
Abstract
Background
Despite the importance of involving nurses in health policy, nurse’s involvement faces many challenges. Literature showed that there is a low level of nurses’ and nurse leaders’ involvement in health policy development.
Aim
The aims of this study were to examine (a) the level of Jordanian head nurses’ involvement in health policy development and their perceived benefits and barriers; (b) the relationships between level of knowledge, competence, and interest in health policy and the level of involvement in health policy development; and (c) the relationship between the level of self-efficacy (efficacy expectation and outcome expectation) and the level of involvement in health policy development.
Methods
A cross-sectional descriptive correlational study design was adopted in this study. A convenience sampling of 250 participants from hospitals affiliated to three health sectors in Jordan (private, governmental, and university) were recruited to complete a self-administered questionnaire. Descriptive statistics and Pearson correlation coefficient were used to answer the study questions.
Results
The results revealed a moderate level of involvement of head nurses in the policy development. The most frequent cited political activity was “providing written reports, consultations, research.” “Lack of time” was the most perceived barrier, while “improving the health of the public” was the most perceived benefit. Workshops or sessions at conferences is the most indicated source of knowledge. Participants had an excellent level of skills with positive relationships between the competence and both of the levels of professional and personal involvement in health policy. Participants reported a low level of confidence in performing political activities as well as the impact of such activities on health outcomes. Positive relationship was indicated between self-efficacy and the levels of professional and personal involvement in political activities.
Health policies focus on the health and well-being of the general population through addressing the issues of cost, quality of care, and accessibility for health care services. Policies reflect the values, beliefs, and attitudes of the persons who made those policies (Etowa et al., 2016). Health policy is defined as “the decisions made to promote the health of individual citizens” (Mason et al., 2013, p. 10). Thus, in order to achieve common goals, all health care professions should be represented and have an input in the decisions related to health policy (Asuquo et al., 2013).
The aim of health policy is to support individuals and shape the practice and workplaces at all levels (Salvage & White, 2019). Nurses are the major health care providers in the health care sector; they are considered as the backbone of the health care system (Asuquo et al., 2013). There are many reasons behind the call for involving nurses in any position in health policy development. Since nurses are the end users of health policies (Salvage & White, 2019), they should have an active role in its development to impact the health and well-being of the general population development, and to ensure that the health services are safe, effective, available, and reasonable (Kunaviktikul, 2014; Shariff, 2015a). Nurses’ involvement in health policy will make them more influential (Avolio, 2014).
Head nurses are the first-line managers who have responsibility and accountability for one or more working unit. Involving head nurses in the policy development process will make the policies that are taken closer to the nurses and reflect the voices and best decisions for them. Nurse leaders’ involvement in policy development can renew and rebound the public image about nursing which will enhance the respect from other professions and achieve equal partnership (Shariff, 2015b). Head nurses should have competence in policy development and implementation and should be empowered and supported to enhance their participation in health policy development (Shariff, 2015b). Furthermore, the involvement of head nurses in health policy development will also support nurses’ involvement, as they are considered as liaison which will support the nursing position in the health policy arena. Nurses in their different positions should activate their role in policy development and understand all its aspects: the policy process, context, stakeholders, and their interests (Salvage & White, 2019). Therefore, head nurses and nurse leaders, in general, have an important role in supporting, mentoring, and developing future nurse policymakers (Shariff, 2014).
Despite the importance of involving nurses in health policy, nurse’s involvement faces many challenges (AbuAlRub & Foudeh, 2017). Literature showed that there is a low level of nurses’ and nurse leaders’ involvement in health policy development. Using a Delphi survey, Shariff and Potgieter (2012) conducted a study to explore the extent of the nurse leader’s participation in health policy development with a sample of 78 nurse leaders working in national or provincial leadership positions in the three East African countries of Kenya, Uganda, and Tanzania. The study results revealed that nurse leaders input in the health policy development process was confined to the implementation stage. The participants were not involved in the health policy development process; they were just members of professional organizations. Furthermore, Ditlopo et al. (2014) and Asuquo et al. (2013) concur with the findings concerning the low level of involvement of nurse leaders and nursing directors as professionals and citizens in health policy development.
Several researchers emphasized the importance of the role of nurse leaders and nurses at any administrative level in activating nurse’s involvement in health policy development (Ditlopo et al., 2014; Shariff, 2014; Shariff & Potgieter, 2012). To overcome the obstacles that face head nurses’ involvement and increase their level of involvement in health policy development, several research studies investigated the barriers to nurse leaders’ involvement in health policy development. Examples of such barriers are lack of knowledge and skills about health policy, lack of collective actions among nursing stakeholders, the negative image of nursing, not being involved, lack of enabling structure and process, lack of public understanding, financial factors, and resources limitations (Avolio, 2014; Ditlopo et al., 2014; P. A. Juma et al., 2014; Salvador, 2010; Shariff, 2014).
