
Abstract
Twenty-eight states have laws and regulations limiting the ability of nurse practitioners (NPs) to practice to the full extent of their education and training, thereby preventing patients from fully accessing NP services. Revisions to state laws and regulations require NPs to engage in the political process. Understanding the political engagement of NPs may facilitate the efforts of nurse leaders and nursing organizations to promote change in state rules and regulations. The purpose of this study was to describe the political efficacy and political participation of U.S. NPs and gain insight into factors associated with political interest and engagement. In the fall of 2015, we mailed a survey to 2,020 NPs randomly chosen from the American Academy of Nurse Practitioners' database and 632 responded (31% response rate). Participants completed the Trust in Government (external political efficacy) and the Political Efficacy (internal political efficacy) scales, and a demographic form. Overall, NPs have low political efficacy. Older age (p≤.001), health policy mentoring (p≤.001), and specific education on health policy (p≤.001) were all positively associated with internal political efficacy and political participation. External political efficacy was not significantly associated with any of the study variables. Political activities of NPs are largely limited to voting and contacting legislators. Identifying factors that engage NPs in grassroots political activities and the broader political arena is warranted, particularly with current initiatives to make changes to state laws and regulations that limit their practice.
Given the rapid and turbulent changes to the U.S. health-care system following the 2016 elections, nurse practitioners' (NPs) political efficacy and participation are important for securing affordable, high-quality care for millions of Americans. The 2016 presidential campaign set the stage for disarray within the Republican party (Jacobson, 2016), while the Democratic party experienced unprecedented division in its voter base (Boys, 2016; Wang, Li, & Luo, 2016). Campaigns were contentious, unconventional, and disruptive. Political unrest is at its highest since 2000 (Boys, 2016; Wang et al., 2016). The implementation of the Patient Protection and Affordable Care Act was a concern during the 2016 campaigns. As of January 31, 2017, 12 million newly insured individuals were added to an already strained health-care system (Associated Press, 2017).
Central to the health-care debate is a well-documented shortage of primary care providers, predicted to become critical by 2020 (Graves et al., 2016). Both the Institute of Medicine (IOM, 2011) and the National Governors Association (2012) recommended removal of restrictive state regulations to enhance access to NP services as a necessary step to address the provider shortage. The Federal Trade Commission (2014) ruled that physician supervision clauses in NP state practice acts create anticompetitive environments and should be removed. Revising outdated laws or regulations to allow NPs to practice to the full extent of their education would ensure patients have full access to NP services (Poghosyan, Boyd, & Clarke, 2016).
Historically, many NPs have not been politically engaged or able to effectively create and sustain political change (Craven & Ober, 2009; Kung & Rudner-Lugo, 2014; Moran, 2014; Oden, Price, Alteneder, Boardley, & Ubokudom, 2000). Understanding political efficacy, and factors associated with political efficacy, of NPs may facilitate the efforts of nurse leaders and nursing organizations to promote change in state rules and regulations.
This article presents the findings of a study examining NP political efficacy and participation. We explain the historical involvement of NPs' engagement in health policy, evidence of their political efficacy, and describe Sharoni's (2012) framework on political efficacy, which was used to structure this study. Methods and data analysis follow with a discussion of our findings and the study's implications for practice, policy, and professional organizations.
Background
Political efficacy is “an activity that has the intent or effect of influencing government action – either directly by affecting the making or implementation of public) policy or indirectly by influencing the selection of people who make those policies” (Verba, Schlozman, Brady, & Brady, 1995, p. 38). It is associated with political participation and often referred to as one's sense of being able to influence the political process (Caprara, Vecchione, Capanna, & Mebane, 2009; Sharoni, 2012). Political efficacy has two distinct constructs: a personal sense of efficacy (internal) and a system-oriented component of efficacy (external) (Neimie, Craig, & Mattei, 1991). Internal efficacy is one's sense of being able to understand and participate in politics. External efficacy is one's trust that the government will be responsive to the demands of citizens (Neimie et al., 1991; Sharoni, 2012).
Electorate politics are increasingly complex, especially in highly competitive elections (Barton, Castillo, & Petrie, 2016). Understanding campaign and electoral dynamics and learning about candidates require initiative; many eligible voters may feel inadequate to the task (Burden & Neiheisel, 2013). Some state and federal laws enacted since 2012 impose new policies on voters. Restrictions include requiring a photo identification to vote, curtailing voter registration times and early voting periods, and enforcing stricter rules for those with past criminal convictions (Wang, 2012; Weiser & Opsal, 2014).
Campaigns and elections that are controversial and competitive are associated with increased voter turnout, usually measured as a percent of registered voters who actually vote (Barton et al., 2016). In the first 12 national primary elections of 2016, 17.3% of eligible Republican voters turned out to vote. This is the highest rate of GOP primary voting since the 1980 elections. In 2016, Democrats had the highest rate (11.7%) of primary election voting since 1992, with one exception, the unusually high turnout in 2008 when the rate was 30.4% (Desilver, 2016; File & Chrissy, 2012). Harrington and Gould (2016) state that rates of eligible voters participating in presidential elections have decreased from approximately 64% in 2004 and 2008 to 61.8% in 2012. In 2016, only 60% of eligible voters cast a ballot (Harrington & Gould, 2016).
Age, gender, race, socioeconomic status (SES), and education are all associated with political participation, and education in the development of civic skills is strongly predictive of political participation (Hillygus, 2005). Schlozman, Verba, and Brady (2012) associated higher income with increased political activity, especially with regard to monetary donations toward political campaigns. Voting data from 2012 indicate that adults older than 65 years of age have higher rates of voting (69.7%) than adults 18 to 24 (38%) or 25 to 44 years of age (49.5%; File, 2013b).
