
Abstract
The growth in undocumented immigration in the United States has garnered increasing interest in the arenas of immigration and health care policy reform. Undocumented immigrants are restricted from accessing public health and social service as a result of their immigration status. The Patient Protection and Affordability Care Act restricts undocumented immigrants from participating in state exchange insurance market places, further limiting them from accessing equitable health care services. This commentary calls for comprehensive policy reform that expands access to health care for undocumented immigrants based on an analysis of immigrant health policies and their impact on health care expenditures, public health, and the role of health care providers. The intersectional nature of immigration and health care policy emphasizes the need for nurse policymakers to advocate for comprehensive policy reform aimed at improving the health and well-being of immigrants and the nation as a whole.
The United States has seen an exponential growth in its immigrant population over the years. According to the U.S. Bureau of the Census (2008), the foreign-born population has grown from 9.6 million (4.7% of the total population) in 1970 to 38 million (12.6% of the total population) in 2007 and is estimated to represent 15% of the U.S. population by 2015. The foreign-born population disproportionately experiences higher rates of poverty and lower levels of education, lacks health care coverage, and receives fewer health services when compared with their U.S.-born counterparts (U.S. Census Bureau, 2007a, 2007b). Although there are similarities between disparities faced by immigrants and those in low-income families, immigrants are further limited to accessing health care due to extraneous factors, including immigration and health policy reform that has occurred over the past two decades. Many of these policy changes that occurred as a result of sociocultural, economic, and political mechanisms emphasized the need to curb the rates of undocumented immigrants in the United States. As a result, undocumented immigrants have become the focus of many political and policy debates that restrict their eligibility for several public services and limit their access to health care.
The Patient Protection and Affordable Care Act (PPACA, 2010) further emphasizes restrictions on access to health care for undocumented immigrants, causing heightened concerns among health care providers and policymakers nationwide. The purpose of this commentary is to examine the role of past, current, and future policymaking as an explanation for disparities in health care access among undocumented immigrants in the United States, making a case for policy reform to increase access to health care, expand health insurance coverage, and improve health outcomes for this growing, disadvantaged population. Expanding access to health care services and insurance coverage can significantly decrease health disparities and improve health outcomes for undocumented immigrant groups and the community at large. Fitting to its definition, this commentary aims to increase awareness and garner support from nurses and other health-related policymakers to support the expansion of health care access for undocumented immigrants in the United States by providing evidence for the impact of policy on reducing health disparities.
Undocumented Immigrants and Access to Health Care
According to the Pew Hispanic Center (2013), there were an estimated 11.7 million undocumented immigrants residing in the United States in 2012, the majority of whom resided in California (2,450,000), Texas (1,700,000), Florida (950,000), and New York (875,000). Roughly 80% of undocumented immigrants come from Mexico and other Latin American countries, followed by Asia (11%), Europe and Canada (4%), and Africa and other countries (4%).
As a highly heterogeneous group, immigrants represent not only a wide array of ethnicities but also a variety of socioeconomic and legal statuses that often affect their ability to access health care (Derose, Bahney, & Lurie, 2009). The three main legal status groups that include approximately one third of immigrants respectively are naturalized citizens, permanent residents, and undocumented immigrants (Derose, Escarce, & Lurie, 2007). Undocumented immigrants are individuals who reside in the United States without federal documentation authorizing them to enter, reside, and work in the country. Most often, overstaying the designated time of a federally authorized visa or failing to renew visas results in the undocumented status. This immigration status determines their ability to access equitable social and health services.
Access to Health Care
Access to health care is generally defined as the timely and appropriate use of health services to achieve the best health outcomes (Centers for Disease Control and Prevention, 2011; Institute of Medicine, 2003). Examining access to health care among immigrants is an important and timely issue as a result of the growing health disparities related to inequitable health care access in this underserved population. Several studies have shown that immigrants are less likely to seek out or spend on health care, interact with the health care system, or have health insurance coverage compared with U.S.-born citizens (Derose et al., 2009; DuBard & Massing, 2007; Goldman, Smith, & Sood, 2006). The literature identifies immigration status, especially being undocumented, as having significant influences on both access to health care and health outcomes (Durden & Hummer, 2006; Khan, Velazquez, O’Connor, Simon, & De Groot, 2011; Quesada, Hart, & Bourgois, 2011).
