
Abstract
Introduction
Durable left ventricular assist devices serve as a critical bridge to heart transplantation for patients with advanced heart failure. Yet the demands placed on care partners (CPs) are often underestimated, and their well-being in supporting postimplant recovery is frequently overlooked.
Methods/Approach
This qualitative single-site study explored the struggles and support needs of 13 CPs who participated in audio-recorded interviews following device placement.
Findings
Data analysis, using inductive content analysis, revealed 6 major themes: feeling unprepared, being hypervigilant, feeling overwhelmed, the vanishing CP, lacking self-care, and needing connection with other CPs. Findings revealed that CPs often felt overlooked by healthcare teams, contributing to emotional distress and isolation, while inadequate education on perioperative complications and minimal peer support reinforced their sense of being unprepared.
Conclusion
These results underscored the integral role that CP well-being played in sustaining successful device management and ensuring patients remained eligible for heart transplantation. Psychosocial services, peer support, and structured educational programs may help mitigate the strain experienced by CPs and improve transplantation outcomes. Embedding CP needs into the transplant pathway, beginning at implantation, was essential to preventing burnout, maintaining candidacy, and improving overall posttransplant success. Refinements in CP-centered interventions may help reduce hospital readmissions, enhance device adherence, and support emotional resilience. By prioritizing CP support within advanced heart failure management, transplant programs can optimize both patient and CP well-being and foster positive outcomes. Such focus ensures bridging to transplantation and hope for families.
Keywords
Introduction
“Every day was like, ‘How's (the patient) doing?’ … no one would ever say, ‘How are you doing?’ It's hard and it still is hard. Because you really lose yourself.” This reflection from a care partner (CP) illustrates the emotional toll faced by individuals supporting patients with advanced heart failure. Durable Left Ventricular Assist Devices (dLVADs) often serve as a bridge to heart transplantation amid donor heart shortages.1,2 However, their success hinges on the dedication of CPs, who shoulder complex responsibilities that persist long after hospital discharge.3,4
Although research underscored CPs' importance in managing advanced heart failure, existing interventions remain patient-centric, leaving CP needs underaddressed.5‐7 This gap impedes the development of collaborative care models that consider CP well-being, leading to insufficient caregiving capacity, disrupted follow-up, and compromised transplant readiness. 8 Understanding their lived experiences was crucial to ensuring they were adequately supported in the transition from hospital to home and equipped for the next phase of the transplant journey.8‐10
When CPs lacked proper support, both treatment adherence and patient outcomes declined.9,11,12 Stable and well-supported care networks were particularly essential for heart transplantation,13‐15 underscoring the need to prioritize CP needs. The primary objective of this study was to explore the struggles and support needs of CPs following dLVAD implantation, particularly during the pivotal phases of hospitalization, discharge, and the first month at home so to inform practices that foster their well-being and ultimately contribute to improved transplantation outcomes.
Methods
This qualitative study was part of the Dyadic Interviews of CPs and Persons Living with a dLVAD project. It employed an inductive content analysis approach 16 and received Institutional Review Board (IRB) approval. Participant anonymity was safeguarded throughout the study.
Setting
The study was conducted at a major medical center in the Southwestern United States that specializes in advanced mechanical circulatory support (MCS). This center routinely performs dLVAD implantations for both bridge-to-transplant and destination therapy. Both CPs and patients were interviewed separately from each other. The present article focuses on CP experiences from the initial hospitalization through the early postdischarge period.
Sampling
A purposeful sampling strategy ensured a broad range of experiences by including CPs whose loved ones had encountered both significant perioperative complications and relatively routine postimplant courses. MCS coordinators contacted potential participants by phone and reviewed an IRB-approved information sheet. CPs were eligible if they were 18 years of age or older, were able to communicate in English, and were identified by the patient as the primary caregiver. Sampling concluded once thematic saturation was achieved.
