
Abstract
This article presents a policy analysis of proposed smoke-free legislation in Kentucky during the 2015 General Assembly. Kingdon's three streams model of agenda setting is used to analyze the failure to pass HB145. Secondhand smoke exposure and related deaths are a significant public health problem in Kentucky, a state with one of the highest smoking rates in the U.S. HB145, a comprehensive smoke-free bill, was designed to protect workers and the general public from secondhand smoke and e-cigarette aerosol in enclosed workplaces and public places, with few exemptions. The bill faced intense criticism from opponents who were concerned about violation of personal and business rights and the belief that the decision should be addressed on a local level. HB145 passed the House with amendments but failed to receive a hearing in the Senate. Failure of the smoke-free legislation was due to partisanship, fragmentation of advocacy groups, lack of political bargaining, and conflict of values. As in past years, the policy window did not open for state smoke-free legislation in 2015.
Tobacco use is a significant public health problem in the United States. In 2011, Kentucky had one of the highest state smoking prevalence rates for adults (51st) and youth (44th). In addition, Kentucky ranked 52nd in smoking-attributable mortality in 2011 (Centers for Disease Control and Prevention, 2012). In 2014, Kentucky's average per capita income ($23,731), percentage of persons in poverty (19.1%), and proportion of population with a bachelor's degree (21.8%) all were below the national average. Kentucky had a population of over 4 million in 2015, and most residents live in rural areas (United States Census Bureau, 2015). Rural, tobacco-growing areas are disproportionately affected by tobacco use and more than 8,000 Kentuckians die of smoking-attributable illnesses annually (Hahn, Rayens, Adkins, Begley, & York, 2015; Kentucky Cabinet for Health and Family Services, 2014; Tobacco Prevention and Cessation Program, 2012). Medicare and Kentucky Medicaid bear a significant financial burden with an estimated $1.2 billion spent annually treating smoking-related illness as reported in 2014 (Kentucky Cabinet for Health and Family Services, 2014). Kentucky's Department for Public Health reported in 2010 that Kentucky employers lose $2.13 billion each year in smoking-attributed productivity costs (Tobacco Prevention and Cessation Program, 2012).
Tobacco use affects the smoker's health and has negative health impacts on those exposed to secondhand smoke. In 2011, Kentucky ranked among the highest (43rd) of all U.S. states in reported overall exposure to secondhand smoke (51.4%; Centers for Disease Control and Prevention, 2012). Moreover, 1,000 Kentuckians die every year from secondhand smoke exposure (Kentucky Education Television, 2015a). Exposure to secondhand smoke causes numerous diseases including heart disease, cancer, and lung disorders (Kentucky Cabinet for Health and Family Services, 2011). Approximately, $128.4 million in annual health-care costs in Kentucky are due to secondhand smoke exposure (Behan, Eriksen, & Lin, 2005).
Secondhand smoke exposure occurs primarily at work and in public places such as restaurants, shopping centers, parks, and schools, and in the homes and cars of people who smoke (U.S. Department of Health and Human Services, 2006). Among Kentuckians who report exposure to secondhand smoke, most identify the locations as workplaces (30%) and public places (32.8%; Centers for Disease Control and Prevention, 2012). There are no safe levels of secondhand smoke exposure and separating smokers from non-smokers, cleaning the air or ventilating buildings does not prevent exposure (American Cancer Society, 2015; U.S. Department of Health and Human Services, 2006). The only way to fully protect non-smokers from exposure indoors is to prohibit all smoking inside buildings.
According to the U.S. Surgeon General, smoke-free policies are the most effective approach to protect against secondhand smoke exposure (U.S. Department of Health and Human Services, 2014). Eliminating non-smokers' exposure to secondhand smoke is one of the four Centers for Disease Control and Prevention (CDC) goals aimed at reducing the amount of tobacco-associated morbidity and mortality (Tobacco Prevention and Cessation Program, 2012). Researchers have shown that smoke-free legislation in other states has improved the health of workers and the general population. In addition, some studies report a reduction in smoking prevalence and improved cessation outcomes (Hahn, 2010).
Comprehensive smoke-free laws reduce smoking prevalence have positive health outcomes and do not have a negative economic impact on businesses. After implementation of a smoke-free ordinance in Lexington-Fayette County, Kentucky, there was a 32% reduction in adult smoking prevalence (Hahn et al., 2008). Moreover, women living in Lexington, Kentucky experienced a 23% reduction in hospitalizations for acute myocardial infarction after implementation of the smoke-free law (Hahn, Rayens, Burkhart, & Moser, 2011). In Kentucky, those living in a community with a comprehensive smoke-free law were 22% less likely to experience a hospitalization for COPD compared with those living in a community with no or weak smoke-free laws (Hahn et al., 2014). Additionally, in Kentucky and Ohio, there was no evidence that either rural or urban counties experienced a loss of economic activity following the implementation of smoke-free laws (Pyles & Hahn, 2012).
