
Abstract
Every state includes nurses as mandated reporters of suspected child maltreatment, and each state has its own law and policy regarding what is reportable and reporting requirements. These differences mean that generic training on child abuse and reporting needs to be augmented by practical state-specific information. In nearly every study of nurses, participants report having inadequate child abuse training. This paper presents an analysis of the information states post on their websites to educate nurses to appropriately identify and report suspected child abuse or neglect. Specifically, this study aims to answer the following questions: (1) how do mandated reporting laws that apply to nurses vary by state, (2) what information do states provide on their child protection and Board of Nursing websites about child maltreatment and mandatory reporting, and (3) what training resources do states make available on their websites to educate nurse mandatory reporters to ably fulfill their obligation? Data on state-by-state practices regarding mandated reporting of child abuse were gathered from the Rape, Abuse, & Incest National Network (RAINN) database, review of state statutes, Child Welfare Information Gateway, Board of Nursing sites, and the Nursing Licensure Compact (NLC) website. This analysis found that states provide little guidance or education about their child maltreatment laws, and few have resources targeted for nurses. Given rising membership in the NLC it is critical for nurses to have education about state specific mandated reporting requirements. States should consider adding mandatory reporting training as a requirement for licensure and for continuing education.
Nurses throughout the United States, across all their areas of practice, are mandated reporters for child abuse and neglect under their state's child welfare statute (U.S. Children's Bureau, 2019). Across the lifespan and in practice settings ranging from community-based and school arenas to outpatient and inpatient care centers nurses are legally mandated and ethically obliged to report suspicions of child abuse or neglect in the course of their professional work. In practice, this involves filing a report with their state agency for child protective services (CPS). The mandate applies to nurses ranging from licensed vocational or practical nurses (LVNs/LPNs), to registered nurses, and includes advanced practice nurses in all clinical roles and across specialties. Because each state has its own law, state variations are present in the definition of reportable child abuse and neglect, the contexts in which reports are mandatory, and penalties for failing to report a suspected case (Levi & Portwood, 2011). These differences mean that generic education about child maltreatment and mandatory reporting needs to be augmented by state-specific information regarding state reporting definitions and procedures (Baker et al., 2021). For nurses, who may be educated and first licensed in one state, a move to another state will require actions to become familiar with their new state's law. This is especially important in light of the growing number of states participating in the NLC, an agreement by one state to recognize a license granted in another member state (National Council of State Boards of Nursing, 2021). States share responsibility with nursing education programs and clinical employers for communicating to nurses the requirements of their laws. If nurses are knowledgeable about the evidentiary standards, reporting, and the investigative processes, appropriate cases are brought to the attention of authorities, potentially preventing harm to children through a failure to report or an unnecessary report (Merrick & Latzman, 2014; Raz, 2020). Ho et al. (2017) found that among reports filed by medical personnel, which includes nurses, only 22% of cases investigated were likely to be substantiated, indicating that under the state's criteria sufficient evidence of child abuse or neglect was found. From this, they emphasize the importance of state-specific understanding of what constitutes child abuse and the needed evidence. This paper, focused on nurses, presents a nation-wide analysis of the accessibility of states’ information about mandatory reporting, their definitions and their processes through an examination of state nursing board and child protection websites.
The literature about mandatory reporting of child abuse includes consideration of nurses and their roles. It spans (a) overviews that define child abuse and neglect and basic information for nurses about mandatory reporting (Adams, 2005; Caneira & Myrick, 2015), (b) findings from surveys that report nurses’ understandings of child abuse and mandatory reporting and their confidence in identifying and reporting suspected child maltreatment (Davidov et al., 2012; Eisbach & Driessnack, 2010; Herendeen et al., 2014; Kuruppu et al., 2020), and (c) reports from surveys of the estimated impact of training for identification and reporting of child abuse or evaluation of a program that provided nurses with such education or training (Dudas et al., 2019; Flaherty et al., 2000; Herendeen et al., 2014; Kuruppu et al., 2020). Barely examined are the methods state governments use and the quality of the information they provide to nurses about state definitions, policy, and procedures for mandatory reporting.