To have a behavioral change, an increase in the confidence level in doing activities as well as the belief that one’s actions could affect outcome should be done (Bandura, 1977). Self-efficacy has a big effect on behavioral change (Bandura, 1977), which includes efficacy expectations and outcome expectations. These two components of self-efficacy are interdependent; because a behavioral change will not take place if a person believes that behavior will have an impact on outcome (outcome expectation), while he/she is not confident of his/her ability to change that behavior (efficacy expectation) (Bandura, 1977). Thus, understanding the relationship between self-efficacy and involvement in health policy can be important to policymakers and nursing organizations who have the attempts to activate head nurses’ role in health policy development. A positive relationship was found between self-efficacy and level of involvement in health policy (Salvador, 2010).
In a research study that was conducted in Jordan by AbuAlRub and Foudeh (2017) to investigate the registered nurses’ involvement in health policy development, the results revealed that there are low levels of involvement of Jordanian nurses in health policy development. One of the recommendations from AbuAlRub and Foudeh study was that head nurses should be role models for nurses and should support them to be involved in health policy development. Little research if existed had investigated the actual head and senior nurses’ level of involvement in health policy development in the Middle Eastern Region including Jordan. Thus, this study will investigate the extent of the head nurses’ involvement in health policy activities in Jordan. The study findings will shed light on the involvement of nurses in management positions in health policy development. The aims of this study are to examine (a) the level of Jordanian head nurses’ involvement in health policy development and their perceived benefits and barriers; (b) the relationships between level of knowledge, competence, and interest in health policy and the level of involvement in health policy development; and (c) the relationship between the level of self-efficacy (efficacy expectation and outcome expectation) and the level of involvement in health policy development.
Methods
Study Design
A correlational cross-sectional descriptive research design was used in this study.
Setting
The targeted hospitals for this study were selected conveniently from three sectors to represent the health system in Jordan which were three private hospitals, one governmental hospital, and one university-affiliated hospital.
Population and Sample
The target population was Jordanian head nurses and senior nurses (in charge nurses who assume the same role of head nurses in other shifts) who are currently working in Jordanian hospitals. The accessible population was head nurses working at the targeted hospitals. According to the rule of thumb formula (number of variables in the study × 10 + 50), 15 × 10 + 50 = 200 participants were needed for this study (VanVoorhis & Morgan, 2007). There are 15 variables in the study: 7 demographics (gender, age, marital status, level of education, years of experience in nursing and in the current work area, type of hospital, and work unit) and 8 main variables (perceived benefits, perceived barriers, level of involvement, level of knowledge, competence, interest, efficacy expectation, and outcomes expectation).
Inclusion criteria for this study sample were male and female nurses who had a working experience of at least 2 years as a head nurse or in charge nurse in the targeted hospitals. A convenience sampling method was used in this study. All head nurses and senior nurses who were willing to participate at the time of data collection in the targeted hospitals and met the inclusion criteria were invited to participate in this study. As the sample is a convenience one and to consider nonusable questionnaires, 320 surveys were distributed. A total number of 250 head nurses and senior nurses completed usable questionnaire with a response rate of (78.1%).
A self-administered questionnaire, consisted of 79 items, revised by Salvador in 2010 (Registered Nurses Involvement in Health Policy) was utilized to assess the variables of the study. The modified instrument was tested by Salvador for its reliability and validity and was determined as a valid and reliable instrument (Salvador, 2010). The instrument which was used in this study was also used with Jordanian nurses in a previous study conducted by AbuAlRub and Foudeh (2017) to assess the level of registered nurses’ involvement in health policy and the Cronbach’s alpha.
Involvement in health policy, defined as “an activity that has the intent or effect of influencing government action—either directly by affecting the making or implementation of public policy, or indirectly by influencing the selection of people who make those policies” (Verba et al., 1995, p. 38), was assessed by a list of 15 political activities for which participants were asked to select those in which they were involved. Involvement in trying to influence health policy as a professional and as a citizen was assessed by two items on a Likert-type scale from 1 to 5, in which (1 = not involved and 5 = very involved). A score of 1 to 2 was considered as a low level of involvement; a score of 3 was considered as moderate level of involvement; and a high level of involvement was assigned a score of 4 to 5 (Salvador, 2010). The level of knowledge was tested by asking participants if they had received any education or training about ways to change health policy, and if yes, they were asked to identify their sources by a list of seven sources.
Perceived barriers, defined as factors that may prohibit persons from acting to obtain their goals (Glanz et al., 2002), was measured by asking the participants to choose from a list of 17 barriers (Salvador, 2010).
Perceived benefits, defined as the positive outcomes as a result of certain actions (Glanz et al., 2002), were measured by asking the participants to choose from a list of 14 items (Salvador, 2010).
