
Abstract
The provision of reproductive health services (RHS) by school-based health centers (SBHCs) is the subject of much controversy. Ideological differences about the role of schools in health care and the sexual activity of youth frame this debate. The purpose of this study was to determine the perspectives of key stakeholders related to access to RHS in SBHCs. Individual, semistructured interviews were conducted with 50 adult stakeholders. Template analysis yielded rich answers to the interview questions. Nine overarching themes emerged during thematic analysis. Subthemes and exemplar quotes revealed important insights into public opinion about RHS at SBHCs. Findings reflect strong stakeholder support for the inclusion of RHS in SBHCs as a way to promote teen sexual health. Nurses have an important role in influencing policies related to teen reproductive health such as those addressed in this study.
Although teen pregnancy and birth rates are declining, Youth Risk Behavior Survey data reveal high rates of youth sexual activity and varying degrees of engagement in safe sexual practices (Kann et al., 2014). Additional data reflect that teen pregnancy and teen birth rates continue to be high in selected populations of youth (Kost & Henshaw, 2013). High rates of teen sexuality, pregnancies, births, and sexually transmitted infections (STIs) prompted school-based health centers (SBHCs) to consider providing or expanding reproductive health services (RHS) in the state of study. This research was designed to determine the perceptions of stakeholders, as a segment representing public opinion, about the provision of RHS by SBHCs.
SBHCs traditionally provide sports physical examinations, nutrition and mental health counseling, oral health care, and primary care screening and treatment (Lofink et al., 2013). Research demonstrates that SBHCs provide equitable, comprehensive, and teen-friendly care that may be most critical for those teens considered high risk (Anyon et al., 2013; Parasuraman & Shi, 2014; Stone, Whitaker, Anyon, & Shields, 2013; Yang & Gaydos, 2010). Some provide care only to students within a school, while others include family members, community members, and the general public in their client base (Lofink et al., 2013). RHS provided by SBHCs may include pregnancy testing, education about and referral or prescription for oral contraceptives, education about and distribution of condoms, classroom education programs, testicular and gynecological examinations, provision of emergency contraception, education about and prescriptions for other birth control methods, sexuality counseling and education, testing and treatment of STIs, and testing and referral for human immunodeficiency virus (HIV) treatment (Lofink et al., 2013; Sisselman, Strolin-Goltzman, Auerbach, & Sharon, 2012). A majority of SBHCs provide abstinence counseling and other educational/counseling services, but there is a high level of debate over the provision of condoms and contraceptives, HIV testing and treatment, and other more invasive interventions (Lofink et al., 2013).
Much of the current controversy related to RHS in SBHCs is rooted in how individuals, including parents, community members, school personnel, and teens, view adolescent sexual activity, the impact of access to RHS on sexual activity, and the role of schools in health care. Quantitative evidence in the literature demonstrates that teens and adults support the placement of RHS in the SBHCs that they already utilize for routine care (Richardson & Wright, 2012; Soleimanpour, Brindis, Geierstanger, Kandawalla, & Kuraender, 2008). Studies about the provision of RHS in SBHCs using qualitative methods are less represented in the literature than those relying on quantitative methods and guided the design of the research reported here.
Review of the Literature
The literature cogent to this study explores the debate surrounding the provision of RHS by SBHCs, the number of SBHCs providing RHS, teen and adult perceptions of RHS in SBHCs, and the impacts of the provision of RHS by SBHCs. The provision of RHS by SBHCs in most states, despite support from professional, medical, and nursing organizations, is characterized by controversy (Forke et al., 2011; Lofink et al., 2013; National Assembly on School-Based Health Care, 2008; Santelli & Kirby, 2010; Schmiedl, 2004). SBHCs were opened in the early 1980s, in part, to provide RHS as part of primary health-care services with the intent of reducing high rates of teen pregnancy (Daley, 2012; Kirby, 2002). Proponents of the provision of RHS contend that SBHCs provide health care that is medically sound, developmentally appropriate, easily accessible, and youth oriented (Forke et al., 2011; Santelli & Kirby, 2010; Schmiedl, 2004). Supporters of the provision of health care in schools, particularly RHS, stipulate that such access surmounts such barriers to access as cost, transportation, embarrassment, confidentiality, and complexity (Santelli & Kirby, 2010; Schmiedl, 2004). Researchers postulate that perhaps the greatest value of RHS provided by SBHCs rest in their ability to offer high levels of education and follow-up for RHS, along with providing ongoing monitoring, troubleshooting, and encouragement related to contraception and so necessary in the teen years (Harrison, Beebe, Park, & Rancone, 2003). Others offer that adolescents’ accessibility to family planning services in SBHCs is vital to continue to decrease teen pregnancy rates and is especially critical for selected groups of teens, including those of minority backgrounds or with special needs (Yang & Gaydos, 2010).