Lack of legal immigration documentation affects the vulnerability of the undocumented population, limiting their access to health and social services equivalent to their legal counterparts (Aday, 2001). Other sources of vulnerability for immigrant groups include socioeconomic background, language barriers, discrimination and marginalization, and federal welfare provisions. Immigrants’ access to health care is largely impeded by socioeconomic factors that are influenced by lack of education, type of occupation, and income. According to the Kaiser Commission on Medicaid and the Uninsured (2003), immigrants with lower levels of education and limited English proficiency are more likely to be poor and work for small businesses, agricultural, labor, repair industry, and other service occupation sectors. Studies have shown that immigrants with limited English proficiency are less likely to have health insurance and seek health services than those who speak English (Ponce, Hays, & Cunningham, 2006; Yu, Huang, Schwalberg, & Nyman, 2006). Additionally, limited knowledge about existing services and lack of sufficient income lead to disparities in accessing health services among immigrants (Derose et al., 2009). Due to the lack of communication between health care providers and immigrants, quality of care and patient safety have also shown to be negatively affected.
Among undocumented immigrants, issues of discrimination and marginalization significantly impede access to services, making immigrants reluctant to seek care due to concerns of unequal treatment or deportation (Lauderdale, Wen, Jacobs, & Kandula, 2006). With the recent implementation of state-enforced immigration laws, immigrants are further restrained from accessing public services. Furthermore, undocumented immigrants cannot obtain Social Security numbers and other forms of federally authorized identification, which is often required to access public health services and health insurance.
Health Insurance Coverage
Health insurance is a significant determinant of health care access and has been directly associated with health outcomes such as chronic illnesses and mortality among immigrants (Khan et al., 2011; Wilper et al., 2009a, 2009b). Undocumented immigrants commonly work in low-level service industry and other low-skilled jobs, which do not provide adequate compensation for health insurance coverage (Passel & Cohn, 2009). Additionally, factors such as immigration status have such extensive effects on acquiring health insurance coverage that discrepancies in access continue to exist despite rises in income levels (Siddiqi, Zuberi, & Nguyen, 2009).
In 2007, the Center for Immigration Studies estimated that roughly 34% of all immigrants (legal and undocumented) in the United States lack health insurance coverage, accounting for 27% of the total uninsured population (Camarota, 2009). Apart from eligibility issues that impede immigrants’ access to health care, lack of health insurance coverage has been a central issue of policy and political debates. The effect of undocumented immigrant status further impinges on the ability to acquire health insurance, especially with the establishment of immigration laws and regulations. Generally speaking, undocumented immigrants are not entitled to receive health care and other federally funded, public welfare programs, posing a severe threat to the health of immigrants and the nation as a whole (Goldman et al., 2006; Torres-Cantero, Miguel, Gallardo, & Ippolito, 2007).
With the recent economic downturn, further steps have been taken to reduce health care expenditures while continuing to provide adequate coverage for U.S. citizens and legal immigrants. However, undocumented immigrants have been restricted from obtaining these services due to the common misconception that they incur higher health care costs than nonimmigrants. Recent studies have attempted to dispel these beliefs, indicating that undocumented immigrants may not be contributing to the increase in health care costs in the United States and that addressing health care needs of this population could in fact reduce expenditure (Mohanty et al., 2005; Stimpson, Wilson, & Eschbach, 2010). These findings support the need to repeal laws that restrict immigrants’ access to health care and promote policies that improve access to health services.
Policy Implementation
The issue of health care for undocumented immigrants has broad sociocultural, economic, and political implications and is largely affected by immigrant and health policy reform. Although necessary, collaborative policy implementation between immigration and health sectors is often unfeasible due to the differences in foci and complexities of agenda setting between administrative structures and policymaking bodies. This is especially true when comparing the focus of policymaking between immigration and health sectors, respectively.
