
Abstract
Medication administration is a critical safety issue in hospitals and the community. Children are especially at risk because of their dependence on adults to safely administer medications. The purpose of this study was to examine non-compliance with state child care medication administration regulations and factors associated with improved compliance. The data included routine, unannounced inspections of child care programs by state licensing specialists collected in two time periods over 10 years. Factors potentially associated with regulatory compliance were included in this secondary analysis. Most child care center medication administration regulations showed decreased non-compliance between the two time periods. However, regulations pertaining to prescriber orders and parent permission revealed a significant increase in non-compliance (58.4%). Factors positively associated with medication administration regulatory compliance included: compliance with annual professional development (p < 0.0001 in both periods), achievement of accreditation (p = 0.0115 in Time 1), and among centers with children under 3 years of age, compliance with a weekly mandatory visit by a nurse consultant (p = 0.0004 in Time 2). Though family child care homes had a lower frequency of medication administration non-compliance, only 19% were administering medications in Time 1. High quality, safe, and affordable child-care is essential for all children including those with special health care needs. This study highlights the importance of medication safety practices in child care programs, national child care health and safety standards, federal and state policies regarding medication administration regulations, and the critical role of nurse child care health consultants in promoting safe medication administration in child care programs.
Medication errors, “any preventable event that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the health care professional, patient, or consumer” (National Coordinating Council for Medication Error Reporting and Prevention, n.d.), are well documented causes of injury and death in hospitals (Hicks et al., 2006; Institute of Medicine, 1999; Kaushal et al., 2001) and increasingly recognized as a problem in community settings (Carvalho et al., 2021; Smith et al., 2014). Children, whose small size creates a narrower margin of error, and whose limited ability to communicate and question potential errors, are especially at risk (Poole & Carleton, 2008). In a study of pediatric primary care practices, Kaushal et al. (2007) reported that adverse drug events occurred in about 16% of children treated with medications. The process of ordering and administering medications has multiple steps: writing the prescription, transmitting the order to the pharmacy, dispensing, administering, and monitoring (Kaushal et al., 2007). Administration of medication accounted for 70% of the preventable adverse drug events and was most commonly due to parent error. In a randomized controlled trial to assess parents’ accuracy measuring liquid medications, Yin and colleagues (2010) reported that 84.4% of parents made at least one or more dosing errors. Child care providers, who usually have no more training in administering medications than parents but may administer medications to a number of children in their care, may be at risk for causing adverse drug events.
Before the COVID-19 pandemic, approximately 12 million children were enrolled in some form of out of home child care (Laughlin, 2013). The data snapshot of children with special health care needs (HRSA Maternal & Child Health, n.d.) revealed that one in four households have at least one child with a special health care need, and many of these children require medication daily or for a life-threatening condition while in child care. Therefore, medication safety in child care programs is critical. All four editions of Caring for Our Children: National Health and Safety Performance Standards (CFOC) (American Public Health Association [APHA] & American Academy of Pediatrics [AAP], 1992; AAP et al., 2002; 2011; 2019) have included standards on medication safety, including training, to address this need. However, in 2011 and 2012 reviews of state child care regulations only 13 states required medication training for providers administering medications in child care centers (Viall & Crowley, 2012) and 5 states for family child care homes who cared for 12 or fewer children (Rei & Crowley, 2013). Furthermore, few studies have explored incidence of medication errors and related morbidity and mortality in child care settings (Sinkovits et al., 2003). The lack of studies may be due to the low percentage of states that require reporting of medication errors in child care programs and consequently insufficient data. To address the potential risk of medication errors in child care programs, The Child Care and Development Block Grant (CCDBG) Act of 2014 (Administration for Children and Families [ACF], USDHHS, 2016) included medication administration training for child care providers among 10 health and safety training requirements for all states and territories which participate in the Child Care Development Fund (CCDF) program.
Connecticut has a long history of requiring medication administration training, which includes not only giving medications but accepting and interpreting prescription orders, handling and storage of medications, and monitoring side effects and adverse reactions, for non-licensed child care providers administering medications (Heschel et al., 2005). The regulations are among the most stringent in the country. However, no published study has examined the prevalence of medication administration regulatory non-compliance and factors which may promote compliance, such as child care provider professional development compliance; child care center accreditation by the National Association for the Education of Young Children (NAEYC); type of program, that is, Head Start, state-funded, public pre-K, nurse child care health consultant visits and median income of the child care program. Thus, such an analysis may provide an evidence-based lens for states that are currently instituting medication administration training and promote efforts to improve medication safety in child care programs.
The purpose of this paper is to describe the prevalence of medication administration regulatory compliance and non-compliance documented during routine, unannounced licensing specialists’ inspections of child care centers and family child care homes and factors, that is, variables, associated with compliance. This study addressed the following research questions: (1) What is the frequency of non-compliance in medication administration regulations of child care centers and family child care homes as determined by unannounced, routine inspections? (2) Is there an association of medication administration regulation compliance with the following child care center factors: (a) NAEYC accreditation, (b) program type (state-funded child care, School Readiness [state pre-K)] programs and Head Start in community settings), (c) access to a trained child care health consultant (CCHC), (d) compliance with professional development for child care providers, (e) compliance with the requirement for a weekly CCHC visit for centers that enroll children under three years of age, and (f) median household income of the child care location?
Methods
This study used data in the public domain and performed a secondary analysis to address the research questions. We examined the findings of routine, unannounced licensing specialists’ inspections of child care centers and group child care homes and family child care homes. In Connecticut centers are defined as programs which enroll 13 or more children. Group child care homes and family child care homes are two designations for child care located in the home of a family licensed provider; the former includes programs enrolling 7–12 children and the later includes homes with fewer than 7 children. Group child care providers must adhere to regulations for center-based programs. Hereafter, centers and group child care homes will be referred to as CCC and family child care homes as FCCH. During the first time period, CCC were routinely inspected every two years and FCCH every three years. Whereas annual routine inspections of CCC and FCCH were conducted during the second time period. The two time periods were selected based on the researchers’ interest in studying trends in regulatory non-compliance, factors associated with compliance, and availability of funding to support this work.
The Time 1 inspections were conducted between January 2006 and March 2008. The CCC sample included both retrospective data, i.e., licensing inspection reports collected between January 2006 and August 2007, which were part of an internal review by Department of Public Health (DPH) Environmental Health Section, and prospective data, i.e., all copies of licensors’ inspection reports collected between September 1, 2007 and March 31, 2008. DPH did not reveal the sampling methodology for the retrospective data. For the CCC sample we collected all inspection reports between September 1, 2007 and March 31, 2008. DPH redacted all the reports, i.e., removed extraneous, confidential data, e.g., child's name; however, all other data that are in the public domain were included in the database. DPH hard-copy licensing-report data were entered into two copies of a Microsoft Access database by research assistants, Health Insurance Portability and Accountability Act trained graduate students, to conduct PROC COMPARE (SAS version 9.2 SAS Institute, Cary, NC) to clean the data to ensure that all key punch errors were corrected. Licensing specialists’ comments were included in the database as well. This sample was part of a larger study which examined CCC and FCCH compliance and non-compliance with all child care regulations during routine unannounced inspections (Crowley & Rosenthal, 2009). Findings, except for compliance with medication administration regulations, were previously published (Crowley et al., 2013; Rosenthal et al., 2016).