Information Collection
Interviews of the CPs took place before or after the patient's scheduled clinic visits to minimize logistical burdens. Each interview lasted approximately 1 h and followed a semistructured guide. The questions focused on CPs' perceptions of preparedness and unexpected challenges related to the dLVAD, as well as their experiences and emotional changes during the initial weeks after discharge. A silent note-taker documented contextual cues, including emotional tone and environmental details.
All interviews were audio-recorded using a password-protected digital recorder. Immediately following each session, the recordings were transferred to an encrypted computer and then sent to a professional transcription service. After the research team verified transcript accuracy, audio files were permanently deleted in accordance with IRB requirements.
The research team employed ATLAS.ti v8 (ATLAS.ti Scientific Software Development GmbH Berlin, Germany) to conduct iterative coding and thematic development. Analysis began with multiple rounds of coding aligned with the interview guide, followed by weekly team discussions to refine emerging categories and resolve discrepancies by consensus. Trustworthiness was enhanced through triangulation of data sources, maintenance of analytic memos, and routine debriefing sessions aimed at clarifying interpretations and strengthening credibility.
Findings
CPs (N = 13) of patients with dLVADs were interviewed, either alone or, in group over a period of 2 months (August to September 2018), totaling 8 interviews. Sample demographics are displayed for CPs and patients in
Demographic Characteristics of Patient-Designated Care Partners and Patients.
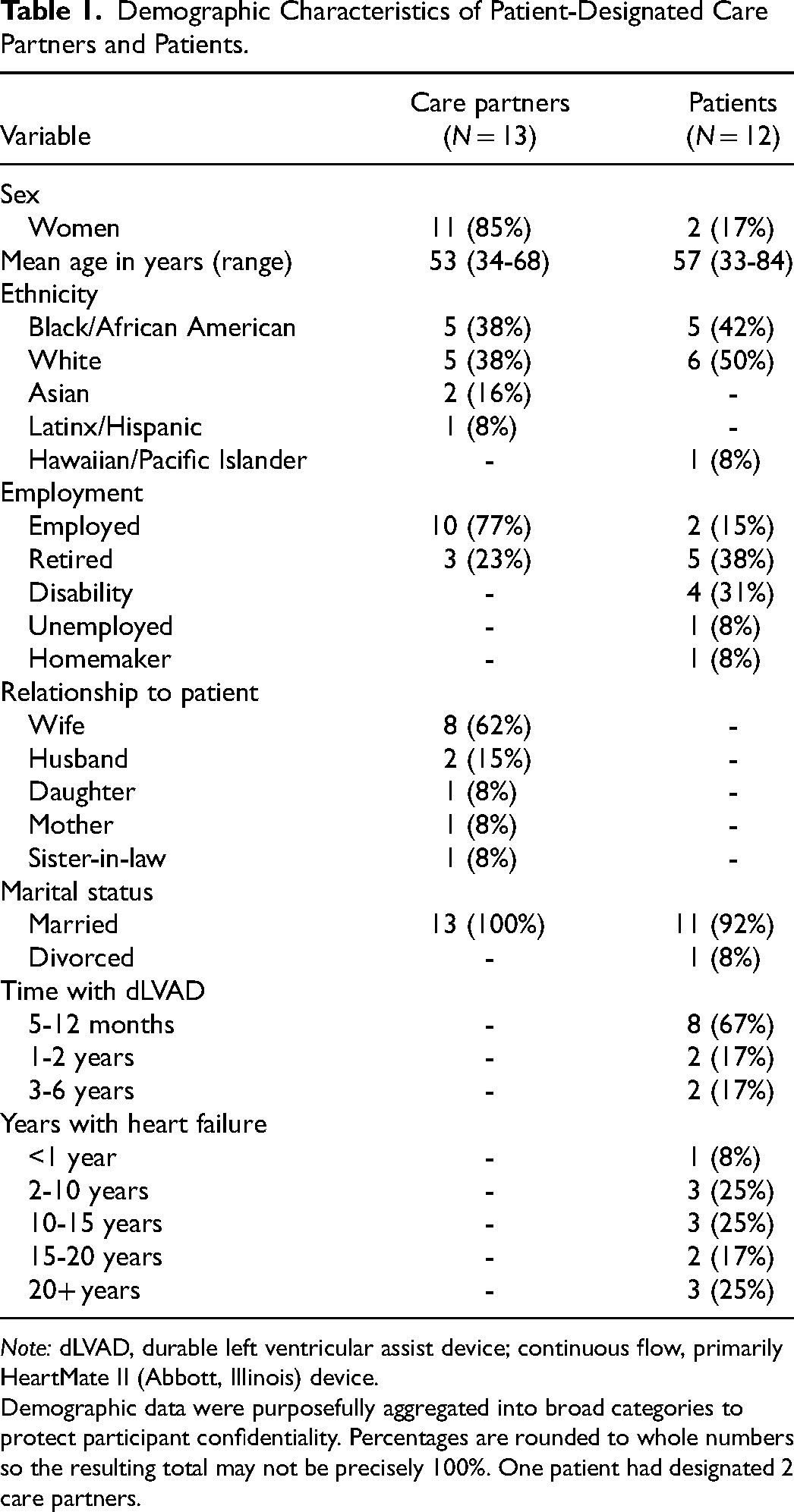
Note: dLVAD, durable left ventricular assist device; continuous flow, primarily HeartMate II (Abbott, Illinois) device.
Demographic data were purposefully aggregated into broad categories to protect participant confidentiality. Percentages are rounded to whole numbers so the resulting total may not be precisely 100%. One patient had designated 2 care partners.
