
Abstract
Smoke-free workplace policies encourage cessation, reduce tobacco consumption, and shift the pro-tobacco norm. However, no research exists evaluating the impact of mandated tobacco-free policies on government property. The purpose of our study was to examine short- and long-term effects of a tobacco-free policy (executive order 2014-747) implemented in November 2014, prohibiting tobacco use on state executive property. Cross-sectional online surveys were administered at two time points to a total of 27,000 employees of the executive branch of the Commonwealth of Kentucky. The short-term evaluation (March 2015) comprised 4,170 employees and the long term (August 2015) included 3,070. Tobacco use, plans to quit using tobacco, personal characteristics, whether the county of their workplace was covered by a smoke-free policy, and social norms for tobacco use were assessed 4- and 9-month post-policy implementation. Current tobacco use and plans to quit were compared between short- and long-term evaluations using multiple logistic regression with relevant covariates included. Controlling for demographics and employment location, employees reported lower rates of tobacco use and higher rates of planning to quit in the long term than in the short term. Tobacco-free policies reduce tobacco use prevalence and promote plans to quit, particularly over time. We found differences in tobacco use prevalence and plans to quit using tobacco products from 4 to 9 months after the policy took effect, as reported by employees following implementation of the tobacco-free policy. These findings support the potential for avoiding long-term health care costs as a result of reduced tobacco use from these policies. Nurses can play an important advocacy and policy evaluation role to promote and assess the impact of tobacco-free policies.
Tobacco use remains the single most preventable cause of death in the United States and is responsible for more than 480,000 deaths per year, including over 41,000 linked to exposure to secondhand smoke (U.S. Department of Health and Human Services [USDHHS], 2014). Tobacco-related illness costs more than $300 billion each year in the United States, including direct medical care and lost productivity costs to employers (USDHHS, 2014). Given the enormous impact of tobacco on our nation’s health and societal costs, there is a need to implement evidence-based tobacco control strategies, including comprehensive smoke- and tobacco-free policies (USDHHS, 2006, 2014).
Smoke-free laws (prohibition of smoking in indoor areas of worksites, restaurants, and bars) enhance the ability of smokers to quit smoking, decrease initiation, reduce exposure to secondhand smoke, and help change the cultural norms toward acceptability of smoking (USDHHS, 2006, 2014). Many communities have adopted comprehensive smoke-free workplace laws with approximately 50% of the U.S. population protected in 2015, compared with 2.7% in 2000 (Tynan et al., 2016). However, regional disparities remain, particularly in the southeastern states, many of which produce tobacco and lack comprehensive state smoke-free workplace laws (Tynan et al., 2016). As of January 1, 2019, only about one third of Kentucky’s population was protected through local comprehensive smoke-free laws (BREATHE, 2018).
Voluntary smoke-free workplace policies show promise in improving employee health by increasing rates of smoking cessation and reducing the number of cigarettes smoked per day among employees (Bauer, Hyland, Li, Seger, & Cummings, 2005; Fichtenberg & Glantz, 2002; Hopkins et al., 2010). Much of the research has focused on smoke-free workplace policy, as compared with tobacco-free policies. Tobacco-free policies extend to other types of tobacco products such as e-cigarettes, smokeless tobacco, cigars, and hookah and include both indoor and outdoor property. Given that tobacco-using employees incur significant health care costs to employers, not to mention the cost of excess absenteeism, decreased presenteeism, and increased costs for pension benefits, compared with those who do not use tobacco (Berman, Crane, Seiber, & Munur, 2014), comprehensive tobacco-free workplace policies are recommended. Research shows that comprehensive tobacco-free policies (i.e., those prohibiting the use of all tobacco products) are more effective than those prohibiting cigarette use only or those with designated smoking areas in reducing secondhand smoke exposure and intent to use tobacco (Fallin, Roditis, & Glantz, 2015).