State Child Protection Legislation
State laws for mandatory reporting of child abuse and neglect have roots in health care settings. In a widely influential 1962 publication, The Battered Child Syndrome (Kempe et al., 1962), Kempe and colleagues argue that physicians have a duty to recognize injuries caused by abuse and act to prevent further harm. Many states then independently legislated mandatory child abuse reporting; however, the federal 1974 Child Abuse Prevention and Treatment Act (CAPTA) caused every state to enact a reporting statute as a condition for receipt of federal financial support for child welfare (Brown & Gallagher, 2014; U.S. Children's Bureau, 2019). CAPTA defines child abuse and neglect as “any recent act or failure to act on the part of a parent or caregiver that results in death, serious physical or emotional harm, sexual abuse, or exploitations, or an act or failure to act that presents an imminent risk of serious harm.” (P.L. 111–320, 42 U.S.C. § 5101, Note (§3)).
States use wording similar to, but not identical to the federal statement for definitions of reportable child maltreatment, with many state statutes articulating categories of abuse to include physical abuse, neglect, sexual abuse, and emotional abuse (Levi & Portwood, 2011). All state statutes cover situations where the reporter has observed evidence of harm or injury and has reasonable cause to suspect (or a variation of this phrase) that it arose from child abuse or neglect (Levi & Portwood, 2011). Nine states also invoke the mandate to make a child maltreatment report based upon a judgment of probable future harm, even if there is no current observation of injury, or the harm is not imminent (Mudrick & Smith, 2017). With this variation, studies of nurses’ understanding of mandatory reporting obligations have noted the need to understand the specific definitions and policies of their state (Davidov et al., 2012; Ho et al., 2017; Merrick & Latzman, 2014).
Nationally reports of child abuse or neglect are either “screened in” and receive an investigation or alternative response, or “screened out” if they do not meet the criteria of the state child protective agency (U.S. Department of Health & Human Services, 2021). Of the 4.3 million reports of suspicions of child maltreatment in 2019, 54.5% were screened in for investigation, and of those, 56.5% were later determined unsubstantiated (U.S. Department of Health & Human Services, 2021). Thus, a little more than 25% of all reports were ultimately substantiated. Child neglect constituted 74.9% of cases in 2019, with physical abuse 17.5%, sexual abuse 9.3%, and 6.8% other maltreatment. By age, children 0–2 were 28.1% of the maltreatment victims. Medical personnel, not broken down to distinguish physicians, nurses, or others, made 11% of the reports of suspected child maltreatment (U.S. Department of Health and Human Services, 2021).
The federal government does not regulate how states organize their child protection systems (CPS) or which persons must be mandatory reporters. Thirty-two states plus Washington, D.C. list specific professionals, including nurses, as legally mandated child abuse reporters, while 18 states use universal mandated reporting (Krase & DeLong-Hamilton, 2015). Universal mandated reporting laws require all adults to report a suspicion of child maltreatment. The intent of the universal reporting mandate is to increase the chances that a case of child abuse or neglect will be reported; however comparison of reports between states with and without a universal mandate found a small increase in the number of reports but no significant difference in the proportion of substantiated cases (Krase & DeLong-Hamilton, 2015). Federal child welfare law also does not require specific actions by states to ensure that mandatory reporters within the state are knowledgeable about the indicators of child abuse and neglect and the parameters of their obligations. Therefore, in addition to state by state variation in the formal definition of actionable child abuse or neglect, there is state-to-state variation in how mandatory reporters are prepared to meet their obligation. Some states offer resource guides for those mandated to report while other states make training modules available, with differences in the content, quality and accessibility of these resources across states (Baker et al., 2021; Mudrick & Smith, 2017).
