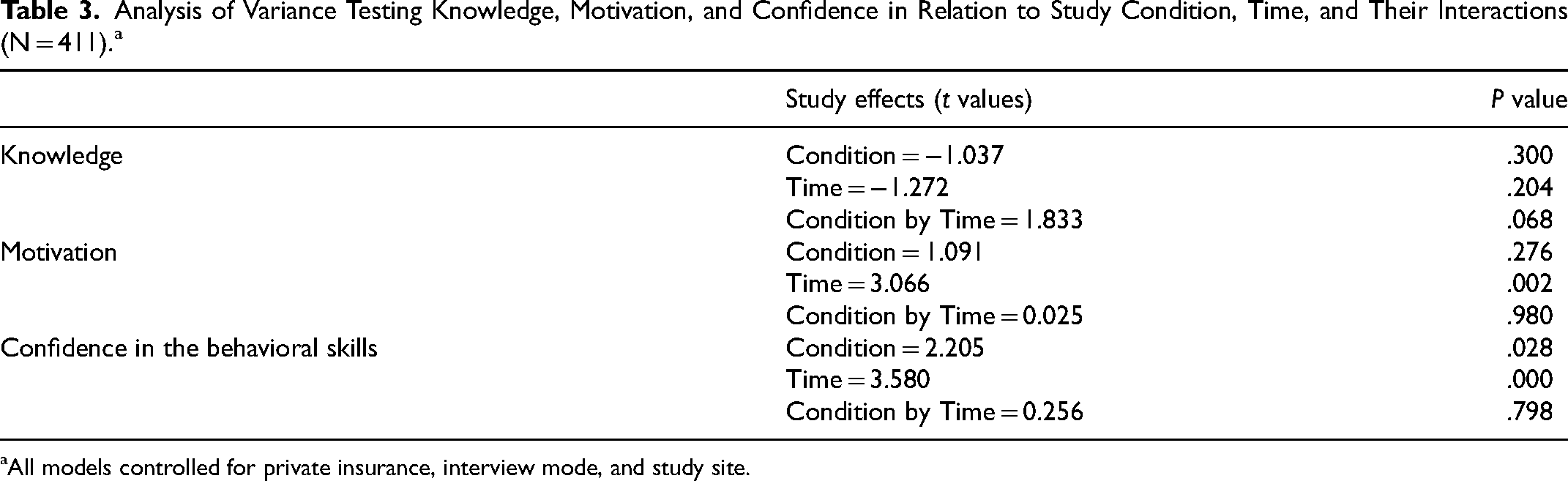
All models controlled for private insurance, interview mode, and study site.
For confidence in pursuing LDKT, the investigators found a significant effect of condition and time (t = 2.205, P ≤ .05; t = 3.580, P ≤ .001), respectively. Intervention participants had higher scores at baseline and follow-up (41.4 and 42.8, respectively) than control participants (40.0 and 41.2, respectively), and both groups increased in confidence from baseline to follow-up. There was no significant condition by time interaction. Finally, the relationship between the study condition and the amount of time participants spent engaging with video content was significant (c2(7) = 51.130, P < .001), indicating that staff perceived longer engagement with video content among intervention participants compared to control participants.
Discussion
The purpose of this study was to evaluate the immediate postintervention efficacy of an adapted culturally sensitive, web-based educational intervention on LDKT for Black patients. This study reports on psychosocial outcomes that are distinct from a subsequent analysis that focuses on clinical outcomes of importance (ie, living donor inquiries). Drawing from the IMB model,18,19 findings suggested that motivation and confidence to discuss LDKT increased immediately following the intervention delivery across both study conditions, although there were no significant effects on knowledge of LDKT.
The previous video-based Living ACTS intervention on which the current intervention was based demonstrated an increase in knowledge, 11 but the adaptation of this intervention for the web environment may have undermined this effect. For example, the decision was made to allow participants to click on the tabs that they were most interested in, understanding that few, if any participants, would click on all 5 tabs and watch all 5 videos included in the website. The advantages of a more nimble, customizable website may undermine the ability to detect changes in overall knowledge, and future interventions may seek to embed brief (eg, 5-item) surveys for each intervention module to detect knowledge changes with greater precision or use other methods to ensure that patients fully engage with website content.