In 2015, for the fifth year in a row, Kentucky legislators introduced a bill prohibiting smoking in public places and places of employment. Although the evidence indicates a need to protect the public from secondhand smoke exposure (Behan et al., 2005; Kentucky Cabinet for Health and Family Services, 2011), HB145 failed passage. The purpose of this article is to present a policy analysis of HB145, the Smoke-free Kentucky Act, using Kingdon's three streams framework (Kingdon, 2011).
History of Kentucky's Smoke-free Bill
In 2004, the Lexington-Fayette Urban County Government became the first community in the state to enact a local smoke-free ordinance (Greathouse, Hahn, Okoli, Warnick, & Riker, 2005). While other counties and municipalities have followed Lexington-Fayette County's example, many Kentuckians remain unprotected. As of October 2, 2015, 26 states had 100% comprehensive smoke-free laws in workplaces, restaurants, and bars (Americans for Nonsmokers' Rights, 2015). While local level smoke-free ordinances in Kentucky currently protect 33% of the population, 66% go unprotected and remain exposed to unhealthy air (University of Kentucky College of Nursing, 2015b). Figure 1 provides a map of local smoke-free ordinances in Kentucky as of August 2015 (University of Kentucky College of Nursing, 2015a).
Strength of smoke-free ordinances in Kentucky communities.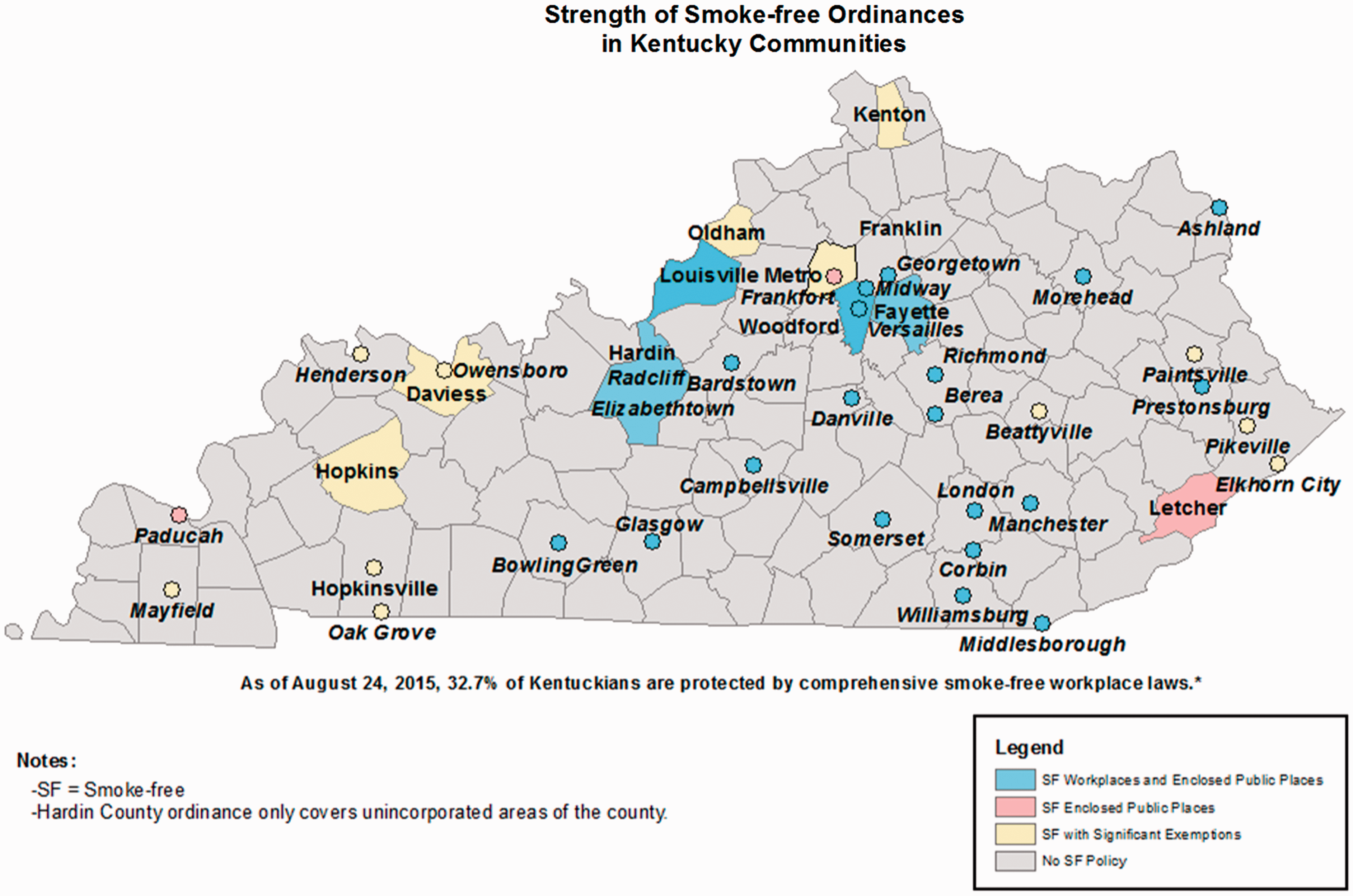
For the past 5 years, Kentucky state Representative Susan Westrom (D-79) has introduced comprehensive smoke-free legislation in the Kentucky House of Representatives that would prohibit smoking in public places and places of employment. In January 2015, Representative Westrom (D-79) from central Kentucky and Representative David Watkins (D-11), a physician from western Kentucky, cosponsored House Bill (HB) 145. The bill prohibited indoor smoking in businesses, places of