
Abstract
Nurse practitioner (NP) advocacy efforts often focus on attaining full practice authority. While the effects of full practice authority in primary care are well described, implications for hospital-based NPs are less clear and may differ because of hospitals’ team-based care and administrative structure. This study examines associations between state scope-of-practice (SSOP) and clinical roles of hospital-based pediatric intensive care unit (PICU) NPs. We conducted a national survey to assess clinical roles of PICU NPs including daily patient care, procedural, and consultation responsibilities as well as hospital-level administrative oversight practices. We classified SSOP as full or limited (reduced or restricted SSOP) practice. We present descriptive statistics and evaluate differences in clinical roles and hospital-level administrative oversight based on SSOP. The final sample included 55 medical directors and 58 lead (senior or supervisory) NPs from 93 of the 140 (66.4%) PICUs with NPs. There were no significant differences in daily patient care, procedural, or consultation responsibilities based on SSOP (p > .05). However, NPs in full practice authority states were more likely to bill for care than those in limited practice states (66.7% vs. 31.8%, p = .003), while those in limited practice states were more likely to report to advanced practice managers (36.7% vs. 13%, p = .03). For PICU NPs, SSOP was not associated with variation in clinical responsibilities; conversely, there were differences in billing and reporting practices. Future work is needed to understand implications of variation in hospital-level administrative oversight.
Nurse practitioner (NP) education and standardized national certification ensure nurses are prepared to practice in Advanced Practice Registered Nurses (APRN) roles and deliver health care as independent providers (APRN Consensus Work Group & National Council of State Boards of Nursing APRN Advisory Committee, 2008). However, state scope-of-practice (SSOP) regulations frequently restrict NPs’ full practice authority, thus limiting NPs’ ability to practice to the full extent of their education and training (Bosse et al., 2017). Currently, 23 states and the District of Columbia allow NPs full practice authority, while the remaining states require NPs to have supervisory or collaborative relationships with physicians to deliver care or prescribe medications (American Association of Nurse Practitioners [AANP], 2021).
Over the past decade, APRN advocacy efforts focused on changing SSOP laws governing APRN practice (AANP, 2019a; National Council of State Boards of Nursing, 2021). Full practice authority is championed by a diverse group of stakeholders, institutions, and governmental organization and allows APRNs to “to evaluate patients, diagnose, order and interpret diagnostic tests, initiate and manage treatments—including the ability to prescribe medications—under the exclusive licensure authority of the state board of nursing” (AANP, 2019a; Dillon & Gray, 2017). Attainment of full practice authority is associated with increased access to care without reductions in quality of care or increased costs (Buerhaus, 2018; Geller & Swan, 2020; Xue et al., 2016; Yang et al., 2020).
Notably though, research on the effects of full practice authority has primarily focused on primary and ambulatory care settings. NPs are increasingly working in inpatient settings with one in eight of all NPs working on inpatient hospital units (AANP, 2019b). However, there have been no studies specifically examining the effect of SSOP regulations on the roles of NPs in acute care settings. There is good reason to believe that the impacts of full practice authority may be different in hospital-based settings as inpatient care is more likely to occur within interdisciplinary care teams, to have different administrative structure including institution-specific requirements for NP credentialing and privileging, and to have more complex billing systems.
Since the APRN Consensus Model delineation of the acute care pediatric NP role in 2008, the availability of educational opportunities increased with nearly 100 focused, pediatric acute care graduate nursing education programs across the country (APRN Consensus Work Group & National Council of State Boards of Nursing APRN Advisory Committee, 2008; Gigli et al., 2020). Nearly a quarter of the pediatric NP workforce works in inpatient settings (Freed et al., 2014). As the presence of NPs in pediatric hospital-based care increased, their roles in health care delivery and their contributions to patient outcomes remain largely unexplored (Freed et al., 2011). Regulations, including SSOP, determine the extent to which NPs can practice independently and may influence how NPs are practicing in hospital-based settings. The absence of data on hospital-based practice hinders policymakers from understanding how SSOP regulations may affect acute care NPs and influence clinical outcomes and patients’ access to care. We attempt to address this gap in the literature. The purpose of this study is to examine how the role of NPs working in pediatric intensive care units (PICUs) varies based on SSOP regulations.
Methods
Study Design
We conducted a national, cross-sectional descriptive survey of PICU medical directors and lead (most senior NP or NP serving in a supervisory role among a group of PICU NPs) PICU NPs to report on the PICU workforce and roles of PICU NPs (Gigli et al., 2018b). Survey development has been previously described, but aspects of the survey that examined the influence of SSOP regulations on PICU NP practice are the focus of this article (Gigli et al., 2018b).