Six major themes were identified from the CP's perceptions of preparedness and self-care at hospital discharge and during the first month after their partner's return postimplantation. These themes were: (1) Feeling unprepared, (2) Being hypervigilant, (3) Feeling overwhelmed, (4) Vanishing CP, (5) Lack of self-care for the CP, and (6) Needing connection with other CPs. Representative quotations from each theme are presented in
Major Themes With Supporting Quotations From Care Partner Participants.
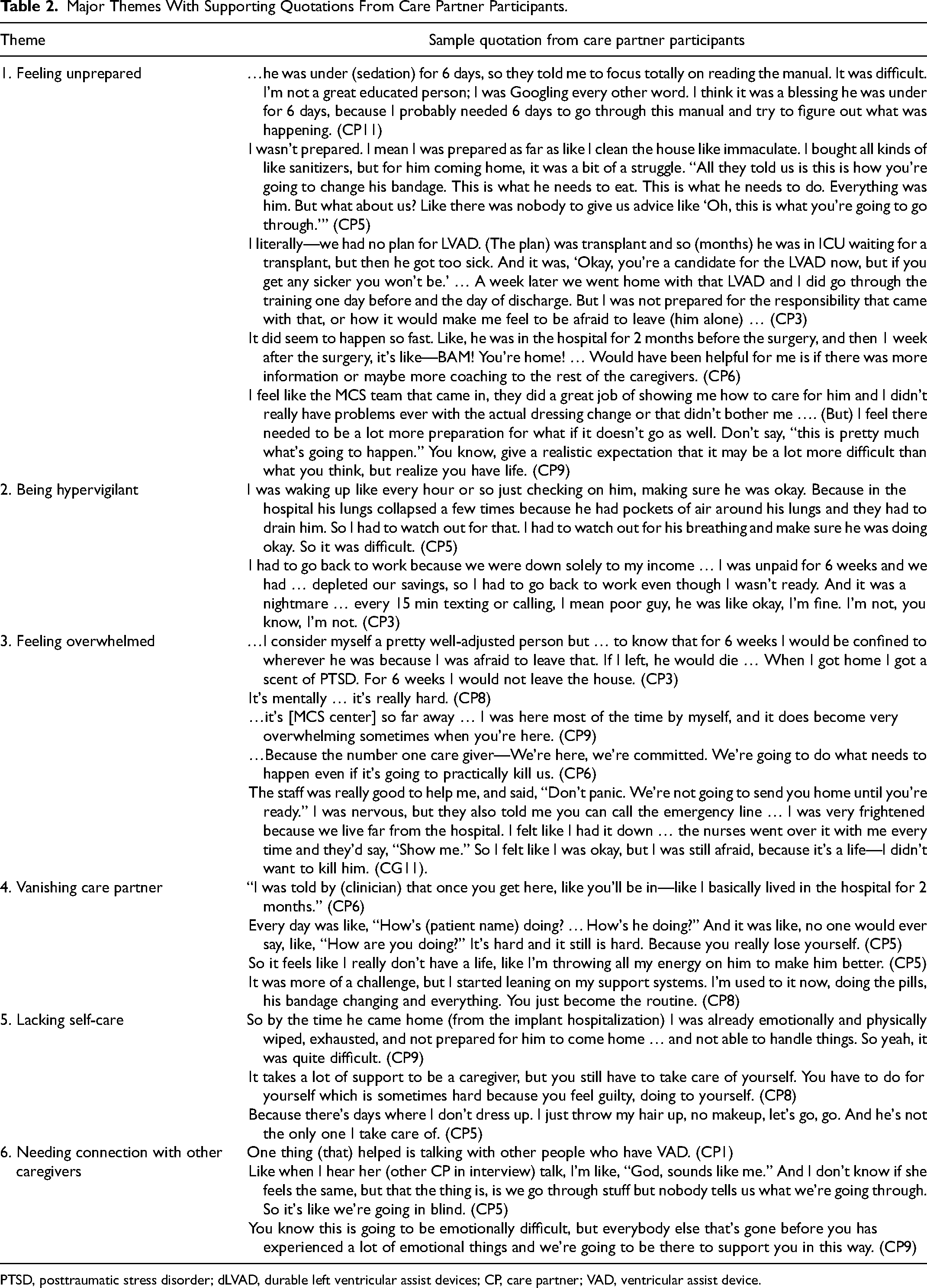
PTSD, posttraumatic stress disorder; dLVAD, durable left ventricular assist devices; CP, care partner; VAD, ventricular assist device.
Theme 1: Feeling Unprepared
When asked about their preparedness at hospital discharge and for the first 2 weeks at home, several CPs highlighted receiving good education from MCS staff, including demonstrations of essential skills. One CP felt well-prepared: I do feel that I was prepared to go home and care for him. I felt that we were educated, and I understood what was going on, what was implanted in him, what the alarms were, changing of batteries, changing bandages. (CP2)
Another CP used her husband's extended hospital stay to educate herself: …he was under (sedation) for 6 days, so they told me to focus totally on reading the manual. It was difficult. I'm not a great educated person; I was Googling every other word. I think it was a blessing he was under for 6 days, because I probably needed 6 days to go through this manual and try to figure out what was happening. (CP11)
In contrast, those who were referred urgently to dLVAD without a clear plan felt unprepared. One spouse said: I literally—we had no plan for dLVAD. (The plan) was transplant … A week later we went home with that dLVAD and I did go through the training one day before and the day of discharge … I was not prepared for the responsibility that came with that, or how it would make me feel to be afraid to leave (him alone). (CP3)