Nurses’ Knowledge and Attitudes About Mandatory Reporting
A number of publications have examined the factors that affect mandatory reporting by nurses or by a sample of medical and health professionals that includes nurses (Adams, 2005; Caneira & Myrick, 2015; Davidov et al., 2012; Eisbach & Driessnack, 2010; Flaherty et al., 2000; Herendeen et al., 2014; Kuruppu et al., 2020; Merrick & Latzman, 2014). Based upon indications that child abuse is under-reported in medical settings these studies aimed to understand perceived barriers to mandatory reporting. The factors affecting reporting that were identified include confidence in their knowledge of the definitions and indicators of child abuse or neglect; understanding when and how to report a case of suspected child abuse; concerns about the relationship with the child and family following a report; and satisfaction with consequences of reporting to CPS (Davidov et al., 2012; Eisbach & Driessnack, 2010; Herendeen et al., 2014; Kuruppu et al., 2020). The Child Abuse Reporting Experience Study (CARES) that surveyed pediatricians (Flaherty et al., 2006), developed an instrument with structured force-choice questions about respondents’ past experiences and a child vignette. The aim was to identify factors that influence recognizing and filing a child abuse report and factors associated with not reporting despite suspicions. A large survey of nurses’ perspectives, conducted by Herendeen et al. (2014), sent a modified version of the CARES survey instrument to pediatric nurse practitioners (643 respondents). The findings mirror what was found in the Flaherty et al. (2006) survey of physicians. Sixty-nine percent expressed confidence in identifying abuse; confidence in managing victims of maltreatment (58%); 41% reported a mix of positive and negative past experiences in reporting suspicions of abuse to CPS; and 14.3% worked with the family but did not make a report despite suspicions (Herendeen et al., 2014).
The NLC, which currently has 34 member states, provides licensure reciprocity. It is important for nurses to be aware of the subtle differences in the mandated reporting laws to ensure their appropriate and legal response to cases of suspected child maltreatment (National Council of State Boards of Nursing, 2021). For example, a nurse moving from Montana to Utah who is seeking reciprocity without new training cannot assume that the mandated reporting requirements are the same. This could pose legal ramifications for the nurse; Utah has a universal reporting mandate which requires the nurse to report suspected child abuse in any context, not just for situations encountered in a professional capacity as is the case in Montana (Montana Code Annotated 41-3-2; Utah Code 62A-4a §403). Moreover, in Montana no written report is required, but in Utah a written report is required within 48 h of an initial oral report. The consequences for failure to report also are different, as Montana only issues criminal charges, whereas Utah issues both criminal and financial penalties. These nuanced differences, even among states who participate in the NLC, provide additional support for the necessity of training for nurses about state specific mandated reporting requirements.
Training and Education
Despite the medical setting origins of the duty to respond to suspicions of child maltreatment, nearly every study of nurses finds these providers report having inadequate training on the nuances of child abuse and mandatory reporting (Davidov et al., 2012; Eisbach & Driessnack, 2010; Flaherty et al., 2000; Herendeen et al., 2014). Nurses expressed the need for guidance where there was violence in the home not directed at the child, or where the suspected abuse was not physical (Davidov et al., 2012; Eisbach & Driessnack, 2010). The authors of these studies suggest differences also may reflect inadequate knowledge about how the child protection system operates, something more education could address. A survey that included physicians (n = 76) and nurse practitioners (n = 8) found that those with some formal education on child abuse in the past 5 years were 10 times more likely to understand mandatory reporting and file a report for all suspected abuse (Flaherty et al., 2000). Similarly, the Herendeen et al. (2014) study with pediatric nurse practitioners found those with recent education about child abuse and mandated reporting were more confident in their ability to properly identify and report cases of child maltreatment (Herendeen et al., 2014). However, 21% of the respondents indicated they did not believe they had adequate training. The study found that the number of hours of child abuse training reported in the past 5 years varied widely, from 0 to 550 h, with a mean of 13 h (SD = 9; Herendeen et al., 2014). However, there is no research that offers a nationwide summary of the hours of child abuse and mandatory reporter training through nursing education (generally, by specialty, or by certification) or through employers or state agencies.
Given that study findings with nurses indicate their interest and recognized need for more training, we investigate the actions of states to support nurses in their responsibility as mandated reporters. Specifically, this study aims to answer the following questions to create a national portrait: (1) how do mandated reporting laws that apply to nurses vary by state? (2) what information do states provide on their child protection and Board of Nursing websites about child maltreatment and mandatory reporting? (3) what training resources do states make available on their websites to educate nurse mandatory reporters to ably fulfill their obligation?