employment, and other public places, similar to the bills that had been filed over the previous 4 years. The bill would exempt private residences except those used for childcare or adult day care. In February 2015, The Kentucky House Health and Welfare Committee passed HB 145. On February 13, 2015, the Democratic-controlled House passed the bill by a vote of 51 to 46 with amendments that significantly weakened the bill. For example, Amendment 13 provided an exemption that would “grandfather” cities or counties that had any smoke-free law in place.
HB145 Summary of Actions in the Kentucky House of Representatives, January 8, 2015 to February 13, 2015.
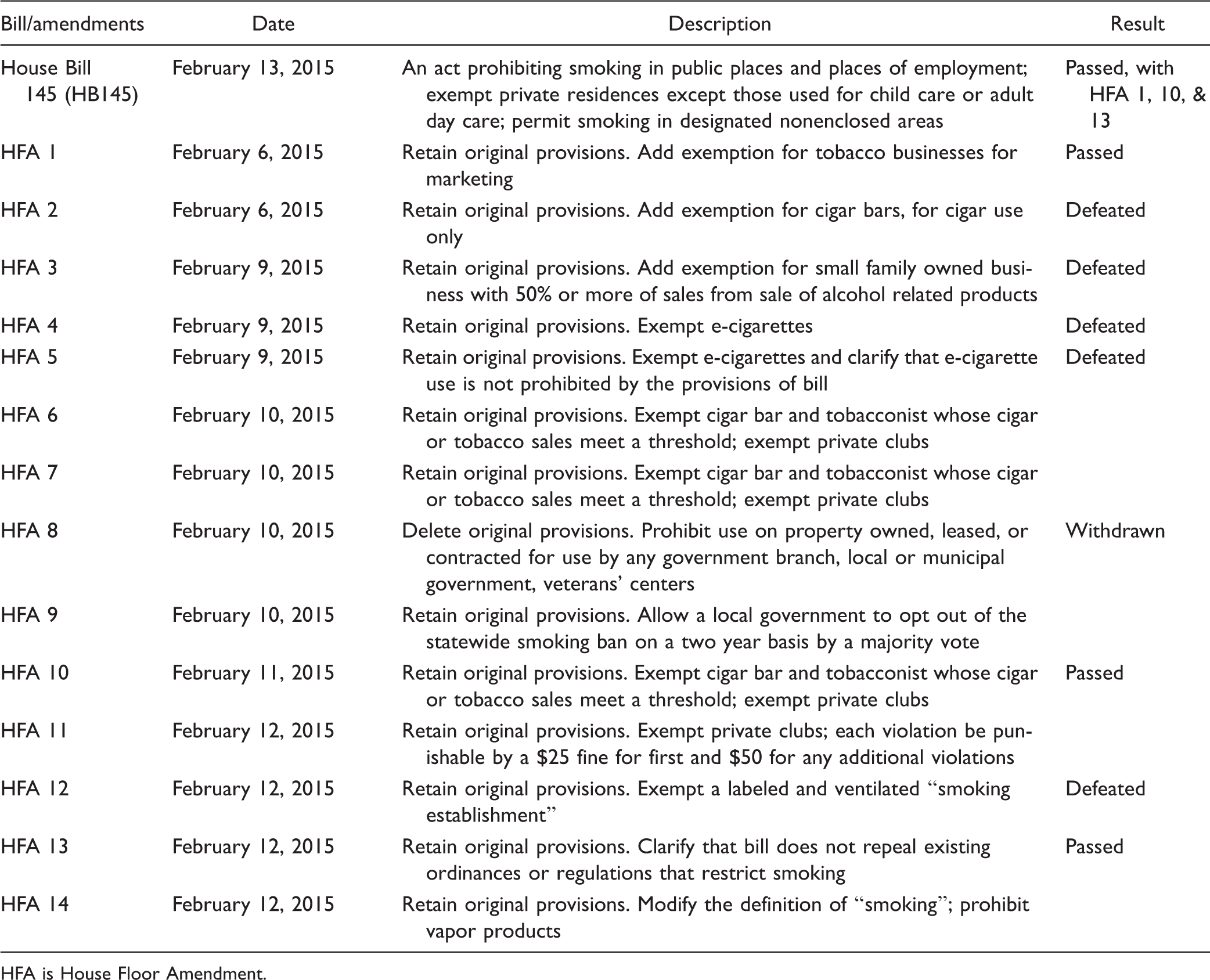
HFA is House Floor Amendment.
Kingdon's Three Streams Model of Agenda-Setting
Kingdon's three streams model has two purposes. The first explains why some problems become part of the policy agenda and others do not. Second, the model describes the generation and selection of policy alternatives (Kingdon, 2011). According to Kingdon, participants and processes affect agenda setting and policy alternatives. Participants are inside (e.g., governor, political appointees, career bureaucrats, legislators) and outside government (e.g., interest groups, researchers, the media, and public opinion; Kingdon, 2011).
The model is composed of three streams that primarily flow independently of each other: problems, policies, and politics. In the problem stream, issues come to the attention of people in and around government. Indicators, focusing events or crises, and feedback comprise the problem stream. In the policy stream, policy communities (e.g., specialists, consultants, and interest groups) generate alternatives and policy proposals. Several policy proposals and ideas exist simultaneously and “float around like soup” until a few ideas survive (Kingdon, 2011). Kingdon identifies certain survival