Sampling/Subjects
We directly contacted institutions that reported a PICU in the 2015 American Hospital Association Annual Survey to confirm the continued operation of a PICU (Gigli et al., 2018b). We sent surveys to a medical director at each operational PICU (n = 326). We placed telephone calls to each PICU to determine whether a PICU NP was employed and, if an NP was employed, we sent an additional survey to the lead PICU NP (n = 140). We excluded responses from this analysis if the institutions did not employ a PICU NP.
Procedures
We contacted eligible participants via postal mail between October 2016 and January 2017, up to three mailings were sent to each participant (Gigli et al., 2018b). Participants returned surveys electronically or by postal-mail. The final sample included 113 respondents from 93 of the 140 PICUs that employ NPs (66.4%). Data were collected and maintained on a secure, web-based platform, Research Electronic Data Capture hosted at Vanderbilt University (Harris et al., 2009). Participants recorded their own responses electronically or mailed survey responses were double-entered by a study team member into the Research Electronic Data Capture system. Returning a survey indicated participant consent. The Vanderbilt University Medical Center’s Institutional Review Board approved this study before recruitment and distribution of any study materials.
Instrument Items Related to the PICU NP Role
As part of the measurement instrument, we asked subjects about expectations for PICU NP participation in roles related to patient care, education, and quality improvement. We specifically assessed 19 PICU NP roles including those related to providing patient care in the PICU, procedural expectations, and consultant roles outside of the PICU. Survey questions asked if these roles