Those who oppose RHS in schools contend that contraception encourages sexual promiscuity, promotes abortion, undermines parental authority, oversteps the role of schools in the private lives of children and families, invades privacy, puts forth political agendas, and opposes fundamental religious beliefs (Santelli & Kirby, 2010; Wald, Button, & Rienzo, 2001; Williams, Litvak, & Moriarty, 2004). Some policy makers and stakeholders consider schools inappropriate sites for the provision of any health services, including RHS (Strolin-Goltzman, Sisselman, Melikis, & Auerbach, 2014). The provision of RHS by SBHCs is the most debated element of their care and often sets the stage for opposition to SBHCs (Broussard, 2002; Kirby, 2002; Rienzo, Button, & Wald, 2000; Wald et al., 2001; Williams et al., 2004).
Rates of SBHCs providing RHS consistently and steadily increased from 2000 to 2009 (Fothergill & Feijoo, 2000; Kohn, Hacker, Rousselle, & Gold, 2012; Santelli et al., 2003; Soleimanpour, Geierstanger, Kaller, McCarter, & Brindis, 2010; Strozer, Juszczak, & Ammerman, 2010). The 2007 to 2008 census report indicated that 70% of SBHCs provided counseling about birth control and 59% providing follow-up for contraceptive users (Strozer et al., 2010). Newer data indicate a slight decrease in the provision of RHS; the 2010–2011 survey of SBHCs revealed the following percentages of sites providing elements of care: 69% screened for and treated STIs, 82% abstinence counseling, 60% HIV screening and counseling, and 81% pregnancy testing (Lofink et al., 2013). In addition, 65% counseled about birth control and 52% provided follow-up for contraceptive users, although only 50.8% were able to dispense contraception at SBHCs (Lofink et al., 2013; Strozer et al., 2010).
Most SBHCs reported offering condoms, birth control pills, and medroxyprogesterone (Depo-Provera), a contraceptive injection, with fewer providing implanted contraceptive devices, intrauterine devices, and diaphragms (Fothergill & Feijoo, 2000; Kohn, Hacker, Rousselle, & Gold, 2012; Santelli et al., 2003). In another study, contraceptive services provided by SBHCs were by referral such that 82% of the sites surveyed provided some level of on-site counseling, screening, pregnancy testing, gynecological examinations, and STI services and clients were referred to outside agencies for contraception prescription or dispensing (Santelli et al., 2003).
This variety in the scope of services is largely attributed to school, local, and state policies (Lofink et al., 2013; National Assembly on School-Based Health Care, 2008; Strozer et al., 2010). Lofink et al. (2013) noted that school district and school policies are the greatest prohibiting factors in the provision of RHS by SBHCs. In a 2003 study, more than 76% of the sites reported some limitations associated with contraceptive provision, with policies of school districts and school boards and state laws providing the greatest level of restrictions (Santelli et al., 2003). Rurally located schools and SBHCs serving middle and elementary schoolchildren were less likely to provide RHS (Santelli et al., 2003).
Studies showed that students who receive RHS at SBHCs reported increased use of contraception, higher numbers of individuals choosing abstinence, and, in some studies, minimal differences in teen pregnancy or STI rates comparing teens who choose abstinence versus those engaging in safe sexual practices (Kirby, 2002; Minguez, Santelli, Gibson, Orr, & Samant, 2015; Ricketts & Guernsey, 2006; Soleimanpour et al., 2010; Zimmer-Gembeck, Doyle, & Daniels, 2001). Another area of study assessed differences in effectiveness in a SBHC voucher system (where students were prescribed and given a voucher for contraception to be received at another site) versus a direct-provider system (wherein students were given the birth control method at the SBHC encounter). Several studies noted that SBHCs were associated with significant rises in rates of filling birth control prescriptions, increased reporting of birth control use, and reductions in initial and repeat pregnancy rates in schools where birth control was immediately accessible at SBHCs rather than those available from another site (Mears, Charlebois, & Holl, 2006; Ricketts & Guernsey, 2006; Sidebottom, Birnbaum, & Nafstad, 2003; Smith, Novello, & Chacko, 2011; Zimmer-Gembeck et al., 2001). Also noted was a decrease in the time from initiation of sexual activity to the use of contraception, significantly lowering the risk of pregnancy and STIs/HIV (Sidebottom et al., 2003). In addition, researchers found SBHCs as highly effective for screening and treating STIs (Braun & Provost, 2010; Joffe et al., 2008; Nsuami, Taylor, Sanders, & Martin, 2006).