criteria that a policy idea needs in order to stay “afloat”: technical feasibility, value-acceptability, and few imposed constraints. He states a problem must have an available solution for decision makers to consider in order for the problem to rise to the decision agenda. The solution must be viable and ready to enact. The politics stream consists of the national mood, organized political forces, administrative turnover, and consensus building. The term national mood, or state mood in this case, refers to the notion that a large number of people share the same public opinion. The national or state mood changes over time in discernible ways. These changes can have important impacts on policy agendas and policy outcomes (Kingdon, 2011). Political parties and partisan factors impact the organization of political forces. For example, Democrats are typically more willing to use government to regulate the private sector than Republicans. Legislators use bargaining to accomplish consensus building in the politics stream. If legislators are unwilling to bargain, the policy is unlikely to get on the agenda or obtain enough votes to pass (Kingdon, 2011).
These three streams flow along until coupling occurs in which the three streams merge and a policy window opens. Policy enactment is most likely to occur when a problem is recognized often through a crisis or “focusing event” (Kingdon, 2011). These events may provide evidence of the need for a new policy and policymakers may be called to action by growing public opinion. In addition, the policy community has a solution available, and the political climate is right for change. This model is not without weaknesses. The model conceptually presents the three streams as independent. However, viewing the streams as interdependent may be more appropriate since changes in one stream may reinforce changes in another (Zahariadis, 2014).