Much of the workplace tobacco policy literature focuses on voluntary worksite tobacco policies (Brownson, Hopkins, & Wakefield, 2002; Hopkins et al., 2010). Less is known about mandated tobacco policies, particularly those adopted by state government. There is a dearth of literature on adoption of tobacco-free policies on state or government property. Legislatively mandated tobacco policies, including state-level clean air laws prohibiting smoking in any workplace, are among the most effective actions that can be taken to reduce smoking prevalence in the United States and around the world (Nagelhout et al., 2012). As of December 2018, five states had implemented tobacco-free policies on executive branch state government property, with varying degree of comprehensiveness: Delaware (State of Delaware, 2013), Kentucky (Beshear, 2014), Oklahoma (State of Oklahoma, 2012), Oregon (State of Oregon, 2012), and South Dakota (State of South Dakota, 2006). However, there is no research evaluating the effect of statewide governmental tobacco-free policy that covers all employees of the executive branch of government. Thus, as states adopt such policies, it is increasingly important to determine the potential impact these policies have on tobacco use behaviors.
On September 4, 2014, the then Kentucky Governor signed an executive order (2014-747) prohibiting the use of cigarettes, cigars, electronic cigarettes, and all other smoked or smokeless tobacco products on all property, indoors and outdoors, that is owned, leased, or contracted by the executive branch of the Commonwealth of Kentucky (Beshear, 2014). A few limited exceptions to the policy include outdoor areas of state parks, highway rest areas, state fairgrounds, and training centers operated by the Department of Military Affairs. Previously, only smoking inside the buildings occupied by executive branch employees had been prohibited, but the prior order did not cover smokeless tobacco or e-cigarettes, nor did it apply to outdoor spaces on executive branch property. Given the dearth of literature related to the impact of tobacco-free government property policies, research in this area is warranted.
Background
The Commonwealth of Kentucky is historically a pro-tobacco state given its long-standing record of tobacco growing and manufacturing. As a result, Kentucky has weak tobacco control policies, high tobacco use rates, and high tobacco-attributable morbidity and mortality (American Lung Association, 2018b; Campaign for Tobacco-free Kids, 2018). The other four states with tobacco-free government property policies have lower rates of tobacco use compared with Kentucky, with 16.2% to 19.6% of adults reporting cigarette smoking (Centers for Disease Control and Prevention [CDC], 2016) and 6.2% to 12.5% of high school students reporting cigarette smoking on at least 1 day in the past 30 days (CDC, 2017). Tobacco control policies, particularly smoke-free laws, in other states appear to be more stringent compared with Kentucky's laws, although each state has room for improvement (American Lung Association, 2018a).
The tobacco industry and their front groups typically oppose any smoking or tobacco use restrictions (American Nonsmokers Rights Foundation, 2016), as they can reduce tobacco use and affect company profits. Furthermore, policymakers with conservative ideology may view tobacco-free campus policies as an overreach of government (Filippidis, Girvalaki, Mechili, & Vardavas, 2017; Kehler & Hahn, 2016). While indoor smoke-free laws are more common, tobacco-free policies that restrict tobacco use inside and outdoors are a relatively new phenomenon for these reasons.
Methods
Purpose
The study’s purpose was to examine the short- and long-term effects of the executive order (2014-747) on tobacco use and tobacco quit behaviors. To our knowledge, this is the first evaluation of the impact of a large-scale tobacco-free policy implemented by a state government.
Design, Recruitment, and Sample
To evaluate the effect of executive order 2014-747, we administered cross-sectional online surveys at two different times to approximately 27,000 Commonwealth of Kentucky employees to measure tobacco use and quitting behaviors 4- and 9-month post-policy implementation. The University of Kentucky’s institutional review board approved the study on December 2, 2014 (Protocol #14-0914-X1B). and granted us a waiver of documentation of informed consent. We attached to each survey the institutional review board-approved cover letter explaining the study purpose, who was invited, time to complete the survey, and data confidentiality. The first survey was distributed via e-mail to all 27,000 executive branch employees in March 2015 (short-term evaluation), 4 months after the tobacco-free policy went into effect. A second, nearly identical (i.e., time since policy implementation changed) survey was sent to the same number of employees in August 2015 (long term), 9-month post-policy implementation. For both surveys, the e-mail invitation was distributed to employees’ work e-mail addresses by the Personnel Cabinet (i.e., human resources office for state government employees), in partnership with the Kentucky Office of Health Policy, and a reminder e-mail was sent one week after the initial e-mail.