Historically, younger voters report feeling isolated or excluded, as political parties have been reluctant to engage and represent their interests (Zukin, Keeter, Andolina, Jenkins, & Carpini, 2006; Henn & Foard 2012). Recent studies report increased interest among younger voters, with 18 to 24 years olds casting 19.9% of ballots in the 2014 election (Center for Information and Research on Civic Learning and Engagement, 2016). The racial demographics of voters also shifted in 2012, showing increased racial and ethnic diversity; 64.1% of eligible non-Hispanic Whites, 48% of eligible Hispanics, and 66.2% of eligible Blacks voted (File, 2013a). While women are more likely to vote than men (63.7% vs. 59.8%), in all other aspects of political participation, men consistently participate in political activities at higher rates than women (Dittmar, 2015; Schlozman et al., 2012).
Higher education leads to higher rates of voting, with the voting rate of college graduates as high as 70%, compared with 27% of those with high school education (“Voting,” n.d.). Based on several single state studies, certified registered nurse anesthetists and other advanced practice registered nurses (APRNs) consistently vote at rates greater than 90%, which is higher than general population voting rates (Casey, 2009; Moran, 2014; Oden et al., 2000; McDonald, 2016).
Political Efficacy and Political Participation of NPs
Research on the political efficacy and participation of NPs is limited. Studies of registered nurses (Barrett-Sheridan, 2009; Vandenhouten, Malakar, Kubsch, Block, & Gallagher-Lepak, 2011), NPs, certified registered nurse anesthetists, and certified nurse midwives report voting to be the predominate form of political participation (Casey, 2009; Moran, 2014; Oden et al., 2000). With the exception of 2008 elections, self-reported voting rates for NPs (89%) are higher than those of the general population (62%) (File, 2013b, Oden et al, 2000). Among NPs, lack of time, knowledge, interest, family obligations, and financial constraints are cited as barriers to other types of political participation (Casey, 2009; Kung & Rudner-Lugo, 2014; Moran, 2014; Oden et al, 2000).
Recent studies show mixed results on political efficacy and political engagement of NPs in areas other than voting (Kung & Rudner-Lugo, 2014; Moran, 2014; Oden, 2000; Ryan, 2015). Oden et al. (2000) report results of a mailed survey of public policy involvement sent to members of the American Academy of Nurse Practitioners (AANP). Time, money, and civic skills were identified as barriers to political participation for the 440 AANP members who responded (74% response rate). Voting was the most common political activity reported; 87% of the participants reported consistent voting patterns (Oden et al., 2000). There was a strong positive correlation between self-rated involvement in political activities and political efficacy (p < .001) with a majority reporting that they received policy education from professional organizations and journals.
Age, socioeconomic resources, and prior engagement in political activities were significant predictors of political participation among a study of 170 advanced practice nurses in Louisiana (Moran, 2014). Kung and Rudner-Lugo (2014) surveyed APRNs in Florida (n = 884); 23% reported being active in policy, despite acknowledging significant barriers to practice in their state. This differs from Ryan (2015), who surveyed 875 NPs practicing in convenient care clinics from 44 states and Australia and reported political involvement in 70% of the NPs, defined as membership in state or national professional nursing organizations. There was wide variation in the level of political engagement, with less involvement in political activities by NP students, unemployed, and retired NPs compared with those still employed. Ryan (2015) also reported that 43.1% of NPs practicing less than 2 years reported having had education or coursework in health policy.
In 1996, healthcare policy was identified as essential core content for master's education for advanced practice nursing (American Association of Colleges of Nursing (AACN), 1996). The purpose of including health policy content was to help students understand “how health policy is formulated, how to affect this process, and how it impacts clinical practice and health care delivery” (AACN, 1996, p. 7). Despite the addition of this content into educational programs, voting remains NPs' primary and most consistent form of political participation (Kung & Rudner- Lugo, 2014; Moran, 2014; Oden, 2000) with fewer NPs reporting involvement with local, state, and national organizations and their legislative activities.
The Future of Nursing: Leading Change, Advancing Health (IOM, 2011) called on the profession to enhance its political efficacy and presence in the policy arena. NP organizations across the country are working to revise their state laws and regulations to include the IOM's recommendation for NPs to practice to the full extent of their education and training. Despite revisions to state laws or regulations, many states still have rules and regulations that restrict NPs from practicing to their full potential, thereby limiting patients' access to primary care. In the 2012 to 2014 legislative sessions, over a dozen states introduced legislation to modernize licensure laws for NPs. Only three of these states were successful in making changes that led to full scope of practice (Phillips, 2015). As of 2017, 23 states and the District of Columbia have eliminated restrictive regulations legislative or regulatory restrictions on practice (AANP, 2017b).
The NP role was first established in the late 1960s and early 1970s (AANP, 2017a). Nearly 50 years later, NPs still face challenges to their professional practice. As legislation continues to drive changes to health-care delivery, it is imperative that NPs have a political voice. The extant literature is limited and lacks the depth of information required to successfully engage the NP population in political activities (other than voting) and advance the political agenda of the profession.
Theoretical Framework
Recognized as an important motivational variable, self-efficacy is an appropriate concept to frame this study on political efficacy and engagement. Sharoni (2012) describes internal and external political efficacy and defines them respectively as “the average American's feelings of political empowerment and his or her perception of the government's receptiveness to public political participation” (p. 119). This framework denotes characteristics predictive of internal and external political efficacy which lead to political interest, knowledge, engagement, and trust in the government and was used as a framework for this study (Figure 1).
