
Abstract
Introduction
Rabbit anti-thymocyte globulin (rATG) induction ideal dosing strategies in kidney transplant recipients have not been fully elucidated.
Project Aims
This study compares the impact of ideal body weight-based versus actual body weight-based rATG dosing on drug purchasing costs and kidney transplant outcomes.
Design
Retrospective, single-center chart review of kidney transplant recipients receiving rATG induction using (1) actual body weight-based dosing between May 17, 2019, and Mar 13, 2020, versus (2) ideal body weight-based dosing between May 17, 2022, and Mar 13, 2023. The primary endpoint is the rATG drug cost/kidney transplant recipient [measured by average wholesale price] compared between cohorts. Secondary endpoints are rates of biopsy-proven acute rejection, readmissions secondary to infection, myelosuppression (leukopenia or neutropenia), and viremia (Epstein-Barr virus, cytomegalovirus, and BK virus) measured for 6 months. Study design adhered to EQUATOR STROBE guidelines for reporting cohort studies.
Results
Overall, rATG ideal body weight-based dosing resulted in a median $3838 saved per kidney transplant recipients, based on average wholesale price, and a statistically significant reduction in cost versus actual body weight-based dosing (P = .02). Secondary outcomes were generally similar between groups, with a difference in Epstein-Barr viremia (P = .017) not translating to a significant difference in readmissions for infection (P = .226).
Conclusion
Our institution conducts around 250 kidney transplants annually, and considering the majority will receive rATG induction, this dosing protocol estimates average wholesale price drug purchasing cost-savings of about $900 000/year without compromising early clinical outcomes.
Introduction
Induction immunosuppression inhibits the immune response and is administered at the time of transplantation. Most kidney transplant recipients will receive some form of induction.1,2 Recently, a 20-year retrospective study of United Network for Organ Sharing data reported on outcomes among recipients receiving either rabbit anti-thymocyte globulin (rATG), IL-2 receptor antagonists, or alemtuzumab. Overall, deceased-donor recipients receiving rATG had better death-censored graft survival; hazard ratio (HR) using IL-2 receptor antagonists versus rATG (HR = 1.065, P = .018) and alemtuzumab versus rATG (HR = 1.075, P = .013). In the same study, similar findings were also found among living-donor recipients. 3
While rATG is the most used induction agent, the ideal dosing strategy in recipients has not been fully elucidated. 1 Previously published literature has described rATG dosing strategies and clinical outcomes.4,5 Vacha et al assessed high-immunologic risk recipients and reported that ideal body weight (IBW)-based rATG dosing (7.5 mg/kg) resulted in similar tolerability outcomes compared with actual body weight (ABW)-based dosing. Unfortunately, the authors did not show an overall statistically significant cost-saving benefit. This study was limited by the inclusion of only high immunologic risk patients and a limited sample size. 4
Potential dosing strategies for rATG include the use of IBW, ABW, or adjusted body weight. 6 The hypothesis for this review was that using IBW dosing for rATG would confer significant cost-savings versus ABW dosing, without compromising patient and transplant allograft outcomes.
Design/Methods
Design
This program evaluation was a single-center, retrospective review to evaluate a pre- and post-implementation standard of care protocol change in rATG dosing. This research protocol was approved by the local Institutional Review Board (IRB).
Setting
The setting is a 988-bed academic teaching hospital and quaternary care center located in an urban setting, serving a racially and ethnically diverse population. The center's catchment area consists of 3 US states, and candidates come from many different zip codes and census tracts, reflecting socioeconomic diversity.
Population
The study population consisted of adult kidney transplant recipients undergoing transplantation and posttransplant management at a single academic transplant center during the specified study periods. Within the time periods of interest, the population was mostly White (56%) or African American (29%), 50 to 64 years old (32%), had a body mass index of 26 to 30 (23%), and male (56%). At the time of transplant evaluation, most of the sampled population were listed with a calculated panel reactive antibody percent (cPRA) = 0 to 9% (85%) and listed with a primary glomerular disease etiology of kidney disease (13%).