Policy Analysis of the Smoke-Free Kentucky Act
Participants
The goal of a comprehensive smoke-free law is to provide universal protection from secondhand smoke for all individuals living and working in Kentucky. HB145 had several proponents. Representative Westrom (D-79), HB145 sponsor, and an advocate for policies to expand and support health and social services, has served in Kentucky's House of Representatives since 1999. She sponsored the same legislation in the 2011, 2012, 2013, 2014 sessions and called for smoke-free legislation to be a priority in 2015 (Patrick, 2014). House Speaker Greg Stumbo (D-95), a former attorney, supported HB145. Senator Julie Raque Adams (R-36), sponsor of SB189 and Co-Chair of the Senate Health and Welfare Committee, is a small business owner and former member of the Louisville Metro Council who has served in the Kentucky General Assembly since 2011. Democratic Governor Steve Beshear was a strong proponent of the smoke-free campaign. In September 2014, Governor Beshear issued an Executive Order making all executive branch properties tobacco-free (Executive Order No. 747, 2014). The Kentucky Chamber of Commerce and the Kentucky Medical Association supported comprehensive smoke-free legislation; over 90% of Chamber members supported a comprehensive smoke-free law (Adkisson, 2015; Patrick, 2015). Smoke-Free Kentucky (SFKY), a coalition of public health groups, community organizations, businesses, and individuals, insisted on a comprehensive smoke-free law to avoid loopholes. For example, they opposed grandfathering communities with smoke-free laws before the state smoke-free legislation thereby exempting them from the stronger law. SFKY also opposed exempting certain businesses from smoke-free legislation, such as hospitality or casino workers, as this would expose both employees and the public to secondhand smoke (Americans for Nonsmokers' Rights, 2009).
The leadership team of Smoke-Free Kentucky comprised staff and volunteers from the Campaign for Tobacco-Free Kids, American Cancer Society, American Heart Association, American Lung Association, Kentucky Center for Smoke-free Policy (KCSP), Kentucky Chamber of Commerce, Kentucky Hospital Association, among others. In addition, Smoke-Free Kentucky was supported by over 500 businesses and organizations representing a wide variety of community groups interested in health. Representatives from Smoke-Free Kentucky organizations signed a resolution supporting smoke-free legislation (Kentucky Center for Smoke-free Policy, 2011; Smoke-free Kentucky, 2014).
Many Senate and House members, mostly Republicans, publicly voiced opposition to HB 145. Senate President Robert Stivers (R-25) stated that HB145 did not offer personal choice and that businesses should have the right to set their own policies (Patrick, 2014). Senate Majority Whip Jimmy Higdon (R-14) supported smoke-free laws only at the local level (Patrick, 2014). The Kentucky Farm Bureau (2013) adamantly opposed any level of government or agency mandating that business prohibits tobacco use and they contended business owners should have the exclusive right to prohibit tobacco use.
In 2015, the first author conducted an interview with a national tobacco control organization to gain a better understanding of opposition to smoke-free policy. The interview revealed that tobacco companies typically do not openly disclose their opposition to smoke-free legislation. Instead, they use front groups and allied industries to push for voluntary or weakened laws (Saloojee & Dagli, 2000). Groups such as the Bluegrass Institute (BGI) and other libertarian-leaning groups in Kentucky (e.g., Northern Kentucky Choice and Freedom Kentucky, an arm of BGI) were opposed to smoke-free legislation (Northern Kentucky Choice, 2011; Waters, 2015). These groups prefer limited government and contend that smoke-free legislation violates private property rights and the personal freedom to use a legal substance.
Problem Stream
Indicators and focus events
Several factors led Kentucky lawmakers to place the Smoke-free Kentucky Act on the government agenda in 2015. First, Kentucky's high smoking rates and secondhand smoke exposure contributes to enormous health and economic burden and mortality rates on the state of Kentucky. On February 11, 2015, the Smoke-Free Kentucky coalition organized a “focus event” at the state Capitol in Frankfort, Kentucky, to encourage advocates to visit their legislators and ask them to support HB 145. Kingdon (2011) defined a “focus event” as “a crisis or disaster that calls attention to a problem or a symbol that catches on in the public view” (pp. 94–95).
The coalition advertised the event on its website, briefed participants, and handed supporting documents to other individuals and groups that backed the proposed legislation. The event culminated with a rally and press conference in the Capitol Rotunda, where Dave Adkisson, President and Chief Executive Officer of the Kentucky Chamber of Commerce, spoke about the business community's support of HB 145. Other speakers included Representative Westrom, the bill's house sponsor, Eugenia Crittenden Blackburn “Crit” Luallen, Kentucky's Lieutenant Governor, and Stephanie Mayfield Gibson, Commissioner of the Kentucky Department for Public Health. This event helped to focus state legislators' attention on the health consequences of secondhand smoke exposure and the public and business support for smoke-free legislation.
