
Abstract
The public and brutal death of Black American George Floyd was a tragedy that had the potential to push the profession of nursing toward a perspective transformation. A summative content analysis of 49 professional nursing organization statements served as a pilot to explore the research question: Did the nursing profession experience a perspective transformation relating to racial justice and health equity following the death of George Floyd? Texts from the statements were analyzed for the presence of an equity lens, which is necessary for a perspective transformation. Each statement was assigned a rating score to determine the organization's readiness for a perspective transformation based on equity competencies adapted from CommonHealth Action. Findings demonstrated that the nursing profession is beginning to articulate the issue of racism in health care and is committed to advocating for patients of color; however, further understanding of the historical context of structural racism and the development of meaningful policy remains necessary for the profession to experience a perspective transformation.
Introduction
Nursing professionals have long recognized the presence of health care disparities in society and the role nurses have in helping the United States achieve health equity (Institute of Medicine, 2011). However, noticeably absent from the profession's guiding documents was acknowledgement that structural racism in America must be addressed to achieve health equity. In 2010, the Institute of Medicine (IOM) published the 700-page Future of Nursing report, which failed to include the word racism (IOM, 2011). In 2015, the American Nurses Association (ANA) Code of Ethics for Nurses was updated. Racism was absent from the code and the accompanying interpretive statements (ANA, 2015). According to leading nurse scholar Dr. Kenya Beard, as recently as 2019, the nursing profession was not ready to talk about racism (NAM, 2021). That position notably changed following the public, brutal death of Black American George Floyd (widely shown on video).

This word cloud shows some of the commonly used terms in the statements.
George Floyd's death, which has been described as an awakening for America (Worland, 2020), has been widely defined as structural racism (Skolarus et al., 2020), including in nursing research (Knopf et al., 2021). Although multiple definitions for structural racism exist, the commonality of each definition is that it is found in the inherent prejudices identified in laws, government, economics, and even cultural or societal norms (Bailey et al., 2021). The Aspen Institute (2016) defined structural racism as the following:
A system in which public policies, institutional practices, cultural representations, and other norms work in various, often reinforcing, ways to perpetuate racial group inequity. It identifies dimensions of our history and culture that have allowed privileges associated with “whiteness” and disadvantages associated with “color” to endure and adapt over time. Structural racism … has been a feature of the social, economic, and political systems in which we all exist. (p. 1)
George Floyd's death was a cataclysmic event that had the potential to change nursing's perspective on racial justice by bringing the issue of structural racism to the foreground of discussions on health equity. According to Mezirow (1978), a perspective transformation, “a structural change in the way we see ourselves and our relationships” (p. 100), can occur when a dilemma creates enough anxiety and pressure to provoke change. Mezirow (1981) defined a dilemma as “the moment when the individual becomes critically conscious of how and why our habits of perception, thought, and action have distorted the way we have defined the problem and ourselves in relationship to it.” (p. 65).
The rapid change in the social consciousness of nursing following the death of George Floyd is demonstrable in several objective ways. In late May and early June of 2020, nursing organizations across the profession released statements condemning police brutality, acknowledging structural racism, and calling for systemic change (National Community Coalition (NCC), 2020). This change was precipitated by months of pandemic lockdown and years of increased racial tension. Nearly one year later, the updated 466-page Future of Nursing report was released, which referenced racism 193 times and structural racism 47 times (National Academies of Science, Engineering, and Medicine (NASEM) 2021).
The quick response from professional nursing organizations following the death of George Floyd signaled that nursing organizations were becoming critically conscious of structural racism. However, the degree of condemnation varied between nursing organizations, and it remained unclear whether nursing was ready to commit to long-term discussions about the relationship between health and structural racism. To empirically explore this issue, a pilot study was performed to determine whether the nursing profession had experienced a perspective transformation relating to racial justice and health equity.
A perspective transformation “implies a conscious recognition of the difference between one's old viewpoint and the new one and a decision to appropriate the newer perspective as being of more value” (Mezirow, 1978, p. 105). Accordingly, a perspective transformation is often perpetuated by a dilemma that causes pressure and anxiety and serves as the catalyst for a change in perspective (Mezirow, 1978). The witnessed death of George Floyd induced both societal pressure and anxiety, thus serving as the dilemma necessary to precipitate a perspective transformation.