Time 2 inspections were conducted between January 2016 and November 2017 by licensing specialists in the Office of Early Childhood (OEC) and selected to ensure at least one unannounced inspection of each CCC and FCCH. For CCC and FCCH that had more than one inspection, the first inspection during that time-period was used for analysis. Data were downloaded from the Connecticut Open Data online platform (CT DATA, n.d.) which was created after the first time period. Connecticut Open Data licensing-report data were uploaded into a Microsoft Access database to filter, extract and clean the data. No human subjects were included in this study, and the analysis was conducted according to prevailing ethical principles. This sample was part of a study which examined FCCH compliance and non-compliance with all child care regulations during routine unannounced inspections. Findings, apart from compliance with medication administration regulations, were previously published (Rosenthal et al., 2020).
Variables and Additional Data Sets
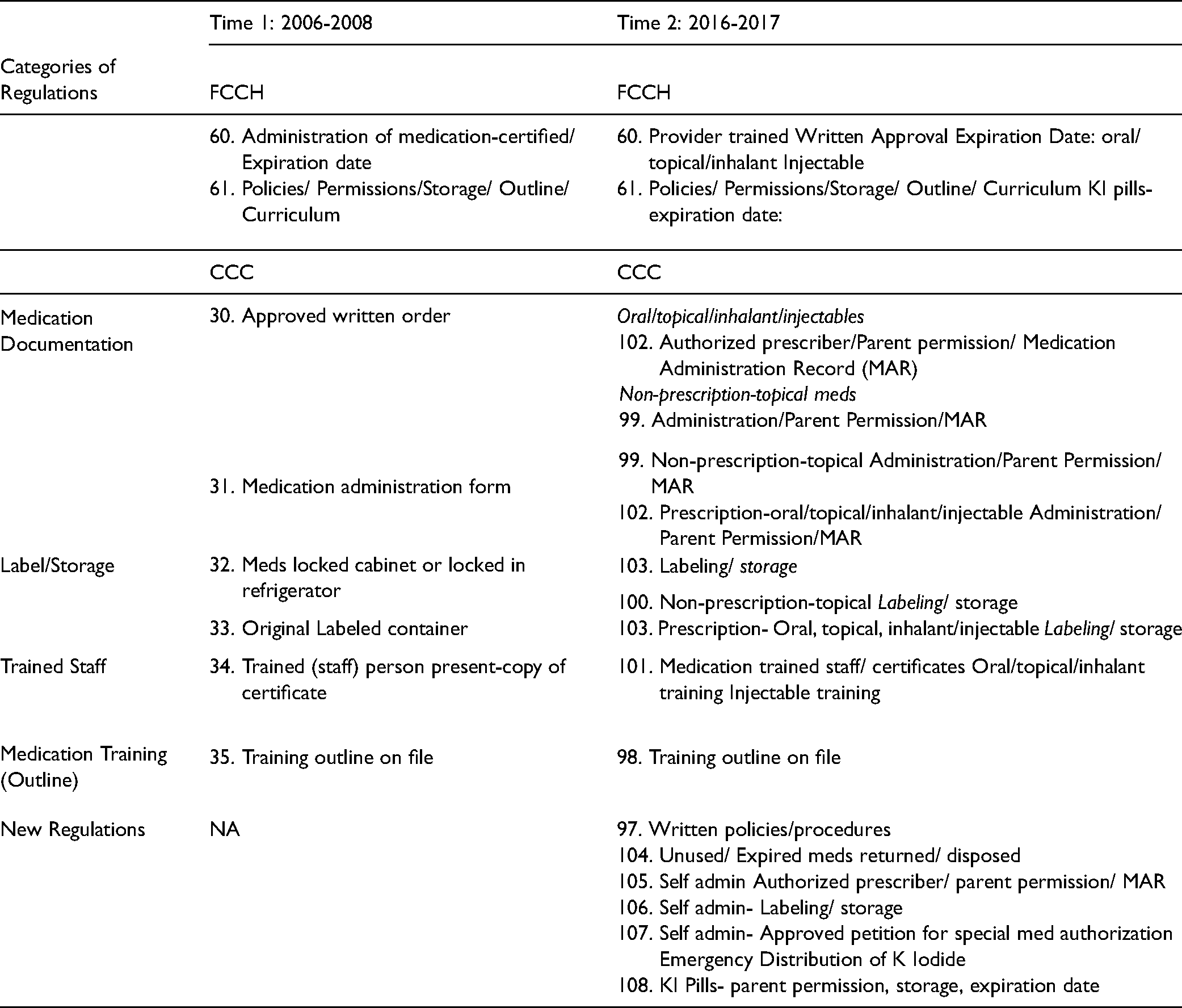
Table 1 lists the medication administration regulations during the two time periods of data collection. Also, included are medication regulations created after Time 1. Although FCCH had the same medication administration regulatory requirements as CCC, only two inspection items pertained to medication administration, which limited our analysis. For the CCC inspection forms in Time 1, 6 regulations pertained to medication administration and in Time 2, 10 regulations. The later regulations are more detailed and specific to types of medication. For example, in 2006–2008, item 32, refers to medications locked and item 33, medications labeled in original container; whereas the regulation for locked and labeled medications are combined in items 100 and 103 in Time 2. Most of these regulations are operationalized as binary variables, i.e., compliant or noncompliant. However, the licensing specialists’ responses, i.e., “pending”,” not observed” and “not applicable at this time”, were included in the database the researchers created in Time 1 but not in the Time 2 database created by the state. OEC staff reported that during Time 2, licensing specialists collected all the responses but did not include: “not observed” and “not applicable at this time” in the data base (D. Johnson, personal communication, July 14, 2017). During Time 1, licensing specialists included comments describing items which did not meet regulation requirements. Although licensing specialists included comments in the Time 2 licensing reports, that information was not in the database and therefore not available to the researchers.
Medication Administration Licensing Regulations: FCCH and CCC.
For Time 1 we had access to data sets that represented the variables of interest, specifically: Head Start, NAEYC Accredited, School Readiness funded, state funded and CCHC trained. Each CCC was categorized as either enrolled in the above groups or not. To accomplish this characterization, first we merged data sets from the Head Start Locator Web site (Head Start, n.d.), NAEYC Accreditation Web site (NAEYC Accreditation, n.d.), Connecticut Department of Social Services School Readiness database (file sent via e-mail by Peter Palermino, Child Care Administrator, on February 6, 2008), and the Connecticut Nurses’ Association database (2002–2007) of trained CCHCs (file sent via e-mail by P. Anderson on January 15, 2008). During both time periods, we categorized CCC as continuing education/ professional development compliant or not; registered nurse (RN) log on-site/ health consultant documentation or not; and median income of CCC zip code per $10,000 increments.
