
Abstract
Uptake of the COVID-19 vaccine by nurses lags behind that of other health care professionals with minimal empirical evidence to understand this phenomenon. In this secondary analysis, we examined nurses’ individual and work-related characteristics and their association with COVID-19 vaccination status. Alumni of three Ohio nursing colleges and members of a professional organization were invited to complete questionnaires from June through August 2021. Logistic regression models were used to evaluate associations between nurse characteristics and vaccination status. Among 844 respondents, 754 (80.30%) had received at least one dose of the vaccine. Older age, having a bachelor's degree or higher, and working in critical care were associated with vaccination. Providing direct care for COVID-19 patients in the last 7 days and a higher perception of one's work being affected by COVID-19 were significantly associated with being vaccinated, whereas prior COVID-19 infection was inversely associated with vaccination status. Our findings suggest that COVID-19 vaccine uptake among nurses is influenced by a host of factors related to virus knowledge, beliefs, and risk perceptions. Awareness of these factors can aid the development of interventions to increase nurses’ acceptance of vaccines.
Introduction
Since the discovery of the first COVID-19 case in December 2019, the SARS-CoV-2 virus has infected more than 91 million people and caused over one million deaths in the United States (Ritchie et al., 2022). In December 2020, a nurse in New York City became the first non-research recipient of the COVID-19 vaccine in the U.S. while the world watched with hope and anticipation for the end of the pandemic (Inskeep & Mann, 2020). Vaccines enable societies and individuals to prosper and prolong life expectancy against infectious diseases that previously killed and disabled a large portion of the population (Piot et al., 2019). However, despite the societal and individual benefits from vaccines on human health in the last century, vaccine hesitancy persists and is considered a global public health threat (WHO, 2019).
Healthcare professionals, particularly nurses, are an important target group for vaccination due to their proximity to patients and critical role in preventing healthcare-acquired infections (Poland & Tucker, 2012). Healthcare professionals generally have higher vaccine uptake than the public. Yet, nurses consistently have the lowest vaccination intent and lowest vaccination rates among healthcare professionals (Lee et al., 2021; Wang et al., 2021). For example, the influenza vaccination rate among nurses during the 2018–19 influenza season was 90.2% compared to physicians at 98% (CDC, 2020). In August 2021 (when our survey was conducted), around 75–88% of nurses in the United States had received COVID-19 vaccines or were planned to receive them compared to 96% of physicians (American Medical Association [AMA], 2021; American Nurses Association [ANA], 2021). This lower uptake is concerning, as nurses for 20 years straight have been rated as one of the most trusted professions in the United States (Gallup, 2020) and have a significant formal and informal influence on the healthcare decisions of patients, families, and the public at large (Larson et al., 2014; Wiley et al., 2013). A nurse's decision to decline the COVID-19 vaccine can potentially affect the public perception of vaccine safety and the safety of patients and communities that the workforce serves (Wendelboe et al., 2015).
Research on COVID-19 vaccination among healthcare professionals provides an emerging view of factors influencing hesitancy, such as concerns about vaccine effectiveness, safety, side effects, and efficacy; misinformation and lack of knowledge; and distrust of the government (Khubchandani et al., 2022; Li et al., 2021). However, little is known about factors that specifically influence nurse COVID-19 vaccination, and this impedes the development of effective interventions to address vaccine hesitancy in a high-risk, high-influence occupational group. Therefore, the purpose of this study was to examine the demographic and professional characteristics of Ohio nurses and their relationship to COVID-19 vaccination.
Study Data and Methods
We conducted a secondary analysis of survey data collected from a larger study of nurses’ moral injury, resilience, and wellbeing during the COVID-19 pandemic (Fitzpatrick et al., 2022). Only the items relevant to the current study are included in this analysis.
Setting and Sample
Data were collected for ten weeks from June to August 2021 using an electronic self-administered survey distributed through QualtricsXM software. To be eligible for the study, nurses had to be engaged in clinical practice either full-time, part-time or per diem in any practice setting in the state of Ohio. Nurses were recruited via the nursing alumni listservs from three large universities located in Ohio and the advertisement on a professional organization document. No incentives were offered.