were expected of all, some, or none of the PICU NPs. The responses were dichotomized into roles expected of PICU NPs (if the respondent indicated the role was performed by all or some of the PICU NPs) and roles not expected of PICU NPs (if no PICU NP was expected to perform the role). Three additional questions asked about presence or absence of specific aspects of hospitals’ administrative oversight on PICU NPs.
Measure of State SSOP
We utilized the AANP (2017) state practice environment classifications from the time of the survey administration. This classification accounts for restrictions placed on NPs related to evaluation, diagnosis, ordering, and prescribing. For the purposes of this analysis, we dichotomized the three state practice environment classifications: full, reduced, or restricted practice, into states with full practice authority compared with those with any limitations in practice, as full practice authority is the gold standard for APRN regulatory advocacy and is more meaningful than incremental changes achieved in moving from reduced to restricted practice (Spetz et al., 2019).
Data Analysis
We conducted all analyses using StataMP version 16 (Stata Corp, College Station, Texas). We generated frequency distributions of item responses for the sample and used cross-tabulations to examine differences by SSOP (full SSOP and limited SSOP). We use bivariate associations to assess differences using Chi square tests. All tests for statistical significance were two-tailed and evaluated at a significance level of α < .05.
Results
There were 113 respondents from a PICU that employed NPs (Table 1). A slight majority, 51%, of respondents were NPs and 49% were medical directors. Respondents had an average of 14 years of board certification and a 12-year tenure in their current role. Respondents were not significantly different between states with full SSOP and limited SSOP. The hospitals represented by respondents were similar in the size of the PICU and teaching status between the different SSOP environments.