In one case, a patient and family did not receive the standard educational binder preoperatively: I feel like that's where we were lacking some information … Because they didn't know all the possible side effects that she could have … They gave us a book, some kind of binder (after we left the hospital). So, if we had seen that before, our reaction probably would have been different … This is what we should have seen when they were giving us time to make up our minds… (CP7b)
Being unprepared for perioperative complications was another concern. The husband of the patient above explained: It seemed like this was going to be a one-day event, and it ended up being months … during the procedure there was … they ruptured something … she had an R (VAD) and an L (VAD), so both of them … We were not prepared for that. (CP7a)
Even among CPs who felt competent with the dLVAD equipment and whose partners did not experience complications, fear at hospital discharge, and the first 2 weeks at home was common: I was scared because there was a lot of things to figure out … the batteries, remembering to take them with you when you went out the door … it's just so much. (CP10)
Participants recognized hospital staff as helpful, but were aware that postdischarge, their partner's life was in their hands: The staff was really good to help me, and said, ‘Don't panic. We're not going to send you home until you're ready.’ I was nervous, but they also told me you can call the emergency line … I was very frightened because we live far from the hospital … I was still afraid, because it's a life—I didn't want to kill him. (CP11)
CPs also felt unprepared for their caregiving role itself: All they told us is, ‘This is how you're going to change his bandage. This is what he needs to eat. This is what he needs to do.’ Everything was him. But what about us? Like there was nobody to give us advice like ‘Oh, this is what you're going to go through.’ (CP5)
Anticipatory guidance was needed for more than expected postoperative recovery and technical management of the dLVAD.