Methodology
This is a descriptive study based upon analysis of data extracted from state government websites. Initially, data on state-by-state practices regarding mandated reporting of child abuse were collected from the Rape, Abuse & Incest National Network (RAINN) database (RAINN, 2020). This database contains both a statistics portal and a state law portal. The state law portal serves as a hub for retrieving information about state policies such as those relating to sex crimes, consent, mandated reporting of child and elder abuse, and criminal statutes of limitation. For this research, summaries of each state's policy about mandated reporting of child abuse and neglect statutes were accessed through RAINN's State Law Report Generator. This application allowed us to gather information on three states at a time, detailing who is required to report (certain professions or universal mandate), what information is required to be in the report, when reporting is required and to whom to send the report, the timing and procedural requirements, as well as the consequences for not reporting. As a second step, data retrieved from the RAINN database was validated by reading the electronic version of each state's statute on their websites. This step also enabled us to gather further information, including the scope of the mandate on professionals. In addition, the Child Welfare Information Gateway website was used to identify state websites pertaining to their resources and trainings available for mandated reporters (Child Welfare Information Gateway, 2020). The Board of Nursing website for each state was analyzed to determine if specifics on training and other useful material surrounding mandated reporting were present. Finally, the NLC website was analyzed to determine which states participate in the licensure reciprocity compact. The IRB confirmed no review was required because this research did not involve any human subjects.
The information for 50 states plus Washington, DC that was extracted from these sources was entered into an Excel spreadsheet. The data in the Excel spreadsheet were then coded and imported into IBM SPSS Statistics (Version 27) to produce descriptive statistics using frequencies and crosstabulation tables. Required reporters were collapsed into two categories: universal reporters or a list of specific professionals. The mandated reporter resources for each state were coded into three categories: (1) generic information resources only (materials not targeted to any specific profession or audience), (2) generic information resources and training modules or links, or (3) generic information resources and training modules or links, with additional resources or trainings targeted to specific professionals. Fisher's Exact Test was used for calculating statistical significance for the crosstabulation due to cell sizes smaller than five (IBM Corporation, 2020).
Results