Sampling
Recipients were eligible for inclusion if they were ≥18 years old, transplanted between 5/17/2019 and 3/13/2020 or 5/17/2022 and 3/13/2023, received rATG monotherapy for induction immunosuppression, and had follow-up at the primary institution 6 months posttransplant. Periods of inclusion were chosen to capture retrospective data after protocol initiation, allow for a minimum of 6-month posttransplant follow-up at the time of IRB approval, and include a cohort of patients transplanted under the previous protocol within a similar period of months. The excluded period between eras aimed to limit the potential influence of COVID-19 pandemic-related immunosuppression protocol adjustments. Exclusion criteria also included: patients with dosing of rATG that varied from the institutional protocol, extrarenal (simultaneous or historical) organ transplants, experienced primary nonfunction, or calculated IBW > ABW. Dosing of rATG in recipients with a calculated IBW that exceeded ABW resorted to dosing based on ABW. For that reason, patients with IBW > ABW were excluded from this analysis.
Data Collection
Baseline characteristics collected as part of the review included patient age, height, and weight at the time of transplant, race/ethnicity, and primary indication for kidney transplant. Baseline transplant characteristics captured include cold ischemia time, frequency, and duration of delayed graft function (DGF), essential donor characteristics, and immunosuppression regimen.
The primary economic endpoint of this retrospective review is the difference in average total drug acquisition cost of rATG per kidney transplant recipient (KTR) between the 2 cohorts based on average wholesale price (AWP). The primary clinical endpoint was measured by the difference in rates of biopsy-proven acute rejection (BPAR) measured within a 6-month follow-up period. The primary tolerability endpoint considered frequency of readmissions for treatment of an infection, frequency of cytomegalovirus (CMV), Epstein-Barr virus (EBV), BK viremia (value above the lower limit of quantification per assay, based on quantitative polymerase chain reaction), and toxicity in the form of myelosuppression (defined as white blood cells [WBC] < 2000 cells/mcL or absolute neutrophil count [ANC] < 1300 cells/mcL).
Data over the 6 months were collected 2 weeks posttransplant (±3 days) and at 1, 2, 3, 4, 5, and 6 months (±7 days) posttransplant.
Data Analysis
Baseline characteristics were summarized with descriptive statistics and corresponding statistical tests to assess differences between cohorts (Fisher's exact test for categorical data and Wilcoxon rank-sum test for continuous data). For the primary economic outcome, the difference in AWP drug acquisition costs between cohorts was assessed with the Wilcoxon rank-sum test. Additional comparisons included an AWP estimated cost calculated based on whether patients had received the alternative dosing strategy and compared that cost with the dosing strategy received (eg, estimated costs of IBW-based dosing in the ABW cohort era vs actual costs of the ABW-based dosing patients received). Essential to the analysis, rounding doses of rATG to the nearest commercially available 25-mg vial size is standard for all KTRs at this institution. In the case of this cost estimation, statistical analysis utilizing the Wilcoxon signed-rank test was implemented. Clinical and tolerability endpoints were assessed with statistical tests as indicated based on variable type (categorical vs continuous). The retrospective review adhered to the EQUATOR STROBE guidelines for observational studies. 7 Data not available at specified time points were considered missing data.
Procedure
The recipient induction immunosuppression protocol transitioned from ABW-based rATG dosing to IBW-based dosing on May 16, 2022. The induction immunosuppression protocol for rATG dosing (3-5 doses of 1.5 mg/kg), other than changing from ABW to IBW dosing, did not differ between eras. The number of doses was based on pretransplant factors, such as race, retransplantation, cPRA percentage, and reported donor-specific antibody. Absolute lymphocyte count was monitored for efficacy. Dosing was paused for 1 to 2 days, but not reduced, for neutropenia or thrombocytopenia, according to the manufacturer's package insert. 8 Otherwise, the maintenance immunosuppression protocol consisted of tacrolimus (goal level 8-12 mcg/L up to 3 months, 6-10 mcg/L 3-6 months), mycophenolate mofetil 500 mg orally every 12 h, and prednisone taper (5 mg/day by postoperative day 10). In terms of early steroid withdrawal, only patients in the IBW cohort were transplanted in an era with a protocol allowing for a steroid-sparing immunosuppression regimen at baseline. Tacrolimus immediate-release capsules or extended-release tablets were used in both patient eras.