A total of 4,854 state employees responded to the short-term survey (18% rate) and 3,522 responded to the long-term survey (13% rate). After omitting the data from those who had completely skipped the tobacco use (n = 338 short term, n = 236 long term) and demographic items (n = 681 short term, n = 451 long term), there were 4,170 employees in the short-term sample (15% effective response rate) and 3,070 in the long-term sample (11% effective response rate). Given the anonymous nature of the survey, it was not possible to follow-up with nonresponders individually or to describe their demographic characteristics.
Procedures
On March 3, 2015, the e-mail invitation to participate in the survey was sent by the Kentucky Personnel Cabinet to all executive branch employees and signed by the Commissioner of the Kentucky Department for Public Health, on behalf of the Principal Investigator. The e-mail invitation included an online link to the survey. Based on the logistics of governmental procedures and human subjects’ protection guidelines, the survey invitation was distributed in partnership with the Kentucky Office of Health Policy by the Personnel Cabinet. A reminder e-mail was sent to all employees 1 week later. The survey was administered using (Qualtrics, Provo, UT), a secure survey administration and database software package.
Measures
The survey assessed tobacco use in each employee group (short term and long term) through a series of questions related to use of cigarettes, hookah, cigars (including cigarillos or little cigars), smokeless tobacco (chewing tobacco, snuff, snus, or dip), and electronic cigarettes (e-cigarette, vape pen, and hookah pen) separately. Two questions assessed current cigarette use: (a) “Have you smoked at least 100 cigarettes in your life?” with “yes” or “no” responses and (b) “When was the last time you smoked a cigarette?” with responses including “ever smoked,” “today,” “1–7 days ago,” “8–29 days ago,” “1–3 months ago,” “4–6 months ago,” “7–11 months ago,” “1–4 years ago,” and “5 or more years ago.” Participants were categorized as current cigarette users if they indicated “yes” to having smoked at least 100 cigarettes in their lifetime and within the past 30 days.
For all other tobacco products, responses to two questions determined current use for each product: (a) “Have you used hookah/cigars/smokeless/e-cigarettes in the past 30 days?” with response options of “yes,” “no, not in the last 30 days,” and “I have never used hookah/cigars/smokeless/e-cigarettes in my life” and (b) “When was the last time you used hookah/cigars/smokeless/e-cigarettes?” with a response set identical to the analogous question for cigarettes. We coded participants as current users if they indicated they had used the specific product in the last 30 days.
One question assessed plans to quit using tobacco, “Which of the following best describes your plans to quit smoking cigarettes/using tobacco products altogether?” Response options included, “I am not thinking about quitting in the foreseeable future,” “I am thinking about quitting in the next 6 months,” and “I plan to quit in the next 30 days.” We categorized those who indicated planning to quit in the next 30 days as “yes” for planning to quit. For plans to quit smoking cigarettes, we only included current cigarette users. Similarly, for estimated plans to quit using tobacco altogether, we only included those indicating current use of any tobacco product (cigarettes/hookah/cigars/smokeless/e-cigarettes).
Personal characteristics included age (in years), gender, race, ethnicity, and county of employment. Response options for race included “White,” “Black or African American,” “Asian,” “Pacific Islander,” “American Indian, Alaskan Native,” and “two or more races.” Because a limited number of respondents identified as a racial/ethnic minority, we combined and dichotomized these options into “White/non-Hispanic” and “Other” for analysis. Response options for county of employment included all 120 counties in Kentucky. A binary variable was created to account for whether the respondent worked in a county with a comprehensive smoke-free ordinance; this was used to indicate region of employment (smoke-free county vs. not; BREATHE, 2018).