Over the years, immigration policies have focused on curbing undocumented immigrants from residing in the United States. Following the September 11 attacks, federal law enforcement agencies responded through the mechanisms provided by the Congress and the U.S. Department of Justice to enlist police in the enforcement of immigration laws (Wishnie, 2004). In 2010, the Support Our Law Enforcement and Safe Neighborhoods Act was passed in Arizona, giving law enforcement officers the authority to determine the immigration status of individuals if they have “reasonable suspicion” that the immigrant is unauthorized to reside in the United States (S.B. 1070, 2010, p. 4). Similarly, the Personal Responsibility and Work Opportunity Reconciliation Act (PRWORA) of 1996 served as a mechanism to restrict immigrants from accessing health care through Medicaid and other publicly funded services (Derose et al., 2007; Okie, 2007; PRWORA, 1996). These policies, among several others, have changed the face of immigration in the United States, leading to limited access to vital services for immigrants and causing additional strain in health care systems (Sonfield, 2007).
The health care sector, on the contrary, has continually focused on health policies that reduce health disparities and provide equal access to health services and insurance coverage, in an attempt to improve the health of the overall community. The PPACA of 2010 was the current administration’s effort for health care reform that requires all citizens and legal immigrants to have health insurance coverage. However, undocumented immigrants are restricted from accessing federally funded services and insurance coverage, creating additional barriers to accessing care. Arguments can be made regarding the reasons for this stipulation as being related to decreasing the financial burden on the federal system and as a means of defusing anti-immigration opposition to the PPACA. Inconsistencies between immigration and health reform policies that occur as a result of the controversial aspects of undocumented immigration create a gray area in policymaking. Ambiguity in immigration policies related to the stipulation of authorized immigration status to access services further deters any advancement in the provision of health care for this population. As policies play a central role in establishing changes in arenas of immigration and health, it is imperative to advocate for comprehensive policy reform to remove restrictions and improve immigrants’ access to health care services and insurance coverage.
Impact on Health Care Expenditures, Public Health, and Practice
As the immigrant population continues to grow in the United States, it has become imperative to address the issue of health care access and coverage in improving health outcomes of this population. Expanding insurance coverage for undocumented immigrants is also essential in addressing the rates of uninsured in the United States (Kaiser Commission on Medicaid and the Uninsured, 2003). Siddiqi et al. (2009) found compelling evidence supporting the provision of health insurance coverage as an effective method for reducing immigrant disparities in accessing health care. The introduction of the health care reform act, which restricts undocumented immigrants from purchasing health insurance through the state exchanges, has led to intense debates among policy reform advocates in immigration and health care sectors. The rippling effects of these restrictions can be seen throughout the health care system and have shown to significantly impact health care expenditures, public health, and the role of health care providers.
Health Care Expenditures
Immigrants are less likely to access health care services, resulting in significantly fewer dollars per capita for health care (Mohanty et al., 2005). Undocumented immigrants account for only 1.5% of total U.S. medical costs, which predominantly incur from visits to emergency departments (DuBard & Massing, 2007; Okie, 2007). However, Mohanty et al. (2005) found that children of immigrants have higher per capita expenditures for emergency department visits compared with native-born children. By law, hospitals are obligated to provide medical treatment to everyone who presents to the emergency room with an emergent condition regardless of ability to pay, health insurance coverage, or immigration status (Grimm & Wells, 2009). Therefore, the cost that incurs from unpaid emergency department bills usually becomes the responsibility of hospitals, increasing overall costs and expenditures of the health care system. Similarly, costs incurred from provision of health and social services to undocumented immigrants become the responsibility of state and local governments, who often do not receive adequate federal support and resources to meet this growing demand (Footracer, 2009). Due to insufficient health insurance coverage, undocumented immigrants are unable to afford their health care costs, resulting in unreimbursed expenses for hospitals.