Outcomes’ expectation, defined as “a person’s estimate that a given behavior will lead to certain outcomes” (Bandura, 1977, p. 193), was measured by a list of 15 health policy activities in which participants rated their perceptions of the impact of their involvement in policy activities on health outcomes on a Likert scale of 1 to 5 (1 = no impact and 5 = major impact; Salvador, 2010). A score of 1 to 2 indicates that participant felt the activity would have a low impact on health outcomes, a score of 3 indicates moderate impact, while a score of 4 to 5 indicates a high impact on health outcomes. The minimum cumulative score was 16 if participants felt that these activities would have no impact on health outcomes, and the maximum cumulative score of 80 if the participant felt that all the listed activities have a major impact on health outcomes. In response classification, a score of 16 to 32 indicates low outcome expectations, 33 to 63 indicates moderate outcome expectations, and a score of 64 to 80 indicates high outcome expectations.
Efficacy expectation, defined as “the conviction that one can successfully execute the behavior required to produce outcomes” (Bandura, 1977, p. 193), was measured by the same list of 15 political activities for which the participants were asked to rate their confidence in being able to perform those activities on a Likert-type scale of 1 to 5 (1 = not confident and 5 = very confident).
The instrument also included a number of background variables including gender, age, marital status, educational level, type of hospital, working years as head nurse or charge nurse in current work area, and work unit.
Ethical Considerations and Data Collection Procedures
Approvals from the institutional review boards of the affiliated university and the targeted hospitals were obtained before starting the data collection. The purpose and importance of the study were explained for the study participants. The researcher explained that their participation is voluntary, and they could withdraw from the study any time they wanted without any penalties. Anonymity and confidentiality of participants were ensured. Participants were informed that only the results will be used and shared for the research purpose and no one will access the data except the researchers. Data were collected by one of the researcher who was available for responding, explaining and answering participant's concerns and questions. Data collection was done between August and September 2019. The data were coded and kept in closed envelopes with the researcher. All head nurses and in-charge nurses in the targeted hospitals at the time of data collection were invited to participate in the study. The questionnaires were distributed, and time was set to collect completed ones when they were ready according to the convenience of participants.
Data Analysis
Data in this study were analyzed using the Statistical Package for Social Science (SPSS) version 22. Descriptive statistics were used to describe the level of involvement, perceived barriers and benefits, self-efficacy, interest in health policy, and demographic data. Data were tested for normality. The results indicated that the data were not normally distributed, thus non parametric tests were used Spearman’s Rho correlation coefficient which was used to examine the relationships between study variables at the significant level of <.05.
Results
Demographic Characteristics
The mean of participants’ age was 34.76 (standard deviation [SD] = 6.43). The majority of participants were females (n = 149, 60.3%) and married (n = 173, 70.6%). Most participants (n = 164, 65.9%) had a bachelor’s degree in nursing, followed by 36 (14.5%) who had a diploma degree. The employment setting for study participants was as follows: 116 (46.4%) were from the governmental hospital; 68 (27.2%) were from private hospitals; and 66 (26.4%) were from the university-affiliated hospital. The most frequently identified work unit was medical/surgical (n = 85, 34.0%). The majority of participants had 6 to 10 (n = 85, 41.5%) years of experience, with a mean of 9.32 (SD = 5.71). The characteristics of participants are presented in Table 1.
Sociodemographic Characteristics of the Participants (N = 250).