Characteristics of Survey Respondents and the Hospitals That Employ Pediatric Intensive Care Unit Nurse Practitioners in the United States.
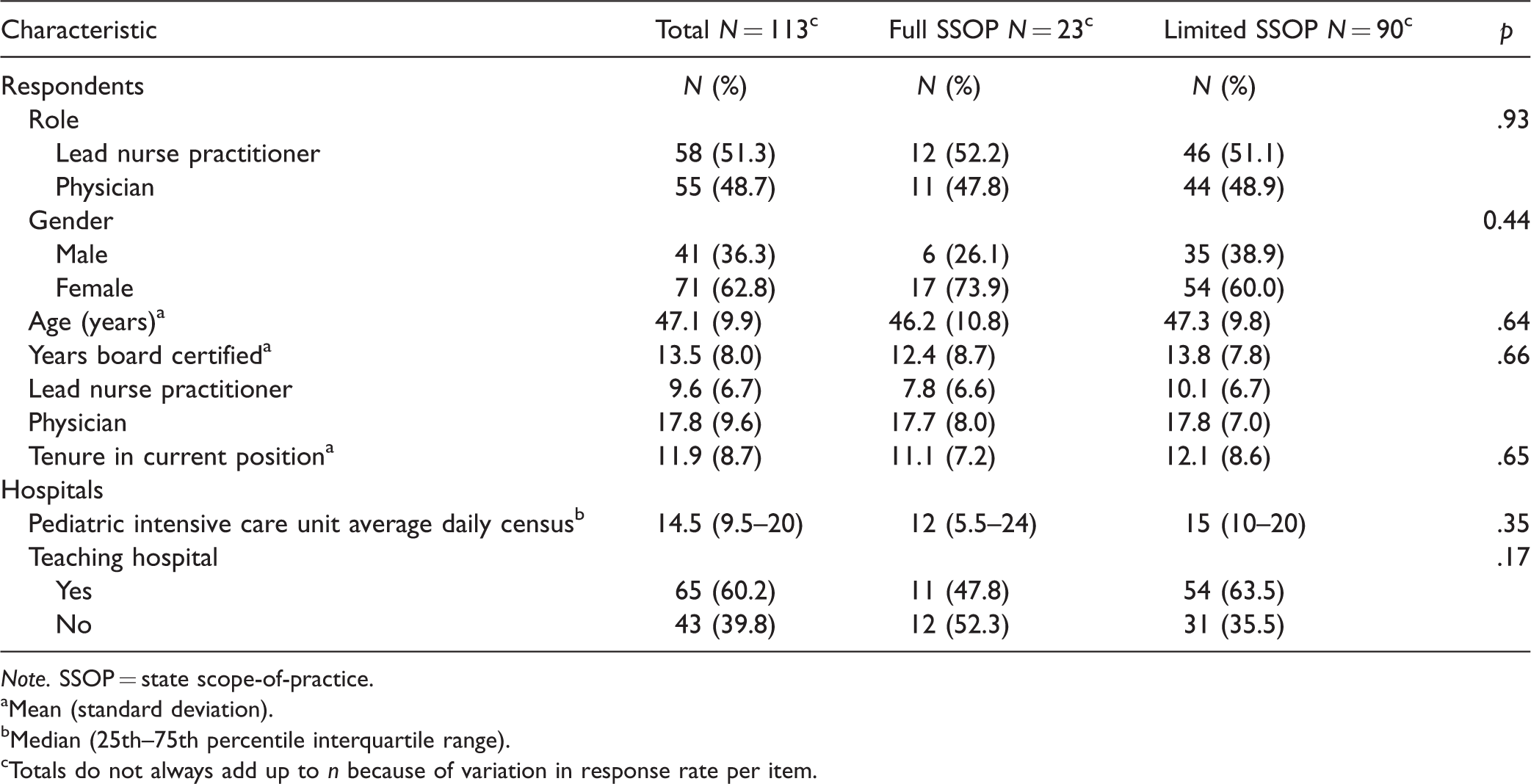
Note. SSOP = state scope-of-practice.
aMean (standard deviation).
bMedian (25th–75th percentile interquartile range).
cTotals do not always add up to n because of variation in response rate per item.
All respondents reported PICU NPs are expected to participate in daily patient care management. Most PICU NPs are expected to be involved in supervising training physicians, residents, and fellows (74.5%) and to be involved in educating training physicians (76.6%) and NP students (92.0%). Majorities also reported PICU NPs have procedural responsibilities for routine PICU procedures. PICU NPs’ clinical care responsibilities (Table 2), procedural expectations (Table 3), or consultant roles outside of the PICU (Table 4) were consistent across all SSOP environments.
Daily Responsibilities Expected of PICU NPs by SSOP Environment in the United States.
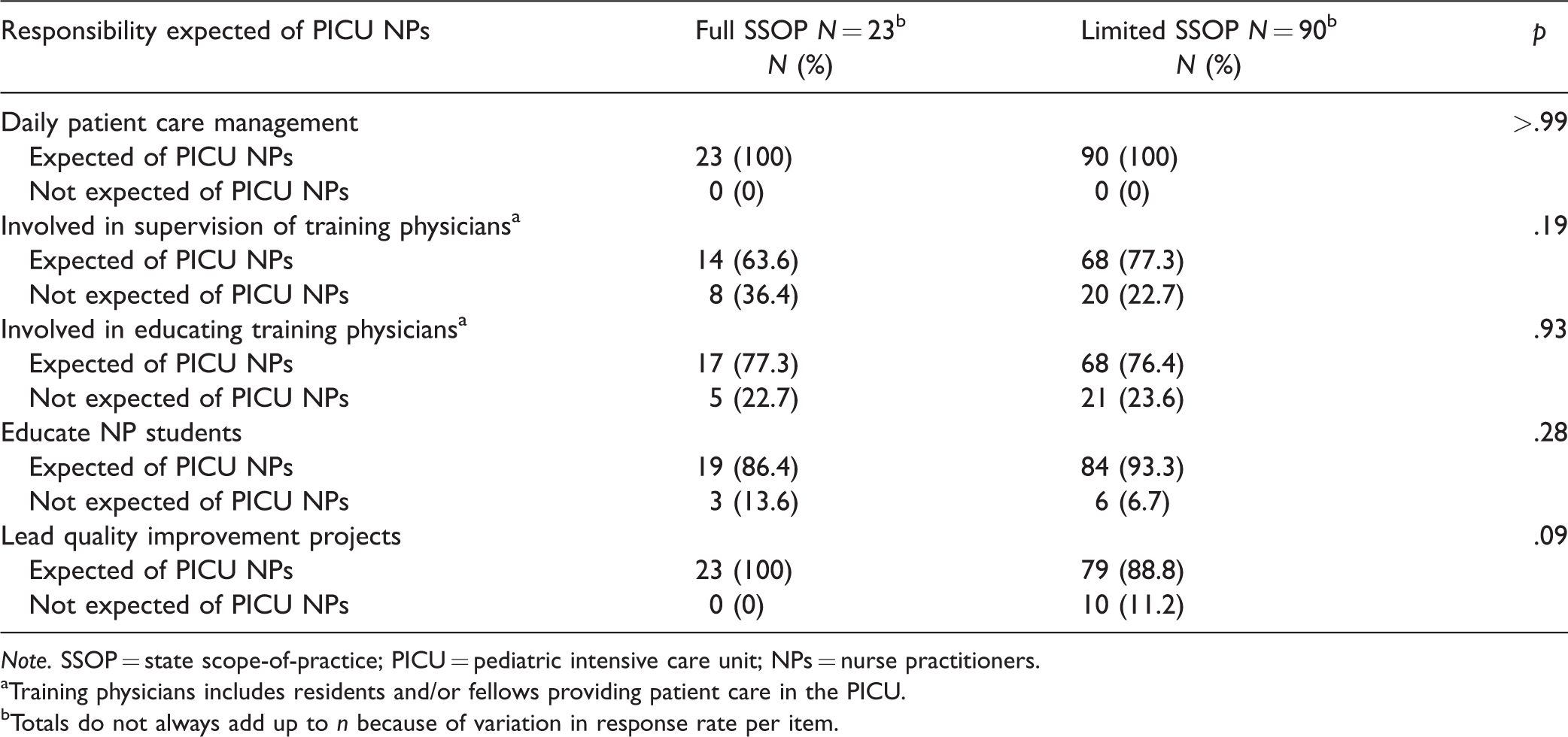
Note. SSOP = state scope-of-practice; PICU = pediatric intensive care unit; NPs = nurse practitioners.
aTraining physicians includes residents and/or fellows providing patient care in the PICU.
bTotals do not always add up to n because of variation in response rate per item.
Procedural Responsibilities Expected of PICU NPs by SSOP Environment in the United States.
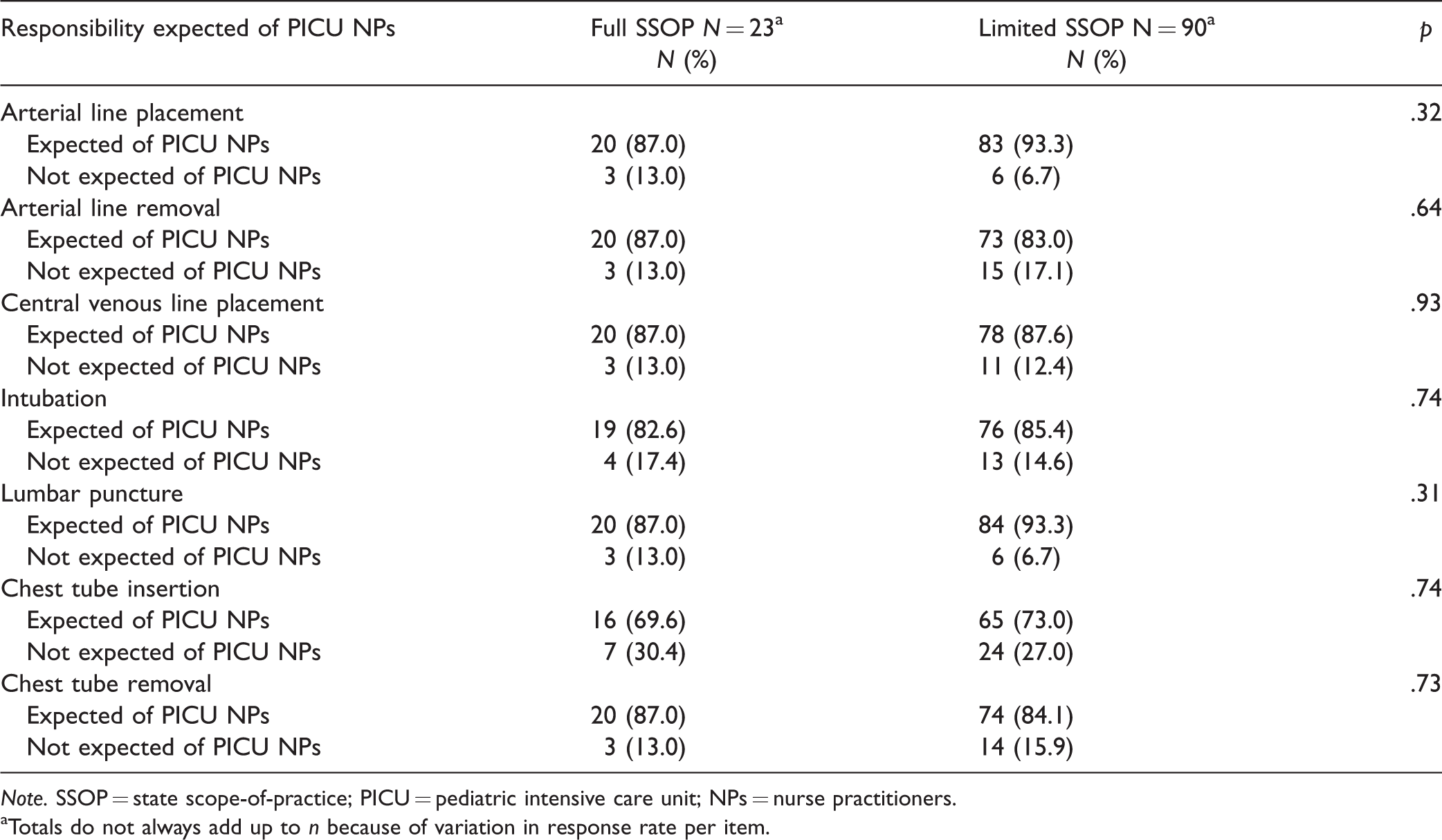
Note. SSOP = state scope-of-practice; PICU = pediatric intensive care unit; NPs = nurse practitioners.