For both time periods, we identified additional regulations, e.g., continuing education, which was identified in 2016–2017 as professional development, and RN log on-site, later referred to as health consultant documentation of visits, that we hypothesized may be markers for compliance. Continuing education/ professional development is a regulation, which is assessed for all CCC. Connecticut CCC regulations require that providers must show evidence of 1% of annual work hours or 20 h for full-time workers of continuing education each year in areas, e.g., early childhood education, child development, and health topics. There is no minimum requirement of hours in any specific topic area, e.g., health and safety, and specific training topics are not listed on inspection forms. The regulation RN log on-site/ health consultant documentation refers to compliance with a weekly health consultant visit for CCC that enroll children under three years of age full-time. Although CCC enrolling preschool children only are required by regulation to have quarterly health consultant visits, during both time periods of this study, licensing specialists reviewed compliance only when children younger than three years old were enrolled. The independent variable “trained CCHC” included nurses, who fulfilled the requirement for RN log on-site and were formally prepared for the role through a federally funded training program. To explore the influence of income as a predictor of medication administration compliance, we first derived median income per $10,000 increments from zip codes of CCC and FCCH. Median household income was merged with zip code data of CCC and FCCH for both time periods (U. S. Bureau of the Census, 2019). We then dichotomized income at the median level. Although zip-code median income does not specifically reflect the resources available for a child care program, it serves as a reasonable proxy (Krieger et al., 1997).
As university-based researchers, we received funding from a private foundation to conduct this study. We used data collected by child care licensing specialists in the Connecticut DPH in Time 1 and by the Connecticut OEC in Time 2 as well as other data sets available during Time 1 to explore these questions and provide the first aggregate report of medication safety of Connecticut licensed CCC and FCCH.
Data Analyses
First, we identified the frequency of compliance with medication administration regulations for CCC and FCCH. We combined related regulations and created four dichotomized categories of regulations, including medication documentation, label and storage, trained staff, and medication training outline using compliance on related regulations in Time 1 and 2. In order to determine characteristics of CCC associated with compliance with regulations, we employed latent class analysis (LCA) using PROC LCA (Lanza et al., 2003; Lanza et al., 2007) and produced compliance groups based on the patterns of dichotomized compliance level (compliance vs. non-compliance) on four categories of regulations (i.e., medication documentation, label and storage, trained staff, and medication training outline) during both time periods. LCA identified compliance groups with similar patterns of compliance for the four categories of regulations and classified CCC into one of the identified compliance groups. The number of compliance groups was determined using goodness-of-fit criteria, including the likelihood-ratio G2 statistic, Akaike's Information Criterion (AIC), Bayesian Information Criterion (BIC), Consistent AIC (CAIC), and the adjusted BIC. We characterized and named the identified compliance groups by the patterns of the four categories of regulations, and the CCC were grouped into one of the compliance groups.
For Time 1, we assessed potential factors, including NAEYC accreditation, program type (specifically, state-funded, School Readiness (state pre-K), or Head Start in community settings), compliance with continuing education, and dichotomized median household income of CCC zip code and factors that might promote medication administration compliance by testing the associations with the compliance group from LCA using the Chi-square test. Compliance with CCHC trained and RN/health consultant log were tested as potential factors only in CCC including children under 3 years old. To address the potential for variability of compliance reported by multiple licensing specialists during Time 1, we tested the associations again using multinomial model with the random effect of licensing specialists incorporating the correlation within center inspected by the same person. This random effect was tested and removed if it was not significant. For FCCH we assessed compliance with dichotomized median household income of FCCH zip code.
For Time 2, we assessed some potential factors, which might promote medication administration compliance, and tested the association between the compliance group and those factors, including dichotomized median household income and compliance on professional development and RN/health consultant log using the Chi-square test. We also tested the compliance on RN/health consultant log only in CCC including children under 3 years old. Since licensing specialist identification was not available in the Time 2 data set, we could not use the random effect model in samples for that time period.
For FCCH, we assessed compliance with two medication administration regulations, and compared the frequency of the compliance between dichotomized median household income of FCCH zip code at Time 1 and 2, separately, using the Chi-square test. This analysis was repeated only for FCCHs with medication on site.
Results
The sample comprises two time periods of data collection. Time 1 included 676 first routine inspections of CCC between January 2006 and March 2008 of which 232 (34.3%) were retrospective and 444 (65.7%) were prospective and represented 41% of CCC since inspections were conducted biannually (Table 2). Because “not observed/ not applicable” responses were entered into the database, we determined that 503 (74%) centers had medications on site since they were required to have a trained staff person at the time of the inspection. At that time, FCCH were inspected every three years; 594 first routine inspections which were conducted between September 2007 and March 2008 and represented 28% of licensed programs were included in the sample. Because the expiration date of medication certification was included and entered into the database in addition to FCCH non-compliant with the training outline requirement, we determined that 114 (19%) of FCCH were administering medications at the time of inspection. Time 2 included the first unannounced annual inspections of 1,161 CCC and 1,934 FCCH between January 2016 and November 2017, and thus includes most, if not all licensed programs. However, programs which were administering medications could not be identified because “not observed”/“not applicable” and certification expiration date responses were not carried over into the database and therefore could not be distinguished from programs not administering medications (D. Johnson, personal communication, July 14, 2017). Consequently, programs that did not administer medications would therefore be designated as compliant, which presents a different condition and could potentially inflate the number of compliant programs.
Frequency of Medication Administration Regulatory Non-compliance in CCC 2006-2007 and 2016-2017.