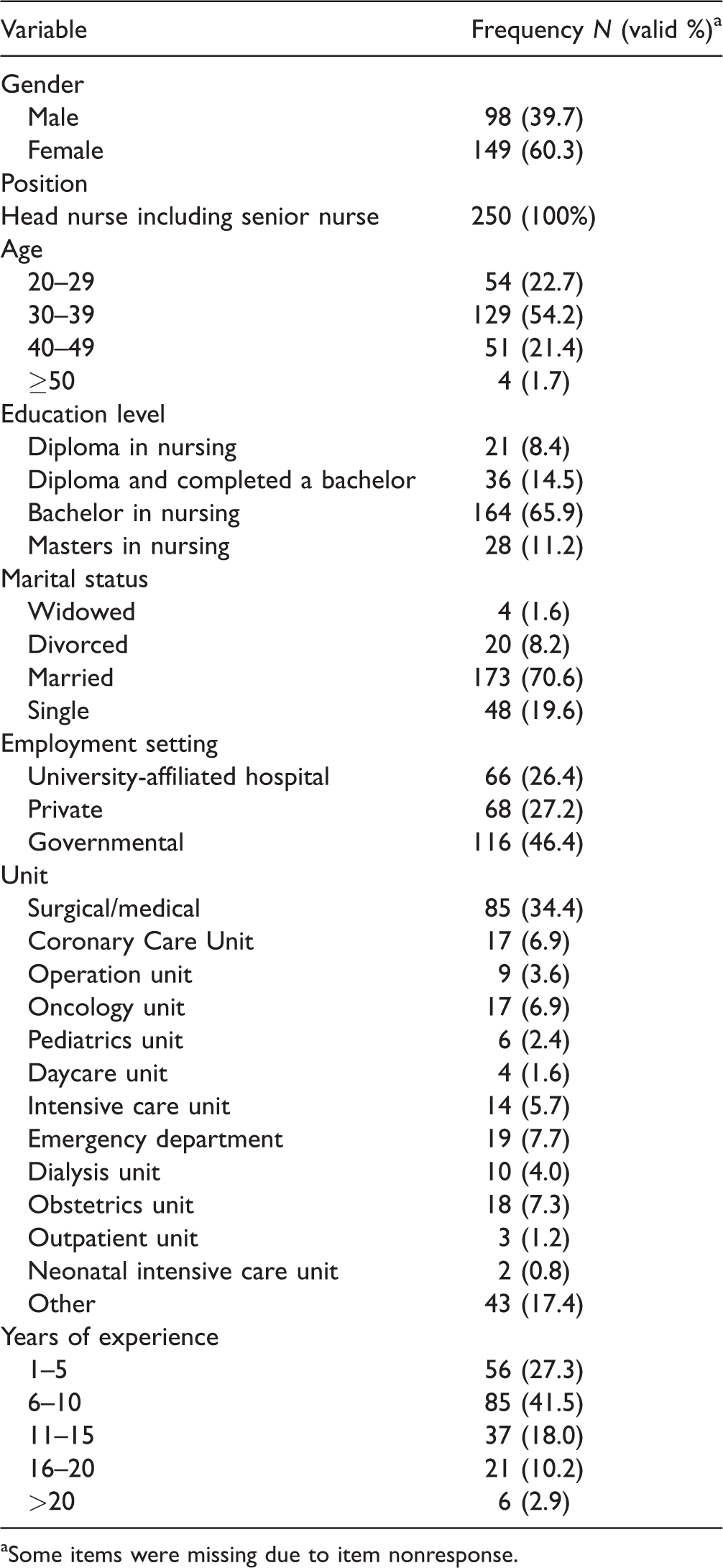
aSome items were missing due to item nonresponse.
Level of Head Nurses Involvement in Health Policy Development
The results showed that the median score of participants’ level of involvement in health policy activities as professionals was three (mean = 3.26, SD = 0.83). The median score for level of involvement in health policy activities as citizens was also three (mean = 3.06, SD = 1.11), indicating a moderate level of involvement as professionals and citizens. The median score of participants’ interest to influence health policy was also three, which indicates a moderate level of interest by study participants to influence health policy.
Concerning the involvement of head nurses in political activities, the results showed that 47 participants indicated that they were not engaged in any political activities (18.8%); 73 participants (29.2%) were engaged in more than five political activities; 31 participants (12.4%) were engaged in three political activities; and 34 participants (13.6%) were engaged in one political activity.
The most frequently chosen political activity was “providing written reports, consultations, research, or other assistance to a public official or for a health issue” (37.2%), followed by “contacting a public official or their office regarding a health issue” (32.8%), then “providing health policy-related information to consumers or other professionals” (31.2%). The results of participation in political activities by head nurses are shown in Table 2.
Head Nurses’ Participation in Politically Oriented Activities.