Measures
The survey included questions regarding individual demographics, work characteristics, COVID-19 vaccination status, and experiences with COVID-19.
Demographic characteristics
Demographics included both individual (age, gender, race) and professional (years of nursing experience, nursing degree, nursing role, employment status) characteristics. Items for work characteristics included the organizational types (e.g., hospital, long-term care facility, etc.) and nursing unit type (e.g., critical care unit, emergency rooms, ambulatory offices, etc.). The geographic locations of nurses’ primary practice were assessed as urban, suburban, or rural settings. The zip codes of the nurses’ primary clinical practice were also collected and then aggregated into five regions (Northeast, Northwest, Central, Southeast, and Southwest) in Ohio, following the map used by the state of Ohio Map (State of Ohio, 2022). All regions except Southeast included large metropolitan cities (Northwest–Cleveland, Northeast–Toledo, Central–Columbus, and Southwest–Cincinnati).
COVID-19 experiences
We included three COVID-19 related questions assessing the participants’ own experiences. The first question asked the participants to rate how much COVID-19 affected their clinical practice on a 10-point Likert scale ranging from “not at all” as 1 to “Extremely” as 10. The second question asked if participants had provided direct care to patients with COVID-19 in the last seven days, and the third question inquired if they had ever tested positive for the COVID-19 virus. These two latter question responses were recorded as either “No” or “Yes.”
COVID-19 vaccination status
The outcome of interest in this study was self-reported COVID-19 vaccination status, which was coded either as 0 “unvaccinated” if they had not received any dose of vaccine or 1 “vaccinated” if they reported having received at least one dose of any available COVID-19 vaccine.
Statistical Analysis
Frequencies and means were calculated to describe individual and work characteristics, COVID-19 experiences, and COVID-19 vaccination status. We performed a univariate analysis of each variable used to describe the sample, including its central tendency (mean and median) and distribution (range, variance, and standard deviation). Multivariate logistic regression models were used to examine associations between nurse characteristics and COVID-19 vaccination status. To determine factors associated with vaccination status, we present results as odds ratio (OR) with 95% confidence interval (CI) and set alpha at p < .05. Assessments of multicollinearity revealed that age and years of experience were highly correlated. Therefore, only age is included in the analysis. Other variables such as direct care to patients with COVID-19 in the last 7 days and the types of nursing units were also tested for multicollinearity using Spearman correlation and found to be independent of one another. Due to the racial homogeneity of the sample (majority white with few respondents from additional racial and ethnic backgrounds), we dichotomized race to white and non-white. Statistical analysis was performed using STATA 16.1 (StataCorp. 2019. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC.).
Ethical Considerations
Participation in the study was voluntary. Informed consent was obtained online when the invited nurse clicked on the “I agree” button to proceed with the survey. To preserve anonymity, the IP addresses of the computers used for the survey were not tracked, and the participants’ specific information on work settings, such as the name of their employers, were not collected. This study was reviewed and approved by the Institutional Review Board of Case Western Reserve University.
Results
There were 1,857 initial responses. After deleting cases with some missing responses, complete data from 844 respondents comprised the analytic sample. We were unable to calculate an overall response rate as the duplicate number of nurses who were on both listservs could not be obtained from the listserv owners. Additionally, the total number of nurses meeting the eligibility criteria was unavailable.
Sample Characteristics
Table 1 summarizes the individual and work characteristics of the participants, with some comparative data for all Ohio nurses. Most respondents self-identified as white (90.4%) and female (92.2%), with a median age of 44 years and a median of 12 years of nursing experience. Respondents most frequently reported holding a bachelor's degree in nursing (48.7%), followed by an associate degree or diploma (31.6%). Most respondents held a full-time permanent position (77.0%), while about 5% were in contract or travel positions. For the work characteristics, almost half of the nurses (48.9%) practiced in urban areas and most commonly worked in hospitals (62.2%). Nurses worked in various types of nursing units, including stepdown/med/surg units (22.5%), critical care (17.7%), emergency rooms/ambulatory offices (18.7%), or rehab/long-term care (15.3%). Approximately 81% of respondents (n = 680) had received at least one dose of the vaccine at the time of the survey.