Data Analysis
Descriptive statistics were used to summarize personal characteristics, current tobacco product use, and plans to quit among survey respondents at each assessment. Comparisons of personal characteristics between 4- and 9-month respondents were analyzed using the two-sample t test, Mann–Whitney U test, or χ2 test of association, as appropriate. Current tobacco use status and plans to quit were compared between groups using multiple logistic regression. Covariates included in the models were personal factors (age, gender, and race/ethnicity) and an indicator for region of employment or whether the county of their workplace was covered by a smoke-free public policy. In the model for intending to quit smoking cigarettes, gender was limited to those indicating “male” or “female” due to convergence issues arising from complete separation (i.e., no participants identifying “transgender” indicated an intention to quit smoking cigarettes); all categories of gender were included in other models. Data analyses were conducted using SAS vs. 9.4 for Windows (Cary, NC), with an alpha level of .05 throughout.
Results
Comparison of Personal Characteristics of Survey Respondents at Short- and Long-Term Follow-Up.
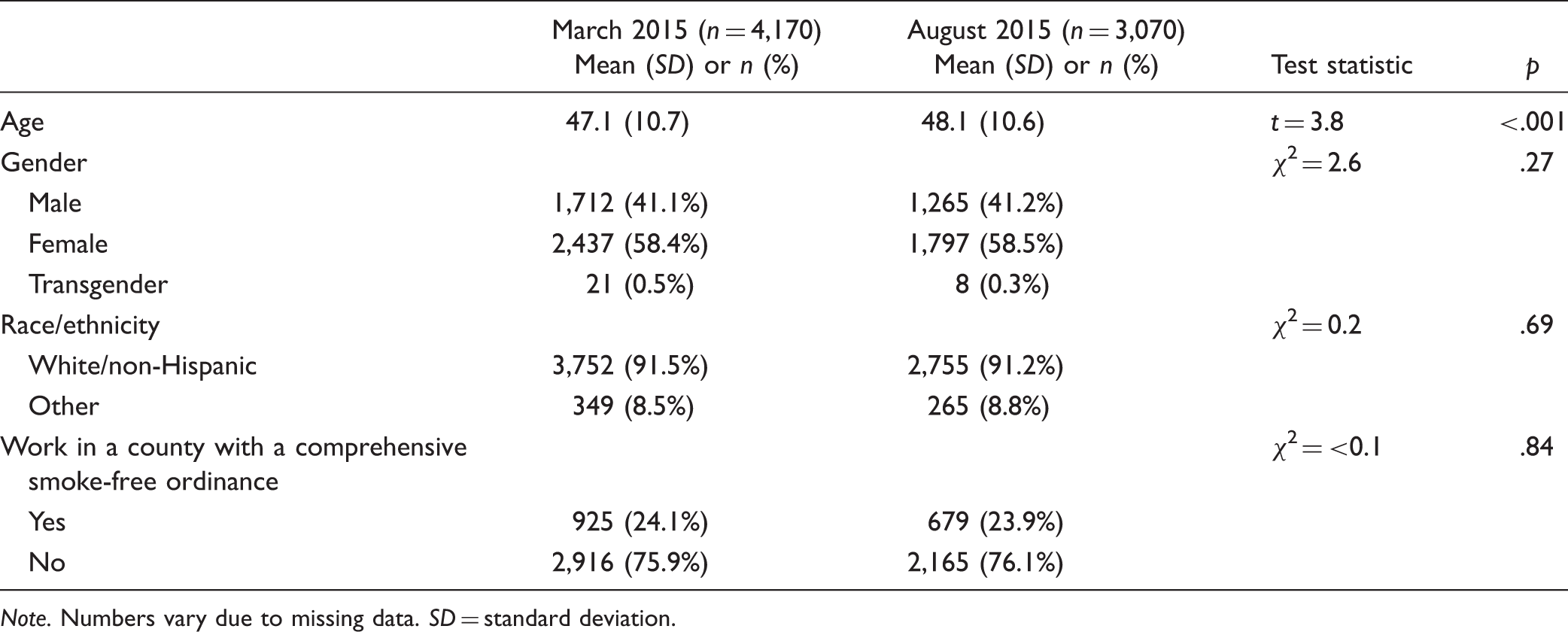
Note. Numbers vary due to missing data. SD = standard deviation.