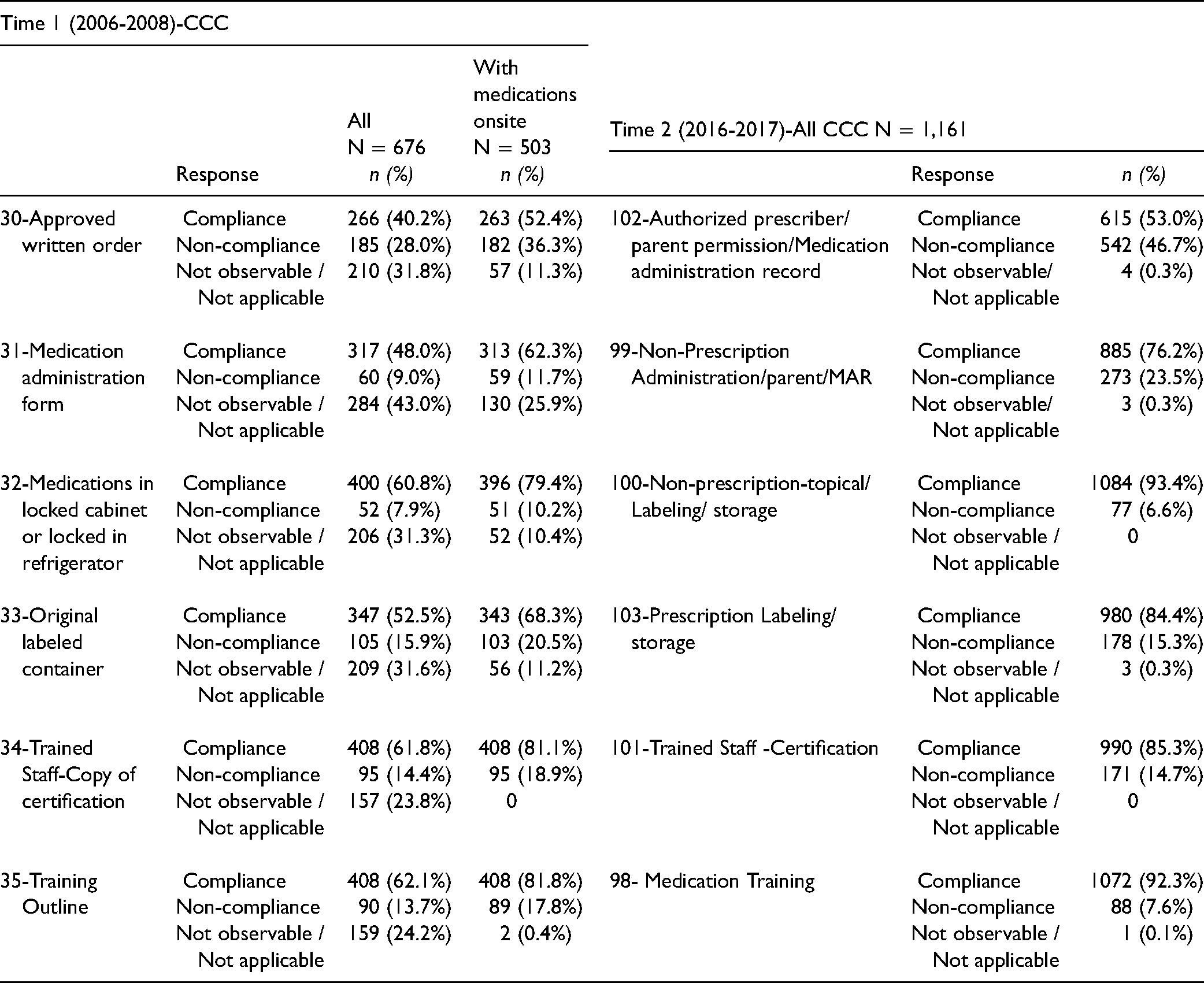
Table 2 shows the proportions of compliance and non-compliance for medication administration regulations for all CCC in Time 1 and 2 and for those CCC with medications on site at the time of inspection in Time 1. In comparing the two time periods of data, Time 1 had a large percentage of “not observable”/“not applicable” results, e.g., item 30 Approved written order 31.8% and item 31.31 Medication Administration form 43%, which must be considered when interpreting compliance and non-compliance for each item. In contrast, the “not observable”/ “not applicable” data were not entered into the Time 2 state data base; thus, we assume that the results, such as, item 102, Authorized prescriber/ parent not observable/ not applicable result 0.3% was a coding error. With this limitation in mind, the CCC inspected in Time 2 had greater proportions of compliance on most regulations compared to the CCC inspected in Time 1. Of note, in Time 1, when CCC with medications on-site were compared with all CCC, which included some without medication on site, all regulation items showed higher rates of regulatory non-compliance, such as, 30 Approved written order: All CCC revealed 28% non-compliance versus CCC with medications on site 36.3% non-compliance. This finding indicates the importance of analyzing those CCC with medication on site.
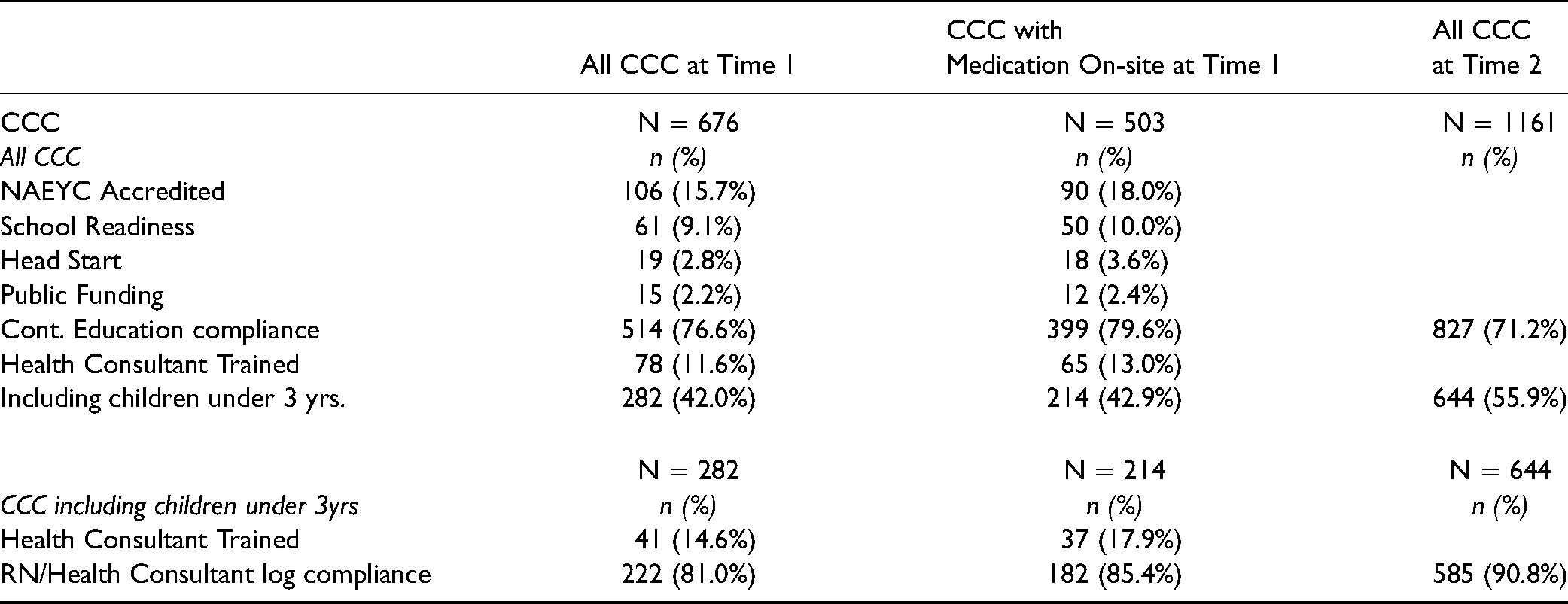
The characteristics of CCC are presented in Table 3. Of the 503 CCC with medications on site and/ or trained staff, 18% were NAEYC accredited and 13% accessed a trained CCHC. Almost half of the CCC included children under 3 years old. The proportions of compliance with continuing education (79.6%) and professional development for child care providers (71.2%) were high in CCC in Time 1 and 2, respectively. New regulations instituted after Time 1 revealed low levels of non-compliance (97 Written policies/ procedures, 3.9%, 105 Self-administration authorized prescriber, parent permission/ MAR 0.34%, 106 Self- admin-labeling and storage 0.09%, 107 Approved petition for self- administration for special med authorization/ emergency distribution of K. Iodide 0.34%, 108. K. Iodide pills- parent permission, storage, expiration date 0.26%), except for 104 Unused/expired meds returned/ disposed 17.3%.
Characteristics of CCC: Time 1 and Time 2.