Theme 2: Being Hypervigilant
CPs described a heightened state of vigilance during the initial weeks following the perioperative period. I was waking up like every hour … checking on him, making sure he was okay … his lungs collapsed a few times because he had pockets of air around his lungs and they had to drain him. So, I had to watch out for that … make sure he was doing okay. It was difficult. (CP5)
Another CP who needed to work due to financial constraints described the added stress of monitoring her spouse remotely. I had to go back to work because we were down solely to my income … I was unpaid for 6 weeks and we had … depleted our savings, so I had to go back to work even though I wasn't ready. And it was a nightmare … every 15 min texting or calling, I mean poor guy, he was like okay, I'm fine. I'm not, you know, I'm not. I had my daughter come in and be with him as much as possible. (CP3)
A more experienced CP compared the initial weeks postimplant to later months, noting her effort to reduce her helicopter (CP2) tendencies by arranging for others to spend time with the patient to encourage his independence. Despite this, she admitted that the thought of needing to be there for a potential heart transplant was always in the back of her mind.
Theme 3: Feeling Overwhelmed
CPs felt a heavy responsibility to keep their partner alive. Many described their partner experiencing poor mental acuity in the hospital and during the first few weeks after the implant. Consequently, CPs needed to demonstrate dLVAD competency, knowledge, and emergency actions to ensure the device's proper functioning and their loved one's survival. I felt like I had it [dLVAD training] down …the nurses went over it with me every time and they'd say, ‘Show me.’ So, I felt like I was okay, but I was still afraid, because it's a life—I didn't want to kill him. (CP11).
CPs often prioritized their partner's needs above their own, feeling an intense sense of duty. One CP encapsulated this sentiment by stating, “We're going to do what needs to happen even if it's going to practically kill us” (CP6).
Theme 4: Vanishing CP
During the patient's perioperative hospital stay, several CPs noticed that clinicians would frequently inquire about the patient but rarely ask how the CP was doing. Every day was like, ‘How's (patient name) doing? … How's he doing?’ And it was like, no one would ever say, like, ‘How are you doing?’ It's hard and it still is hard. Because you really lose yourself. (CP5)
This illustrated the first level of vanishing, where CPs begin to lose their identity and personal needs as they become fully immersed in patient care. Another CP shared: So, it feels like I really don't have a life, like I'm throwing all my energy on him to make him better. (CP5)
An older CP reflected on her first 2 weeks after her husband's dLVAD implant, comparing it to later months and years. She shared advice to a new CP and explained: It was more of a challenge, but I started leaning on my support systems. I'm used to it now, doing the pills, his bandage changing and everything. You just become the routine. (CP8)
The phrase, “You become the routine,” reflects the first stage of vanishing, where the CP is fully immersed in caregiving. This may start during the hospital and continue indefinitely as the CP loses themselves in the caregiving routine. The second stage of vanishing occurs when the CP reaches a breaking point and may disengage or leave the caregiving role entirely.
Theme 5: Lacking Self-Care
A common thread among the CPs was the lack of time, energy, or priority given to maintain their own well-being. This neglect often began during the hospitalization period: So. by the time he came home (from the implant hospitalization) I was already emotionally and physically wiped, exhausted, and not prepared for him to come home … and not able to handle things. So yeah, it was quite difficult. (CP9)
For many, this lack of self-care did not improve in the first weeks after return home.