Adapted from Sharoni, 2012.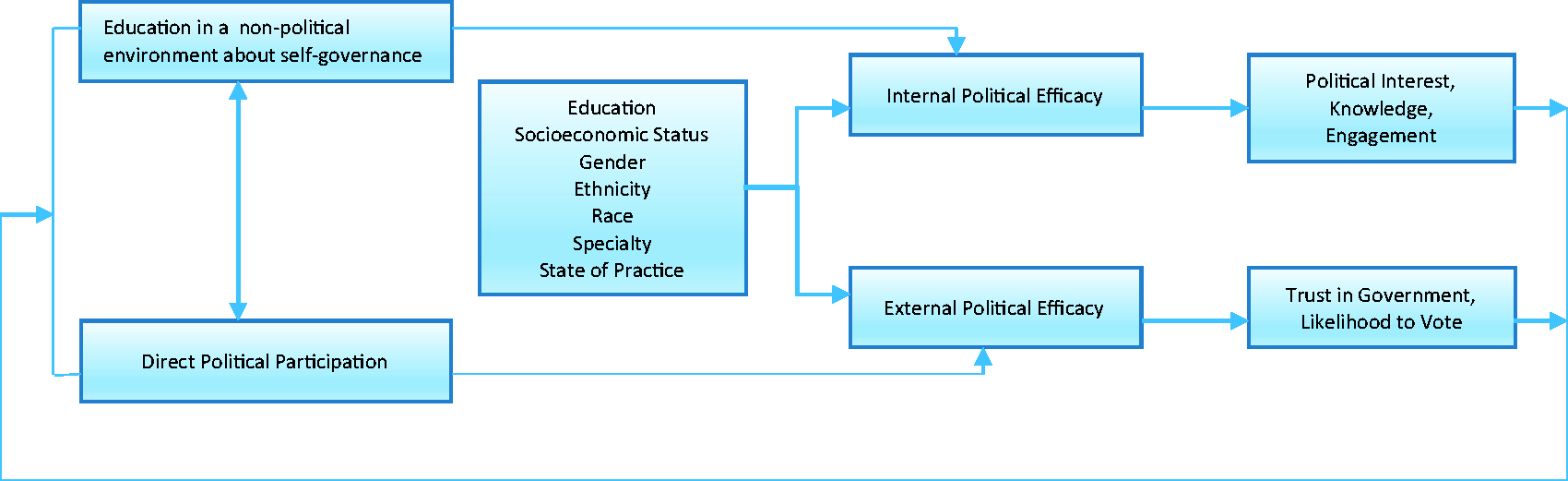
Personal characteristics (age, gender, SES, race, ethnicity education, and educational experiences in nonpolitical environments about self-governance) are factors associated with achieving internal political efficacy in the general public (Sharoni, 2012). Education about self-governance refers to teaching the general public they have a duty to participate, that their participation counts, and they have some control over their political destiny by participating in the process. Sharoni's (2012) conceptualization that education about self-governance in a nonpolitical environment is a form of political socialization, which leads to a sense of increased internal efficacy, is supported by the literature (Kahne, Crow, & Lee, 2013; Schlozman et al., 2012; Zukin et al., 2006). Specifically, higher education, higher SES, older age (>65 years), race (White), and gender (male) are predictive of a higher sense of political efficacy (Schlozman et al., 2012; Zukin et al., 2006).
In addition to the variables in Sharoni's model (Figure 1), we have added NP specialty and practice settings. We hypothesize that these factors will impact NP internal political efficacy. Kahne et al. (2013) have also shown that external political efficacy is influenced by one's direct political activity. Mentoring by someone more knowledgeable in health policy was included in direct political participation, as we hypothesized this may impact external political efficacy. Sharoni (2012) proposes a typography based upon high and low levels of internal and external political efficacy. She suggests a person with high internal and external political efficacy is an “Empowered American Citizen,” a person with high internal and low external political efficacy is an “Engaged Grassroots Activist,” a person with low internal and high external political efficacy a “Complacent American Citizen” and a person with low internal and external political efficacy a “Politically Alienated American” (Sharoni, 2012). Each category is indicative of varying political engagement. Use of this framework will yield valuable insights to achieve the goal of this study and to provide a foundation to spur further research to improve the political position of the NP profession.
Study Aims
Using a political efficacy framework, the purposes of this study were to evaluate the political efficacy and political participation of NPs across the United States and to better understand factors associated with political interest, knowledge, and engagement. The specific aims of this study were to: (a) describe internal and external political efficacy of NPs in the United States; (b) examine the association of select NP characteristics (age, gender, race, ethnicity, education, income, NP population foci, full practice authority, and relationship with a health policy mentor or role model) and health policy education in nonpolitical environments (academic coursework or continuing education offering on health policy) with internal political efficacy; (c) examine the association of select NP characteristics (age, gender, race, ethnicity, education, income, NP population foci, full practice authority, and relationship with a health policy mentor or role model) and previous political participation (direct political participation or mentoring by another with this experience) with external political efficacy; and (d) examine the relationship between internal and external political efficacy and NP political interest, knowledge, participation, and likelihood to vote.
Methods
Design, Sample, and Setting
A descriptive cross-sectional survey design was used to explore the political efficacy and participation of a random national sample of NPs. The sample was drawn from the American Association of Nurse Practitioners (AANP) database which includes all AANP members licensed in the United States (76,000) and is inclusive of all specialties (acute care, adult, family, geriatric, neonatal, pediatric, women's health, and psychiatric NPs).
The AANP database allows for systematic sampling, minimizing sampling error, and supporting the generalizability of the findings. We used geographically stratified data to identify a relationship between political efficacy and practice in states with full practice authority; we also wanted to have NPs representative of all 50 states.
Sample size was calculated based on a confidence level of 95%, confidence interval of half-width 0.05, standard deviation of 0.5, a 2015 population of 182,000 NPs, based on a 40% or less response rate. To address Aim 1, a required sample size of 385 was calculated for estimating mean internal and external efficacy to within plus or minus 0.05 points with 95% confidence, assuming a standard deviation of 0.5. For Aims 2 through 4 involving associations with efficacy, using two-sided hypothesis testing, a Type 1 error rate of 0.05, and 80% power, this sample size also allows a mean detectable between-group difference in efficacy of at least 0.3 standard deviations for two approximately equally sized groups. To accommodate a participation rate of at least 20% (conservative estimate), we randomly selected 2,020 NPs for our sample. Inclusion criteria included the following: (a) current licensure as an NP in the United States, (b) ability to read and write English, and (c) inclusion in the AANP database. There were no additional exclusion criteria.