aTotals do not always add up to n because of variation in response rate per item.
Consultation Responsibilities Expected of PICU NPs by SSOP Environment in the United States.
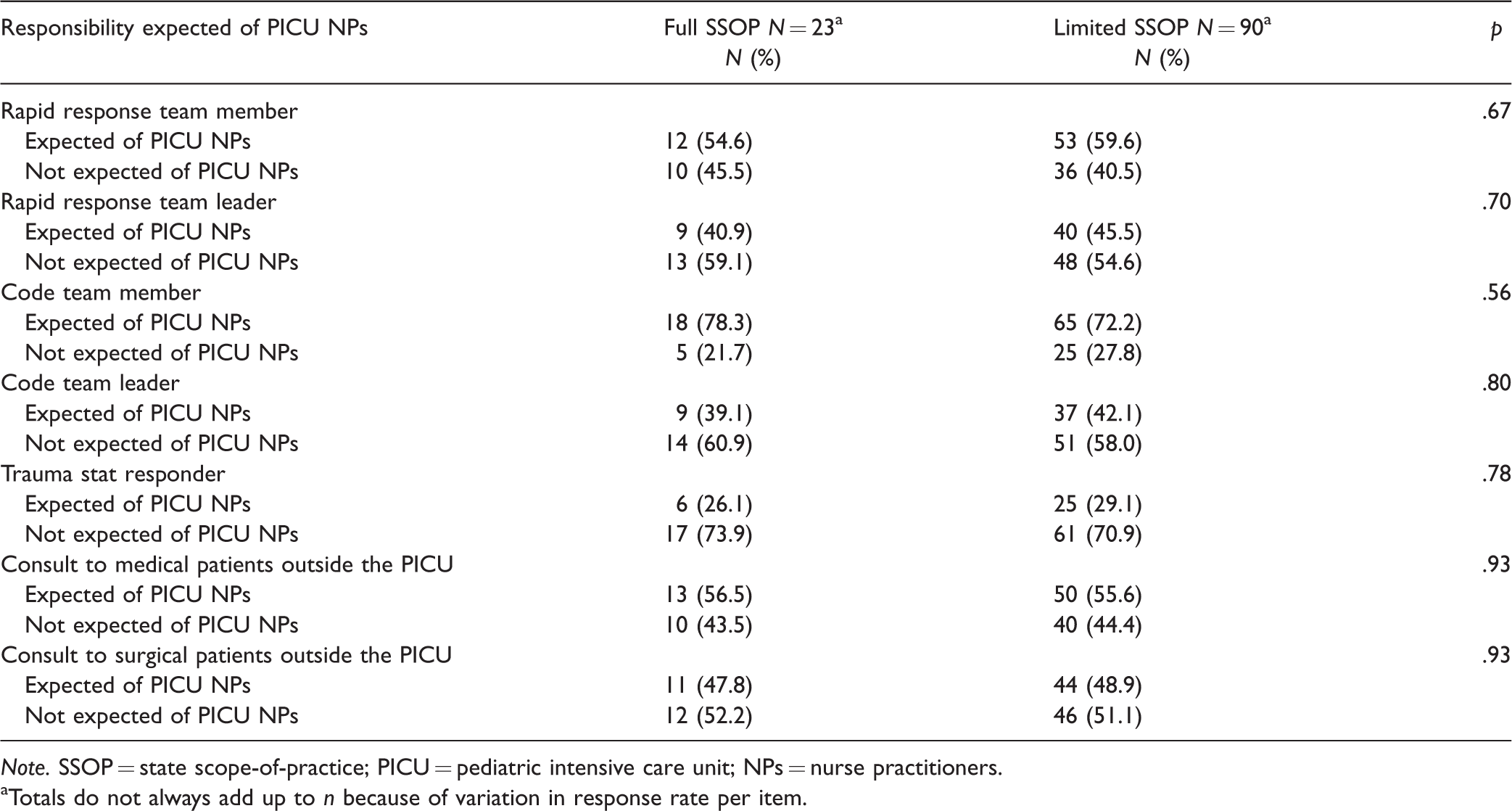
Note. SSOP = state scope-of-practice; PICU = pediatric intensive care unit; NPs = nurse practitioners.
aTotals do not always add up to n because of variation in response rate per item.