Caring for a partner following dLVAD significantly disrupted routine activities for their own wellbeing. Many who did attempt to prioritize time self-care described feeling guilty for doing so, expressing that “you have to do (care for) yourself, which is sometimes hard, because you feel guilty.” (CP8) Overall, the CPs felt their ability to care for themselves diminish as they took on the responsibility of caring for the patient at home.
Theme 6: Needing Connection With Other CPs
Throughout the interviews, it became evident that most CPs had not spent formal time with other CPs. Many CPs found solace and support connecting with others who shared their experiences. One CP highlighted the benefit of connecting with other CPs: One thing (that) helped is talking with other people who have VAD. (CP1).
Another CP expressed how hearing similar experiences from others made them feel understood and less alone in their journey: Like when I hear her (other CP in interview) talk, I'm like, ‘God, sounds like me.’ And I don't know if she feels the same, but the thing is, we go through stuff but nobody tells us what we're going through. So, it's like we're going in blind. (CP5)
This sentiment was echoed by others who emphasize the importance of emotional support from those who have gone through similar challenges: You know this is going to be emotionally difficult, but everybody else that's gone before you has experienced a lot of emotional things and we're going to be there to support you in this way. (CP9)
CPs expressed a clear need for structured opportunities to connect with others in similar situations. Such connections can provide a crucial support network, making CPs feel less isolated and better prepared for the emotional difficulties they face. By sharing experiences and challenges, CPs can gain valuable insights and coping strategies.
Discussion
This qualitative study identified 6 themes illustrating the interconnected challenges CPs face: feeling unprepared, being hypervigilant, feeling overwhelmed, becoming a vanishing CP, lacking self-care, and needing connection with other CPs during the pivotal transition from hospital to home after a dLVAD placement. A dLVAD bridges advance heart failure patients to transplantation, though some require permanent support. The findings underscored that CP support is essential for both dLVAD management and long-term transplantation success. Patients with strong CP support more effectively maintain device function, prevent adverse events, and meet transplant candidacy requirements. 17 Consistent with other high-acuity care context (eg, prolonged mechanical ventilation, 18 spinal cord injury, 19 advanced cancer 20 or cognitive impairment 21 ), CPs faced rapid decision-making, extensive home care responsibilities, and heightened state of vigilance. Strategies shown to work in other acuity context such as psychoeducational interventions22‐24 and peer support networks25,26 may likewise benefit dLVAD populations.
The results extend prior work in 3 ways. First, they highlight the “vanishing” phenomenon, wherein CPs feel invisible, undermining both caregiver and patient well-being. This underscores the need to involve CPs in multidisciplinary discussions to prevent “flight” (ie, the CP leaving the patient). Failing to address CP well-being can exacerbate emotional strain and burnout, adversely affecting the entire care dynamic. By openly acknowledging the psychological toll on CPs and provide timely resources or referrals to support services, these individuals may be better equipped to sustain long-term caregiving roles. Second, the findings showed that participants received limited anticipatory guidance on perioperative complications and day-to-day problem-solving. Addressing these gaps was vital to minimizing readmissions and sustaining adherence,27,28 which is crucial for transplant readiness. Inadequate preparation often leaves CPs uncertain and stressed when confronted with sudden or complex postimplantation issues. By offering more comprehensive information early on, clinicians can help avert preventable crises, thereby enhancing the safety and well-being of both patients and their CPs. Third, many CPs expressed a strong desire for peer networks that offer the emotional support and practical advice often missing from clinical interactions. Support groups for CPs can reduce isolation, improve coping strategies, and facilitate respite, thereby enabling them to sustain caregiving roles and engage in self-care. 29
Bridging patients with advanced heart failure from dLVAD therapy to heart transplantation is a complex, interdependent process. Ensuring that CPs are adequately supported through robust education, psychosocial assistance, and peer connections can help sustain the patient-CP dyad and promote a stable transition to heart transplantation. By strengthening CP preparation and well-being, transplant programs not only reinforce device management but also enhance the likelihood of successful transplantation outcomes.