How teens perceive and use RHS by SBHCs may be an important variable when assessing accessibility. Examination of the National Longitudinal Study of Adolescent Health revealed that about 13.3% of those teens receiving family planning services and 8.9% of those receiving STI-related services obtained such care at SBHCs and reported satisfaction with services (Crosby & St. Lawrence, 2000). In another study, students reported using SBHCs for 30% of medical, 63% of family planning, and 31% of their counseling services (Soleimanpour et al., 2010). Researchers found that teens perceived that other youth would seek out family planning services at SBHCs related to confidentiality, free services, convenience, higher quality of care, and youth-friendly services (Soleimanpour et al., 2010). Teens most likely to positively view RHS at SBHC included those who are relatively young, living in rural areas, without a driver’s license, and from minority backgrounds. These are perhaps students most in need of SBHC services (Crosby & St. Lawrence, 2000).
Additional research suggests that high school students reported they would be most likely to use pregnancy and STI/HIV prevention interventions, education, and counseling if these services were available in the SBHC (Brown, Pennylegion, & Hillard, 1997; Coyne-Beasley, Ford, Waller, Adimora, & Resnick, 2003; Soleimanpour et al., 2008). Students claimed that SBHCs were optimal locations for these services because students obtained routine and gynecological care at the centers and care was known to be safe, respectful, and confidential (Brown et al., 1997; Soleimanpour et al., 2008). Other researchers studied teens with a history of pregnancy or reports of inconsistent use of condoms. They found that these teens voiced a desire to have access to condoms and contraception at school, reinforcing that high-risk populations could benefit from such services (Coyne-Beasley et al., 2003; Ethier et al., 2011).
Whether teens should have access to birth control and condoms in SBHCs is a highly debated issue. Research suggests a moderate to high level of public support for the provision of RHS by SBHCs as means to prevent teenage pregnancies (Baldassare, 2005; Eisenberg, Bernat, Bearinger, & Resnick, 2009; Herrman, Solano, Stotz, McDuffie, 2013; Lindley, Reininger, & Saunders, 2001; Richardson & Wright, 2012; Yarber, Milhausen, Crosby, & Torabi, 2005). Adult opinions about youth access to contraception were generally positive and varied based on the teen’s age, level of parental consent required, cost of services, education associated with services, and breadth of RHS made available to teens (Baldassare, 2005; Eisenberg et al., 2009; Herrman et al., 2013; Lindley et al., 2001; Richardson & Wright, 2012; Yarber et al., 2005; Zeanah et al., 1996). Less threatening interventions, such as counseling and education, were more favorable than other services including prescribing birth control, dispensing condoms and birth control, and treating STIs/HIV (Lindley et al., 2001). These studies demonstrate a growing area of interest as we continue to develop policies and programs designed to prevent teen unintended pregnancy and STIs/HIV. The provision of RHS by SBHCs is one such important strategy and key stakeholders have the capacity to inform provision of these services. This study fills a needed gap in the literature by collecting and analyzing these perceptions.
Methods
Design and Setting
The purpose of this study was to evaluate the perceptions of adult key informants regarding the provision of RHS by SBHCs. Following approval by the academic institutional review board and the state human subjects committee, this study explored stakeholder thoughts through individual, semistructured interviews on the provision of RHS at SBHCs. The principal investigator (PI) conducted the interviews using an interview guide that asked participants to consider their thoughts about teens’ accessibility and use of RHS, the provision of RHS in SBHC, and policy implications (see Figure 1). The interviews ranged from 25 to 70 min in length. Eight interviews were done by telephone, mostly related to scheduling difficulties, and 42 interviews were conducted in person. In-person interviews were conducted in private locations deemed convenient by participants; all participants signed consent forms.