Procedures
The names and addresses of a geographically stratified random sample of 2,020 NPs were purchased from AANP in 2015. To increase response rates, a postcard announcing the delivery of the survey was sent one week prior to survey mailing, as recommended by Dillman, Smyth, and Christian (2014). The survey mailing contained a letter of introduction, a survey containing the Political Efficacy and Trust in Government indices, a demographic questionnaire, a postage paid return envelope, and an Opt-Out postage paid postcard for those who chose not to participate. Approval was obtained from the University of Massachusetts Medical School Institutional Review Board. We piloted the survey with a random sample of 20 NPs to evaluate the survey instruments for ease of use, understandability of the directions, time for completion, and overall acceptability. No issues were identified. These data were included in the final sample. Completed surveys were accepted up to six weeks after the initial mailing.
Measures
The Efficacy Index (Sharoni, 2012) was used to assess internal political efficacy. Sharoni (2012) tested this index in a study on Internet use and trust in government with a sample of 924 adults. It is composed of 13 questions, derived from the American National Elections Study and political efficacy theory. This index uses a 1 to 5 Likert scale and ranks agreement or disagreement with each statement. An overall higher score indicates a higher sense of internal political efficacy. Analysis of the data showed a range from 0 to 44, mean score of 24.3, a skewness of −.389, and Cronbach's alpha of 0.775, demonstrating good reliability (Sharoni, 2012).
The Trust in Government Index, used to assess external political efficacy, includes 10 scale questions, based on a Gallup poll on “Trust in Government.” These 10 questions were designed to evaluate an individual's trust and confidence in government. The Likert type scale has participants rate their opinions on a scale of 1 to 5. Greater trust in government is demonstrated by high overall score. Sharoni (2012) tested the scale in a study on internet use and trust in government (n = 915). In her study, the scale had a range of scores from 0 to 41, a mean score of 17.6, a skewness of −.034, and a standard deviation of 7.2. Cronbach's alpha of 0.881 indicated high reliability (Sharoni, 2012).
A researcher developed demographic questionnaire was used to obtain data on characteristics thought to influence political efficacy, as described in Sharoni's framework. Characteristics included age, gender, ethnicity, SES, race, and education. Data on NP population foci and years of NP practice were also included. The following three additional variables were included: (a) relationship with a politically active mentor or role model, (b) specific education either during initial NP education program or focused continuing education on health policy, and (c) state where employed.
Statistical Analysis
Data analysis was performed using IBM SPSS statistics for Macintosh version 22. Descriptive statistics were calculated for all study variables as appropriate to the level of data. For continuous variables, mean, median, skewness, standard error of the mean, standard deviation, and histograms were calculated. Frequencies were run on all categorical variables. All continuous variables were checked for normal distribution by calculating Fisher's measure of skewness. Internal consistency and reliability were estimated using Cronbach's alpha for all multi-item scales.
Characteristics of the sample were summarized using frequencies for categorical variables and means (standard deviations) for continuous variables. Descriptive statistics for internal and external political efficacy are presented (Specific aim 1). To identify unadjusted associations of the outcomes internal and political efficacy with demographic characteristics (Specific aims 2–3) and political activities (Specific aim 4), one-way analysis of variance (ANOVA) was used for each predictor of interest. For Aims 2 and 3, multiway ANOVA was employed to estimate adjusted associations of participant characteristics with efficacy, including all predictors that were statistically significant in unadjusted analyses.
For Specific aim 4, analysis by one way between-subjects' ANOVA was conducted to compare the association of political activities with internal and external efficacy. Multiway ANOVA including all predictors that were statistically significant in unadjusted analyses was also performed.
Results
Characteristics of the Participants
Characteristics of Nurse Practitioners (N = 632).
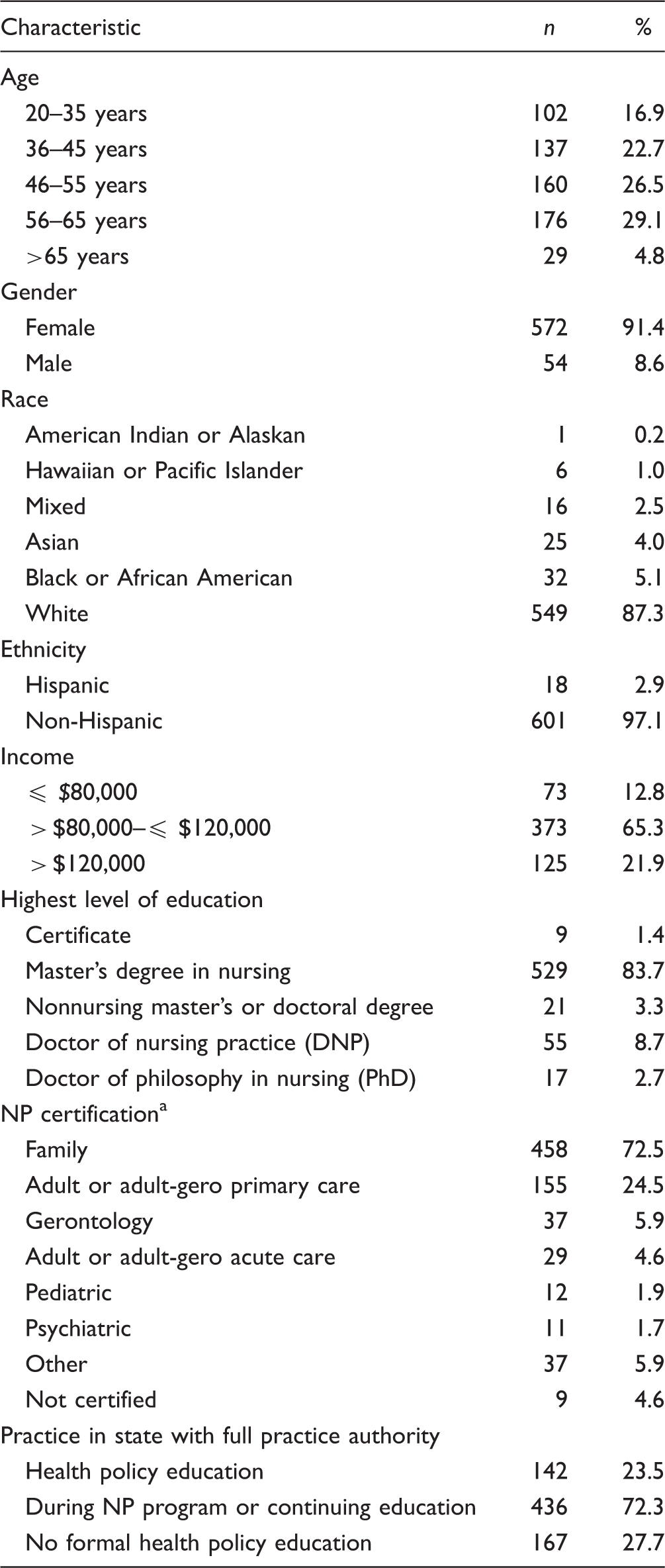
aSome NPs reported > 1 certification.