Candidates who met the inclusion criteria were identified using an internal kidney transplant programmatic database of recipients. Data points were collected via retrospective chart review for all recipients meeting exclusion criteria mentioned above and stored in a centralized database (REDCap). Statistical analyses were performed with Microsoft Excel® and Stata Statistical Software version 18 (College Station, TX: StataCorp LLC).
Results
A total of 359 patients were assessed for inclusion, with a final sample of 241 patients analyzed (ABW cohort—128 patients, IBW cohort—113 patients), which is illustrated in Figure 1. The most common reason for exclusion from the study in both groups was a calculated IBW exceeding ABW.
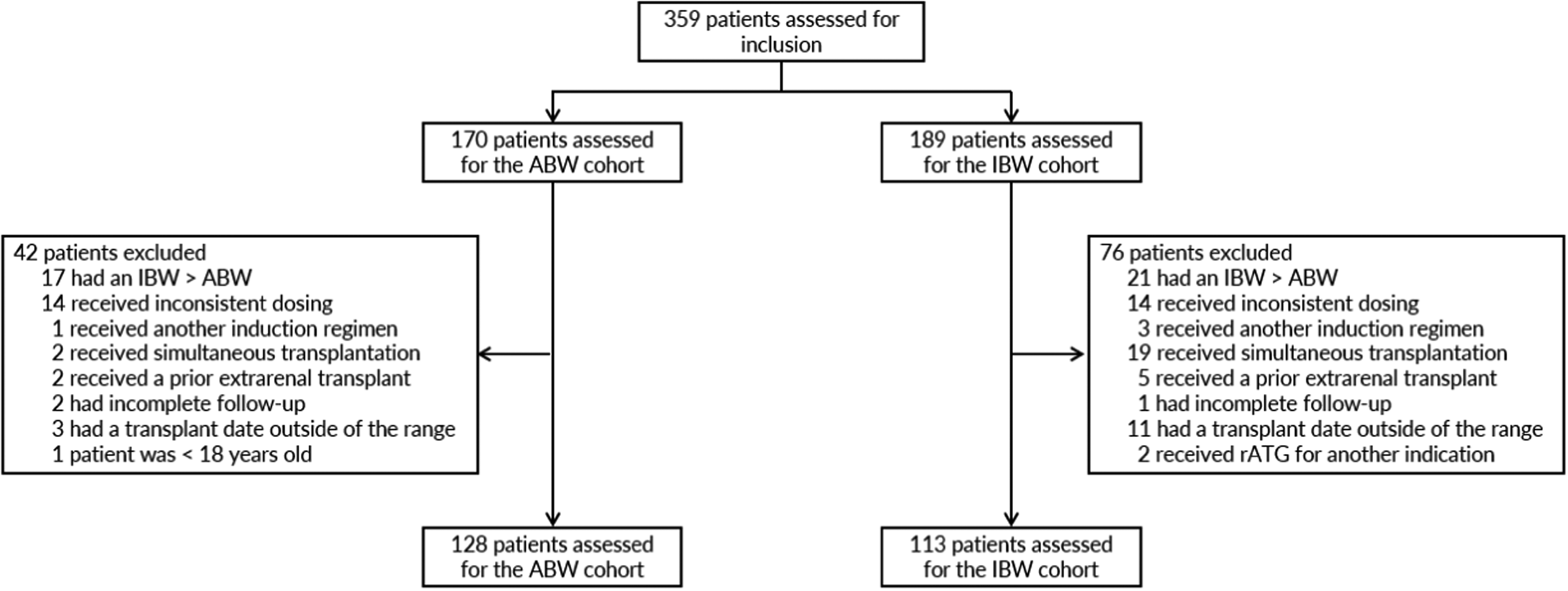
Initially, a total of 359 patients were assessed for inclusion, with 170 KTRs considered for the ABW cohort and 189 KTRs considered for the IBW cohort.