Feedback
At the rally, smoke-free policy leaders and victims of secondhand smoke exposure told stories about their suffering. For example, a volunteer for the American Cancer Society who was also a lung cancer survivor, said he represented those with cancer “who did not make it.” He attributed his lung cancer to the smoke-filled Capitol building where he worked as a lobbyist for 10 years. A physician and a breast cancer survivor explained how she had no other contributing factors for cancer other than waiting tables in smoky bars and restaurants between the ages of 16 and 22. She shared that wait staff have the highest rate of exposure to secondhand smoke among all occupations in Kentucky. In addition, she cited a 70% increased risk of getting breast cancer in young pre-menopausal women who are exposed to secondhand smoke compared with those exposed later in life (Patrick, 2015). This feedback from constituents likely had a profound impact on elevating HB 145 to the agenda (Patrick, 2015).
Negative feedback also played a role in the bill's defeat. According to Kingdon (2011), negative feedback is one reason why problems fade from the legislative agenda. For example, Representative Richard Heath (R-2) stated because he represented an agricultural district and tobacco is a legal product; he did not support smoke-free legislation. He wanted to protect the farm economy and the families that depend upon farming for their livelihood (Kentucky Education Television, 2015a). Other representatives opposed smoke-free legislation founded on a rights-based approach. In February 2015, Representatives Tim Moore (R-18), Phil Moffett (R-32), and Addia Wuchner (R-66) stated in comments to the full House that no one had the right to impose on personal freedoms or the rights of business owners (Kentucky Education Television, 2015a). Although evidence indicates smoke-free legislation reduces serious health risks, protects the rights of non-smokers, and lowers the cost of tobacco-associated health care (Hahn et al., 2014; Hahn et al., 2011), negative feedback related to tobacco farming and property rights contributed to fading of the problem.
Problem definition
Kingdon (2011) defines a policy problem based on values, comparisons, and categories. These three components all had a part in defining the problem of secondhand smoke exposure in the workplace. Kentuckians' values influenced the problem of secondhand smoke exposure and policy stakeholders categorized the problem differently. Advocates of smoke-free legislation saw the problem as an issue of public health and emphasized the dangers of secondhand smoke in causing disease and premature death in non-smokers. Representative Westrom said on the House Floor, “they (the workers) don't have a choice and I want to protect those workers” (Kentucky Education Television, 2015a). In contrast, opponents tended to define the policy problem as one of rights. They argued government does not have the right to impose such restrictions on businesses and personal choices. Representative Addia Wuchner (R-66) said business owners should have the choice of instituting a smoke free workplace and “I am sure they will do the right thing” (Kentucky Education Television, 2015a).
Policy Stream
Specialists inside and outside government generate policy alternatives. These ideas can appear and often fade. In this mix of ideas, some survive and are considered important policies. We evaluated the impact of policy communities, criteria for the bill's survival referred to by Kingdon (2011) as survival criteria, alternatives, fiscal impact, and unintended consequences of policy alternatives.
Policy communities
When legislators filed HB 145 in January 2015, it was a comprehensive bill providing the most protection for all workers and the public. Initially, the policy community outside of government, the Smoke-Free Kentucky coalition, was tight-knit and sound, representing 500 organizations. Advocates originally had common goals for smoke-free legislation, but once HB 145 passed with amendments, some organizations changed their views on whether a comprehensive law was necessary. While some members of the coalition continued to work toward a comprehensive law, other members wanted to get some form of smoke-free legislation passed even if it was not comprehensive (A. Barkley, personal communication, March 24, 2015). The added amendments “fragmented” the policy (Kingdon, 2011) and affected the stability of the coalition supporting it.
The policy community inside government was not a unified group. Not all House members favored a comprehensive smoke-free policy. One legislator, Representative Johnny Bell (D-23) called for Amendment 13 to be added to HB 145. This revision exempted a city or county that already had a smoke-free mandate regardless of the strength of the policy. Representative Stan Lee (R-45) filed Amendment 5, which would exempt e-cigarettes from the bill (Kentucky Education Television, 2015a). Of the 14 amendments filed on behalf of HB 145, the House passed three. All proposed revisions would have weakened the bill by either exempting specific businesses or allowing grandfather provisions. The fragmentation of the policy community led to passage of HB 145 with amendments by a narrow margin (51-46) in the Kentucky House, on February 13, 2015.
Survival criteria
Kingdon (2011) defines survival criteria as components a policy alternative must have in order to be part of a policymaker's agenda. Survival criteria are based on technical feasibility and value acceptability, The Smoke-free Act was technically feasible. HB 145 would prohibit smoking in public places and places of employment, and local health departments would enforce the law.