Interview Guide.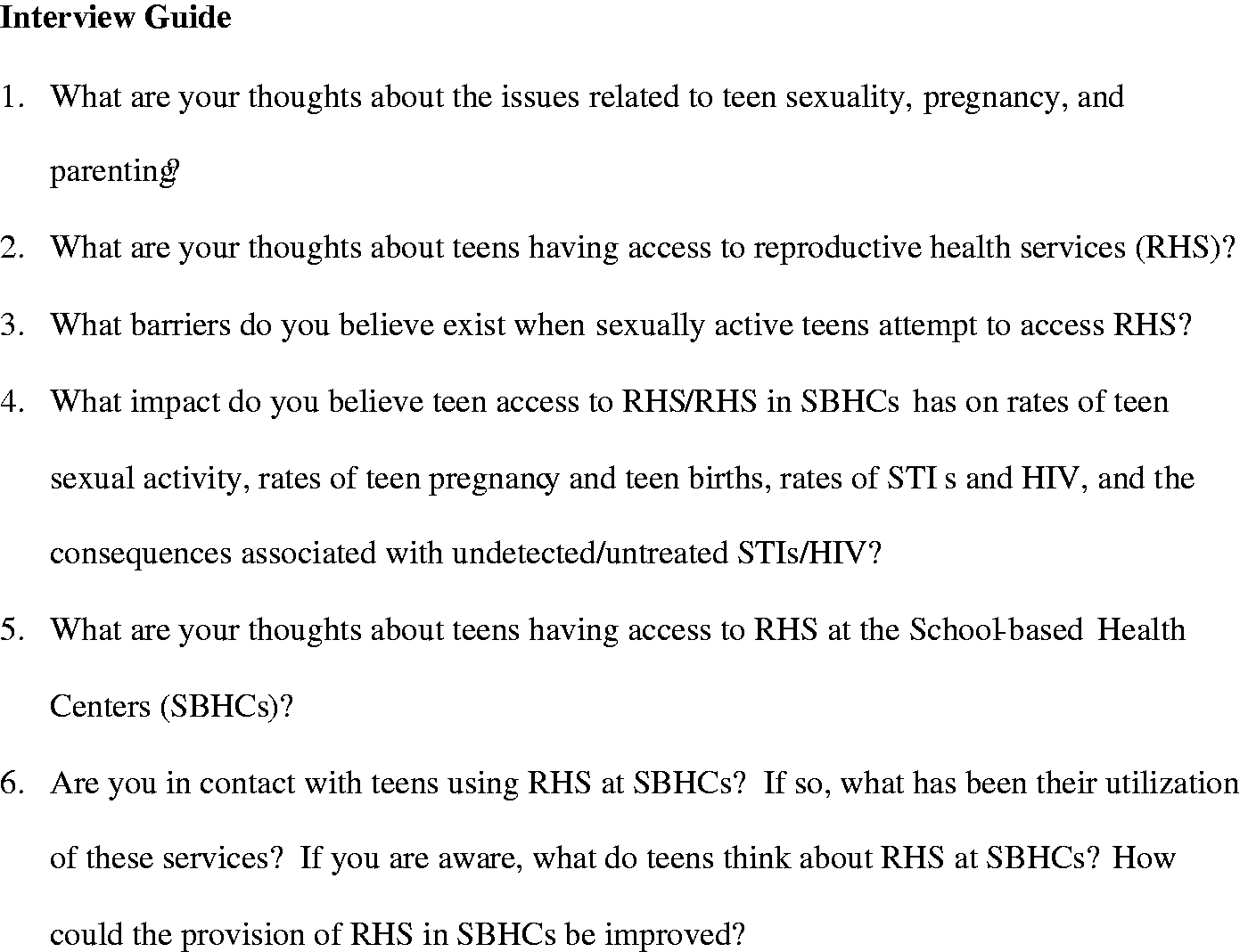
To protect confidentiality, we decided not to audiotape interviews. Because of the controversial aspects of RHS in SBHCs and concerns expressed by several potential subjects, the interviews were documented through note-taking, verbatim writing of key quotes, and immediately handwriting notes after each interview. Al-Yateem (2012) discussed the potential effects of audio recording on participant comfort, candidness, and authenticity during interviews when research topics are deemed sensitive or controversial. Moll (2012) further explored qualitative research methods with politically charged issues, noting that participant authenticity may be compromised with audio recording methods. Therefore, during each interview, the PI took detailed notes reflecting participant answers to each question. After the interview, the PI filled in notes to include full clauses and to augment data with additional details. If a client made a quote that was an important component of the data, the PI wrote the statement verbatim. The PI made every effort to authentically depict the words and meaning of the participants. As noted by Rubin and Rubin (2005), the PI bracketed personal biases, wherein personal opinions were recognized and consciously placed aside during data collection and analysis, to ensure accuracy of the data. Transcriptionists typed up the handwritten notes and the PI proofread and organized the transcripts for readability and fidelity to participants’ responses. No identities were linked with individual data items. Transcripts were reread several times in preparation for data analysis and ascription of themes.