Background
The death of George Floyd has been linked to institutional, systemic, and structural racism (NCC, 2020) and is emblematic of a system that has reinforced racial inequities. Regardless of which term is favored, the consensus is that nursing should be doing more to acknowledge the impact of racism on health outcomes (Iheduru-Anderson et al., 2021). The health care system in which nurses engage with patients is part of a greater societal structure; thus, it is important to consider the role nurses have in reinforcing or dismantling structural racism. Two separate studies have determined that naming institutionalized racism in public health and nursing literature is rare (Hardeman et al., 2018; Thurman et al., 2019); and that the most preferred term was structural racism (Hardeman et al., 2018). Therefore, for the purposes of this study, the term structural racism will be utilized.
Gee (2016) described racism as a social determinant of health; the racial hierarchy impacts where people live, work, learn, and access health care services. According to Weitzel et al. (2020), the nursing profession in the United States operates under the constructs of structural racism. Adherence to policies rooted in structural racism and a history of professional silence reinforces racist policies and allows health inequities to exist (Hall & Fields, 2013; Weitzel et al., 2020).
The murder of George Floyd at the hands of police exemplifies the disadvantage of color for Black males and the institutional practices and cultural representations that have led to disparate outcomes for Black, Indigenous, and People of Color (BIPOC) in the United States. As such, the death of George Floyd is consistent with the definition of structural racism and serves to remind nurses of how structural racism impacts health outcomes and their role in advocating for social justice.
Nurses have been ethically mandated to advocate for social justice since 1985, when language on social justice was explicitly added to the ANA Code for Nurses (Hanks, 2013). The most recent iteration of the nursing code of ethics is the profession's commitment to society (Epstein & Turner, 2015) and includes a commitment to integrating social justice into health care and health policy (ANA, 2015). Provision 9 of the ANA Code of Ethics details this commitment and further defines social justice in the following manner:
A form of justice that engages in social criticism and social change. Its focus is the analysis, critique, and change of social structures’ policies, laws, customs, power, and privilege that disadvantage or harm vulnerable social groups through marginalization, exclusion, exploitation, and voicelessness. Among its ends are: a more equitable distribution of social and economic benefits and burdens; greater personal, social, and political dignity; and a deeper moral vision for society. It may refer to a theory, process, or end (ANA, 2015, p. 46).
Despite nursings’ embrace of social justice, a lack of discussion regarding racial injustice still exists. Although a number of barriers to health are included, race is noticeably absent. Instead, the document highlights the nursing profession's responsibility to culturally diverse groups (ANA, 2015).
Evidence on racial disparities is widely accepted (American Public Health Association, 2001; IOM et al., 2003; NASEM, 2017), and the nursing profession readily acknowledges that health disparities exist for a number of reasons (ANA, 2015). In 2003, the IOM released a report titled Unequal Treatment that detailed the experience of BIPOC in the United States (IOM et al., 2003). This unequal treatment remains starkly visible through the lens of the COVID-19 pandemic as racial disparities related to infection rates, access to care, vaccine distribution, and mortality rates continue to be reported (Lopez et al., 2021).
Racial disparities and unequal treatment are not unique to the United States, and other countries have found themselves grappling with the realities of structural racism in health care. Nursing organizations in Canada, impacted by the death of George Floyd, released statements condemning structural racism and reaffirming their commitment to antiracism by referencing a policy statement on racism initially adopted in 2002 (Registered Nurses’ Association of Ontario [RNAO], 2020). However, the Canadian Nurses Association Code of Ethics for Nurses (2017) does not include the word racism. Similarly, the code of ethics for nurses in Australia (International Council for Nurses, 2021) and the United Kingdom (Nursing and Midwifery Council, 2018) fail to mention racism.
The last time the ANA Code of Ethics was updated was 2015 (ANA, 2015). Since that time, a racial reckoning has occurred in the United States precipitated by the Black Lives Matter (BLM) movement (Brandeis, 2020). In 2020, as the nation began to realize the implications of the COVID-19 pandemic, the dual pandemic of racism was fully acknowledged (Brodie et al., 2021). This acknowledgment followed the deaths of Ahmaud Arbery, Breonna Taylor, and George Floyd (Tsega & Childs, 2021). Nursing's increased focus on structural racism following the death of George Floyd was mirrored by society. Trends monitoring support for the BLM movement saw a significant uptick following the death of George Floyd, as evidenced by both social media postings and polling data (Anderson et al., 2020; Horowitz, 2021; Shah & Widjaya, 2020). Twitter postings referencing #BlackLivesMatter spiked to an unprecedented number of 8.8 million two days after the death of George Floyd (Anderson et al., 2020). Some of those posts were made by professional nursing organizations (APHA Public Health Nursing, 2020).