Demographics
Baseline characteristics of patients are summarized in Table 1. Overall, both cohorts were similar at baseline. Notable similar baseline characteristics include: the median ABW (ABW 83 kg vs IBW 86 kg, P = .06), calculated IBW (ABW 66 kg vs IBW 68 kg, P = .09), and median BMI (ABW 28.5 vs IBW 29.5, P = .26). There was a higher proportion of patients who were White, non-Hispanic in the ABW cohort versus the IBW cohort (56% vs 37%, P = .01) and a lower proportion of patients who were Black, non-Hispanic in the ABW cohort versus the IBW cohort (29% vs 46%, P = .01). Additionally, among patients receiving a deceased kidney donor transplant, the ABW cohort had a shorter median cold ischemic time (10 h vs 14 h, P < .01). The longer cold ischemia time was associated with significantly higher DGF rates in the IBW cohort (11% vs 31%, P < .01). This did not affect the median length of DGF, which was similar between the 2 groups (5 [interquartile range (IQR) = 2-11] versus 5 [IQR = 4-11], P = .74). Among the IBW cohort, 5% of patients (n = 6) were maintained on steroid-sparing immunosuppression regimens after transplant versus 0% of patients in the ABW cohort (P = .01), secondary to the option of early steroid withdrawal being implemented during the IBW cohort era.