Sample
The purposive sample of participants was accessed through researcher identification and snowball technique, wherein current participants suggested future sample members. Seventy-two potential candidates for interview were contacted by e-mail and invited to participate in the study. These potential interview subjects received e-mail attachments consisting of a brief introduction to the study, an invitation to participate, an information letter, consent form, and interview guide. Participants were asked to respond to the e-mail and a repeat e-mail was sent to those not responding to the first call.
Of the 72 stakeholders invited to be in the study, 50 consented to participate and were interviewed. The remaining 22 were not included in the study because they either failed to respond to the invitation or they responded but declined the invitation to be interviewed. Other reasons included difficulty scheduling an interview time or the invitee delegated someone else to be interviewed. About one third of the sample represented SBHC staff, including nurse practitioners, physician assistants, social workers, counselors, and nutritionists. Other subjects included public health clinicians and administrators, individuals working in reproductive health, advocates, community members, vendor administrators, physicians, school nurses, school administrators, teachers, school resource officers, school board members, and parents.
Data Analysis
The data analysis process included template analysis and thematic analysis to identify recurring and emerging themes (Rubin & Rubin, 2005). The interview guide provided the template such that each concept could be reviewed individually. Reexamination of the results in an iterative manner led to the identification of nine themes. These themes typically spanned several questions. Extrapolated subthemes clarified larger themes and exemplar quotes associated with themes and subthemes grounded the themes in the findings.
Results
Themes of Perceptions of the Provision of RHS by SBHCs.

Note. RHS = reproductive health services; STI = sexually transmitted infection; SBHCs = school-based health centers; STDs = sexually transmitted diseases.
Issues Related to Teen Sexuality, Pregnancy, and Parenting
Study participants disclosed significant concern about the rates of these issues in the state of study. They were aware of the rates in this state and expressed such concerns as “sexual activity is the norm,” “multiple sexual partners . . . that’s a concern,” and “teens are having sexual activity earlier” (see Theme #1). There was some discussion of the inevitability of teen pregnancy. Participants discussed the potential for intentional teen births and differences among cultures and communities. They commented that teen pregnancies “are accepted” and “a large segment of teens want to get pregnant.” As noted in Theme #6, participants also spoke of teens perhaps not intending to become pregnant but also not engaging in prevention efforts while sexually active. The group appeared very concerned about these issues as a whole and considered the subject of study worthy of attention relaying that “teen sex and pregnancy are symptoms of problems in society, troubled families with limited supports.”
Participants emphasized that not all teens are sexually active and that there was a disconnect between relationships and sexual activity, indicating an area for teaching and means to support teen self-esteem and relationship skills. Much discussion ensued about parent–child communication and the need for both parents and children to be educated about sexuality and sexual activity. Participants related that “there’s always a younger group needing education” and “education with teens needs to happen over and over to have an impact.” The need for education of all stakeholders was noted by several participants and is also highlighted in Theme #2.
Several participants noted that parents often do not speak with their children about sex or they have “unrealistic expectations that telling a teen not to have sex is going to work.” Others noted that parents could share misconceptions about sex or limit teen access to accurate information, further complicating the teen’s ability to implement safe sexual practices. Interviewees noted the critical role of parents or other adult support systems with regard to sexuality education, role modeling, and shared values, as cited in Theme #3.
Teen Access to RHS
Most of the interviewees shared that RHS may be provided by community centers, physicians, primary care providers, stores for nonprescription supplies, and SBHCs (see Theme #7). Those that supported RHS most often considered condoms and birth control pills as feasible. Other RHS, such as emergency contraception, more invasive hormonal methods such as medroxyprogesterone (Depo-Provera), and implanted hormones, were less avidly supported. Participants voiced concerns over the potential for HIV testing, citing issues with confidentiality and the referral process for positive tests. Sample members contended that issues associated with HIV testing were surmountable with clearly delineated policies and training.