Research Question
The public and brutal death of Black American George Floyd created a cultural dilemma that had the potential to push the profession of nursing toward a perspective transformation. A summative content analysis of 49 professional nursing organization statements served as a pilot to explore the research question: Did the nursing profession experience a perspective transformation relating to racial justice and health equity following the death of George Floyd?
Theoretical Framework
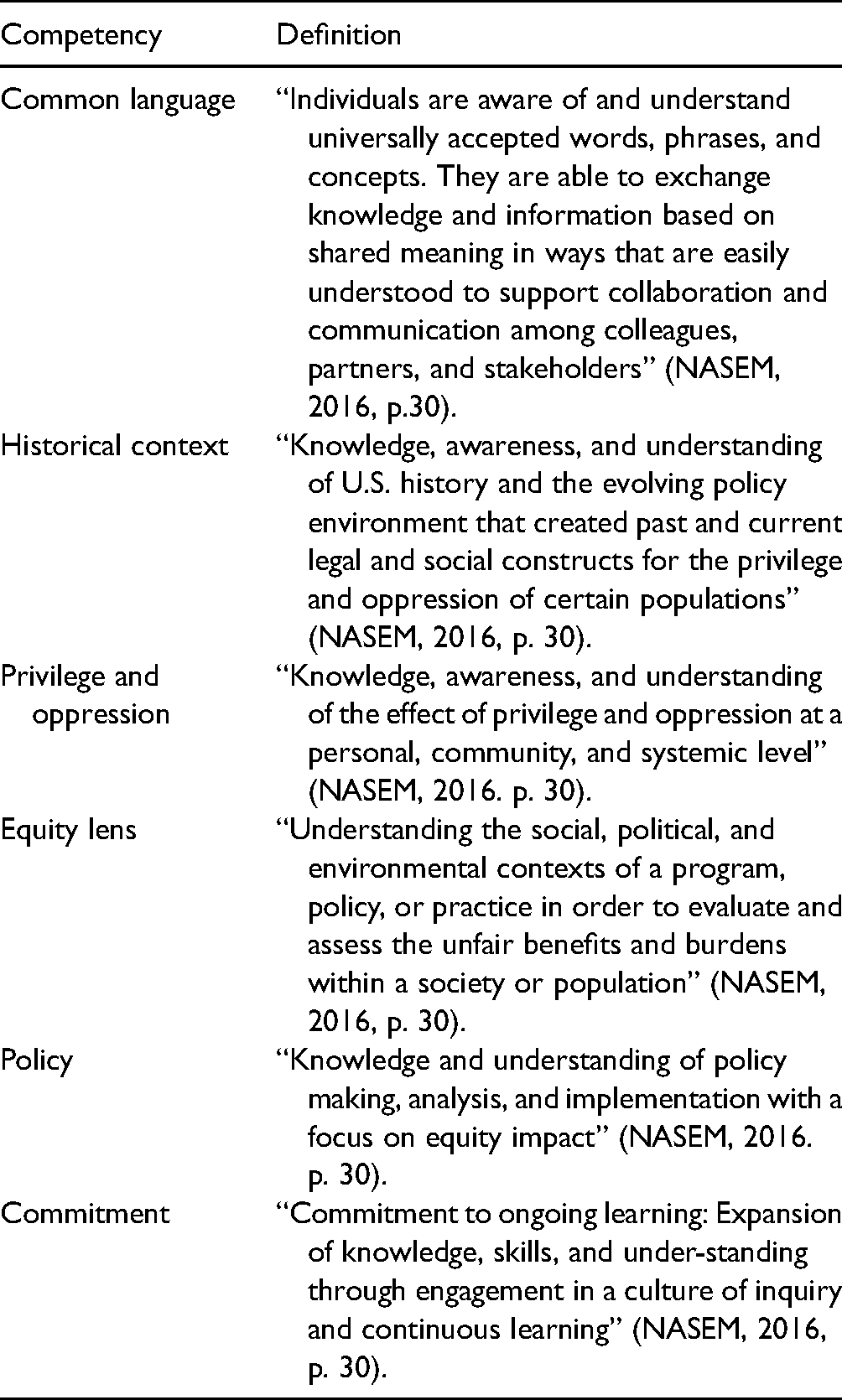
The CommonHealth Action Equity Competencies are part of an equity, diversity, and inclusion (EDI) framework that aims to assist organizations in developing an equity lens (see Table 1; NASEM, 2016). According to the CommonHealth Action (NASEM, 2016), development of an equity lens is requisite for experiencing a perspective transformation as defined by Mezirow (1978). Essentially, an equity lens is required to “understand the social, political, and environmental context of a program, policy, or practice in order to evaluate and assess the unfair benefits and burdens within a society or population” (NASEM, 2016, p. 30).