The significant increases in motivation to pursue and confidence to discuss LDKT across both study conditions suggest that the Living ACTS website was no more effective than the control site at improving these 2 outcomes, regardless of time spent with the intervention. This finding was surprising given the attention to cultural sensitivity in developing Living ACTS and the strong theoretical foundation on which the intervention was based. Specifically, there was support for the importance of culturally sensitive interventions across a range of chronic diseases, 13 and the IMB model 14 has been associated with positive health outcomes in a variety of different disease entities.18,19 Nevertheless, there were a range of different reasons for this finding that included methodological considerations as well as characteristics of the intervention itself.
From a methodological standpoint, the process of completing the baseline assessment may have primed participants across both study conditions to consider LDKT simply based on the completion of the baseline and follow-up measures. Moreover, in administering the intervention, a few challenges became apparent. First, getting participants to engage with the intervention in the context of a busy clinical environment was difficult. It was important to deliver the intervention in between appointments so that the flow of care delivery was not interrupted, but this may have led to participants being distracted and only engaging with the intervention materials superficially. It is arguable that there was simply too much information provided in both the website and the embedded videos for patients (who could have been tired, distracted, or feeling ill) to retain.
There was much learned from implementing and evaluating the Living ACTS intervention that may be helpful as administrators of other US transplant centers think about how to effectively address racial disparities in LDKT. Dismantling systematic barriers to LDKT is critical to improving access for patients of color. This study suggests that engaging patients in education to supplement system-level interventions may have some limited added benefit. The individual-level intervention may need to be tailored to specific patient concerns if it is to be most effective. Studies of individually tailored interventions in other health conditions support this contention. 20 It may be useful to take the intervention outside of the clinic, given the challenges of delivering the intervention in a busy clinical environment. With the rise of telehealth, there are opportunities for more individually targeted interventions to patients and their families in their home environment, as has been done in other contexts. 21
Pursuing LDKT is a difficult life decision that has implications for the health of a family member. The investigators viewed individually targeted education as part of a protracted decision-making process. It was possible that patients preferred to discuss the educational content and have conversations about LDKT with friends and family, such that immediate changes in outcomes may not be observable. The investigators made the decision to recruit study participants who had been referred for evaluation to increase the viability that they would be approved for transplant. Moving earlier in the pipeline (eg, dialysis centers) could allow for a broader range of patients to receive the intervention and possibly spur interest in transplant for some patients prior to evaluation referral. Finally, a recent systematic review and meta-analysis underscored the importance of moving beyond psychosocial outcomes to evaluate the effect of educational interventions on actual health behaviors (ie, actual LDKT, donor evaluation, and living donor inquiries) with the possibility that findings may vary based on the specific health behavior. 15
This study had additional limitations. First, there was no website usage data collected during the duration of this study. This would have provided greater precision in the measure of how long patients spent on the website (than what staff perceptions provided) and allowed us to track what topics patients engaged with the most. The study lacks generalizability in that only 2 centers participated in data collection and the self-selection of patients into the study may itself, generate a somewhat biased sample. Moreover, this study generated small effect sizes where clinical significance was less certain. The COVID-19 pandemic forced the pivot to Zoom format for data collection, which was not ideal, thus, the investigators controlled for format in the multivariable analyses. Lastly, this study was limited to self-reported psychosocial outcomes. The primary outcome of living donor inquiries at one year could show different results.
Conclusion
This randomized trial determined the effect of an individual-level intervention on psychosocial outcomes in the context of a larger structural intervention that sought to improve access to LDKT among Black patients. This study supported the importance of systems-level interventions and suggests the need to carefully understand the role of individual-level education alongside these systems change. Given the consistent and pervasive inequities in access to LDKT for Black patients, more work is needed to understand the most effective mechanisms for intervention given the logistical challenges of the healthcare environment.
Footnotes
Acknowledgments
The authors are grateful to Melissa Ruth Thomas, BS for her editing assistance on this manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Institute of Health, National Institute of Diabetes and Digestive and Kidney Diseases (5R01DK114891-05). The clinical trial registration number is NCT03819686.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Correction (June 2025):
“MPH” appearing erroneously as Courtney Tresslar's educational degree in the original publication has now been removed upon author's request.