Table 1 summarizes the findings from analysis of the information states publish on their websites about mandated reporting in general, and with a focus on nurses. The information is summarized in three categories: (1) whether mandated reporters are limited to a list of professionals or whether all persons in a state are obligated as mandatory reporters, (2) whether the state offers on its website resources and training information as guidance for mandatory reporters and if that information is targeted to different audiences among mandatory reporters, and (3) whether the state Board of Nursing website contains information or links to support nurses’ mandatory reporting obligations.
Characteristics of State Mandated Reporting Requirements for Child Abuse or Neglect.
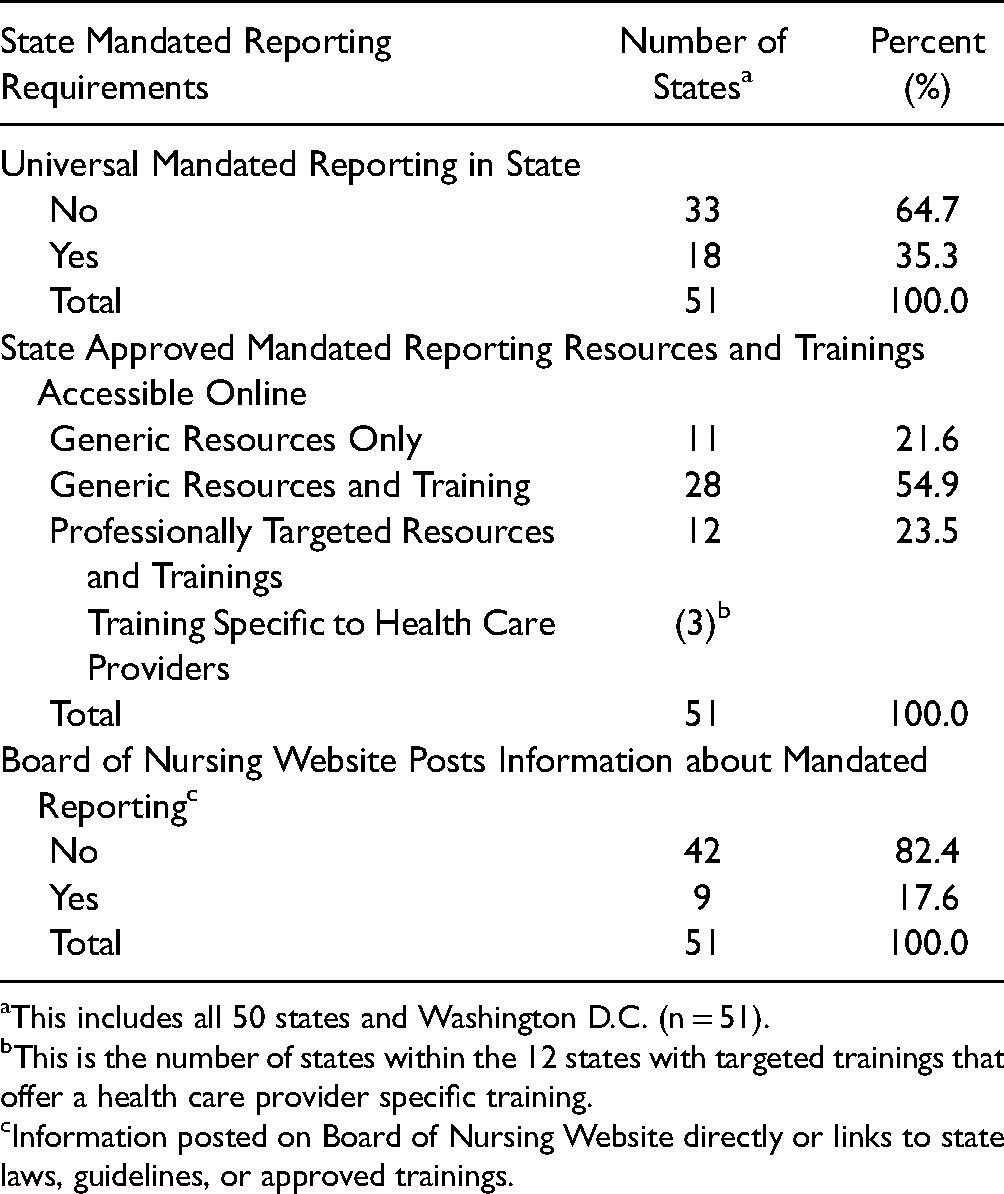
This includes all 50 states and Washington D.C. (n = 51).
This is the number of states within the 12 states with targeted trainings that offer a health care provider specific training.
Information posted on Board of Nursing Website directly or links to state laws, guidelines, or approved trainings.
Specific Versus Universal Mandatory Reporters
States either identify specific professions subject to the mandate or utilize a universal reporting mandate. A universal mandate means that everyone in the state is considered a mandated reporter of child abuse. Table 1 shows that 35% of states (18) extend the mandate to everyone who observes suspected child maltreatment. A universal mandate raises the question about whether every state resident needs to be trained to understand the state definition of child maltreatment and what it means to be a mandated reporter. Because all residents do not receive specific training to recognize child maltreatment as legally defined in their state, there is concern that a universal mandate produces more reports to be investigated, but not greater child safety (Ho et al., 2017; Krase & DeLong-Hamilton, 2015). By contrast, nearly 65% of states, including Washington, DC (n = 33) list specific professionals who are mandated to report suspected child maltreatment or face a penalty. Where states require specific professions to report their suspicions, nurses and other medical personnel are always included, although there is some variation across these states with regard to the other professions listed. Limitation of the mandate to an individual's observation in a professional capacity occurs in 20 states, whereas 31 states require nurses to report suspected child maltreatment in any context. For example, in New York State, a nursing professional's mandate to report suspected child maltreatment applies only where the nurse has seen the child in the course of professional activities (New York Social Service Law, 2021). A nurse is not mandated to report a behavior observed while shopping in a mall, although free to voluntarily make a report as is any community resident.