Before performing LCA, we used the categories of regulations presented in Table 1 and observed the most non-compliance with medication documentation in both time periods (Table 4). Except for medication documentation, which revealed increased non-compliance in Time 2 (58.4%), the proportions of non-compliance were lower in that time period for the other three categories of regulations. With the smallest model fit criteria (AIC = 31.20; BIC = 107.04; cAIC = 121.04; Adjusted BIC = 62.56), LCA identified three latent classes which include Low Non-compliance (Class A), Medication Documentation Non-compliance (Class B), and High Non-compliance (Class C) in Table 5. The probability of non-compliance on the four regulation categories are very low and high in Low and High Non-compliance groups, respectively. Medication Documentation non-compliance had a very high probability of non-compliance with medication documentation only. The Low Non-compliance group included 193 (30.4%) and 429 (36.9%) centers at Time 1 and 2, respectively. High Non-compliance was 11% which is about half of 20% for High Non-compliance at the Time 1. Approximately 42% and 52% of CCC at Time 1 and 2 respectively were in the Medication Documentation non-compliance group.
Frequency of Medication Administration Regulations Category Non-compliance in CCC.

Latent Classes of Medication Administration Non-compliance in CCC with Latent Class Analysis.
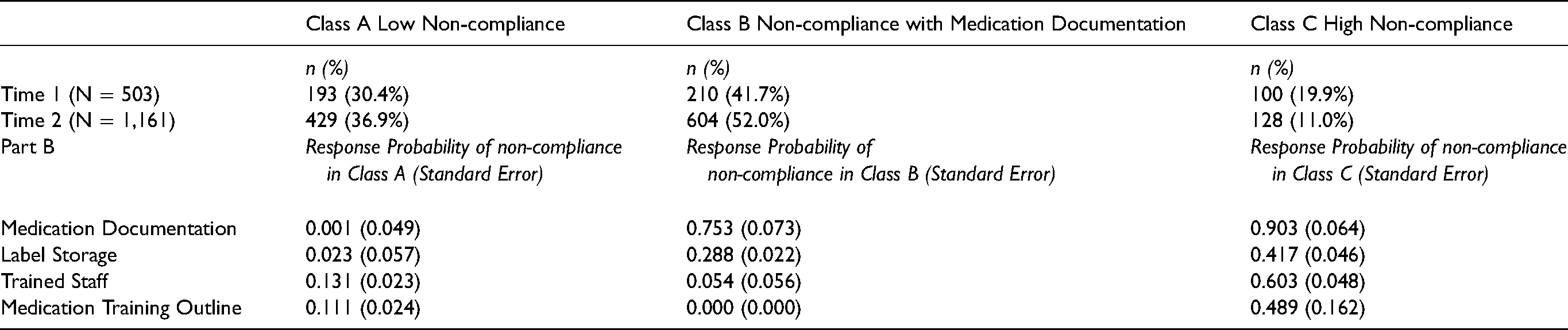
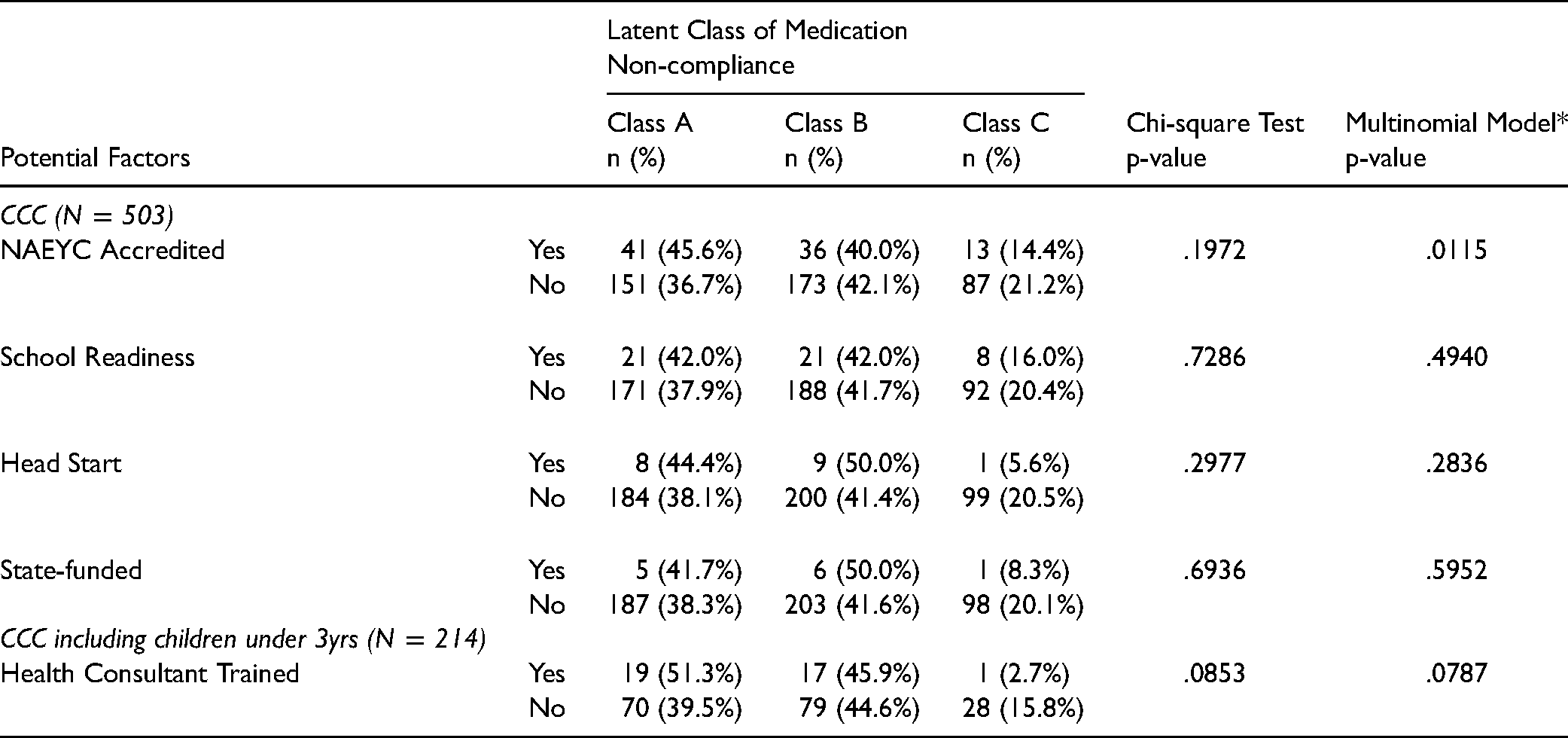
Table 6 shows the proportions of factors which may promote medication administration compliance across the three compliance groups at Time 1. Lower proportions of High Non-compliance in CCC with NAEYC accredited (14.4% vs. 21.2%), school readiness (16.0% vs. 20.4%), Head Start (5% vs. 20.5%), and state-funded (8.3% vs. 20.1%) were observed, but no statistical significance was revealed in Chi-square test, which does not consider the variability of licensing specialists. We found significant random effect variances (1.04 (SE = 0.51) & 2.50 (SE = 1.53) for the Medication Documentation Non-compliance and High Non-compliance, respectively, with p-values ≤ 0.05) explained by licensing specialist. In the multinomial model incorporating the random effect of licensing specialist, NAEYC Accredited was significantly associated with the low Non-compliance Group (p = 0.0115). Among 214 CCC including children under 3 years old, half of CCC with a trained CCHC were classified as Low Non-compliance with medication administration while only 39.5% of CCC which did not have a trained CCHC were in the Low Non-compliance group. This finding reveals that CCHC trained may reduce non-compliance with medication administration, but statistical significance was marginal with a p-value of 0.08.