Expectations of PICU NPs roles within the hospital, but outside the PICU, as a consultant demonstrated the most variability (Table 4). Approximately a quarter of PICU NPs respond to trauma stat situations while nearly three-fourths are considered members of the code team. Despite variations in PICU NPs’ consultation role expectations, there were no significant differences in roles based on SSOP (p > .05).
There were significant differences in hospital’s administrative oversight of PICU NPs based on SSOP (Table 5). Notably, PICU NPs in states with full SSOP reported that they were more likely to bill for their care than those with limited SSOP (66.7% vs. 31.8%, p = .003). In addition, PICU NPs in states with limited SSOP were more likely to report to an advanced practice manager (36.7% vs. 13.0%, p = .03), but a majority of all PICU NPs in all practice environments still reporting to the medical director (74.2% vs. 82.6%, p = .40).
Administrative Oversight of Pediatric Intensive Care Unit NPs by SSOP Environment in the United States.
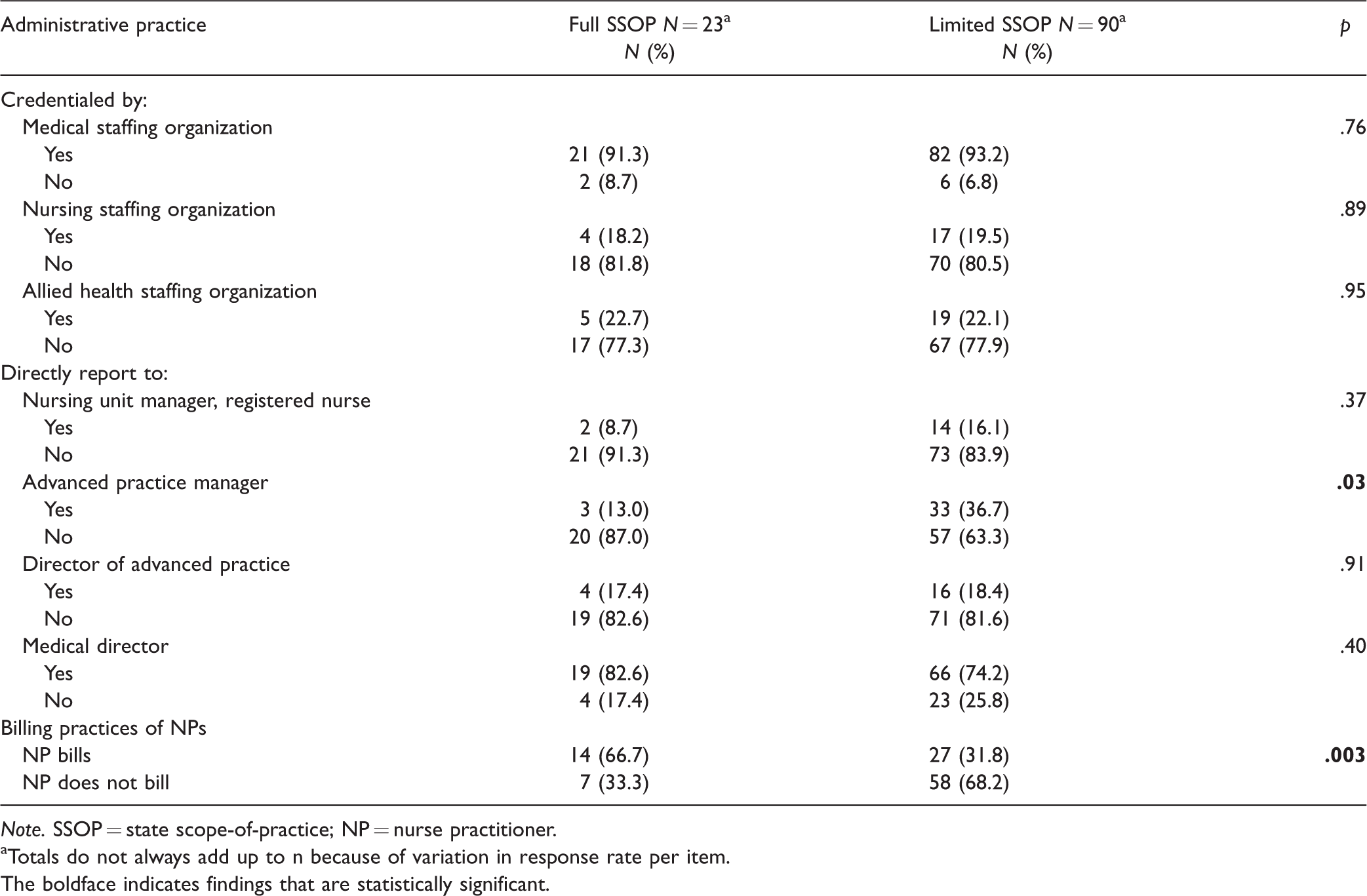
Note. SSOP = state scope-of-practice; NP = nurse practitioner.
aTotals do not always add up to n because of variation in response rate per item.