In addition to technical feasibility, the public accepted HB 145. In 2014, Interact for Health and the Foundation for a Healthy Kentucky conducted an opinion poll. Public opinion in Kentucky indicated a steady increase in favor of a smoke-free law with the current rate at 66% (Institute for Policy Research, 2015). Similarly, a study of randomly selected residents in Lexington-Fayette County revealed a statistically significant increase in public opinion from 56% before to 63% after the smoke-free law (Rayens et al., 2007). Public opinion polls are open to criticism. Due to the nature of opinion polling, respondents' views may differ from the general public and not represent an unbiased sample. However, the opinion polls used in these studies utilized a large randomized sample to reduce selection bias.
Although the public supported HB 145 and it was technically feasible, the bill suffered from a lack of value-acceptability. Not all policymakers agreed on the proper role or size of government. Advocates in favor of HB 145 supported government mandates. Indeed, the Kentucky Supreme Court ruled in favor of Lexington's smoke-free ordinance saying that government has the responsibility as well as the manifest duty to provide a safe community (“Lex-Fayette Co Food and Beverage Assoc v Lex-Fayette Urban Co Govt et al.,” 2004). Although she had not supported statewide legislation immediately, Representative Westrom came to realize that local leaders had not stepped up to protect Kentuckians with only 32% covered by strong local smoke-free laws (Patrick, 2014). Other legislators continue to oppose statewide legislation as they argue it is a local issue, or they disagree that government has the right to mandate smoke-free laws. The Senate President, Robert Stivers, stated that it should be left up to the business owner to set their own policies (Patrick, 2014). Once legislators introduced SB 189 in the Senate, President Stivers sent the bill to an unfriendly, Republican-led committee where it died. The smoke-free bill failed to meet all three survival criteria.
Short list of ideas (tipping and amendments)
The more legislators in Kentucky debated the smoke-free issue, the more it came into focus. Kingdon (2011) states that “tipping” occurs when an idea has caught on or when both political parties and the public widely support an idea. The State Journal in Frankfort, Kentucky, reported that Westrom stated: We are right at the tipping point with some undecided [legislators]; it just takes a couple. Public opinion over a five-year period has done exactly what we expected it to do. Five years ago there were many people at the local level who were against and they didn't understand what smoke-free meant. We are just asking them to step outside 15 feet and most smokers already do that. (Bowman, 2015, para. 11 and 14)
Westrom went on to say “950 Kentuckians die every year from secondhand smoke related causes, an average of 66% of Kentuckians support smoke-free legislation, and with over 500 businesses supporting a smoke free bill…a tipping point has been reached” (Kentucky Education Television, 2015a).
The three amendments the House passed included HFA 1, which exempted tobacco businesses for marketing; HFA 10, exempting cigar bars and tobacconists; and HFA 13, which grandfathered existing ordinances regardless of how strong the policies were (Kentucky Legislature, 2015). The amendments to HB 145 were inconsistent with best practices recommended by the CDC and the collaboration of national tobacco control partners. These entities recommend a comprehensive approach including eliminating exposure to secondhand smoke in order to protect the health of all workers (Americans for Nonsmokers' Rights, 2009; Centers for Disease Control and Prevention, 2014).
The available alternative
HB 145 as introduced was a viable solution for the problem of secondhand smoke exposure. However, as amended in February 2015, most smoke-free advocates found HB 145 to be unacceptable because it was no longer a comprehensive solution. Furthermore, even in its amended form, lawmakers did not accept HB 145 as a viable solution. They were still concerned with what they deemed as an inappropriate government mandate and/or a violation of individual rights.
Fiscal impact
A law prohibiting smoking inside public places and places of employment would not have a negative fiscal impact on the Commonwealth of Kentucky. Senator Ralph Alvarado (R-28), a family physician, testified before the House committee, saying “The bill won't cost taxpayers a dime, only savings in health care costs” (Kentucky Education Television, 2015b). In addition to health-care cost savings, there is no evidence that smoke-free legislation harms business (Adkisson, 2015; Pyles & Hahn, 2012; Pyles, Mullineaux, Okoli, & Hahn, 2007). Moreover, there is no evidence that urban or rural county businesses in Kentucky or Ohio experienced economic loss as a result of smoke-free laws (Pyles & Hahn, 2012).
Unintended consequences
HB 145 was intended to protect Kentuckians from the dangers of secondhand smoke exposure. One unintended consequence of such legislation is an increase in the likelihood that smokers will quit. Smokers in communities with comprehensive smoke-free workplace ordinances are more likely to quit than those who live in communities without smoke-free workplace laws (Hahn et al., 2008). Adult smoking prevalence in Lexington, Kentucky, declined by nearly one third during the 20 months after the smoke-free ordinance was enacted in 2004, compared with similar Kentucky counties without smoke-free ordinances (Hahn et al., 2008).