Participant Characteristics (N = 844).
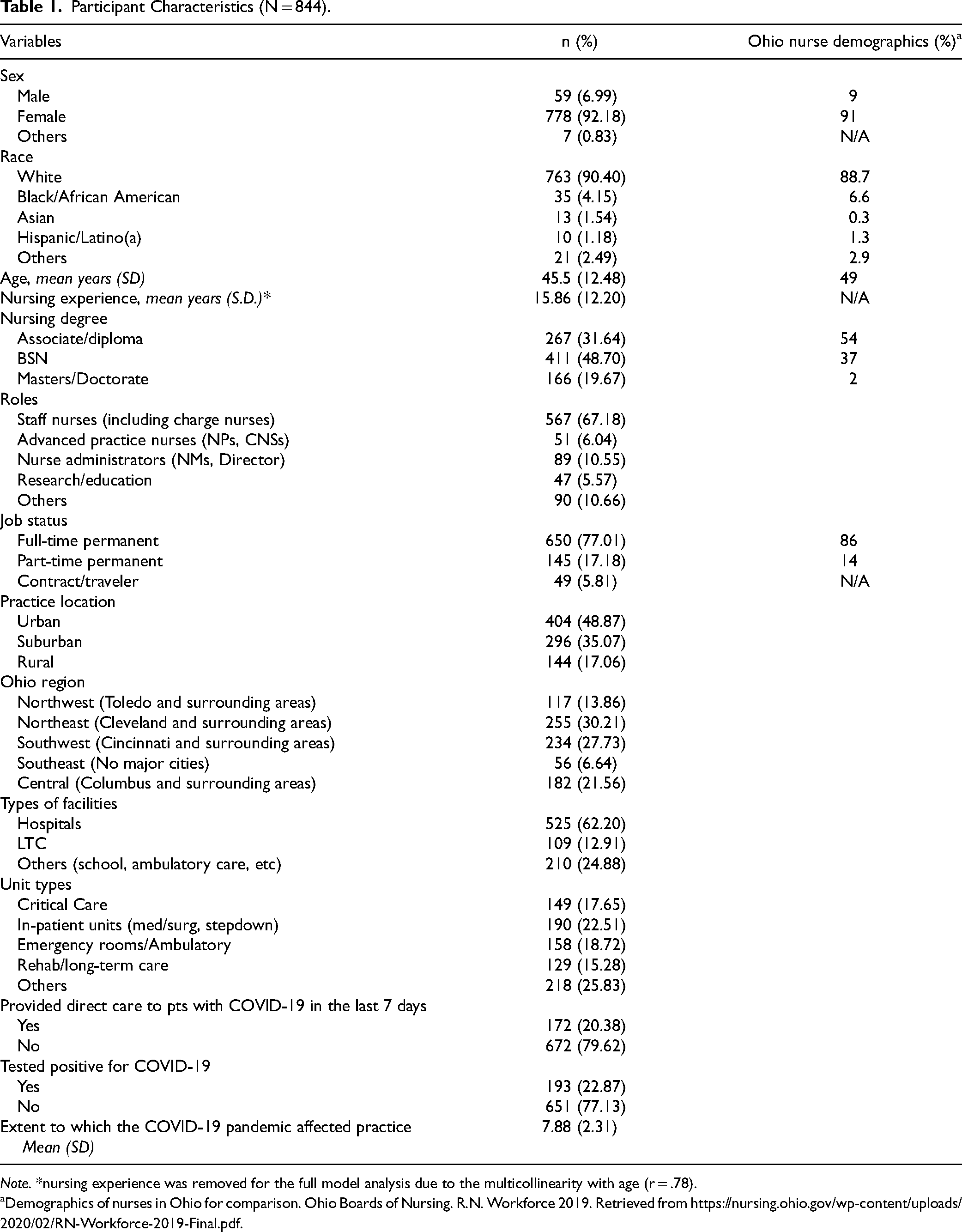
Note. *nursing experience was removed for the full model analysis due to the multicollinearity with age (r = .78).