The boldface indicates findings that are statistically significant.
Discussion
In a novel examination of the relationship between SSOP and hospital-based NP roles, we found that SSOP resulted in limited variation in PICU NP clinical roles. However, we found that PICU NPs in full practice states were more likely to bill for care they provided than those in limited SSOP states. In addition, PICU NPs in states with limited SSOP were more likely to report to an advanced practice manager. This means that SSOP regulations had administrative and financial implications for NPs but little clinical practice significance, providing insight to the implications SSOP regulations on hospital-based NP practice.
The lack of an association between SSOP and NPs’ clinical roles could be explained by several factors. PICUs rely extensively on team-based care which integrates NPs as members of the interprofessional teams (Gigli et al., 2018a). As teams collaboratively provide care to a group of patients, the census of a PICU, local culture, and team configurations can exert greater influence on the NP role than the regulatory environment (Poghosyan, 2018). SSOP regulations determine the degree to which an NP requires physician supervision. However, in hospital-based settings with team-based care, like the PICU, the team always includes physicians (Gigli et al., 2018a). The differences in the degree of physician supervision may be less burdensome to practice and role actualization. Therefore, hypothetical “independence” may be far less important when practice is inherently collaborative, limiting the significance of SSOP regulations on the scope of a PICU NPs work.
In addition, institutions that employ PICU NPs often place additional regulations on practice beyond those required by SSOP regulations through the process of credentialing and privileging (Gigli et al., 2018c). Some research suggests within-state variation in practice regulations may be more significant than interstate regulations for hospital-based NPs (Pittman et al., 2020). These differences could be accounted for with the institutional variation in hospital-based NP credentialing and privileging. Ultimately, institutional practices may result in the perception of more independence in practice, with less obtrusive oversight in team-based care in states with more restrictive SSOP regulations, or more restrictive practice, with burdensome institutional regulations in full practice authority states. This might muddle the effect of SSOP regulations for PICU NPs. Untangling the implications of team-based care and credentialing and privileging on the roles of hospital-based NPs merit future examination.
The finding that NPs working in full SSOP states bill at higher rates than those in limited SSOP states is consistent with research on NPs in primary care practices (WestStat, 2015). In critical care, NPs are eligible to become credentialed to bill by payors and bill under their own national provider identification (Centers for Medicare and Medicaid Services [CMS], 2017). They may “direct bill” for critical care time (minutes) spent in management, evaluation, and delivery of critical care (CMS, 2017). However, the billing NP must be employed, constituting at least a portion of their NP salary, by the same practice plan as their critical care attending physician colleague (CMS, 2017). This can be a barrier to billing as many hospital-based NPs are employed by hospitals/health systems and not physician practices (CMS, 2017). In addition, the PICU NP cannot bill for time spent concurrently providing care with the physician (e.g., only one provider—the physician or NP, can bill for time spent actively managing a patient during a postarrest period even if both providers are involved in caring for the patient). As a result of unequal reimbursement, current regulations require NP reimbursement at 85% of the physician rate, for hospitals it is more feasible for a physician to bill for shared care delivery time at a higher reimbursement rate than an NP would receive for the same care time (Medicare Payment Advisory Commission [MEDPAC], 2019).
When PICU NPs do not bill, physicians direct bill for all PICU care and the cost of PICU NP care is incorporated into the global cost of hospital care. This practice effectively renders NP care “invisible” in billing data (Poghosyan, 2018). The ability of NPs to bill is important for provider accountability and role actualization. Studies that utilized NP billing data were foundational to evaluating NPs’ contributions to patient care, quality and cost in primary care, and without the availability of this type of data in PICU care, similar studies to assess care delivery are not possible (Buerhaus, 2018). Specifically, billing studies can validate the self-reported similarities in practice across SSOP environments found in this study and, more importantly, evaluate patient outcomes in different SSOP to address if variations in regulations contribute to differential quality or patient outcomes. Furthermore, among NPs in primary care barriers to billing in limited SSOP states are associated perceptions of limitations on clinical practice opportunities (Park et al., 2018; Yee et al., 2013). It is unclear, however, if PICU NPs have the same perceptions of billing, as a practice limitation, given the interdisciplinary nature of their practice and lack of practice variation across SSOP environments.