Political Efficacy
Political efficacy was assessed with two instruments; the Efficacy Index was used to measure internal efficacy, and the Trust in Government Index was used to measure external efficacy (Sharoni, 2012). With this sample, Cronbach's alpha for the efficacy (internal) and trust (external) indices were .648 and .892, respectively, indicating good reliability. Factor analysis was used to determine if reliability could be improved by removing low performing items. However, reliability did not improve when items were removed, therefore original scales were used. Internal efficacy scores ranged from 0 to 65 with a mean score of 44.3 (standard deviation of 5.9) and a median of 45. External efficacies ranged from 10 to 50, with a mean of 29.4 (standard deviation of 7.1) and a median of 30.
We divided the Trust and Efficacy Indices into high and low scores, based upon the median possible score, as suggested by Sharoni (2012). According to Sharoni's (2012) Trust in Government and Political Efficacy typology, NPs in this sample have low internal and external political efficacy and are categorized as “politically alienated Americans.” The sample was one point short of being classified as “empowered American citizens.”
Variables Associated With Internal and External Political Efficacy of NPs
Relationship Between NP Characteristics and Internal Political Efficacy (N = 622) a .
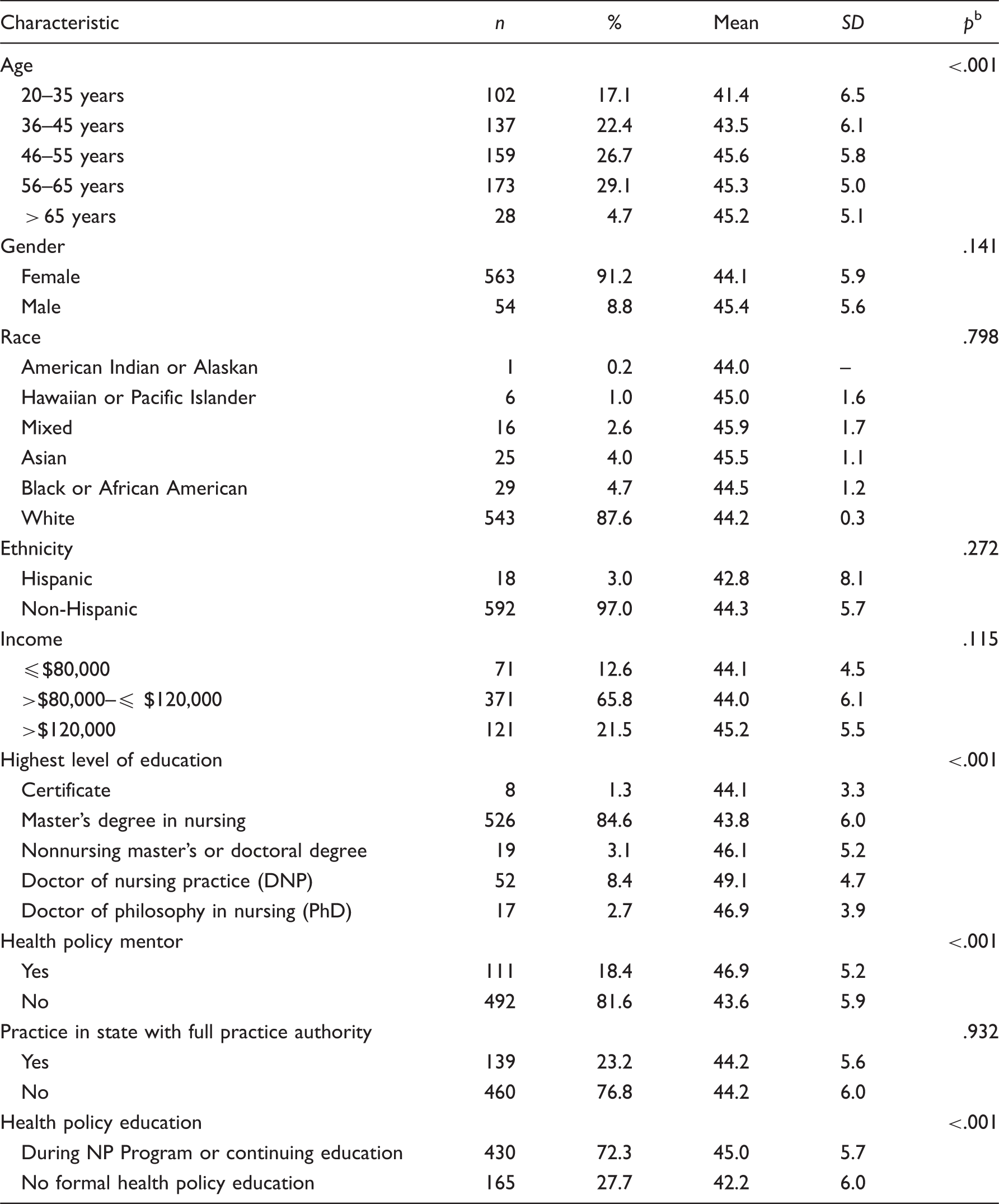
aTotal numbers differ from Table 1 due to missing data on efficacy measurement.
bANOVA.