Demographics and Clinical Characteristics of Study Population.
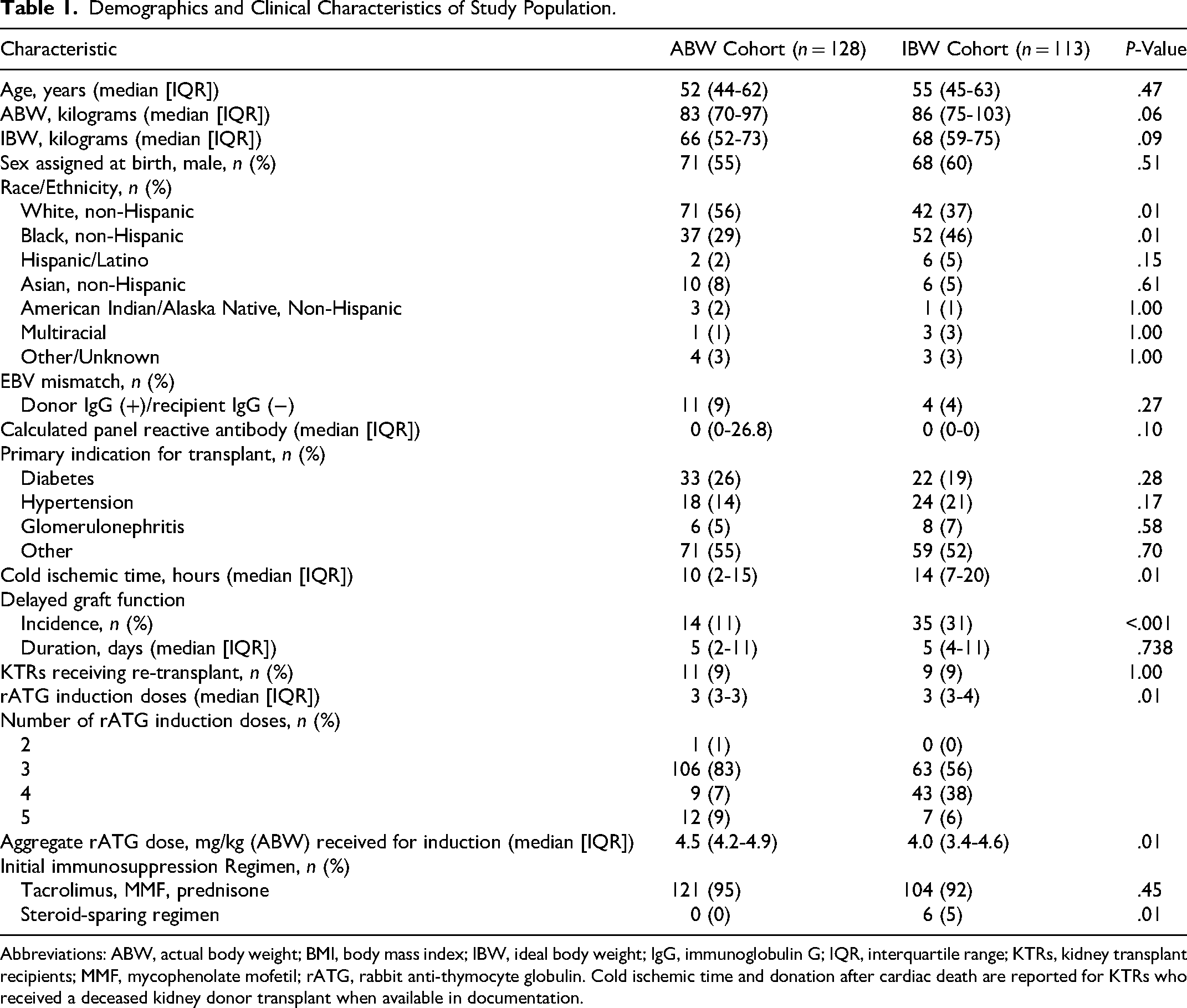
Abbreviations: ABW, actual body weight; BMI, body mass index; IBW, ideal body weight; IgG, immunoglobulin G; IQR, interquartile range; KTRs, kidney transplant recipients; MMF, mycophenolate mofetil; rATG, rabbit anti-thymocyte globulin. Cold ischemic time and donation after cardiac death are reported for KTRs who received a deceased kidney donor transplant when available in documentation.
Primary Economic Endpoint
Cost data based on AWP is summarized in Figure 2. Using IBW-based dosing compared with ABW-based dosing resulted in a statistically significant median cost-savings of $3838 per patient (comparing doses actually received, P = .02). This difference remained statistically significant when considering estimated costs from the alternative dosing strategy for each cohort (P < .01).
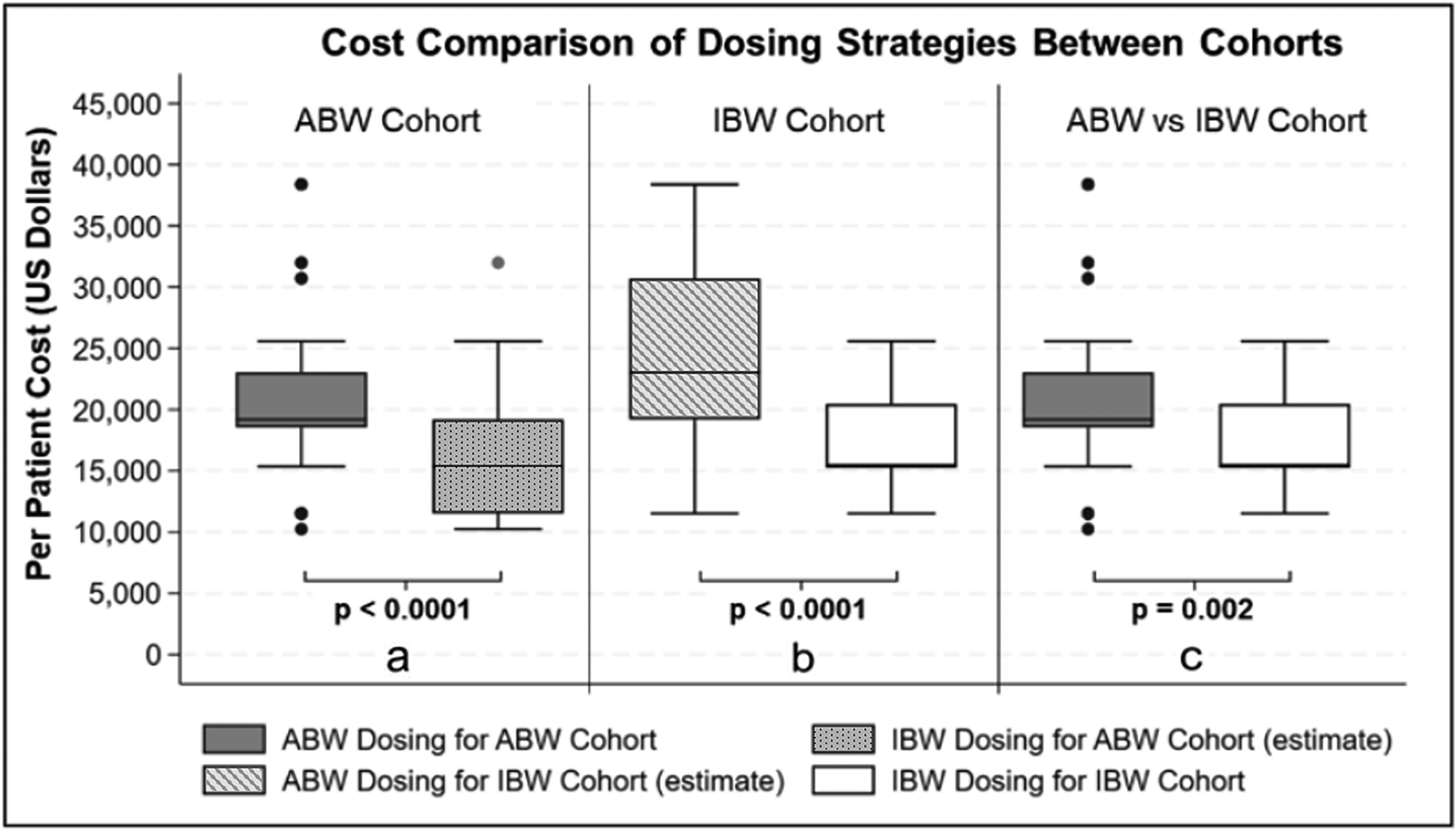
Summary of drug-related costs based on AWP for each cohort is shown in the graph below. Panel (a) compares ABW-based dosing cost with the estimated IBW-based dosing cost for the ABW cohort. Panel (b) compares the estimated ABW-based dosing cost with the IBW-based dosing cost for the IBW cohort. Panel (c) compares the actual costs between the ABW and IBW cohorts. Dosing of rATG was always rounded to the nearest commercially available 25-mg vial when doses were calculated for each cohort.
Primary Clinical and Tolerability Endpoints
Clinical outcomes are summarized in Table 2. Overall, there were comparable rates of BPAR at 6 months (2% vs 4%, P = .48). Regarding the comparison of tolerability between the 2 regimens, overall, there were comparable rates of leukopenia (20% vs 26%, P = .28) and neutropenia (21% vs 26%, P = .45) between the cohorts. Of note, patients in the ABW cohort experienced a lower rate of EBV viremia compared with the IBW cohort (4% vs 12%, P = .02), but this effect did not translate into a higher rate of readmissions for treatment of an infection (20% vs 13%, P = .23). As reported in Table 1, the ABW cohort had a higher proportion of patients with EBV immunoglobulin G (IgG) donor (+)/recipient (−) status (9%) compared with the IBW cohort (4%), although this difference was not statistically significant (P = .27).
Clinical Outcomes for Study Cohort.