State Training and Resources for Mandatory Reporters
States support their mandates to report child maltreatment by offering information resources and training courses with the aim of ensuring that reporters are knowledgeable enough about child maltreatment to recognize it, and to inform them about the process of making a report. The information materials may be developed by the state, with the delivery of trainings completely state controlled; states may contract with private entities for materials and trainings on behalf of the state; or private entities may develop materials and offer trainings that have been state approved. The review of state child protection websites revealed that the extent and depth of content that states offer varies widely. Eleven states offered generic information about child maltreatment and reporting. This information is not tailored to the context of any specific profession. Generic information includes a spectrum of content, from simple restatement of the mandated reporting law and contact numbers to PowerPoints or manuals and FAQ documents. The majority of states, 55% (n = 28), have generic state approved training courses, offered without regard to the specific professional discipline or context. Twelve states (23.5%) target their mandatory reporter resources and have at least one training specific to a profession, with context-relevant information to support the professional's mandate. Profession specific trainings include those for school personnel, child caregivers, health care providers, law enforcement, and volunteers at organizations with mandated professionals. The majority of specially targeted trainings are for school teachers with only three of the twelve states, California, Delaware, and Pennsylvania, offering training specifically geared toward health care providers.
State Boards of Nursing Website Attention to Mandatory Reporting
Since State Boards of Nursing are responsible for licensing nurses, we reviewed the state board websites to see whether they addressed nurses as mandatory reporters. We looked to see if websites offered specific guidance to nurses about identifying and reporting child maltreatment and/or contained a link to the state's other information about mandatory reporting. Only nine (17.6%) State Board of Nursing websites contain any information about the licensed nurse's role and responsibility as a mandated reporter (Table 1). Of these, five provide only the legal code about mandated reporting of child abuse. The remaining four states provide links to resource guides or state approved mandatory reporting trainings.
We were curious to know whether the states in the NLC were engaging in any practices to help nurses transferring their licensure become aware of the mandated reporting laws in the new state. As Table 2 shows while 34 states are currently in the NLC, only 5.9% of them provide information about mandated reporting on their Board of Nursing website. However, of the 17 states that are not members of NLC, 41.2% provide information about mandatory reporting on the Board of Nursing Website. This difference is statistically significant (p = 0.004 using Fisher's Exact Test). This finding is somewhat unexpected, as it would be logical for the states involved in the NLC to be attentive to information needs associated with nurse legal obligations that are state-specific, whether on the nursing board website or the state child welfare website.
Mandated Reporting Resources on Board of Nursing Website by NLC Membership (%).
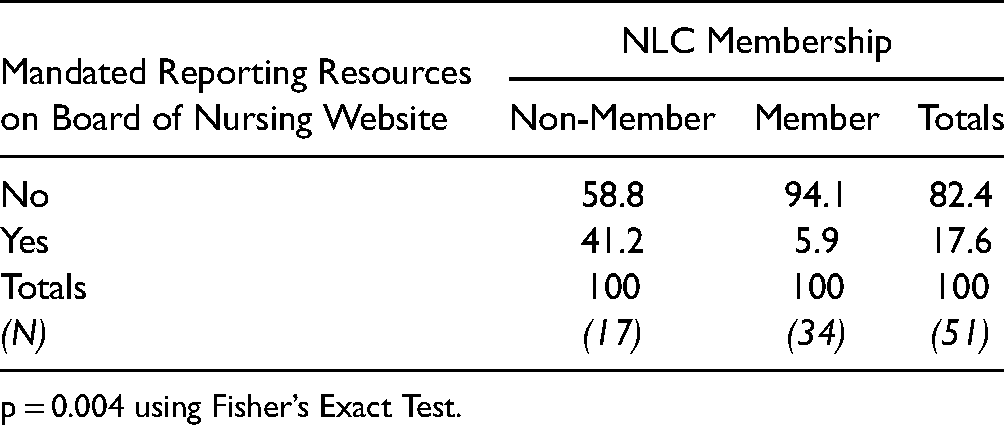
p = 0.004 using Fisher’s Exact Test.