CommonHealth Action Equity Competencies (NASEM, 2016).
The relationship between developing an equity lens and achieving a perspective transformation served as a theoretical framework for the research question. We surmised that viewing structural racism through an equity lens did allow nursing to experience a perspective transformation.
Method
Study Design
Using classical content analysis, word count, keyword in context (KWIC), and a rating scale, each organization statement was evaluated for a perspective transformation. The rating scale measured the presence of the code families (see Supplementary Resources) that were adapted from the CommonHealth Equity Competencies. Determining these ratings was necessary for inferring whether nursing had experienced a perspective transformation because meeting these competencies allowed organizations to develop an equity lens necessary for a perspective transformation (NASEM, 2016). The George Washington University Institutional Review Board determined this study to be exempt.
Sampling Frame
Professional nursing organizations serve as a collective voice for the nursing profession. According to the ANA Code of Ethics (2015), professional nursing organizations are obligated to advocate for social justice and to serve as the collective conscience of nursing. Historically, published statements from nursing leadership on structural racism have been absent, and in a recent call for U.S. nursing leadership to address structural racism, leadership was only able to cite international organizations as examples (Nardi et al., 2020). However, following the death of George Floyd, professional organizations across medicine and nursing released statements that have been reviewed by researchers across disciplines to identify common themes and key elements (Kiang & Tsai, 2021; Knopf et al., 2021).
According to Nurse.org (2021), 189 national nursing organizations exist in the United States. After consulting with an expert on nursing organizations from the George Washington University School of Nursing, we were directed to the NCC. The NCC consists of 63 member organizations that are representative across the nursing profession and includes organizations encompassing practice, education, regulation, and research (NCC, n.d.). In June 2020, the NCC released a unified statement on racism and injustice with accompanying links and texts to 48 individual member statements (NCC, 2020). This document served as a census document for a convenience sample of professional nursing organization statements.
Search Strategy
Since the NCC document was incomplete and some member statements were not listed, snowballing was required to increase the sample size. Using a simple Google search for the name of the organization and its statement on George Floyd, e.g. Dermatology Nurses’ Association statement on George Floyd, an additional nine statements were located on member websites or social media platforms, including Twitter and Facebook. Statements that did not have a date or text that allowed for context relative to the death of George Floyd were eliminated.
Data Collection
Ultimately, 49 member statements were located and included in the final sample.
Coding
A coding scheme was developed based on the literature (Gee, 2016; Giddings, 2005; Hall & Fields, 2013; Iheduru-Anderson et al., 2021; Jones, 2002; Mezirow, 1978) and competencies from CommonHealth Action (NASEM, 2016). The competencies served as a framework for developing a codebook (see Supplementary Resources) that was applied during the content analysis. After the preliminary codebook was developed, the codes were applied to two pilot statements. The codebook was then further refined and clarified. In addition, texts from the two pilot statements were added to the codebook to serve as exemplars for each coding category.
Analysis
The codebook included explicit instructions on how to complete the data analysis.
Using classical content analysis and abductive reasoning (Krippendorff, 2018), the 49 organization statements were reviewed, and text was highlighted and coded according to the codebook categories. After reviewing each statement, the process was repeated to capture any remaining codes. The content analysis was completed by two separate coders, both of whom serve as faculty for university schools of nursing and are experienced in qualitative research. The coders worked independently of one another during this process and then completed an iterative process to consult on any discrepancies. There was high level of compatibility between the two coders, resulting in a Kappa statistic of 0.80 −1.00. The Kappa statistic was calculated by a third independent researcher.
The KWIC method was utilized to search for key terms that were previously identified using the Racial Equity Tools glossary (2020). The coders then reviewed the context surrounding keywords and applied any additional codes using the codebook. A simple word count function allowed coders to quantify the total number of times keywords were utilized, identify additional keywords, and to quantify how often professional nursing organizations invoked the death of George Floyd when framing the issue of health equity and racial justice. Coding and data analysis were completed using NVivo 12 software.