Frequency of Potential Factors that Promote Medication Administration Compliance in CCC with Medication On-site at Time 1: 2006-2008.
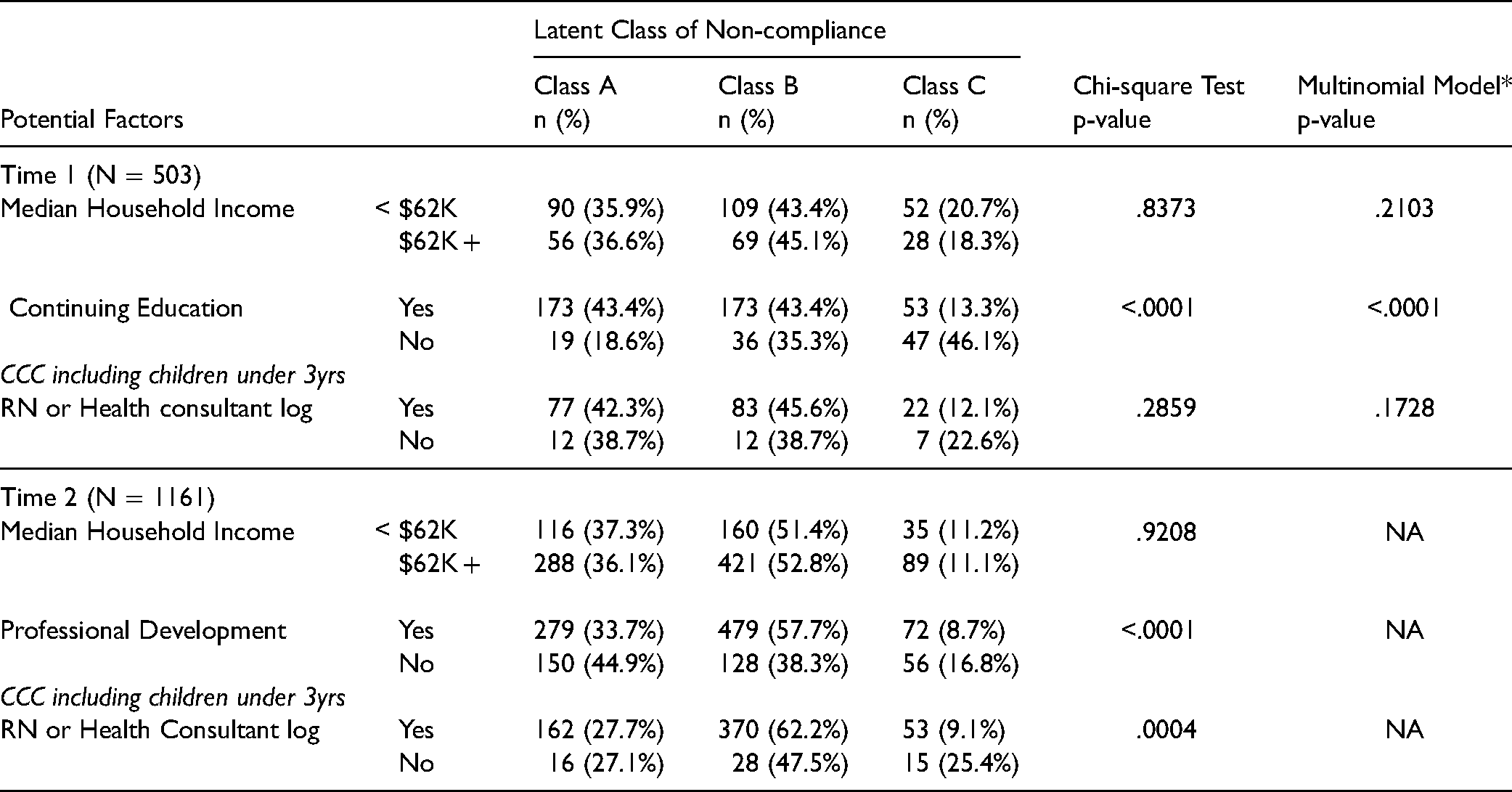
The proportions of other potential factors (median household income and compliance with continuing education/professional development, and RN/health consultant log) across the non-compliance groups at both time periods are presented in Table 7. We dichotomized median household income with <$62,000, which was 25th percentile in the current study. The proportion of the non-compliance groups was not different by the median household income (<$62 K vs. $62K + ) in both time periods. CCC compliant with continuing education/professional development were less likely to be classified as High Non-compliance at Time 1 and 2 (p-values <0.0001). In Time 1, a lower proportion of High Non-compliance was observed in CCC that were compliant with RN/health consultant log (12.1% vs. 22.6%), but it was not statistically significant (p = .2859). However, in Time 2 among 644 CCC including children under 3 years old, those compliant with RN/ health consultant log were less likely to be classified as High Non-compliance (9.1% vs. 25.4%) compared to those not compliant (p = 0.0004).
Frequency of Potential Factors that Promote Medication Administration Compliance in CCC at Time 1 (2006-2008) and Time 2 (2016-2017).