Relationship Between NP Characteristics and External Political Efficacy (N = 620) a .
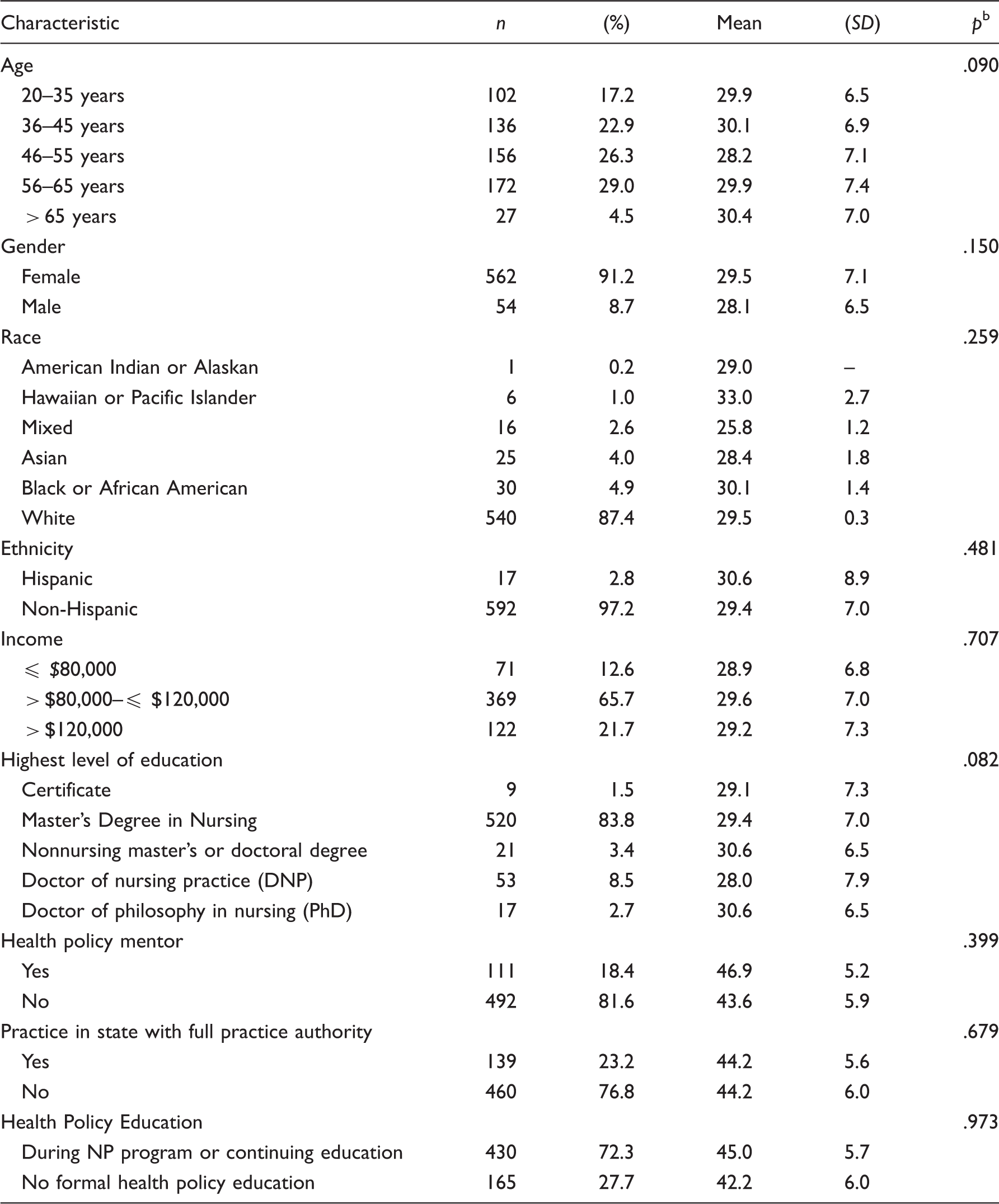
aTotal numbers differ from Table 1 due to missing data on efficacy measurement.
bANOVA.
NP Political Activities and Association With Political Internal and External Efficacy (N = 631).