Trustworthiness
A number of processes support the trustworthiness of the content analysis, including method, investigator, and theory triangulation (Carter et al., 2014). We believe we demonstrate trustworthiness and credibility in our study through documented and systematic description or of planning and methodological processes. Collectively, we believe that the application of the theoretical framework to guide this work, our systematic methodological and sampling procedures, the NVivo analysis conducted by two coders to assess inter coder reliability, which also produced an audit trail for data and findings, and calculation of the kappa statistics further supports the trustworthiness, credibility, and rigor of our methods, data analysis, and findings (Nowell et al., 2017).
Results/Findings
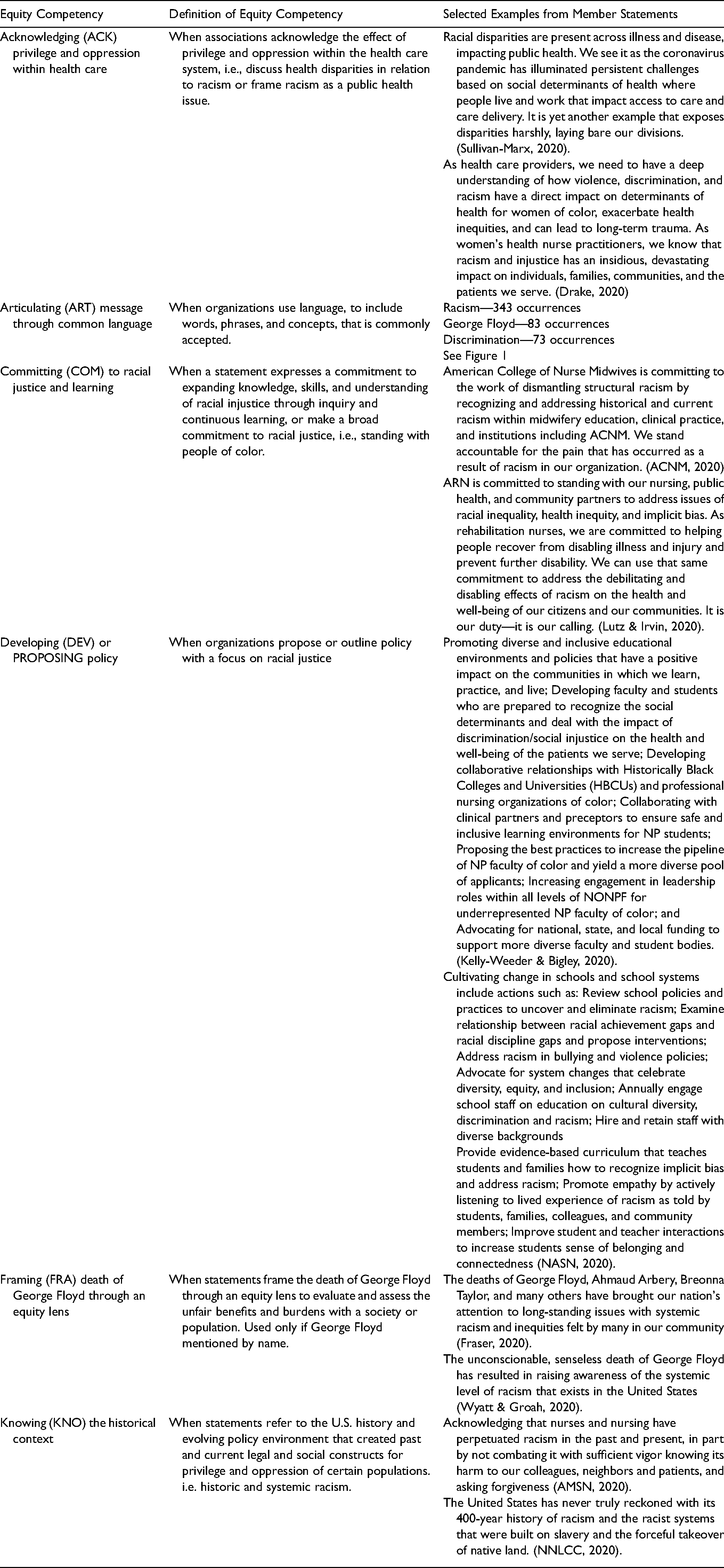
The adapted equity competencies served as a checklist based on the codebook and resulted in the following six categories: acknowledging, articulating (ART), committing (COM), developing (DEV), framing (FRA), and knowing (KNO). See Table 2 for definitions and for selected examples from text.