The Immigration Policy Center (2009) argues that overall health care costs can be reduced when a larger number of people pay into the new health care system as proposed by the PPACA. Undocumented immigrants are restricted from purchasing health insurance through the health reform state exchanges due to their immigration status. Excluding undocumented immigrants from purchasing health insurance from the state exchanges and barring them from subsidies can be detrimental to others who are paying into the system. According to the National Immigration Law Center (NILC, 2009), exchanges will be more expensive due to the lack of distribution among all those utilizing the health care system. Others (Majority Staff, Committee on Oversight and Government Reform, 2007; Ross, 2007) argue that taxpayer dollars should not be wasted on immigration status verification systems and other documentation schemes that create additional barriers for those who need health care. Instead, policy reform must change its focus from enforcing exclusionary immigration laws to finding ways to include immigrants in the health care system.
Public Health
As a result of the cultural, economic, and legal barriers to health care access, immigrants are more likely to access emergent as opposed to preventive health care, delaying early detection and prevention of illnesses. Studies have shown that immigrants are less likely to have a primary care provider or other regular source of health care, which results in delays in seeking care for more than 1 year (Guendelman, Schauffler, & Pearl, 2001; Lasser, Himmelstein, & Woolhandler, 2006). Advances in the stages of the disease process that are left undetected can pose serious threats to the health and well-being of the community as a whole while consequently increasing health care expenditures.
Access to preventive health care services improves community health and reduces health care expenditures. However, studies have shown that immigrants are less likely to access or utilize preventive services, especially in areas of cancer screening, vaccinations, and pediatric and prenatal preventive care (Cohen & Christakis, 2006; Echeverria & Carrasquillo, 2006; Goel et al., 2003; Lees, Wortley, & Coughlin, 2005). Prenatal and pediatric preventive measures have shown to be effective in improving health outcomes of children in a cost-effective manner (Cohen & Christakis, 2006). Carrasquillo, Carrasquillo, and Shea (2000) state that providing prenatal care for undocumented immigrants would lead to a decrease in the rates of prematurity, low-birth-weight babies, and related postnatal costs. Therefore, improving access to health care services for undocumented immigrants can have significant impacts on health indicators for the nation as a whole.
Role of Health Care Providers
Health care providers are obliged to follow their respective codes of ethics that generally address justice, nondiscrimination, and confidentiality in the provision of health care for all people (Mappes & Degrazia, 2006). As a result, several professional organizations such as the American Medical Association (AMA), American College of Physicians (ACP), and the American Nurses Association (ANA) oppose laws that restrict provision of health care to undocumented immigrants or require providers to report undocumented immigrants (Footracer, 2009). The ANA (2001) code of ethics states that nurses are required to practice with “compassion and respect for the inherent dignity, worth, and uniqueness of every individual, unrestricted by considerations of social or economic status, personal attributes, or the nature of health problems” (p. 1). In adhering to the ethical principles of their practice, nurses are often faced with the ethical dilemmas of withholding health care services or documenting and reporting immigration status when treating undocumented immigrants.
As patient advocates, nurses and other health care providers are obligated to provide care to all those in need, regardless of immigration status (Grimm & Wells, 2009). However, without valid immigration documentation and Social Security numbers, undocumented immigrants are restricted from accessing health care services. The primary goal of health care providers is to improve the overall health and well-being of the community. This can be achieved by providing equal access to health services and insurance coverage and through active engagement in health policy reform. Over the years, nurses have become increasingly active in health policymaking and implementation that focuses on eliminating health disparities and providing equal access to health care for immigrants. With the introduction of the PPACA, nurse policymakers are faced with new challenges in addressing the health care needs of immigrants, especially the undocumented. Effective health policy reform is imperative to overcome barriers to health care access for undocumented immigrants. Understanding the pivotal events that have shaped policymaking over the years is essential for future health policymakers who aim to address current and future needs of immigrants.
Past Policies
Addressing issues related to unauthorized immigration has been an ongoing struggle for policymakers both in immigration and health care (Sonfield, 2007; Wishnie, 2004). Over the years, the increase in terrorist threats in the United States has led to heightened levels of anti-immigrant rhetoric, which inevitably intersects with debates over the provision of public services to undocumented immigrants. Although inaccurate, increased blame has been placed on immigrants for the increase in health care expenditures (Mohanty et al., 2005; Stimpson et al., 2010). Attempts to address these community concerns have been viewed as more of a political strategy rather than a public welfare concern. As a result, numerous changes have been established in immigration and health care reform policies over the past two decades. The following section will highlight several central policies that changed the course of immigration and health care in the United States.