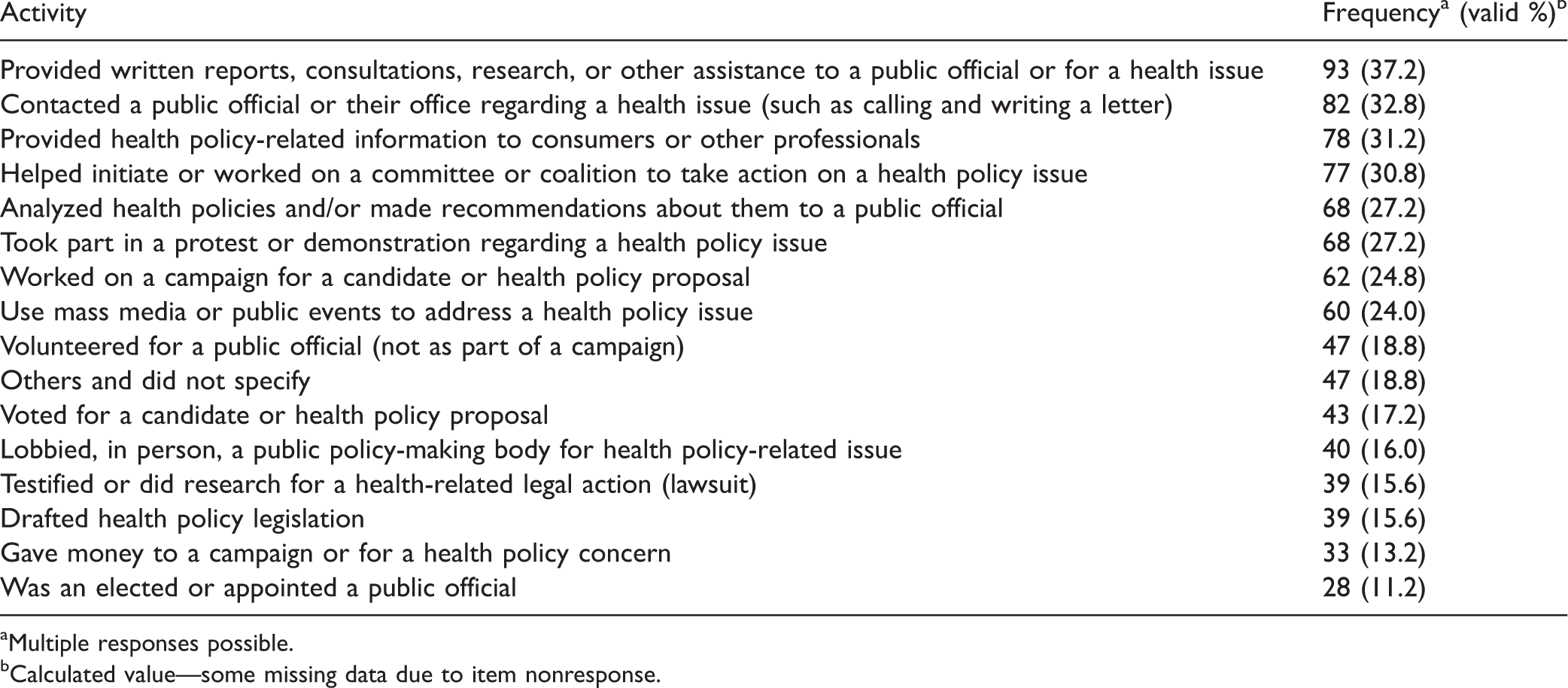
aMultiple responses possible.
bCalculated value—some missing data due to item nonresponse.
Perceived Benefits and Barriers of Head Nurses' Involvement in Health Policy Development
The results showed that the most cited barriers by participants were lack of time (61.6%), followed by lack of support from others (47.6%), and then lack of money/resources (39.2%). Few participants (14.8%) citied no barriers to being involved. Perceived barriers to involvement in health policy activities are presented in Table 3.
Frequency Distribution of Perceived Barriers to Involvement in Health Policy Activities as Perceived by Head Nurses (N = 250).
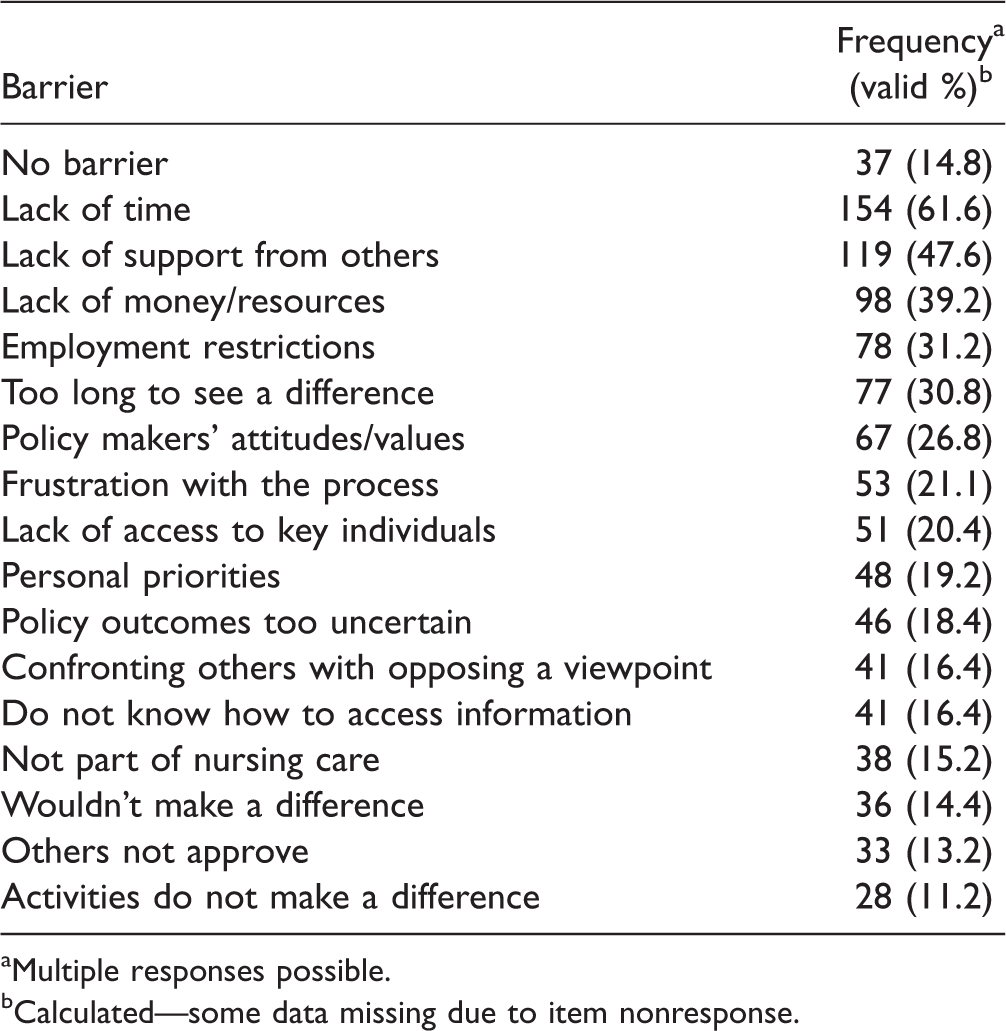
aMultiple responses possible.