Adapted Equity Competencies with Example of Supporting Text.
As with any competency checklist, we assumed that the more competencies an organization has met, the more competent the organization. A nursing organization statement with a higher rating score met a higher number of equity competencies. An organization with a rating of 6 met all of the equity competencies. We inferred that these organizations were most likely to be viewing the death of George Floyd through an equity lens and thus were able to experience a perspective transformation. See Table 3 for the equity competency checklist results and perspective transformation ratings for each of the 49 member statements.
Organization Statement’s Equity Competencies Checklist with Perspective Transformation Rating Score.
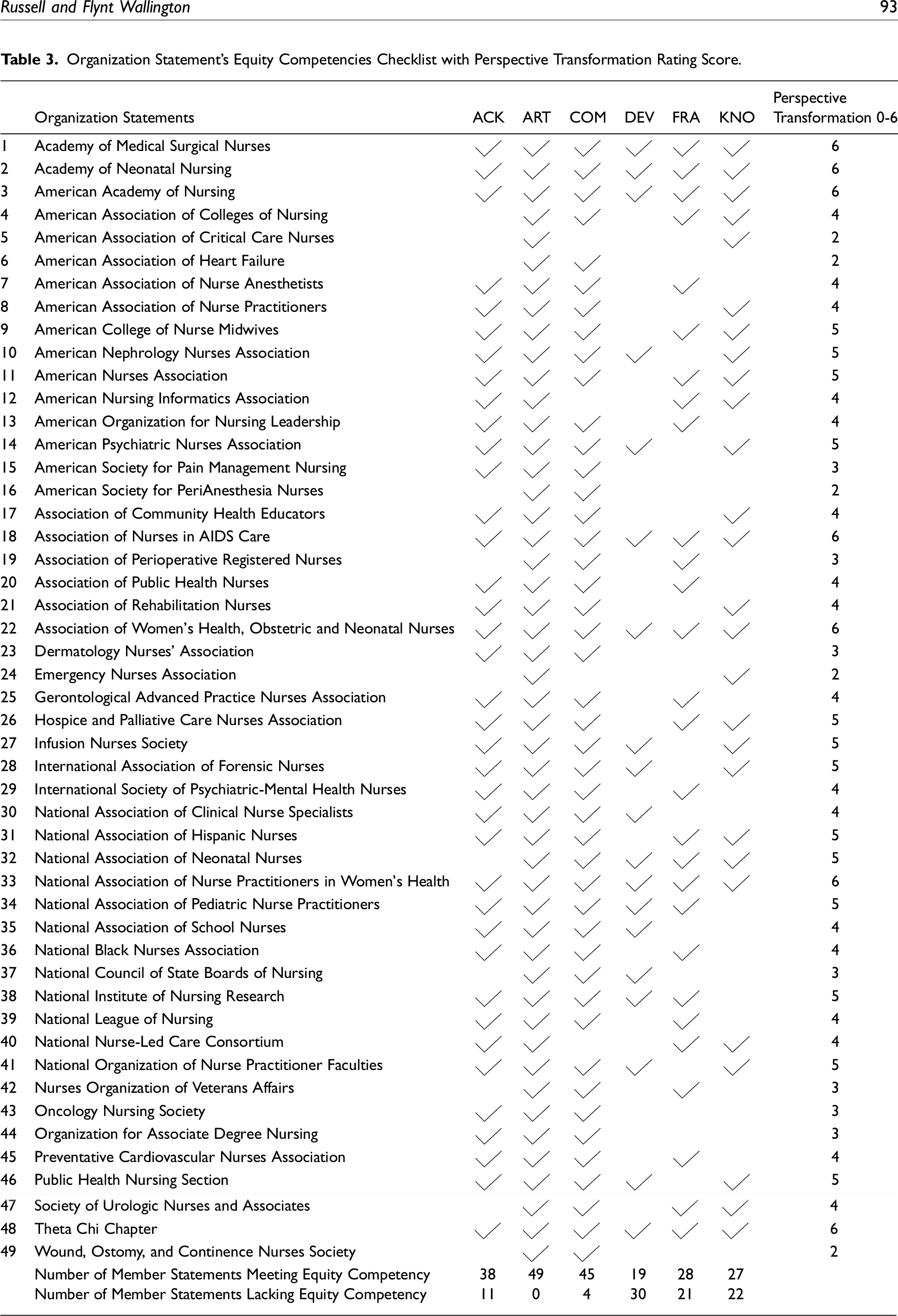
A total of seven organization statements were determined to have met all of the equity competencies based on the coding schematics and scored a 6 on the rating scale. These organizations—the Association of Women's Health, Obstetric, and Neonatal Nurses (AWHONN); the Academy of Medical Surgical Nurses (AMSN); the Academy of Neonatal Nursing (ANN); The American Academy of Nursing (AAN); the Association of Nurses in AIDS Care (ANAC); the National Association of Nurse Practitioner's in Women's Health (NPWH); and the Theta Chi Chapter of Chi Eta Phi Sorority—represent a cross section of specialty groups active in nursing practice and policy.