Discussion
Noticeable differences exist in how states structure their child protection systems and rules for mandatory reporting because the federal government does not offer a single model that requires state compliance. The most significant difference among states is whether mandated reporting is a universal obligation to all residents or for a more limited list of persons who regularly work with children. However, nurses are mandated reporters no matter the state in which they practice. This makes the subtle differences between states’ mandatory reporting laws pertinent to them. Since nurses may receive their education in a different state than the one in which they practice, it is surprising that states apparently play little role in providing guidance and education about their unique mandated reporting laws. Moreover, given the growing number of member states providing license reciprocity through the NLC, attention to state-by-state differences is important.
This state-by-state analysis shows that states provide little direction to child maltreatment educational resources for nurses. Thus, it is unsurprising that in previous research a notable percentage of nurses reported they lacked confidence in their ability to properly identify and report child abuse and neglect (Herendeen et al., 2014). Few state-approved websites about child abuse and mandated reporting provide nurse-focused information. The three rare occurrences have a training for health care personnel, which includes generic medical contexts to educate doctors, nurses, and others in medical settings or practices. Whereas information and training resources targeted to nurses do exist, locating them may be difficult. Less than one fifth of states include information about mandated reporting on their Board of Nursing website and even fewer link nurses to educational resources. Moreover, the finding that only two member states in the NLC provide these resources on their Board of Nursing website has important practice implications. Since nurses who benefit from the NLC have their licenses already and thus have completed their formal education, adding mandated reporting education to the required nursing curriculum is not enough. Only two states, New York and Pennsylvania, require nurses to receive education on identifying and reporting child abuse for initial licensure (New York State Office of the Professions, 2020; Pennsylvania Department of State, 2021a); one additional state, Iowa, requires continued education on this topic every five years for license renewal (Iowa Board of Nursing, 2020). Nationally, nurses are not currently provided clearly accessible opportunities and resources to fulfill their legally proscribed roles as mandated reporters.
More could be done by states to support nurses in their role as mandated reporters. The Commonwealth of Pennsylvania shows it is possible to provide nurses and others with tools specific to their professional roles so they can confidently fulfill their reporting responsibility. Pennsylvania's Board of Nursing website is unique in that it contains an explicit link about mandatory reporting on the homepage (Pennsylvania Department of State, 2021b). At the top of the mandatory reporting page there is a link to a PDF addressing frequently asked questions about mandatory reporting that directly pertain to nurses. This page goes on to summarize the laws pertaining to reporting child abuse in the state of Pennsylvania and provides links to approved trainings. The state is also one of three that provide a training tailored to health care professionals. Pennsylvania does not merely list educational resources for nurses through the licensing board's website, but requires mandatory reporter training for initial licensure and as continued education for bi-yearly license renewal (Pennsylvania Department of State, 2021a). Pennsylvania's policies are fairly new; the original child abuse laws were enacted in 1975, however the policies outlined here as best practices were updated in 2013 and 2014. These changes were implemented due to a thorough review of current policies and issues by a joint state government commission (The Task Force on Child Protection, 2012). The timeline for these changes suggests there is a precedent for additional states to reflect upon the areas for attention in their child abuse and reporting laws and to make the appropriate amendments.
Study Limitations
While this study offers useful insights about the macro level support nurses receive regarding their legal mandate to report child abuse, it is limited in scope as only publicly facing state child abuse reporting and Board of Nursing websites were examined. It is possible that nurses, through a portal or log-in platform, have access to additional resources on these websites that we were not able to view. It also is possible that a child abuse training requirement embedded in curricula for nursing program state accreditation is present but not mentioned on the Nursing Board or mandatory reporting websites. Additionally, the study is limited in its ability to assess quality of the support and resources for nurses. This study does not examine educational materials or training about mandated reporting delivered in nursing education or practice settings. Nor did we analyze non-profit or professional organizations at the local, state, or national level that might be providing training or information resources. Together these factors limit our ability to make conclusions about the overall support or lack thereof for nurses regarding mandated reporting of child abuse. Instead, the scope of our conclusions is limited to states, themselves, and in tangent, the state-run licensing of nursing.