bCalculated—some data missing due to item nonresponse.
Concerning the benefits of involvement in political activities, the results showed that the most cited benefit was improving the health of the public (56.8%), followed by improving situation/issue (47.6%), and then developing new skills (42.4%). However, 12.8% of participants perceived no benefits. The perceived benefits to involvement in health policy activities are presented in Table 4.
Frequency Distribution of Perceived Benefits to Involvement in Health Policy as Perceived by Head Nurses (N = 250).
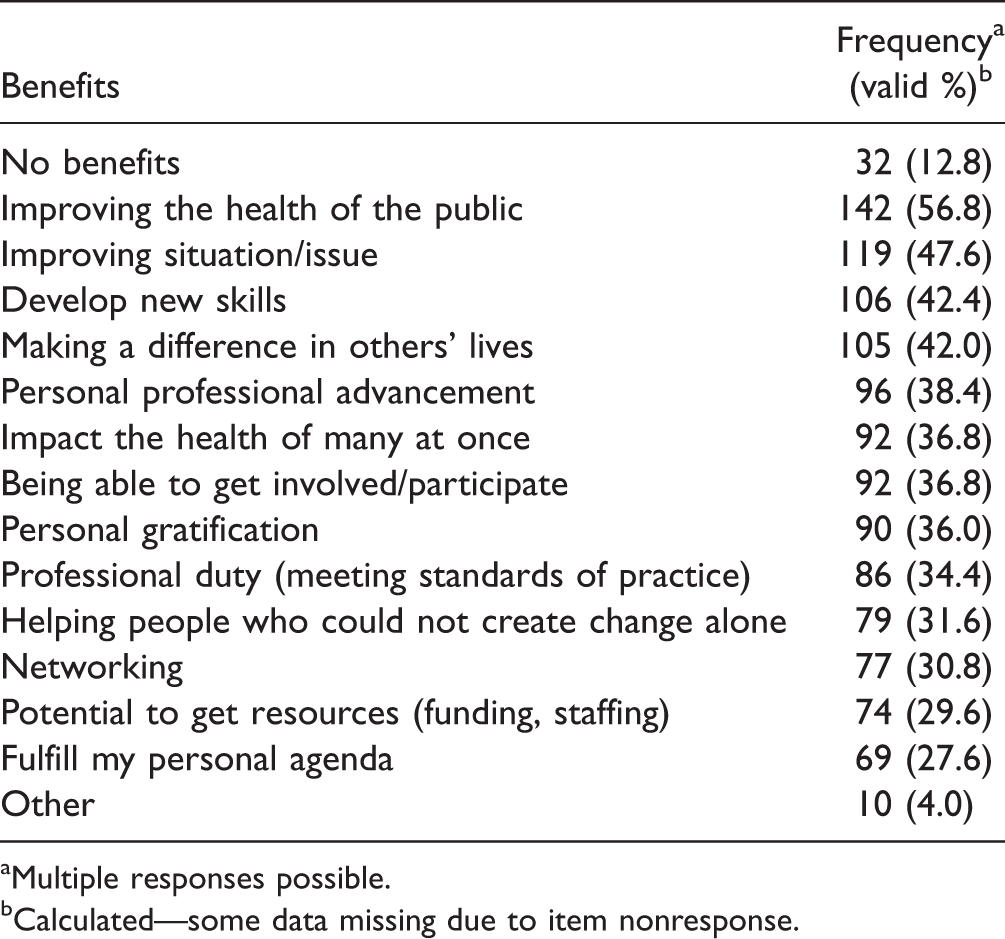
aMultiple responses possible.
bCalculated—some data missing due to item nonresponse.