1990s
The Immigration Act of 1990 changed the admission and priority levels of immigrants, bringing a significant influx of immigrants to boost the workforce and economy of the United States. As levels of diversity started to increase, disparities in socioeconomic status and health correspondingly increased in the community. Federal and state legislatures turned their focus to immigration reform in an attempt to curb the rates of unauthorized immigration in the United States. With the option of being more restrictive than the federal government, states continued their efforts to further restrict immigrants from accessing state-wide public services (Sonfield, 2007). The first wave of anti-immigration policies started with Proposition 187, which was passed in California to prohibit undocumented immigrants from accessing any public services, including health care and education. Although this law was later deemed unconstitutional and overturned by a federal court because it gave Congress exclusive jurisdiction over immigration policy, several states continued to exercise their ability to exclude undocumented immigrants from accessing public services.
In 1996, PRWORA restricted legal immigrants from accessing federally funded health services through Medicaid by delaying eligibility until permanent resident status was attained for 5 years (Derose et al., 2009). Undocumented and nonpermanent residents were denied benefits through Medicaid. Although 25 states provided full coverage for immigrants who did not qualify for Medicaid or State Children’s Health Insurance Program (SCHIP) in 2004, studies have shown that states that failed to meet this gap resulted in poor access to health care for immigrants (Borjas, 2003; Kaushal & Kaestner, 2007). Despite budget constraints, several states managed to provide health care through public services for ineligible immigrants. However, these attempts were short-lived as a result of the next wave of immigration and health policy reform in the 2000s.
2000s
The Deficit Reduction Act (DRA) of 2006 required both state and local Medicaid agencies to obtain proof of citizenship and identity from those who applied for these services. According to Sonfield (2007), the DRA was passed by Congress in an attempt to preserve services for citizens by reducing levels of fraud by undocumented immigrants. Interestingly, evidence suggested that a significant threat of fraud by immigrants did not exist, shedding light on alternative motives of the DRA (Ku & Pervez, 2010). Sonfield predicted that an estimated 1 to 2 million, low-income American citizens will be forced to delay care and eligibility through Medicaid due to the difficulties and associated costs in obtaining documentation. More recent literature supports this projected trend, indicating that documentation requirements for Medicaid eligibility have delayed access to vital health care services for eligible citizens and documented immigrants, resulting in additional strains on the health care system (Angus & Devoe, 2010; Bauer et al., 2011; Repasch, Finnegan, Shin, & Rosenbaum, 2008).
As a result of the DRA, state laws were modified in attempts to further restrict or expand immigrants’ eligibility for certain public services. Documented immigrants must now wait for 5 years to be eligible for Medicaid and the Children’s Health Insurance Program (CHIP; Centers for Medicare and Medicaid Services, 2010). The latest modifications to Medicaid and CHIP allow states to waive the 5-year waiting period for lawfully residing pregnant women and children, which 24 states have established since January 2012 (Kaiser Commission on Medicaid and the Uninsured, 2012). Despite these changes, undocumented immigrants continue to be exempt from accessing public services due to the lack of valid immigration paperwork. States continue to struggle with expanding coverage for documented and undocumented immigrants while meeting federal laws and regulations. Similarly, the PPACA has introduced additional challenges to the dilemma of equitable access to health care services for immigrants.
Current Policies
Health Care Coverage Eligibility for Legal and Undocumented Immigrants.