Seventeen statements scored a four on the rating scale, with the vast number of those statements lacking proposals on how to address structural racism and thus not meeting the standard for the developing (DEV) competency. Overall, the equity competency most lacking within the statements was the DEV competency, followed by KNO, and FRA. All 49 member statements met the ART competency, indicating that commonly accepted racial equity terms and phrases were used to compose the statements. In addition, all but four organizations had committed (COM) to racial justice and ongoing learning.
The findings of this content analysis demonstrate that members of the NCC were ready to articulate the issue of structural racism in America following the death of George Floyd. These organizations, in large, committed to standing by communities of color and participating in structural change. The organizations consistently demonstrated an understanding of racism's impact on health outcomes and acknowledged racism as a public health crisis.
Discussion
The content of the statements depict that nursing organizations are beginning to discuss race and the impact racism has on health, as well as COM to stand with BIPOC individuals. However, these statements were inspired by the death of George Floyd, and 21 member statements failed to mention George Floyd by name, thereby failing to frame the issue of his death through an equity lens. How can nursing undergo a perspective transformation if the professional organizations cannot invoke the name of a man whose death necessitated the release of the statements analyzed?
Insight into the historical context of structural racism was missing in 22 member statements. This lack of knowledge results in overlooking the policies, institutions, and systems that have perpetuated structural racism—including the health care system and the profession of nursing. Last, developing and proposing policy solutions is necessary for nursing to fully view structural racism through an equity lens. Concrete proposals on how the organization planned to address structural racism was absent from 30 member statements. This failure to put words into action is perhaps the largest barrier nursing must overcome to achieve a perspective transformation and dismantle systems and institutions that reinforce racist policies.
Since the completion of this content analysis, two studies have been published that analyzed institutional statements released following the death of George Floyd (Kiang & Tsai, 2021; Knopf et al., 2021). Kiang & Tsai (2021) completed a cross-sectional study of medical school statements and identified key elements each statement should contain to provide meaningful leadership from the medical community. These elements, while separate from our adapted equity competencies, did share some commonality with the codes used in this content analysis. For example, naming the victim by name is the same as the requirement to frame the statement through the death of George Floyd. Explicitly naming racism and using language of support is similar to ART health equity language. Similar to the nursing statements, the medical school statements failed to knowingly state the historical context of structural racism in the United States (Kiang & Tsai, 2021). The commonalities between criteria lend credence to the health equity competency codes utilized in this study.
The qualitative study by Knopf et al. (2021) used thematic analysis to identify common themes from three professional nursing organizations. The three statements included in their sample were all included in our sample of 49 NCC member organizations. Although their study used inductive reasoning to identify themes to then apply to nursing school statements (Knopf et al., 2021), our study focused on using abductive reasoning and an adapted health equity competency checklist that allowed us to apply a perspective transformation rating score. The themes identified by Knopf et al. (2021) also share commonalities with the health equity competencies, including ACK the impact of racism on health and commitments to end structural racism. These similarities between the themes and health equity competency codes reinforce the appropriate use of the CommonHealth Action Equity Competencies (NASEM, 2016) as a theoretical framework for this study.
Implications for Future Research
Although the aforementioned studies support the use of the CommonHealth Equity Competencies, further research is necessary to validate this method of evaluating for perspective transformation. This process could include reviewing all 189 professional nursing organizations for statements on George Floyd and completing a summative content analysis more representative of the nursing field. In addition, further appraisal of professional nursing organizations’ contemporary activity can serve to determine whether additional equity competencies were achieved at more recent dates and whether organizations were able to maintain competence over time.