Tobacco Use
Percentage of Current Tobacco Users by Product and Time of Survey at Short- and Long-Term Follow-Up.
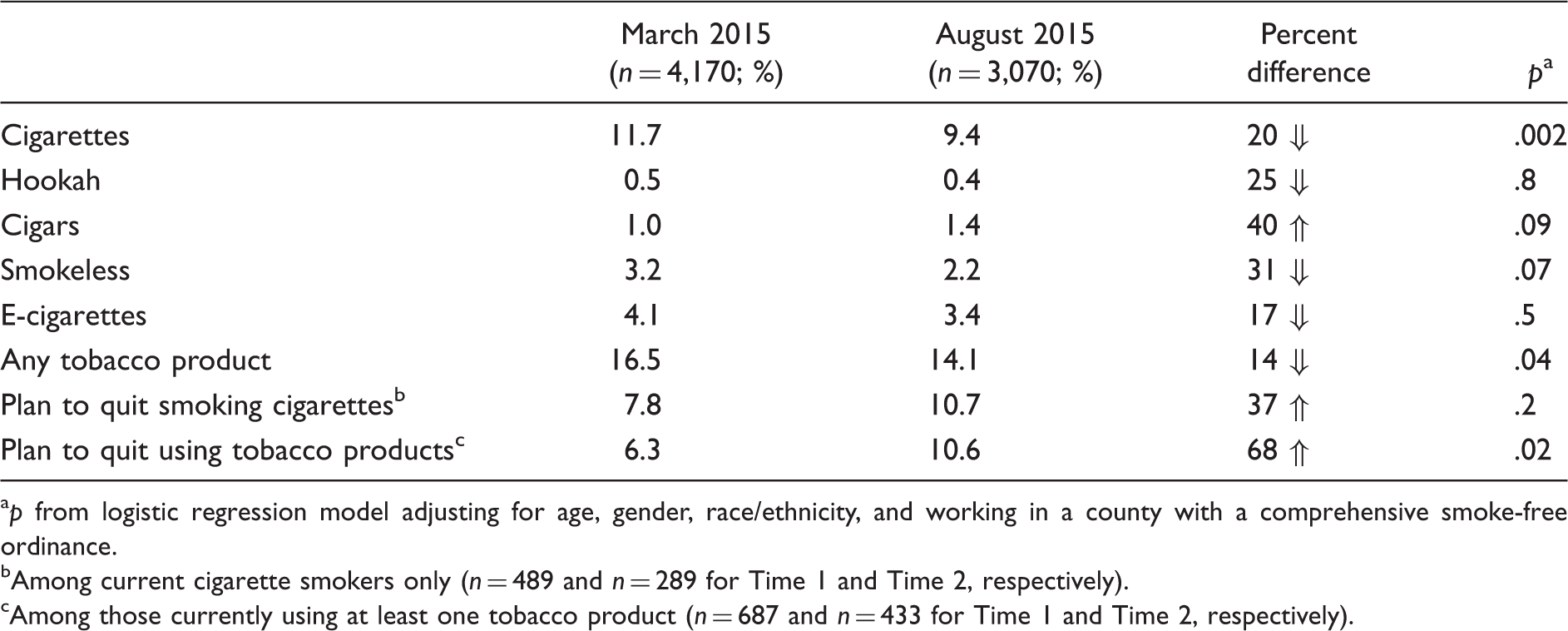
ap from logistic regression model adjusting for age, gender, race/ethnicity, and working in a county with a comprehensive smoke-free ordinance.
bAmong current cigarette smokers only (n = 489 and n = 289 for Time 1 and Time 2, respectively).
cAmong those currently using at least one tobacco product (n = 687 and n = 433 for Time 1 and Time 2, respectively).