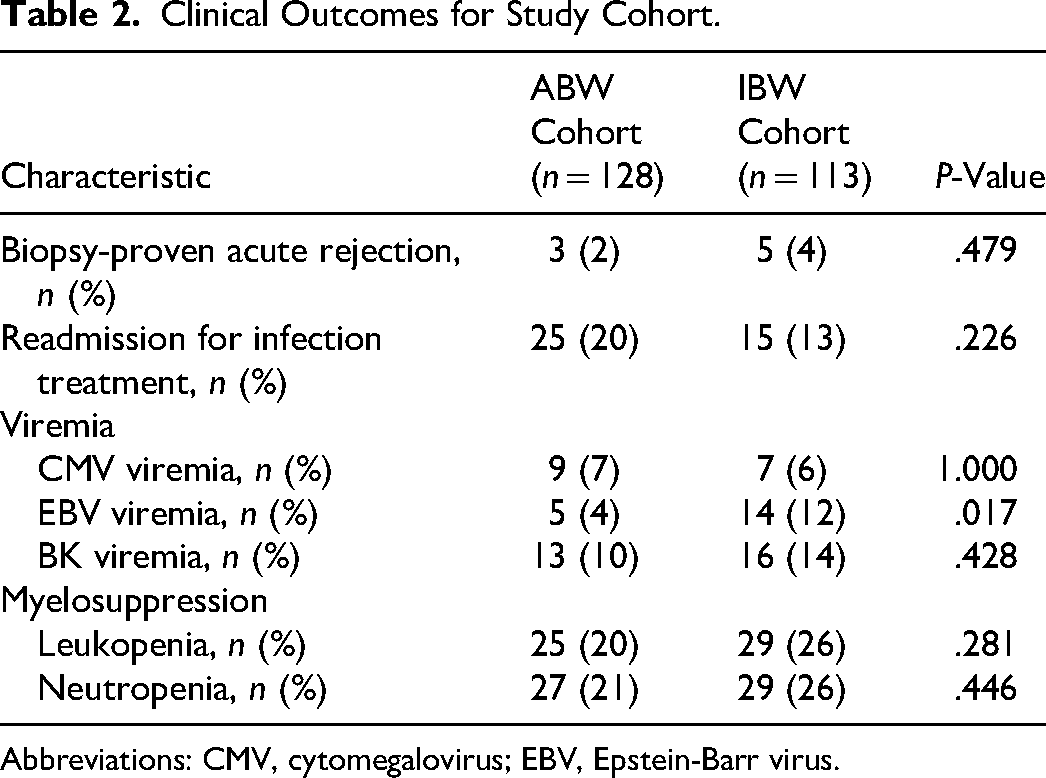
Abbreviations: CMV, cytomegalovirus; EBV, Epstein-Barr virus.
Discussion
Based on this analysis, IBW-based rATG dosing conferred a significant cost-savings benefit over ABW-based dosing, calculated using AWP, and did not compromise commonly reported transplant clinical outcomes or affect tolerability. Incidence of BPAR was relatively low overall and similar in both cohorts. Other factors, specifically medication nonadherence to the maintenance immunosuppression, could have contributed to BPAR, but this was not directly measured as part of the review.
Although there was a higher incidence of EBV viremia seen in patients in the IBW cohort, this did not result in an increase in readmissions, potentially indicating a milder presentation. Interestingly, further review of pretransplant characteristics revealed that the ABW group had higher rates of donor to recipient EBV IgG serology mismatch.
While there was a higher incidence of DGF in patients in the IBW cohort than the ABW cohort, patients in the IBW cohort receiving a deceased kidney donor transplant also had a more prolonged median cold ischemic time, comparatively. Consequently, the difference seen in DGF may be attributable, at least in part, to the circumstances of donation rather than the choice of induction immunosuppressant. The IBW cohort was transplanted in the era after the enactment of the Kidney Allocation System (KAS 250), occurring in March 2021. This new allocation process was shown to increase both cold ischemia times and rates of DGF.9,10
The findings in this study are in line with those of Bubik et al, who reported a cost-savings benefit when transitioning to IBW-based dosing, based on their institutional acquisition cost. 5 Of note, the use of institutional costs compared with the use of AWP results in a variance in terms of the magnitude of cost savings calculated. The per-patient savings calculated in this review are slightly higher compared to those of previous studies, which may be attributable to a larger sample size and variability in the number of doses patients received (ie, Bubik et al: 4 rATG doses vs current population: 3-5 rATG doses). In terms of rejection, the reported rejection rate was lower in this review, but Bubik et al also included rejections without biopsy confirmation. Finally, in the current population, patients were only included if they were dosed according to the specific protocol guidance, ensuring a direct comparison of the dosing strategy. In contrast, Bubik and colleagues reported a 77% IBW-based protocol adherence rate. 5
The study by Vacha et al found a cost savings benefit when transitioning to IBW dosing from ABW dosing. However, this cost savings benefit noted by Vacha et al was not statistically significant, unlike the findings of the current study. 4 Notably, the precise value for cost was not specified in the previous report, which could represent a variance in terms of the magnitude of cost savings in comparison with the current review. Unlike this cohort, Vacha et al assessed patients considered “high immunologic risk,” whereas this review did not distinguish based on that factor. Regarding clinical outcomes, Vacha et al identified similar rates of BPAR between patients receiving either ABW or IBW dosing, in alignment with this report. 4
Limitations
Even though this retrospective review included a relatively large sample size, there are a few notable limitations. In particular, the design was retrospective, and patients were not matched between cohorts. As a result, there may be inherent differences at baseline. Also, the absence of chart documentation could have resulted in missing data. However, outcomes were considered in the context of the presence or absence of each endpoint (eg, incidence of myelosuppression), thus limiting the impact of missing data.