Conclusions and Policy Recommendations
This analysis of the mandatory reporting information that states provide on their websites for nurses has found that states offer little to no guidance regarding their laws, policies, and nurses’ obligations. States do very little to ensure that as mandatory reporters, nurses are adequately trained when to suspect or not suspect child maltreatment. States also offer little information to nurses about how CPS works, what happens after a report, what information may be shared with them, and what options may be available to the child and family as a result of a CPS report.
Policy Recommendations
These findings suggest a number of policy actions by states. First, states should require state-approved child abuse training for nurse licensing that could be delivered as a part of nursing education or through state offered modules. New York and Pennsylvania do this; California requires seven hours of child abuse training for Public Health Nurse certification (New York State Office of the Professions, 2020; Pennsylvania Department of State, 2021b; State of California Department of Consumer Affairs, n.d.). The requirement should extend to licenses transferred via the NLC. A second action could be to require periodic re-training. Two states have implemented this requirement, Pennsylvania and Iowa (Pennsylvania Department of State, 2021b). The specialized education nurses receive and their position in a variety of practice settings give them access to additional indicators of potential child maltreatment. It is logical then that they should be provided with a tailored mandatory reporter training, either specific to nurses or for health professionals as a whole. Such training could offer information specific to a state's evidentiary standard, especially where physical or emotional indicators of abuse or neglect are subtle.
Because state licensure boards are positioned to reach all nurses, they could assume responsibility in partnership with state CPS for provision of state specific education about their duty as mandated reporters. A minimum action would be to provide a link on the nursing licensing board website that connects to the state's website on mandatory reporting and child protection. A stronger response would use an approach similar to Pennsylvania's and provide information directly on the nursing board website.
Future Research
In practice, nurses work with children and families where there may be the presence of family violence, differing cultural approaches to parenting, or parental disability. Research to provide greater guidance for child abuse assessment in these situations would be helpful. For example, child abuse reports dropped during the spring 2020 COVID-19 shutdown, but child abuse related emergency department visits that ended in hospitalization were above the prior year (Swedo et al., 2020). With children learning from home, school nurses were forced to use different methods to detect or prevent child abuse (Haas, 2021). Nurses also must navigate identifying and reporting child abuse and neglect with respect for the intersecting identities of their patients and their patients’ families. While ongoing concern exists about under identification and reporting of child abuse, there also is concern that some families are unnecessarily subjected to a report and investigation based upon stereotypes of parental characteristics (Raz, 2020; Wunder, 2010). Children from racial or ethnic minority households make up a disproportionate share of child protection cases, with indications that reporter bias may play a role in some cases (Flaherty & Fingarson, 2012). Therefore, cultural competence should be incorporated into the education and resources about mandated reporting of child abuse. Similarly, even without evidence of injury or other abuse, parents with disabilities may be reported to child protection based upon assumptions about their fitness to parent (Mudrick & Smith, 2017; National Council on Disability, 2012). Assumptions or misconceptions about a disability may lead a nurse to inaccurately assess child maltreatment where either a parent or a child has a disability (Caneira & Myrick, 2015; Wunder, 2010). Nurses receive limited education about, or little interaction time with, patients with disabilities, both of which influence attitudes of health care personnel towards individuals with physical disabilities (Satchidanand et al., 2012). Other examples of contexts that require nuanced understandings of child abuse and mandated reporting include situations involving domestic violence, substance use, or poverty (Davidov et al., 2012).
Each of these areas requires further study to determine best practices for educating nurses about, and supporting them in, their responsibility to identify and report child maltreatment. Future research also could assess the presence, content, and effectiveness of child abuse training across nursing educational programs, employers, and state agencies. The research could examine resources only accessible through licensure, the economic implications of additional training requirements, and the impact on outcomes for children and families. The responsibility for addressing these training challenges does not rest solely with the state agencies that license nurses and operate CPS. However, states can do more than they currently do to equip nurses to meet their mandatory reporter obligation confidently and ably.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.