Controlling for demographic and personal factors (age, gender, race/ethnicity, and comprehensive smoke-free public policy in county of employment), employees were significantly less likely to use cigarettes in 9-months post-policy compared with 4-months post-policy (p = .002); there was a 20% difference in frequency of use between those who responded to the short-term and long-term surveys, with less use in the latter group. In addition, the prevalence of use of any tobacco product indicated a significant difference between the two time points (p = .04); the percent difference for this indicator was 14% less. The difference in prevalence for each of the other individual tobacco products was not significant between the short- and long-term assessments.
Plans to Quit Using Tobacco
Controlling for age, gender, race/ethnicity, and employment in a county with a smoke-free policy, there was no significant difference between March and August 2015 in the percentage of current cigarette smokers who planned to quit in the next 30 days (7.8% and 10.7%, respectively). However, the percentage of employees reporting any tobacco use within the last 30 days who planned to quit in the next month was significantly different between the two groups (6.3% in March; 10.6% in August; p = .02). In both the 4- and 9-month post-policy implementation groups, the percentage of those reporting smoking in the previous 6 months who said they had also attempted to quit smoking cigarettes in the previous 6 months remained constant at 32%. Those who reported attending smoking cessation classes, talking to a health care provider about quitting, or calling 1-800-QUIT-NOW did so at roughly the same rate in March (24%) and August (28%; p = .13).
Discussion
Kentucky Governor Beshear’s Executive Order (2014-747) prohibiting the use of all tobacco products on nearly all executive branch property was effective in reducing cigarette smoking and any tobacco use among employees. Employees were significantly less likely to use cigarettes 9-months post-policy compared with 4-months post-policy; use prevalence of any tobacco product by the long-term group of participants was 14% less than corresponding use prevalence of any tobacco product by those in the short-term group. Considering this study is the first to evaluate the impact of a mandated tobacco-free policy on governmental property, the success of the policy in lowering tobacco use rates has implications for health policy decisions in other states. Only four other states have adopted tobacco-free policies comparable to the one implemented in Kentucky. The results of our study provide the evidence supporting the potential impact of tobacco-free policies as more states consider adoption of these policies. Future studies are needed to compare changes in tobacco use behaviors and associated health care cost savings outcomes pre-policy and long term, as states adopt similar policies to provide additional support for comprehensive tobacco-free policies. There is also a need to determine whether outcomes vary across states with differing tobacco use rates and strength of tobacco control policy and programs.
The findings of this study reinforce the importance of comprehensive tobacco-free policies that include all tobacco products, including e-cigarettes (Fallin et al., 2015). Differences in tobacco use across multiple products between 4- and 9-months post-policy were reported by employees. There is much concern among health professionals and the public health community about dual or polyuse of tobacco products (i.e., current use of more than one tobacco product) that may interfere with successful quitting and increase associated health risks (Agaku et al., 2014; Sung, Wang, Yao, Lightwood, & Max, 2015). Comprehensive tobacco-free policies may be beneficial in decreasing the prevalence of polytobacco use, although further research is needed.
Over time, current tobacco users were significantly more likely to plan to quit in the next 30 days, from 6.4% at 4 months to 10.3% at 9-months post-policy implementation. Although there was no significant difference over time in percentage of current cigarette smokers who planned to quit in the next 30 days, 8.3% and 10.6% of current cigarette smokers reported intention to quit at the two time points, respectively. Nationally, approximately 70% of current smokers want to quit (CDC, 2011). Similar data are not available for users of other tobacco products. Kentucky reports the lowest proportion of smokers who report a quit attempt in the past year (Lavinghouze et al., 2015). In a state with continually high rates of tobacco use, Executive Order 2014-747 prompted individuals’ intention to quit tobacco, which may lead to quit attempts. Among employees in this study, fewer than 3 in 10 tobacco users took advantage of quit resources: 24% of current tobacco users in March and 28% in August reported they had attended a smoking cessation class, talked to a health care provider, or called 1-800-QUIT-NOW in the previous 6 months. These findings reinforce the need to promote and offer a sustained menu of accessible and affordable evidence-based tobacco treatment options (Fiore et al., 2008) prior to the implementation of such policies and to continue offering a menu of options once the policy takes effect and over time.