Findings from this large single-center population over the first 6 months after transplant may not apply to KTRs at other centers. For instance, it is common for individual institutions to negotiate discounts with drug manufacturers, thus impacting the reported benefits of this review. The current study's choice to compare drug acquisition costs based on AWP, representing publishable drug prices accessible for reference, instead of institution-specific prices, was aimed at standardizing comparisons. Additionally, the number of doses administered to each patient could affect the overall results, particularly for patients with larger body habitus. As expected, the ABW cohort received a significantly higher aggregate dose for induction, despite there being a trend in higher ABW among the IBW cohort. However, the effects of such variability were balanced, given that the analysis of costs for each cohort used to estimate an alternative dosing strategy showed a similar significant reduction in costs.
Under the institutional protocol, patients are prescribed doses in a range between 3 and 5 doses, based on pretransplant sensitization. The IBW group more frequently received 4 doses of rATG for induction immunosuppression, although the same protocol was used during both eras. As illustrated in Table 1, there was no significant difference in pretransplant cPRA levels or rates of retransplantation. However, there were significantly more Black/non-Hispanic recipients in the IBW cohort. This characteristic accounted for more frequent use of 4 rATG doses. Also, maintenance medications might have been adjusted throughout the course of the 6-month follow-up period, with agents held in the setting of myelosuppression given their potential causality (eg, valganciclovir). As a result, some of these effects may have been iatrogenic instead of directly attributable to the persistent lymphodepleting effects of rATG.
Regarding clinical outcomes, the benefit of IBW versus ABW rATG dosing was assessed using established outcomes, specifically BPAR. Alternative laboratory results cited in the literature for assessing rATG doses, but not collected in this review, also include monitoring absolute lymphocyte counts or flow cytometry. Similarly, when considering drug-related costs in economic endpoints, other healthcare aspects are intertwined with the drug acquisition costs, such as costs related to administration, hospital length of stay, and management of adverse drug effects. Secondly, with regard to the retrospective design of the review, these results were not included in the data collection. Lastly, the review only evaluated early postoperative outcomes, specifically the 6-month follow-up period, given that these were most directly impacted by the induction immunosuppression patients received, and not long-term outcomes.
Conclusion
The results of this retrospective review support the use of IBW-based dosing for rATG induction of recipients, based on drug purchasing cost-savings and similar 6-month BPAR rates. For example, a transplant center that converted to IBW dosing instead of ABW dosing of rATG and performed 250 kidney transplants annually would result in an estimated annual drug cost-saving of $900 000, assuming most recipients receive rATG induction.
Footnotes
Abbreviations
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jennifer Trofe's institution has received research funding from Veloxis Pharmaceuticals for a separate study initiative, none of which was used for study design, performance, data analysis, or manuscript preparation of this study.
Abigail Forte is currently an employee of HealthMap Solutions; the work contained within this article was performed prior to this affiliation and is independent of HealthMap Solutions.
Data Availability Statement
The data from this retrospective review are available based on a reasonable request.