Implications for Nursing
The Registered Nurses’ Association of Ontario, motivated by the death of George Floyd, went “beyond a moment” (Brathwaite et al., 2022, p. 3) by creating a Black Nurses Task Force. In the United States, leading nursing organizations also sought to go beyond the moment and created the National Commission to Address Racism in Nursing in 2021 (ANA, 2021). The commission meets monthly with a goal of proposing and outlining strategies and policy with a focus on racial justice across the spectrum of nursing (ANA, 2021). Brathwaite et al. (2022) speaks to the importance of going beyond a task force and commission to actively engage stakeholders and build a social movement. Nursing organizations need to connect with their members. The profession needs leadership and guidance from nursing organizations, but we also need a grassroots movement where nurses at the practice level are motivated to improve patient outcomes and sustain change through acknowledgement of structural racism.
The new Future of Nursing report provides a roadmap for nursing to advance health equity by dismantling the confines of structural racism in health care (NASEM, 2021). We need to update the ANA Code of Ethics for Nurses to include the terms racism, structural racism, and health equity. We need to be explicit in our language and our duty as nurses. We cannot forget our pledges, inspired by George Floyd, to commit to racial justice. We need bold and sustained change that goes beyond issuing statements so that nursing's allyship to racial justice is fully recognized.
Limitations
A number of limitations within our study must be acknowledged. First, we did not review all 189 national nursing organization websites for statements related to the death of George Floyd. Although our sample consisted of representative organizations across the profession, we did rely on a convenience sample, which lends itself to sampling bias.
Additionally, it should be noted that while most statements met the COM equity competency, the level of commitment was variable between statements. Some organization statements outlined a commitment that was present throughout the statement and left no doubt that the organization was committed to ongoing advocacy for racial justice. Other statements met the threshold by voicing support for communities of color or standing against racism but lacked insight into how this commitment should be honored.
Last, in assigning a rating score based on the equity competencies met, each equity competency was given equal weight. This would imply that simply ART language that is consistent with racial equity is of equal merit to FRA the death of George Floyd through an equity lens, or that ACK statistics and health outcomes impacted by racism is meaningful without knowing the historical context behind structural racism in the United States. Furthermore, granting equal weight to each equity competency could imply that a commitment to people of color is possible when there is no clear plan to dismantle structural racism through development of meaningful antiracist policy.
The professional organization statements lend insight into the nursing profession's stance on structural racism following the death of George Floyd, but these statements are only snapshots in time. While an important body of information, the statements provide an incomplete picture of whether the profession of nursing has experienced a perspective transformation. What we can say is that these statements are evidence of a readiness to name and discuss structural racism in a way that has been historically limited in nursing literature. This articulation, acknowledgement, and commitment are positive steps forward toward a perspective transformation. Now the profession must knowingly discuss the history behind structural racism, frame issues of racial inequity through an equity lens, and develop meaningful policy. Achieving a perspective transformation may allow nursing to address structural racism within our own ranks, within the health care system, and within the lives of our patients of color—a necessary feat for achieving health equity.
Conclusion
Through public statements, professional nursing organizations make their values known to the public, including a dedication to social justice (ANA, 2015). Analyzing statements made by professional nursing organizations provided insight into the nursing profession's stance on structural racism. The NCC organizations represent the major sectors of the nursing profession: practice, education, regulation, and research. These statements provide a roadmap for the nursing profession to address structural racism in nursing and deserve further scrutiny through additional research and ongoing dialogue with professional nursing organizations.
Nursing's often passive role has reinforced structural racism and a cycle of discrimination that has both historical and contemporary health care consequences. Mezirow (1978) indicated that a dilemma is necessary for perspective transformation and allows for advancement toward a perspective that is more inclusive and integrative. The death of George Floyd was a dilemma for nursing, one that forced the profession to confront its role in perpetuating structural racism and to collectively label racism a public health crisis. This summative content analysis substantiates that nursing is ready to discuss racism through an equity lens, an integral step required for perspective transformation and a more inclusive and integrative profession.
Supplemental Material
sj-docx-1-ppn-10.1177_15271544221089657 - Supplemental material for Structural Racism in America: A Summative Content Analysis of National Nursing Organization Statements
Supplemental material, sj-docx-1-ppn-10.1177_15271544221089657 for Structural Racism in America: A Summative Content Analysis of National Nursing Organization Statements by Naila C. Russell and Sherrie Flynt Wallington in Policy, Politics, & Nursing Practice
Footnotes
Acknowledgments
The authors would like to thank Dr. Joyce Pulcini for her thoughtful guidance and support and the George Washington University Center for Health Policy and Media Engagement for the fellowship opportunity.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.