Levels of Knowledge and Skills in Health Policy
The results showed that 91 of 250 respondents indicated that they had not received any education or training about ways to change in health policy. For those who did receive education or training, 56.6% (n = 90) of respondents indicated the source of education they had which was workshops or sessions at conference, followed by on the job experience (54.7%), college coursework (45.3%), and materials from professional organizations (40.3%). On the other hand, the sources from a professional colleague (30.8%), mass media (30.2%), and professional journals (30.2%) had a similar frequency response. Furthermore, more than half of participants (57.3%) rated their skills as excellent, 29.4% of participants rated their skills as moderate, and 13.3% rated their skills as poor.
A Spearman’s Rho correlation coefficient indicated that as participants’ level of skills increased, their perceived level of involvement as professionals (r = .21, p = .001) as well as citizens (r = .25, p < .001) increased as well. However, there was no relationship between the level of skills and the number of political activities in which participants were engaged in (r = .02, p = .76).
Outcome Expectations and Efficacy Expectations
The median score for the perceived impact of involvement in health policies on health outcomes was 29 (mean = 29.204, SD = 8.3) indicating that participants felt that involvement in policy activities had a low level of impact on health outcomes. On the other hand, the median score for efficacy expectations was 29 (mean = 28.74, SD = 7.55) which indicated participants perceived a low confidence level in performing the given political activities.
The Spearman’s Rho correlation coefficient indicates a significant positive relationship between efficacy expectations and involvement in health policy development as professionals (r = .32, p < .001) as well as citizens (r = .24, p < .001). In other words, the level of involvement as professionals and citizens increased when the self-rated level of confidence in performing political activates increased. However, there was no significant relationship between efficacy expectation and number of political activities (r = .089; p = .196). Similarly, the Spearman’s rho correlation coefficient indicates a significant positive relationship between outcome expectations and involvement in health policy development as professionals (r = .20, p = .003) as well as citizens (r = .14, p = .04). There was no significant correlation between outcome exceptions and number of political activities. The relationship between efficacy expectation and level of involvement in health policy are shown in Table 5.
Relationship Between Efficacy Expectation and Level of Involvement in Health Policy.
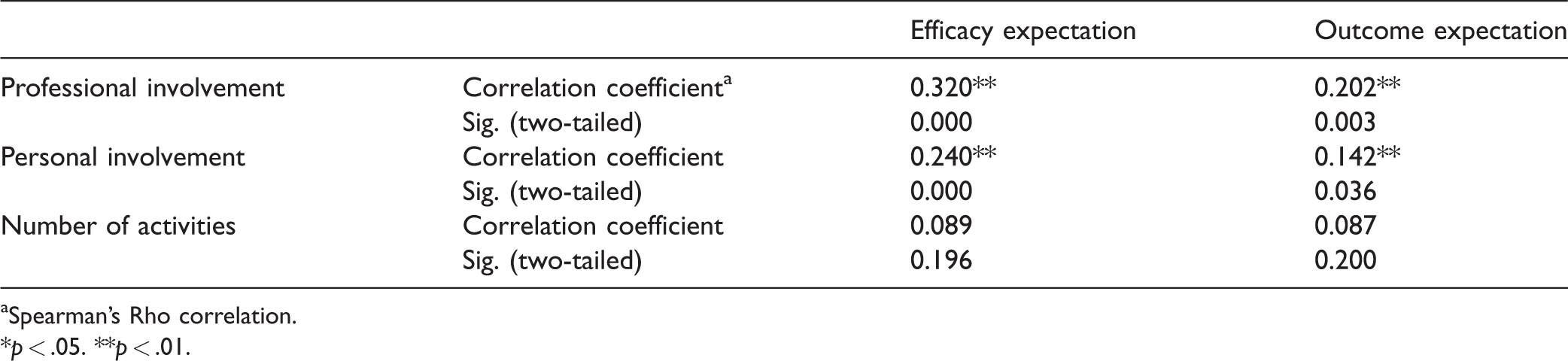
aSpearman’s Rho correlation.
*p < .05. **p < .01.
Discussion and Implications
Level of Head Nurses Involvement in Health Policy Development
The study results indicated that head nurses were moderately involved in health policy development both as professionals and citizens. Previous research studies indicated a low and limited level of nurses leaders’ involvement in health policy development (Ditlopo et al., 2014; Shariff, 2014; Shariff & Potgieter, 2012). This difference in results could be explained by the different research designs and instruments that were used by researchers to assess level of involvement in health policy development. For example, Shariff and Potgieter (2012) used a Delphi design and a self-reported questionnaire that was developed by the researchers based on literature. Furthermore, the results indicated that the level of interest to influence health policy was moderate, which is congruent with the results from other studies in the literature (AbuAlRub & Foudeh, 2017; Salvador, 2010).