Demographics of nurses in Ohio for comparison. Ohio Boards of Nursing. R.N. Workforce 2019. Retrieved from https://nursing.ohio.gov/wp-content/uploads/2020/02/RN-Workforce-2019-Final.pdf.
COVID-19 Experiences
Approximately one in four nurse respondents (22.9%) reported they had previously tested positive for COVID-19, and one in five nurses (20.4%) cared for patients with COVID-19 in the seven days prior to completing the survey. Nurses indicated that the COVID-19 pandemic greatly affected their clinical practices, with a mean score of 7.88 (SD 2.31) out of 10.
Characteristics Associated with COVID-19 Vaccination status
Several individual and work characteristics were significantly associated with vaccination status in the fully adjusted model (Table 2). For individual characteristics, each additional year of age was associated with a 4% increase in odds of being vaccinated (OR 1.04, 95% CI 1.02- 1.05). Further, compared to nurses with an associate degree or diploma, respondents with a bachelor's degree had twice the odds of being vaccinated (OR 2.14, 95% CI 1.39–3.28), and those with a master's or doctorate degree were 97% more likely to be vaccinated (OR 1.97, 95% CI 1.14–3.48) at the time of the survey. There were no significant differences in vaccination status according to respondent sex or race.
Characteristics Associated with Vaccine Uptake (N = 844).
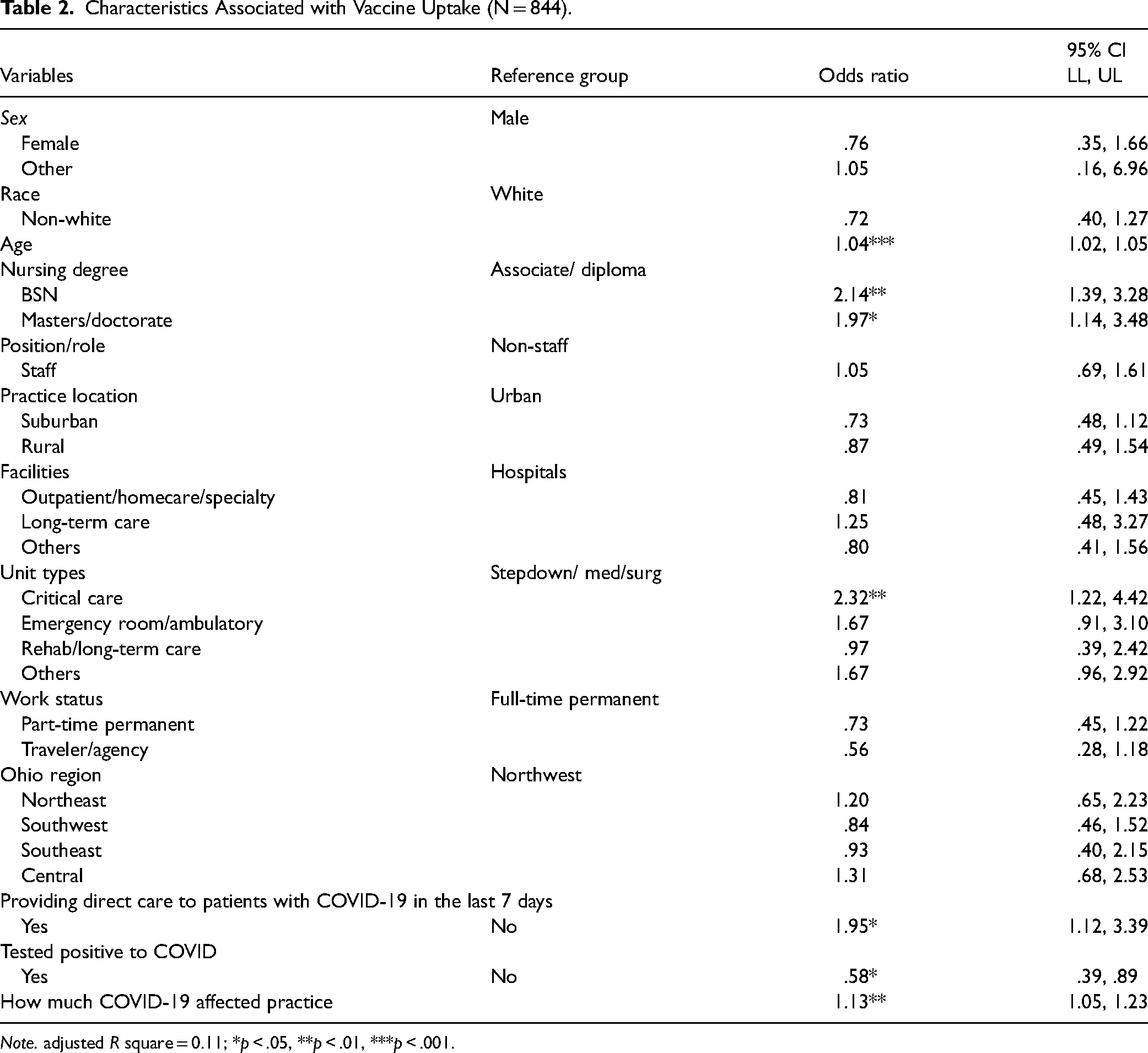
Note. adjusted R square = 0.11; *p < .05, **p < .01, ***p < .001.
Participants working in critical care units had significantly greater odds of being vaccinated (OR 2.33, 95% CI 1.22–4.42) compared to those working in stepdown/med/surg units. Other work characteristics such as nursing role, job status, or geographic location were not associated with vaccination status. Nurses who reported providing direct care to COVID-19 patients in the last seven days were almost twice as likely to have received a COVID-19 vaccine (OR 1.95, 95% CI 1.12–3.39). Lastly, for each point increase in nurses’ perception that COVID-19 affected their clinical practice, the odds of nurses being vaccinated increased 13% (OR 1.13; 95% CI 1.05–1.23). Respondents who reported previously testing positive for COVID-19 were 40% less likely to be vaccinated at the time of the survey (OR 0.59, 95% CI 0.39–0.89).