Some participants complained that “teens do have access to condoms—they just don’t use them or take the time.” Several interviewees said that youth with goals for the future and motivation to prevent pregnancy will “get birth control” and other teens may not consider that repercussions of unsafe sex, stating “it’s the teen brain.” Other participants stated that RHS should be provided “in the drinking water” or “on every street corner” to best meet youths’ needs.
Barriers to Accessing RHS
Study participants identified several barriers. Certain regions in the state were noted as having the greatest challenges associated with access, especially the more rural communities. The leading barrier to access was to transportation, citing the poor mass transit system, distance of services, lack of cars or ability to drive, and the ability to garner transportation in a confidential manner, as paramount. Other barriers included cost, lack of teen-friendly services, limited hours, and knowledge of services or potential for cost-free care. These barriers were captured in Theme #5. Concerns about confidentiality were also barriers, especially for teens. Parents and other adults were also mentioned as barriers. For example, one participant stated, “Teens are trying to do the right thing . . . parents think if I tell you not to have sex, you won’t” and “parents prevent prevention.”
Impact of Teen Access to RHS on Outcomes Pertaining to Rates of Sexual Activity and Other Consequences
Participants heartily endorsed RHS as positively affecting health outcomes. They generally did not believe that sexual activity would increase in response to access to RHS, as noted in Theme #1, but that other more negative outcomes could be prevented as a result of safe sexual behavior. Most did not believe rates of sexual activity would decrease either, citing sexual activity as a component of “growing up.” Some indicated that education and counseling, a negative pregnancy test, or diagnosis and treatment for an STI, all potential services of SBHCs, may curtail sexual activity. In contrast, one parent opposed to RHS noted, “I worry about contraception in schools. Every teen will think it is okay to have sex.” Interviewees expressed hope that access would decrease pregnancy rates but also cited, “teens have had access in other areas and the rates of teen pregnancy are still high” and “the norms of teen births and pregnancies are hard to battle.”
Teens Access to RHS at SBHCs
This question provided the forum for discussion about the controversy over the provision of RHS in schools and at SBHCs. The most prevalent response was that access in schools, and thereby the SBHCs, was optimal to attend to the unique needs of teens. The ability for services to be provided during the school day, with little interruption in classes, on-site, and in a confidential manner supported these assertions. Those interviewed reinforced that access should be provided in an “educational way—don’t just hand out condoms in a fish bowl.” The education and opportunity for follow-up, along with ongoing contact and access to students associated with SBHCs, were frequently cited as the assets of SBHC provision. One participant noted that RHS could be a “gateway for teens to access health services.” Most participants supported provision of condoms, birth control pills, and testing and treatment for STIs, whereas fewer considered emergency contraception or HIV testing as appropriate. Participants noted that RHS should be “perceived as part of fully integrated healthcare rather than isolated dimension,” and that “teens just think of this as another part of healthcare,” leading to the ascription of Theme #4.
Those opposed to RHS at SBHCs cited religious tenets, the obstruction of parental control over teens’ health and decision making, the potential to encourage teens to have sex, the lack of involvement of parents in shaping their children’s values, and the potential for unsafe health practices as reasons for schools not to provide RHS. Participants who were against youth accessing RHS focused on the need for parental consent and control in making decisions about teens’ health care. One parent commented, “I worry about girls being prescribed to get contraception when birth control is free . . . it makes them feel pressured to have sex.” Another reinforced this point, saying that health-care providers “should not step over parents’ rights . . . once they (RHS) are in schools, everyone will be getting it” and “all children have a parent or guardian who helps make decisions—it confuses children when you take decision-making away from parents.” In contrast, other parents said, “parents need to get with the times,” “I understand their [parents’] need to be respected for parental rights, but teens also have needs,” and “people need to understand . . . those who don’t have parental support—they really need these resources.”
Two participants cited that schools were not appropriate cites for health care, especially RHS. Although this sample was largely supportive of providing RHS, some in the study commented that the “conservative community members won’t allow our school board to approve them” and “the religious right limits the rights of others in getting the RHS they need to stay safe.” Others contended that the school boards and administrations feared community reprisal and did not want to address the controversy. Participants also discussed the potential for school board members to represent their own interests, rather than representing the health and social needs of their constituents, leading to construction of Theme #8. One respondent stated that “conservative board members think only about themselves and their own children.” Some of the interviewees noted that schools were confronting other problems, such as standardized testing scores, poor graduation rates, and school violence. Provision of RHS, although not addressed, was not necessarily opposed. Others expressed fear of bringing the issue of RHS to the attention of the community because SBHCs were objects of scrutiny within state funding. These participants wanted to “stay under the radar” and not “stir up any new issues.”