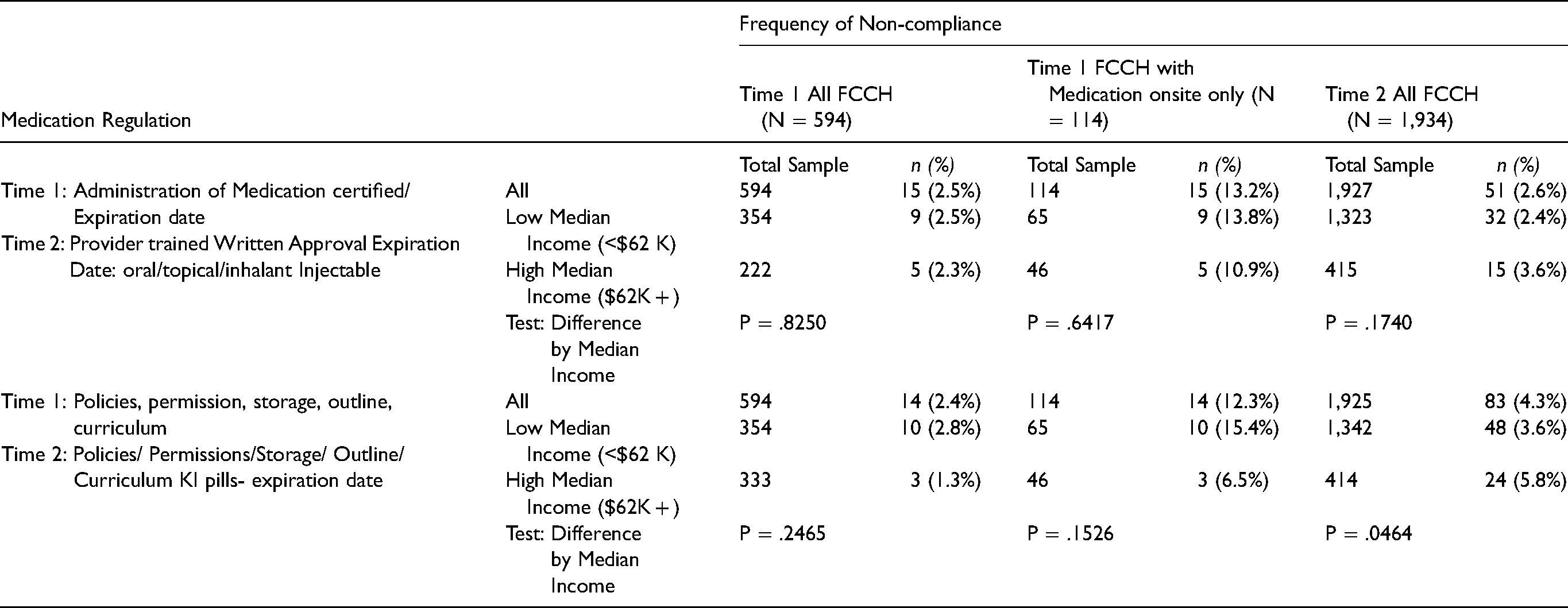
The frequencies of non-compliance with medication administration regulations in FCCH are presented in Table 8. At Time 1, the FCCH inspection form had two variables pertaining to medication administration. One item ascertains whether a child care provider is certified in medication administration and the training expiration date. The second item specifically lists: policies, permissions, storage, outline, and training curriculum. Out of 594 FCCHs, 15 (2.5%) FCCH were non-compliant with certification and 14 (2.4%) FCCH with policies, permissions, storage or training curriculum. Of the 114 FCCHs with medication on site, the proportions of non-compliance increased to 13.2% and 12.3% respectively. Like CCC, analysis of FCCH programs with medications on site, revealed a more precise picture of regulatory non-compliance. Tests for comparing the non-compliance between low (<$62 K) and high (≥$62 K) median household income at each time period are also presented in Table 8. Findings at Time 1 did not show a statistically significant difference between the household income levels and either regulatory item. However, in Time 2, compliance with the regulations pertaining to polices, permissions, storage, outline, curriculum, and KI pills-expiration date were significantly greater in high household income (5.8%) compared to low household income (3.6%).
Non-compliance with Medication Administration Regulations in FCCH by Median Household Income.
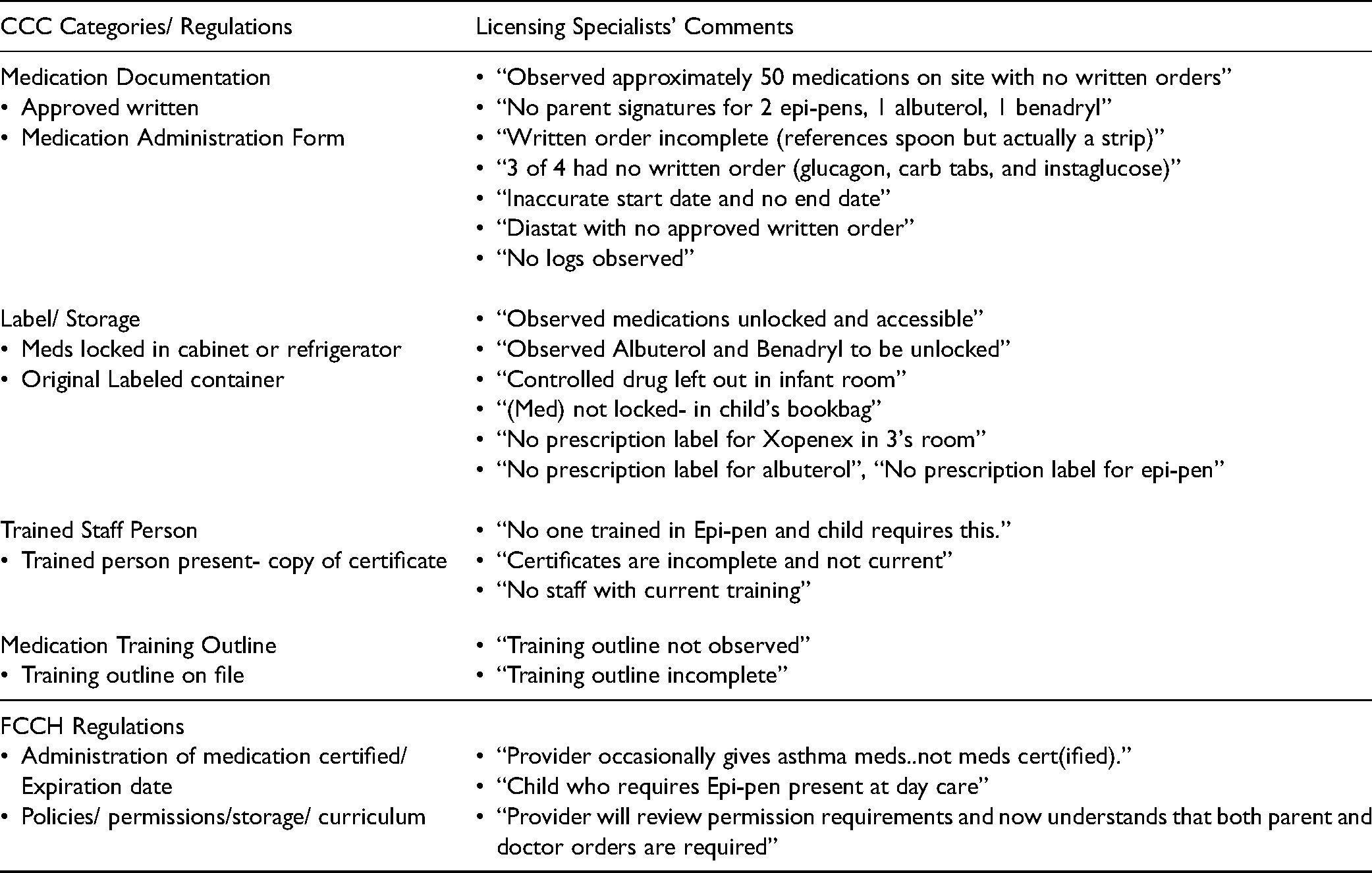
Licensing specialists frequently add comments explaining the cause for non-compliance. In Time 1, 558 comments were included in the 594 CCC inspection reports. Among the CCC reports approximately one-third (32%) addressed written orders, followed by labeled container (18%), training (17%), training outline (16%), medications locked (9%), and medication administration forms (8%). Table 9 lists selected comments illustrative of non-compliance issues.
Selected Licensing Specialists’ Medication Administration Non-Compliance Comments: Time 1: 2006-2008.
Discussion
Medication safety is a critical issue in the community as well as hospitals. Few studies have examined medication errors in child care programs despite the fact that millions of children are enrolled in CCC and FCCH. Many of these children have special health care needs and require daily or emergency medication while in care. In 2014 the Reauthorization of CCDBG, which provides federal guidance for state child care infrastructure and significant child care funding to each state, required for the first time that states include medication administration training among 10 health and safety mandates (ACF, USDHHS, 2016). In addition, states must report serious injuries and deaths occurring at child care programs. Giving parents access to the health and safety status of child care programs in order to make informed choices is an important pillar of the legislation.