Discussion
The COVID-19 vaccination rate among Ohio nurses in this study (80.56%) was similar to the U.S. national vaccination rates of nurses in other studies (Lee et al., 2021; Moniz et al., 2021). An American Nurses Association survey conducted in July 2021 revealed that 83% of nurses in Ohio had already received or planned to receive the COVID-19 vaccine. The data for our study were collected between June and August 2021, when almost all nurses (and healthcare workers) were eligible for the vaccine. However, organizational or government mandates were not in place until later, with the U.S. federal emergency mandate issued in November 2021 (CMS, 2021). Therefore, our findings highlight that most nurses chose to be vaccinated voluntarily. Nevertheless, we identified several demographic and work-related characteristics associated with COVID-19 vaccination status in this sample of Ohio nurses, including older age, higher levels of formal nursing education, working in a critical care setting, a recent experience providing direct patient care for COVID-19 patients, and a perception that the pandemic had significantly affected their clinical practice. We also found a significant negative association between prior reported COVID-19 infection and vaccination status.
Our finding that age, education, and the type of nursing unit were associated with nurses’ vaccination status is consistent with results from other studies (Dubov et al., 2021; Fakonti et al., 2021; Paris et al., 2021; Wang et al., 2020). Of these characteristics, age was the only non-modifiable characteristic. In general, older adults are at a greater risk for negative consequences of the SARS-CoV-2 virus. Age has been consistently associated with one's vaccine uptake across the general public and healthcare professionals alike (Alshurman et al., 2021; Dubov et al., 2021; Fakonti et al., 2021). This trend may be due, in part, to public health messaging and policies prioritizing older individuals with earlier vaccine eligibility and outreach, thus increasing their awareness and self-perception of heightened risk compared to younger individuals.