When PICU NPs bill, there are potential implications for the cost of care (WestStat, 2015). However, the effect of shifting critical care billing responsibilities from only physicians to joint physician and NPs billing is uncertain. Under current reimbursement models, if a PICU NP bills for care that would have otherwise been billed for by a physician, it is possible the cost of hospital care may decrease, as the cost of similar care from an NP is lower (MEDPAC, 2019). This could result in potential lost revenue for organizations and providers, potentially threatening hospitals’ financial viability. Conversely, if PICU NPs being billed for care they were providing all along, care previously “invisible” in the global hospital cost, hospital costs and reimbursement may actually increase. As policymakers consider regulatory changes to SSOP and NP reimbursement rates, the use of PICU NP billing data from full practice states, where PICU NPs are more likely to bill, can inform baseline cost evaluations and forecast how policy changes may affect hospital costs and revenue (Exec. Order No. 13890, 2019).
As the presence of NPs increase in hospital-based settings, organizations are increasingly developing centralized management structures for these providers to support the workforce and improve patient and organizational outcomes (Hunt, 2019; Love, 2018; Sullivan Cotter, 2018). As found in this study, NPs often report to a variety of personnel including physicians, other advanced practice providers, and registered nurses (Sullivan Cotter, 2018). While a large majority of PICU NPs report to a medical director, further research can elucidate the significance of different in reporting structures, particularly as there is variation in reporting practices for PICU NPs by SSOP. We are unaware of existing literature describing the advanced practice management workforce or relationship between organizational support for hospital-based NP practice and SSOP that can place these findings in context of the current composition and distribution of the advanced practice management workforce. Given limited variations in PICU NP roles by SSOP and more PICU NPs working limited SSOP states, reporting structure might influence employment decisions in ways that SSOP regulations do not for the PICU NP workforce and thus merits further attention.
Policy Recommendations
While PICU’s increasingly incorporate NPs on provider teams, federal, state, and institutional policies may hamper NP role actualization and contributions to care delivery (Gigli et al., 2018c). Federal policy sets standards for NP reimbursement (MEDPAC, 2019). Efforts to modernize billing regulations, allowing equitable reimbursement, are necessary to increases the feasibility and practicality of PICU NP billing. Furthermore, policy changes bolster NPs’ accountability for practice and support the ongoing evaluation of the quality of NP care. While SSOP did not result in different clinical expectations among PICU NPs, significant evidence evaluating NP practice demonstrates the benefits of full SSOP (Institute of Medicine, 2010). As a result, state-by-state efforts to remove practice barrier and implement the APRN Consensus Model should continue (National Council of State Boards of Nursing, 2021). Most importantly, this study shows the need for scrutiny of institutional policies. Given the similarities in practice across SSOP, the question of organizational constraints on PICU NP practice must be considered as a contributing factor. Institutional policies, including credentialing and privileging of NPs, that support autonomy and independence can improve patient and organizational outcomes—including teamwork which is essential for care in the interdisciplinary PICU environment (Park et al., 2016; Poghosyan & Liu, 2016).
Limitations
This study has several limitations. First, there were a small number of respondents from full SSOP. However, full SSOP states tend to be larger, rural states with fewer PICUs than states with limited SSOP which may influence the number of respondents based on SSOP (Gigli et al., 2020). In addition, PICU NPs are a small population of all hospital-based NPs, and thus the results may not generalize to NPs working in hospital-based roles outside the PICU. The survey only asked about major clinical roles of the PICU NP, not specific management responsibilities for patient care; as a result, we cannot delineate aspects of care PICU NP might perform independently. Furthermore, the survey examined billing practices with a single survey item, “Do PICU NPs bill for services or procedures.” Separate survey items to examine billing for services and procedures would provide greater insight into current practices inform the feasibility of examining PICU NP roles in care delivery using administrative data. Despite these limitations, the study contributes to knowledge of how the role of NPs working in PICUs varies based on SSOP regulations.
Conclusions
In the United States, pediatric hospital-based care delivery is changing in response to patients with greater acuity and chronicity of illness, an increasingly interdisciplinary workforce, and health care payment reforms that allow for participation in value-based payments (Berry et al., 2013; Watson & Hartman, 2014; Weled et al., 2015). PICU NPs assume multiple roles: direct care providers, team members, educators, and consultants, among others. This study found SSOP regulations did not change the role expectations of PICU NPs. Further qualitative work is needed to understand whether role actualization or interdisciplinary collaboration is different based on SSOP. Leveraging PICU NP billing data from states with full SSOP will provide insight cost and quality of care provided by these clinicians. Ultimately, interventions should be designed to optimize the role responsibilities of PICU NPs to achieve organizational priorities and improve pediatric health outcomes regardless of state practice environment.
Footnotes
Ethical Approval
The Vanderbilt University Medical Center’s Institutional Review Board approved this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from National Institutes of Health (T32HL007820).