The study results also indicated that the most frequently chosen political activity was “providing written reports, consultations, research, or other assistance to a public official or for a health issue,” followed by “contacting a public official or their office regarding a health issue.” Research studies that addressed the registered nurses’ involvement in health policy development indicated that voting was the most cited activity by nurses (AbuAlRub & Foudeh, 2017; Avolio, 2014; Salvador, 2010; Vandenhouten et al., 2011). The reason behind that is unlike nurses, head nurses have more chances to be part of political activities because of their position and their job responsibilities.
The results of the study also indicated that the most cited benefits of being involved in health policy development were “improving the health of the public,” and “improving situation/issue.” Such results were similar to the results of AbuAlRub and Foudeh’s (2017). These findings engrained in the nursing profession as a selfless profession and its code of ethics that call for helping their communities and improving health.
On the other hand, the most citied barrier in this study was “lack of time,” followed by “lack of support from others,” which is also consistent with the results (AbuAlRub & Foudeh, 2017; Avolio, 2014; Salvador, 2010). The barrier of “lack of time” can be explained by the fact that nurses have family roles as well as work roles which might impede their involvement in health policy activities. “Lack of support from others” might be due to the decision-making style which is centralized and the climate of the organization which is usually unsupportive (AbuAlRub & Foudeh, 2017). All these barriers can be overcome by nurses at the executive level who should strongly support them so that this will facilitate their involvement (Richter et al., 2013).
This study results indicated that 36.4% of head nurses responded that they did not receive any education or training about ways to change health policy. While for those who did, the most indicated sources were from “workshop or sessions at the conference” and from “job experience.” Such results suggest that health care organizations are not working on introducing important concepts such as is health policy and its development that affect their profession. Furthermore, nursing education programs should increase their focus on equipping nurses with necessary knowledge and skill in health policy development to facilitate their engagement in the process.
The results of the study indicated a positive relationship between the level of competence (gaining skills in health policy) and the level of head nurse’s involvement in health policy development. This means, as the level of competence enhanced, the level of involvement of head nurses in health policy development increased. Thus, facilitating nurse leaders’ involvement in health policy could enrich their competences, level of confidence, and their whole experience in the process (Shariff, 2014).
The study results also indicated that participants had a low confidence level in performing the given political activities and in the impact of these activities on health outcomes. Such results were congruent with the results of O'Rourke et al (2017) and Salvador (2010). The results also indicated the most cited political activities that the participants felt highly confident in were “providing written reports, consultation, or research to a public official on a health issue” and “analyzing health policies and/or make recommendations about them to a public.” However, the most cited political activity that nurses felt highly confident in performing was voting. This can be explained by the fact that because of the head nurses’ positions, they might be more exposed to such activities more than nurses, so they gained experience about it, which raised their level of confidence.
This study results showed that the level of head nurses’ involvement in health policy development increased when their confidence in their ability to perform political activities as well as their confidence of the impact of the political activities on health outcome increased. Such results are congruent with the findings of Gil de Zúñiga et al. (2017) and the results of O’Rourke et al. (2017). This positive correlation between self-efficacy and level of involvement emphasize the importance of raising the head nurses’ level of self-efficacy by policymakers which in turn will increase their level of involvement. This could be done by vicarious experience, performance realization, verbal persuasion, and emotional willfulness (Salvador, 2010).
The limitations of the study are the convenience sampling method which limited the generalization of study findings. The use of self-reporting questionnaire also might create a reporting bias. Despite such limitations, the study has several implications. Policymakers should start working on the barriers that impede head nurses’ involvement in health policy development process. This can be done by increasing the level of knowledge and skills about health policy development among head nurses which will increase their confidence in their ability to perform political activities. The nursing education institutions should have a strong position in activating nursing profession role in health policy development through providing adequate knowledge about health policy development in nursing education; and through conducting workshops, conferences, and sessions that focus on addressing health policy development and implementation.
Conclusion
Health policies affect nurses and their practice. Overcoming the barriers to nurse leaders’ involvement in health policy activities and enhancing their knowledge and competence regarding health policies can help activating their role in health policy development. Head nurses need to be role models for nurses in terms of being involved in health policy development. They need to activate nurses’ role and encourage them to participate in health policy activities. This study highlights the situation of head nurses’ involvement in health policy development in Jordan and provides policy makers with baseline information. Policymakers need to fill the gaps and work on eliminating barriers that stand behind head nurses’ involvement in health policy development.
Footnotes
Declaration of Conflicting Interests
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support for the research and/or authorship of this article