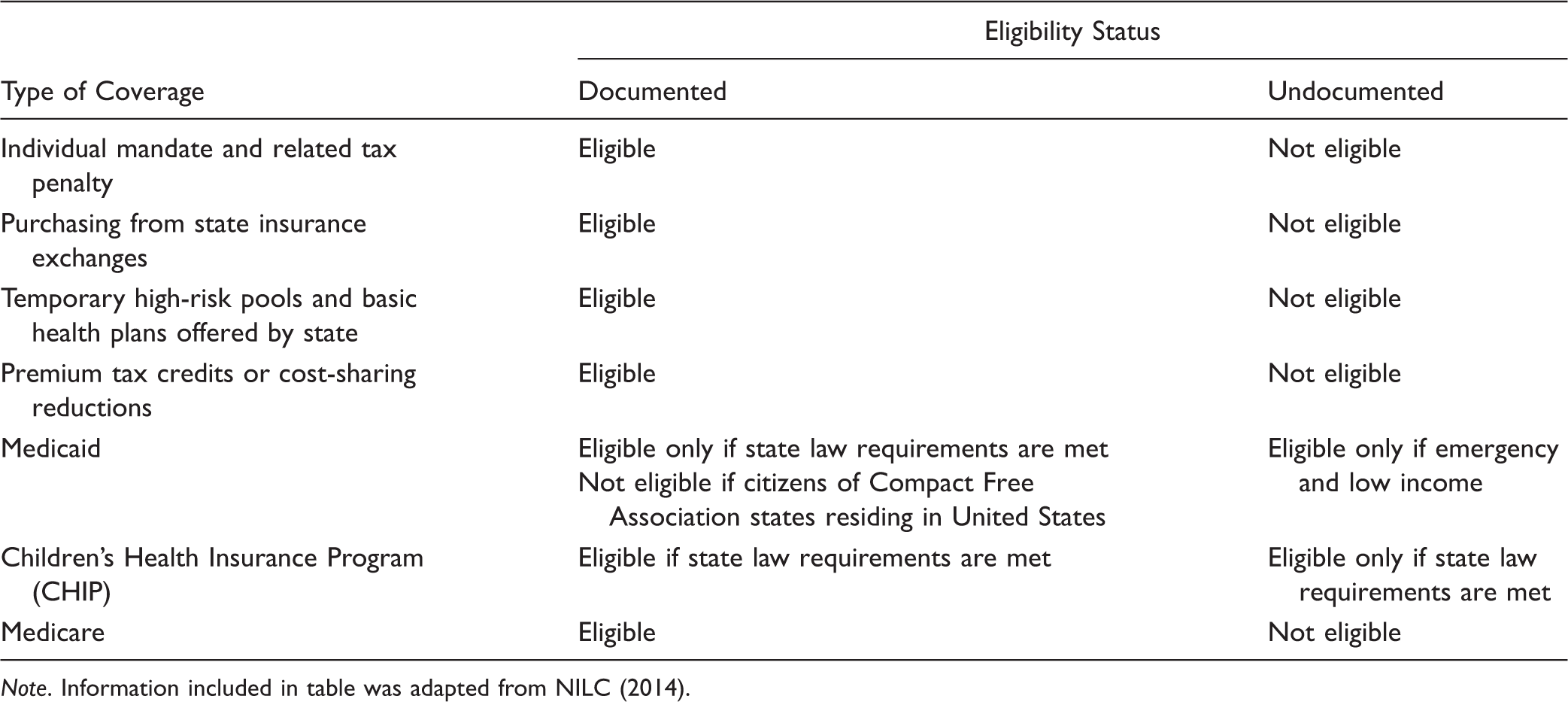
Note. Information included in table was adapted from NILC (2014).
The health care reform act establishes several barriers to federally funded health care programs and insurance coverage for undocumented immigrants. This population is exempt from health insurance exchanges even if they are able to pay out-of-pocket. Despite the lack of restraints on accessing emergency services, undocumented immigrants are less likely to utilize emergency services than U.S.-born citizens (Huang, Yu, & Ledsky, 2006). With the establishment of these new laws, undocumented immigrants are further discouraged from seeking health care due to fears and confusion over rules of eligibility (California Immigrant Policy Center, 2006). Restricting access to health care places increased danger on public health and results in higher health care costs. Realization of these negative consequences has caused concern among health care providers and policymakers, highlighting the need for immigrant health policy reform.