This study examined the findings of routine, unannounced licensing specialists’ inspections during two periods of time. Medication administration regulations for CCC were more explicit in Time 2; thus, we created four categories of regulations to compare compliance and non-compliance over time. Three of the categories of regulations, label and storage, trained staff, and medication training outline showed increased compliance over time. However, medication documentation revealed increased non-compliance in Time 2. The purpose of training is to improve safety. While medication storage and handling improved, medication documentation, i.e., correct orders, parent permission and precise recording of medication administration demonstrated an alarming frequency of non-compliance.
Access to other databases in Time 1 allowed us to examine potential factors potentially associated with CCC medication administration compliance. Child care centers which achieved NAEYC accreditation demonstrated greater compliance. We also examined compliance with other child care regulations, specifically requirements for continuing education/ professional development for CCC and a weekly visit by a CCHC, almost all of whom are RNs, for programs that enroll children under three years of age. Compliance with continuing education/ professional development was associated with medication administration compliance in both time periods and highlights the critical importance of training to improve medication administration safety. Interestingly, compliance with a CCHC (RN log) visit was not associated with medication administration compliance in Time 1 although those CCC with a trained CCHC, that is, nurses with formal child care health consultation preparation, were more likely to be compliant with medication administration regulations. However, Time 2 analysis revealed that compliance with a weekly CCHC visit for programs enrolling children under three years of age was associated with medication administration compliance.
Because FCCH regulations were compressed into two items our analysis was limited. Of note, far fewer FCCH providers were administering medications at Time 1 and an unknown number at Time 2. Household income as a proxy for resources was not statistically significant for FCCH in Time 1 but was for regulations pertaining to policies, permissions, storage, and training outline in Time 2. FCCH providers are more likely to care for low-income children many of whom have chronic health conditions requiring medications; thus, providing FCCH providers access to free or low-cost training and CCHC visits is essential.
In 2009, Crowley and Rosenthal published a report of Time 1 findings and recommended: health and safety professional development, information and resources; development of an electronic data system with an annual report of CCC and FCCH licensing inspections, training of licensing specialists to reduce the variability of reporting; and development and dissemination of a best practice medication administration training curriculum as in other states, e.g., New York (Professional Development Program, n.d). Between the two time periods, multiple efforts to improve child care health and safety were instituted including annual inspections of CCC and FCCH, playground improvements, licensing specialists’ training, and an electronic database of licensing specialists’ reports. Through private foundation and federal funding (CHDI, 2015) the Connecticut Medication Administration in Early Care and Education (CMAECE) curriculum in English and Spanish was created and disseminated widely to nurses, many of whom were CCHC and had participated in federally funded national health consultant continuing education between 2002–2013. Since nurse educators are experts in teaching medication administration, faculty at five Connecticut Schools of Nursing were invited to participate in piloting the CMAECE curriculum (Crowley et al., 2015). They also expressed interest in creating a state wide system of medication administration training. The training of nurse consultants and dissemination of a high-quality medication administration training curriculum may explain improvement in medication administration regulatory compliance and the statistically significant effect of CCHCs in Time 2. In 2016 the CT OEC ended the funding of the CMAECE program. Since that time nurses and other designated health care providers may use or create any curriculum that meets regulatory requirements which was the case before and during Time 1; the impact of which is yet to be studied.
A comparison of the two databases deserves attention. The Time 2 data we obtained from the Connecticut Open Data online platform (CT DATA, n.d.) were in several Microsoft Excel files with a tremendous amount of duplicated information. The files could not initially be used to build a relational database. We had to clean the data files and find unique keys in order to link the files to extract the data needed. State data administers should make raw data files available in addition to data report files to facilitate dataset preparation and analysis of compliance with regulations. Furthermore, the database created in Time 1 included all data collected by the licensing specialists including “not observed”/ “not applicable” responses and licensing specialists’ comments. Although similar data were collected in Time 2, not all results were carried over into the database, which limits analysis and could potentially skew results. States are now required to report CCDBG training requirements for continued funding (ACF, 2016). To document the impact of training, databases should include all licensing specialists’ observations and compliance with medication administration regulatory compliance. Policy makers should then disseminate an annual report so that parents can make informed child care choices.
The primary limitation of this study was changes in medication administration regulations after Time 1. As noted, the researchers created categories of regulations to compare findings across the two time periods. In Time 2 because of missing data (“not observed” and “not applicable”) which would identify programs that were administering medications, the researchers were unable to compare regulatory compliance and non-compliance of programs administering medications over the two time periods. The two time periods offered some comparison of trends in medication administration regulatory compliance. Ideally, the state should analyze licensing specialists’ reports and disseminate findings annually.
This is the first published study that found a statistically significant association between nurse CCHC visits and compliance with medication administration regulations. CFOC (AAP et al., 2019) recommends that all child care programs engage a CCHC, a licensed health professional preferably with preparation in consultation, to promote the health and development of children, families and staff. The CCHC provides a range of activities including observing the safety of the indoor and outdoor environment and health practices, monitoring children's health and development, supporting staff health, and teaching and monitoring medication administration and safety. Like Connecticut, some other states have a regulatory requirement for CCHC visits to child care programs (Honigfeld et al., 2017). However, state systems for such infrastructure varies. Despite decades of mandating CCHC visits, Connecticut has no system of training, organizing, and supporting health consultants and child care providers who are required to seek their services. In contrast, other states, e.g., North Carolina, which does not have a regulatory requirement for visits, has a robust system of health consultation to child care programs (NC Child Care Health and Safety Resource Center, 2021). A growing body of literature (Crowley, 2000; Isbell et al., 2013; Johnston et al., 2017) demonstrates that nurses, especially those who are formally prepared for the CCHC role, play an important role in children's health and safety in child care programs.
The COVID-19 pandemic highlighted the critical role of child care as an essential service in the U.S. Child care providers are underpaid, and most parents bear the burden of costs (Child Care Aware of America, 2021). Language and funding in the proposed Build Back Better Act of 2021 suggests the desire and intent of national leaders to improve access to a high quality child care system for families (Congress.Gov, 2021). Healthy and safe care is the foundation of quality child care. The CCDBG requirement that providers show evidence of medication administration training is only a first step. A high-quality training curriculum and frequent visits to both CCC and FCCH by nurse CCHC, who are prepared for the role, are essential to ensure inclusion of all children and safe medication practices in child care programs. Nurse educators and policy makers should lead efforts to shape safe medication practices in child care at the state and national levels.
Footnotes
Acknowledgments
We acknowledge with gratitude support for this research from The Children's Fund of Connecticut and The Child Health and Development Institute of Connecticut, Inc. and our colleague, research partner and friend, Marjorie Rosenthal, MD, MPH (1967–2020), who contributed to this work and was a tireless advocate for children and families.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The Children’s Fund of Connecticut and The Child Health and Development Institute of Connecticut, Inc granted permission to use portions of an earlier report for this article.
Funding
The author(s) disclosed receipt of the following financial support for the research of this article: This work was supported by The Children’s Fund of Connecticut and The Child Health and Development Institute of Connecticut, Inc.