Contact With Teens Using RHS at SBHCs, Their Utilization of These Services, and How Provision of RHS in SBHCs Might be Improved
At the time of study, in 2014, 14 of the 28 SBHCs provided RHS in the state. Selected individuals from the SBHCs were asked about their experiences in providing RHS. They responded that the use of RHS was “slow but steady,” with “not huge numbers but a big service to those who are using them.” Participants noted very little “parental push back,” “no irate phone calls,” and “good support from the administration and teachers.” There was no “line down the hall.” Sample members noted that the services were well received by teens, stating “teens love it” and “they trust us and know they get good care,” leading to the identification of Theme #9.
Sample members discussed that those using services at the SBHCs were the “ones that needed it most, they lack parental help or transportation,” “they are most at risk of birth control failure, they have lots of questions,” and “the RHS help the teens stay in school.” One study participant relayed, “[We] need to understand those [students] who don’t have parental support . . . they really need these services.” In response to the controversy over teen versus parental rights and notification of parents about use of RHS, one participant noted, “we encourage teens to discuss with their parents . . . its better when they are not a barrier.”
No obstacles to provision of RHS were identified except the need to ensure that RHS did not interfere with school or student’s classes. Regarding possible improvements in provision of RHS, interviewees identified the ability to enhance the variety of birth control methods offered, expand HIV testing, and the prescribe emergency contraception if needed.
Discussion
Participants in this study agreed that RHS must be teen friendly, convenient, confidential, low- or no-cost, developmentally appropriate, evidence based, medically accurate, and part of holistic care. SBHCs, along with other clinics and health-care provider agencies, were optimal sites for the provision of RHS because of their ability to conduct accurate assessments, comprehensive education, and careful monitoring and follow-up. Those interviewed perceived that access to prevention education and services is paramount in establishing cost-effective practices to reduce teen pregnancy and STI/HIV rates. They conveyed that education of teens, parents, and those involved in decisions related to sexual health and SBHC services should be ongoing and medically accurate.
This study clarified perceptions among a group of key stakeholders as additional schools and school boards consider the provision of RHS by SBHCs. Participants voiced overwhelming agreement with the provision of RHS, thereby substantiating public opinion noted in the literature (Baldassare, 2005; Eisenberg et al., 2009; Herrman et al., 2013; Ito et al., 2006; Lindley et al., 2001; Richardson & Wright, 2012; Yarber et al., 2005; Zeanah et al., 1996). These perceptions of RHS in SBHC and those noted in the literature provide a foundation upon which to build efforts to provide reproductive services in other SBHCs.
In accordance with the literature, this sample cited that school boards and, to a lesser extent, school administrators are the major opponents to the provision of RHS in SBHCs (Broussard, 2002; Kirby, 2002; Rienzo et al., 2000; Wald et al., 2001; Williams et al., 2004). Fears of public rebuttal, parental opposition, or other controversies surrounding the introduction of RHS into SBHC noted in this study substantiate those found in the literature (Wald et al., 2001; Williams et al., 2004). The school board members interviewed in this study expressed similar concerns. In contrast, the school administrators interviewed in this study were either supportive or neutral on the topic. They expressed concerns over parental opposition and public outcry but personally supported the practices.
A majority of the sample was also parents, although many had children who were either younger or older than teenagers; only a few had teenagers at the time of study. Study participants who were also parents supported the provision of RHS in the schools, citing the need to keep teens healthy and the high rates of sexual activity in the state. Two school board members expressed staunch opposition to the provision of RHS and any counseling other than abstinence-focused education. Again, the overwhelming support of the provision of RHS by SBHCs was constrained by a small, but vocal minority replicated the barriers to the provision of RHS noted in the literature (Baldassare, 2005; Daley, 2012; Eisenberg et al., 2009; Herrman et al., 2013; Ito et al., 2006; Lindley et al., 2001; Richardson & Wright, 2012; Wald et al., 2001; Williams et al., 2004; Yarber et al., 2005; Zeanah et al., 1996).