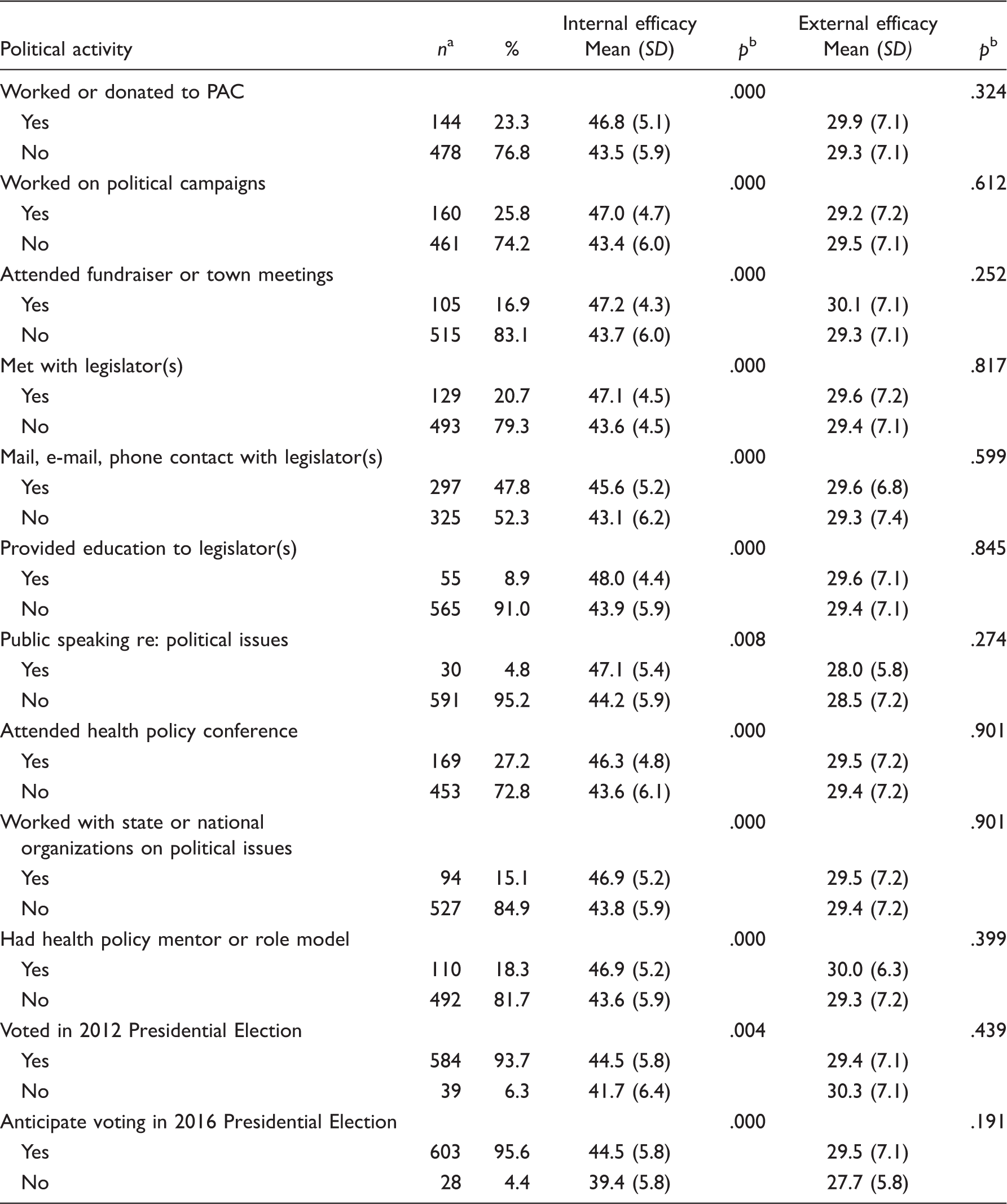
PAC = political action committee.
an reflects totals for Internal Efficacy Scale.
bANOVA.
NP Political Activity and Internal and External Political Efficacy
Voting in the last election, intent to vote in 2016 fall election, working on or donating to a political action committee, working on campaigns, attending fundraisers or political meetings, meeting with legislators and contacting legislators, publicly speaking about health policy issues, attending health policy meetings or conferences, and working with a state or national NP organization, all had statistically significant associations with internal efficacy, with p values ranging from ≤ .001 to .008 (Table 4). None of the factors we assessed were significantly associated with external efficacy.
Discussion
Studies of the general public identify gender, race, income, and ethnicity as factors positively associated with one's sense of internal and external political efficacy (Schlozman et al., 2012; Sharoni, 2012). This is in contrast to our findings, which showed that gender, race, income, and ethnicity were not associated with political efficacy. In our study, NPs were predominately White, middle aged, educated with a master's degree, and in a middle- to high-income bracket. These characteristics different from those of the general population and may account for the differences seen in our results.
In this study, older age, health policy mentoring, and specific education on health policy were all positively associated with increased internal political efficacy, as demonstrated in previous studies (Hillygus, 2005; Schlozman et al., 2012; Sharoni, 2012) and supportive of Sharoni's (2012) framework. The working hypothesis is that education fosters skills and efficacy levels that support the ability to participate in political interactions with confidence and ease (Condon, 2015; Hillygus, 2005; Persson, 2015; Schlozman et al., 2012; Sharoni, 2012). Education, in general, is widely accepted as a well-established predictor of political participation (Condon, 2015; Hillygus, 2005; Persson, 2015; Schlozman et al., 2012). Hillygus (2005) noted that programs that concentrate on developing civic skills strongly predicted increased political participation. In our unadjusted analysis, education was significantly associated with internal political efficacy, with NPs holding a master's degree in a field outside of nursing having the highest internal efficacy. Graduate education, however, was no longer significant in our multivariate analysis when we controlled for other factors.
Eighty-four percent of respondents in this study had not worked with state or national organizations to advance a political agenda, nor did they participate in many other political activities aside from voting or contacting a legislator. This is consistent with findings from Kung and Rudner-Lugo's (2014) study, where 23% of APRNs in Florida reported being active in policy. Ryan (2015) reported different findings, with greater than 70% of NPs being involved in political activity (measured by membership in state and national professional nursing organizations). These findings are in stark contrast to our findings and those of Oden et al. (2000). Considering membership in a professional organization as a reflection of political activity yields a high percentage of politically engaged NP and leads to questions of the limitations of this as a measure of engagement.
Applying Sharoni's (2012) framework to our results, NPs have low internal and external political efficacy, as well as limited active political participation beyond voting and contacting legislators. Given technologic advances and the national organizations' coordination of letter or e-mail writing campaigns, contacting legislators is an easily accessible method of engagement for many NPs. We did not specifically measure political donations made to a national organization, which like membership in a professional organization may represent indirect political participation and may yield a higher percent of NP involvement. However, indirect involvement does not necessarily increase grassroots involvement on critical issues. Less than 25% of NPs in this study engaged in a political activity such as meeting with a legislator, working on a campaign, or attending a fundraiser or town hall meeting. Political efficacy is not the same as one's sense of civic responsibility (Kahne & Westheimer, 2006), and it may not be the primary driving force behind NP participation in broader political activities.