Strengths and Limitations
This is the first study to evaluate the impact of a mandated tobacco-free policy on governmental property and includes a large sample size of employees in a tobacco growing state. Previous research focused on voluntary smoke-free workplace policies, and although these policies increase rates of smoking cessation and reduce the number of cigarettes smoked per day among employees (Bauer et al., 2005; Fichtenberg & Glantz, 2002; Hopkins et al., 2010), this study reinforces the impact comprehensive tobacco-free policies have on overall tobacco use among employees.
The primary limitation of this study was the recruitment of two groups of employees, one short term and the other long term, but both after the tobacco-free policy went into effect. There are inherent methodological challenges in measuring the effectiveness of the tobacco-free policy, including inability to follow the same employees and maintain anonymity in this relatively large and fluctuating group of potential participants. Related to the requirement for anonymity, we were not able to track respondents and follow-up with targeted reminders. We recommend that researchers create confidential identifiers to be able to link responses over time in future policy evaluation studies. Furthermore, 2% to 3% of respondents in each employee group omitted demographic information and could not be used in these analyses. In addition, although the relatively low response rates are consistent with most e-mailed surveys (Dillman, Smyth, & Christian, 2009), these rates could not be determined precisely as we were not able to monitor either the exact number of survey invitations distributed or the number of surveys that were not received by the intended recipient. Furthermore, current tobacco users may have been less inclined to participate in this survey, which may also be reflected in the response rate. Finally, we had minimal representation of racial/ethnic minority groups in the samples. Although similar to the demographic profile of the state, results obtained here may not be generalizable to areas with more diverse populations.
Implications for Research, Policy, and Practice
The findings of this evaluation support implementation of comprehensive tobacco-free government property policies and confirm the achievement of one of the primary goals of Executive Order 2014-747 to positively impact tobacco use among employees. Tobacco use is a significant driver of health care expenditures (Xu, Bishop, Kennedy, Simpson, & Pechacek, 2015); thus, states need to consider adopting tobacco-free policies as a means of decreasing future health care costs from tobacco-related disease. It is estimated that excess annual costs to employers per smoking employee are $5,816 per employee and that these costs can be eliminated when employees quit smoking (Berman et al., 2014). These data may also be relevant to other large organizations (e.g., worksites, universities, hospitals) considering adoption of tobacco-free policies, given the positive impact on employees’ tobacco use and tobacco quit patterns. The broad impact these policies can have on the health and well-being of employees and the community needs to be reinforced to encourage other states to implement similar comprehensive policies restricting the use of tobacco products on all state government properties.
Nurses have an enormous role to play in promoting tobacco-free policies in the United States and around the world (Hyland, Barnoya, & Corral, 2012). Given the momentum in enacting and implementing smoke-free policies globally as prompted by the World Health Organizations’ Framework Convention on Tobacco Control, the first global public health treaty (Gneiting, 2016), nurses are well positioned to form alliances to advocate for comprehensive smoke- and tobacco-free policies (Framework Convention on Tobacco Control Article 8; Hyland et al., 2012). Nurses are prepared to mobilize grassroots organizations and multiple stakeholders to build capacity for smoke-free campaigns (Hyland et al., 2012), translate and disseminate science, and build demand for policy development and effective policy implementation (Hahn et al., 2014). In addition to policy advocacy, nurse researchers can evaluate the health impacts of smoke- and tobacco-free policies globally (Gneiting, 2016), as in the study reported here. As countries and municipalities around the world enact and adopt these policies, there is a need for nurses and their multidisciplinary partners to monitor policy outcomes, especially among disparate populations, and policy implementation effectiveness (e.g., adherence to the policies; Ickes, Wiggins, Rayens, Edwards, & Hahn, 2018).
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported through a contract between the Kentucky Department for Public Health Tobacco Prevention and Cessation Program and the University of Kentucky Research Foundation.