Lack of logistical complications in implementing RHS in SBHCs offering such services in the state validates the potential for ongoing exploration of the provision and expansion of services. Teens’ perspectives on the normalization of holistic health care to include sexual health and RHS emphasize the importance of such services as public health interventions that protect teens and their rights to comprehensive health care (Fothergill & Feijoo, 2000; Santelli et al., 2003; Sidebottom et al., 2003).
The main reason for opposing RHS is rooted in the notion that access to contraception increases teen sexual activity. Renowned researchers refuted this concept and its place in this debate (Daley, 2012; Kirby, 2002; Smith et al., 2011; Zimmer-Gembeck et al., 2001). One study indicated that provision of RHS in schools may decrease levels of sexual activity subsequent to education and counseling about responsible sexual behavior (Kirby, 2002). Several participants in the current study claimed that the provision of RHS could reduce sexual activity through education, counseling, and confidential services.
Limitations
The sample was obtained through PI identification and the snowball technique. As such, it tended to represent health-care professionals, administrators, and others who espoused similar views about the issues. Efforts were made to identify parents, school administrators, and school board members that would ensure sample diversity, but it is unknown whether all perspectives were represented.
Also unknown is if the note-taking practice during the interviews limited the interpersonal nature of the discussions. In addition, the PI took notes in phrases and later completed these sentences. Subtle changes in meaning could have resulted from these practices. Although every effort was made to bracket biases, the lack of audio recording is a limitation to the accurate representation of participants’ responses. Reviewing and expanding the notes after each interview, reviewing the transcriptions repeatedly, and having a single interviewer minimized the potential threats to authenticity of the findings.
Implications for Further Research
To further examine this issue and to broaden the research and generalizability of findings, researchers might develop a quantitative survey that could be implemented with a larger group, allow for randomization of participants, and yield data that could be analyzed through statistical analyses. Future research might include examination of teens’ views. Current research reinforces the need for teens to participate in research and to voice their perspectives, rather than to be analyzed through the lenses of adult stakeholders (Daley, 2012; Herrman et al., 2013). Confirmation of a significant relationship between the provision of RHS by SBHCs and decreasing rates of teen pregnancies, teen births, STIs, and infection with HIV are other possible topics for future investigation. In addition, research connecting RHS provision with positive school outcomes, such as school completion, achievement, and connectedness, may provide support for continued adoption of these practices.
Implications for Policy and Practice
Most of the participants in this study supported youth access to RHS and their inclusion as standard health practices and options for teens using SBHCs. Proponents of SBHCs’ provision of RHS might engage those who oppose these services and search for resolutions focusing on common ground, compromise, family and parental rights, the cost-effective nature of prevention, and optimal strategies to promote teen health. It is important that school board members and education administrators be fully informed on the benefits and consequences associated with the provision or withholding of RHS at SBHCs. Including parents, community serving agencies, and community members on advisory boards, with teen representation, may also provide the forum for information sharing and policy change. Ensuring that policies and programs are based on the realities and needs of today’s teens, while focusing on health and safety, provides a role for nurses as experts in teen development and health.
Findings of this study and related research, along with evidence affirming the negative impact of unprotected sexual activity on the health and success of students, can inform school board members, legislators, school health personnel, and policy makers involved with school health. Parents also need education and information to foster health in their children in concert with their values and personal beliefs (Daley, 2012; Soleimanpour et al., 2010). The provision of RHS in SBHCs acknowledges sexual health as one component of comprehensive public health services for youth.
Nurses have an important role in influencing policies related to teen reproductive health such as those addressed in this study. They may advocate for teens who choose to be sexually active and support policies that ensure safe sexual behavior. Several studies affirm the positive impacts of SBHCs on school success, school completion, and school connectedness (Anyon et al., 2013; Parasuraman, & Shi, 2014; Stone et al., 2013; Strolin-Goltzman et al., 2014). In advocating for comprehensive services, including RHS, nurses and others may highlight the correlation of health with positive school outcomes.
Conclusion
U.S. teen pregnancy and birth rates continue to decline largely related to improved prevention education and behavior changes. Yet, they remain higher than rates in any other developed nation in the world (Kearny & Levine, 2012). Although abstinence is a viable and important message for teens, nurses and others working with youth need to acknowledge that some teens have sex. Hence, facilitating access to safe, evidence-based, developmentally focused, and medically accurate information is important. This study highlights the need for consensus building, ongoing efforts to reach compromises, and exploring options for provision of optimal reproductive health-care services for teens.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Division of Public Heath Delaware Department of Health and Social Services.