Limitations and Strengths
The limitations included potential recall bias for events up to 6 years prior and a single-site design that limits generalizability. Nonetheless, the sample captured both uncomplicated and complex perioperative experiences. Most CPs were persons of color, highlighting the need for further diverse inquiry. Direct quotes were used to enhance credibility.
Implications for Practice and Research
These nuanced findings call for systematic improvements in CP education, psychosocial support, and resource provision. Clinically, dLVAD programs should:
Pre-implant: Encourage early connections between new and experienced CPs, and provide comprehensive dLVAD education (technical, emotional, and practical). Hospital setting: Greet CPs by name, routinely assess their well-being, and ensure they receive self-care materials—such as a dedicated binder that includes anticipatory guidance and practical self-care strategies—to prevent the vanishing phenomenon. Post-discharge period: Maintain formal check-ins with CPs, encourage support group participation, and provide access to financial resources (eg, free or discounted parking) that alleviate stress.
Quality improvement initiatives include standardizing the predischarge education process for both technical and emotional preparedness and embedding mental health professionals in MCS teams to address high stress or burnout. Future research should feature longitudinal, multisite evaluations of CP experiences across the dLVAD continuum, linking CP well-being with patient transplant candidacy, waitlist times, and outcomes. Interventional studies on psychosocial support, structured home-care training, and flexible resources could establish best practices to lessen caregiving burdens and enhance quality of life for both patients and CPs.
Because long-term transplant success relies heavily on stable support within the home environment, 30 CP well-being must be recognized as a critical determinant of patient readiness especially during the dLVAD period. 9 Based on this study's findings, evidence-based interventions such as self-care strategies, anticipatory guidance, social work consultations, and peer support can directly address the 6 key challenges identified for CPs. By providing structured resources that promote emotional well-being, reduce isolation, and prepare CPs for day-to-day problem-solving, such interventions could bolster patient outcomes, lessen the risk of readmissions and streamline the pathway to heart transplantation. By embedding CP support as a core element of heart transplantation programs, clinicians, researchers, and policymakers can help guarantee that both patient and CP thrive from the time of dLVAD implantation through the achievement of a successful heart transplant. Fostering CP resilience through proactive support and intervention is essential to preserve their capacity to provide sustained care throughout the challenging journey from dLVAD to successful heart transplantation.
Conclusion
The findings underscored the pivotal role that CPs play in bridging advanced heart failure patients to heart transplantation following dLVAD implantation. Pervasive challenges of Feeling Unprepared, Being Hypervigilant, Feeling Overwhelmed, Vanishing CP, Lacking Self-Care, and Needing Connection with Other CPs were identified and, that, if left unaddressed, significantly heighten risks such as device complications, hospital readmissions, and emotional distress. Successful bridging to transplantation and favorable long-term outcomes hinge upon a well-prepared and supported CP. By embedding CP needs into the transplant pathway through structured education, psychosocial and financial support, and peer networking, healthcare systems can reduce burnout, maintain transplant candidacy, and optimize outcomes for both patients and CPs. Recognizing CP well-being as central to transplantation candidacy and policy will further improve overall success throughout the entire transplant process. Future research should continue to explore these findings, developing and evaluating more comprehensive strategies that promote positive outcomes for all involved.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support for this research from the Bethel University Professional Development Grant and Edgren Scholarship (Kristin E. Sandau, PhD, RN) and the Sigma Theta Tau Zeta Chapter Research Grant (Kristin E. Sandau, PhD, RN). Research reported in this publication was supported by the National Center for Advancing Translational Science (NCATS) of the National Institutes of Health under the UCLA Clinical and Translational Science Institute (Grant No. 5UL1TR001881-08).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with the research, authorship, and/or publication of this article.