In 2012, in an attempt to move immigration reform forward, President Obama signed a memo establishing Deferred Action for Childhood Arrivals (DACA), one of the foundational provisions of the Development, Relief, and Education for Alien Minors Act (S. 1291, 2001). The DREAM Act is aimed at providing amnesty to young, undocumented youth based on levels of educational attainment and military service. Deferred action grantees are lawfully permitted to work but do not gain legal immigration status and consequently are ineligible for access to Medicaid, CHIP, and other benefits from the PPACA (NILC, 2014). Issues pertaining to expansion of access to public health and social services for this population have yet to be discussed in detail (Ross, 2007). The DREAM Act has not been passed in its entirety due to opposition from various public leaders and political parties. Local advocacy groups continue to fight for equal rights and justice for the undocumented community. The stalemate in immigration reform has discernible influences on health policy and consequently on health care access for undocumented immigrants.
Future Policy Recommendations
The intersectional nature of immigration and health care reform indicates the need for future policies that focus on improving access to care for undocumented immigrants. Both health economics and public health perspectives support the need for health policy reform that provides equitable access to health care services and insurance coverage (Nandi, Loue, & Galea, 2009). Providing better access and quality of care for immigrants benefits the community as a whole, signifying the need for collaboration of policymakers from different public sectors, especially immigration and health care.
Various international and national health professional organizations such as the International Council of Nurses (2006), the ANA (ANA 2010 House of Delegates, 2010), and the ACP (2011) have voiced their support for the provision of health care services for immigrants, including the undocumented. The ANA reaffirmed its longstanding position in support of the provision of health care for all individuals residing in the United States despite their immigration status. The ACP calls for a national immigration policy that addresses expansion of health care for immigrants and currently leads the way in immigrant health policy reform in the United States. It is recommended that other health professionals, especially nurses in public health and policymaking, support the implementation of policies that focus on improving undocumented immigrants’ access to health care by joining forces with professional organizations that support this cause.
Nurses and nurse policymakers are quintessential patient advocates and have been instrumental in improving community health and equity in health care access through various active roles in lobbying and policy implementation and evaluation. This commentary makes recommendations for nurses to increase their focus on policy reform aimed at reducing the vulnerability of undocumented immigrants by expanding health insurance coverage and safety-net infrastructures, decreasing barriers to accessing care, and revising the current provisions of the PRWORA and the PPACA (Derose et al., 2007). To expand access to health services, it is imperative for future policies to address the need for increased funding of public programs, community health centers, and organizations that provide free or subsidized care to immigrants. The establishment of the health care reform act calls for policies aimed at increasing employer-provided health insurance in immigrant employment sectors that will both expand health coverage and encourage health-seeking behaviors (Buchmueller, Lo Sasso, Lurie, & Dolfin, 2007).
To reduce language barriers and promote health-seeking behaviors among immigrants, federal funding should be allocated to provide interpreter services in primary care centers and to develop educational programs for bilingual proficiency among health care providers. According to Derose et al. (2007), policymakers should reconsider provisions that were set forth by PRWORA. Restricting immigrants from Medicaid but allowing them to access emergency Medicaid services can have a significant impact on deterring preventive health behaviors among immigrants, eventually leading to the overburden of the health care system and jeopardizing the health of the broader community.
Conclusion
This commentary makes a case for policy reform that expands access to health services and insurance coverage for undocumented immigrants. An analysis of past, current, and future immigrant health policy changes and the implications of these policies on quality and cost of health care provide a basis for comprehensive immigration and health policy reform to expand health care access for undocumented immigrants. With the establishment of the PPACA, policymakers have shown concern for the exclusion of undocumented immigrants in the new health care model. It is evident that restricting this population from receiving equal access to care can have several negative repercussions on health care costs and community health.
Policymakers have a limited window of opportunity to evaluate the effects of the PPACA in its early stages of implementation and recommend appropriate changes to expand health insurance coverage and access to health care services for undocumented immigrants. During this time, it is essential to increase awareness about the unjust exclusion of undocumented immigrants from receiving the basic human right of health care. Nurses and other health care providers are urged to take action by supporting policies aimed at expanding health care access for undocumented immigrants by collaborating with national and international professional organizations and other policymaking bodies. The future health and well-being of immigrants and the nation as a whole lies in the hands of policymakers, whose influential roles can establish health policy reform to expand equitable access to health care for all.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.