Implications for Policy and Practice
NPs face barriers to practice, reimbursement, and professional recognition. Efforts to advance practice have been met with steep resistance in many states, and our grassroots efforts fall short many times (Dower, Moore, & Langelier, 2013; Phillips, 2015). In many organizations, institutional policies and by-laws hinder our abilities to practice to our full potential (Poghosyan & Aiken, 2015). Some insurers continually refuse to credential, reimburse, and recognize our contributions to the health-care system (Sharp & Monsivais, 2014). Each state determines the scope of practice for NPs in its jurisdiction, making action at the local and state level imperative. Advocating for policy change through legislation and regulation can influence NP practice environments.
Making legislators aware that over 90% of NPs report regular voting could allow our voice to be heard. Although technologic approaches (e.g., mass e-mail campaigns) to communicate with legislators may be increasing frequency of NP contact with policymakers, lack of engagement on other levels is a concern. The findings from this study reveal that we are not adequately engaging the NP population in political activities (beyond voting and letter writing) that can sway legislative initiatives. Barriers to participation include time, financial resources, civic skills, and lack of education (Casey, 2009; Kung & Rudner-Lugo, 2014; Moran, 2014; Oden et al, 2000). Identification of successful strategies that inspire NPs to address practice issues through the legislative arena is clearly needed.
Implications for Education
The 1996 recommendation to add health policy content to NP curricula was intended to improve political knowledge and engagement (AACN, 1996).. Based on our results, perhaps curricular reform is not enough to broaden NP political participation beyond voting and contacting legislators. Ryan (2015) noted that of NPs in practice for less than 2 years, 43% reported participating in any formal health policy education. Eighty-one percent wanted more formal educational opportunities on political activism. Our findings indicate 46.6% reported receiving formal health policy education during their initial NP program. Although some NPs in our sample were educated prior to the 1996 recommendation to incorporate health policy content into curricula, having less than half the sample recall this content is concerning. The quality and effectiveness of teaching health policy content warrant further review. Kahne and Westheimer (2006) note education that targets external efficacy does not impact one's sense of internal efficacy or one's sense of civic responsibility and actually may hinder the development of internal efficacy.
It is important for educators to discern desired outcomes of curricular content. For example, is the goal to have NP graduates be knowledgeable about health policy and the impact they might have on policy? Or, is it for them to become politically active and engage in the formation of health policy? Educators should find a way to incorporate health policy and political socialization throughout the curricula, to motivate and engage the “rank and file” NPs in the political processes that impact their work. Ryan (2015) suggests that adding political and policy questions to the national certification examinations may stimulate interest.
Implications for Professional Organizations
In this study, our sample falls into the “politically alienated” group, but only by one point. Given the sample are all members of the national organization, they may be more politically engaged and informed those who are not members. This holds significant implications for organizations to advance their legislative agendas. Organizing and mobilizing grassroots NPs are key to advancing the profession's political agenda. This is an important issue when the profession is seeking to obtain full practice authority across the country and substantially influence the changing health-care system.
Identification of barriers to NP engagement in health policy is clearly needed. Examining states that have created and sustained successful grassroots engagement, and duplicating these efforts, is one strategy to consider. Another option may be to create a database of NP activists for each state with the potential of linking interested NPs with mentors to develop expertise and foster new leaders. Although each state's context, political culture, and demographics are unique, the skill set to work with legislators and to mobilize NPs may be transferable. Expanding existing mentorship programs, such as the AANP Fellows Mentorship (AANP, n.d.), is another way to promote leadership development.
The association between political mentoring and political efficacy and participation challenges professional organizations to develop and increase opportunities for student and practicing NPs. Ryan (2015) reported that survey respondents identified a formal mentoring program as the most desirable way to promote engagement and that over 35% of the NPs were interested in participating in such a program. It is important for nurse leaders in practice, academia, and nursing professional organizations to engage NPs at the grassroots level. Increasing nurses' involvement in programs like the Robert Wood Johnson Foundation Health Policy Fellows is another option to increase knowledge and awareness (National Academy of Medicine, n.d.).
Strengths and Limitations
Demographics of the study population are consistent with AANP's 2016 membership database, which includes 76,000 NPs from across the United States. AANP demographic data report an average age of 49 years, White, predominately female, holding a graduate degree and practicing in primary care (AANP, 2016b). The NP demographics from the Kaiser Family Foundation (Henry J. Kaiser Family Foundation, 2016) are similar, suggesting our sample is representative of the U.S. NP population. The strengths of a random, geographically stratified sample with similar demographic characteristics of the overall NP population, as validated by AANP and Kaiser Family Foundation, are important and support generalizability of the results. This study also used reliable indexes to measure political efficacy, adding to the credibility of the findings.
The study had several limitations. Using a cross-sectional design provides information specific to this population at one point in time. Moreover, the survey relied on self-reporting. Underreported or overreported political participation due to inaccurate recall or perceived social desirability could pose a threat to the internal validity of the findings. Although external validity may be affected by nonresponse, as those choosing to respond to a mailed survey may be different in some ways from the nonrespondents, our sample was similar to the general NP population suggesting little nonresponse bias. The AANP database comprised NPs who are members in a professional organization and thus, we may have targeted those NPs more likely to be politically engaged and who have a higher sense of political efficacy than those who are not.
Conclusion
Using Sharoni's (2012) typology, our findings indicate that NPs have low political efficacy, labeling them as “politically alienated Americans.” Older age, health policy education, and mentoring are associated with internal political efficacy and political engagement of NPs. The political activity of NPs in the United States is largely limited to voting and contact with legislators. Identifying strategies to engage NPs in the broader political arena is warranted, particularly with current initiatives to change state laws and regulations that limit NP practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.