Politics Stream
State mood
With 2014 public opinion polls of Kentucky adults' increase in support of a smoke-free state, Westrom agreed that the state was ready for a statewide smoke-free law when she proclaimed, “Their soft speech has now turned into a roar” (Patrick, 2014, par. 4). Overall, the mood of Kentuckians toward HB 145 was positive.
Organized forces
According to Kingdon (2011), if all of the interest groups and other organized interests point in the same direction, this pushes lawmakers in that direction. Conversely, if there is conflict among the organized forces, lawmakers experience a “for and against” environment that can split their support. This was the case for HB 145. Proponents were very vocal about a comprehensive smoke-free law. Smoke-Free Kentucky had a “take action” link on its website, http://ctfk.salsalabs.com/p/dia/action3/common/public/?action_KEY=541. Where they were prompting constituents to send messages to their state representatives, and the Smoke-free Kentucky Day at the Capitol brought supporters together in a unified voice. In contrast, opponents such as the Bluegrass Institute have consistently opposed smoke-free legislation since 2008 through its president, Jim Waters' weekly column, the “Bluegrass Beacon,” appearing in various local newspapers. On February 8, 2015, Waters wrote, “three northern Kentucky counties have voluntarily gone smoke-free without government mandates indicating that we don't need Frankfort bullying local communities on this issue” (Waters, 2015, para. 11). The Farm Bureau's stand on business owners rights and the tobacco companies' tactics of using front groups (Apollonio & Bero, 2007; Malone, 2009) to press for voluntary or weakened laws added to the organized opposition. These opposing forces divided lawmakers over HB 145.
Consensus building
The House achieved consensus for HB 145 by adding three amendments. Without significant turnover in the Kentucky General Assembly since the start of the smoke-free legislative campaign in 2010, lawmakers used bargaining in order to pass HB145 out of the House by a slim majority. The votes were primarily along party lines with only 9 of 44 Republicans voting in favor of the bill. Once the bill was sent to the Republican-controlled Senate, Stivers assigned it to the Senate Veterans, Military Affairs and Public Protection Committee. Senator Albert Robinson (R-21) was chair of the committee and opposed to smoke-free legislation (Loftus, 2015). The bill did not receive a hearing and died.
Coupling
For the fifth year in a row, coupling of the three streams did not occur for smoke-free legislation in Kentucky. Although indicators, feedback, and a focusing event brought attention to the negative health effects of secondhand smoke exposure and facilitated agenda-setting, the House weakened the smoke-free bill with amendments. Furthermore, the Senate lacked support for its version of the bill (SB 189) and it did not survive.
Summary and Conclusions
Although Kentucky leads the nation in smoking prevalence, has a high rate of secondhand smoke exposure, and an enormous health and financial burden from associated health costs, lawmakers who supported smoke-free legislation in 2015 failed for the fifth year in a row to gain enough support for a comprehensive statewide smoke-free bill to pass through both the House and Senate. Using Kingdon's three streams model, this policy analysis illustrates how strong supporters became fragmented when amendments were added, weakening the legislation. Although the bill passed the House, the Senate received SB189, similar to the original version of HB 145, and assigned it to an unfriendly committee where it was not discussed. Smoke-free legislation has support from Kentuckians, but lawmakers are divided on whether the issue should be considered at the state or local level, or if the decision should be left to individual business owners. Kentucky is a disparate state with high poverty and tobacco use rates, but until support builds through negotiation or increased public education and demand, statewide smoke-free legislation in Kentucky will likely remain on hold.
Discussion
We used Kingdon's three streams model for agenda-setting to guide this analysis of smoke-free legislation in Kentucky. Although the model adequately explained how and why the bill did not pass into law, there are some limitations to the generalizability of the analysis. For example, we only performed a one state analysis. However, other researchers could apply the lessons learned from this analysis to understanding the complexities of highly debated topics within government. Historically, Kentucky is a tobacco-growing state and is considered disproportionately affected by tobacco use, secondhand smoke exposure, and weak tobacco control policies (Hahn et al., 2015). In many rural communities, growing and using tobacco are social norms, and therefore, policy change requires community interventions and assessments of readiness to change (Hahn et al., 2015; Liber, 2010). Nurses can use their advocacy skills in the policy arena through policy literacy and professional organizations (Malone, 2005). Nurses may empower their patients by increasing awareness of the benefits of smoke-free legislation and help to more effectively address health problems within their communities.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.