The other individual characteristics—education and type of nursing unit—are modifiable factors associated with nurses’ vaccination status. Education has been consistently associated with vaccination preference and status among the general public (Joshi et al., 2021), and nurses (Kwok et al., 2021; Li et al., 2021). In our study, those with bachelor's or more advanced degrees in nursing were more likely to be vaccinated compared to those with an associate degree or diploma. We could not locate another study that examined differences in vaccination rates among nurses by types of nursing degrees. However, evidence linking educational preparedness and patient care quality and safety is increasing (Liao et al., 2016), pointing to the educational gap between different entry degrees in nursing (Djukic et al., 2015). The variation in vaccination rates by education in nursing may be due to differences in the depth of the coursework offered at bachelor's or more advanced degree programs compared to associate degree or diploma programs. Nonetheless, the inadequate inclusion of immunization policies and infectious disease exposure in nursing education was identified as early as three decades ago (Goetz et al., 1992), highlighting the need to revisit today's nursing curriculum in associate degree and baccalaureate nursing programs to ensure adequate educational preparedness of nurses.
It is also possible that education and unit type indirectly influence vaccination status; these characteristics may be proxy indicators for one's knowledge and perceptions of the virus and/or vaccines. Existing literature demonstrates that strong predictors for COVID-19 vaccine choice were the perception of disease severity, self-perceived risks, knowledge about the virus, and information about the vaccine (Biswas et al., 2021; Dini et al., 2018; Dubov et al., 2021). For example, in a survey of nursing students and COVID-19 vaccination status, those rated higher on their perceived knowledge of the virus and the vaccines were more likely to be vaccinated (Patelarou et al., 2021). In our study, nurses were more likely to be vaccinated when they had provided direct care to patients with COVID-19 in the previous 7 days and/or perceived COVID-19 as having a great influence on their practice. Critical care units are where seriously ill patients receive more intensive monitoring and advanced life support. Therefore, nurses working in critical care units witness more long-term negative consequences of COVID-19, including deaths. These first-hand experiences are most likely associated with their perceived risks, thus contributing to the higher vaccination rate. The findings of our study and the previous literature are aligned with the Health Belief Model, a theoretical model used to guide health promotion and disease prevention programs (Champion & Skinner, 2008). According to the Health Belief Model, one's desire to avoid illness and the belief that a certain specific health-related action will prevent illness are the two foundational components of one's health-related behaviors (Champion & Skinner, 2008). Thus, the ultimate course of action often depends on one's perceptions of the threats of illness and the benefits of and barriers to health behaviors, while socioeconomic and demographic factors modify these perceptions (Champion & Skinner, 2008).
Interestingly, prior COVID-19 infection was inversely associated with vaccination status. This relationship could be a result of policies requiring a waiting period after infection before becoming eligible for the vaccine. Alternately, nurses with prior infection may hold a belief that natural immunity to the virus reduces or eliminates the need for a vaccine and/or that infection carries fewer individual risks than vaccination. Subjective perception of risk involves complex nuances of individual risk toleration, beliefs, experiences, and health behavior (Joshi et al., 2021; Rhudy et al., 2010). Therefore, the dichotomous grouping of “anti” or “pro” vaccine may not be adequate or accurate in capturing nurses’ perception and/or knowledge of the COVID-19 vaccine. In a recent study of healthcare professionals and their vaccination intention (Dubov et al., 2021), unvaccinated healthcare professionals were categorized into one of four groups: misinformed, undecided, uninformed, or unconcerned. Of these, all except the misinformed group indicated that they were open to changing their decision on vaccination if given relevant information and guidance (Dubov et al., 2021).
Our findings hold important implications for organizations, education, research and public policy. Even before the COVID-19 pandemic, vaccine mandates for nurses were a challenging topic even as contagious viral respiratory infections like influenza impose significant healthcare and socioeconomic burdens worldwide (Dini et al., 2018; Josephson et al., 2021). The Advisory Committee on Immunization Practices has recommended influenza vaccinations for healthcare workers to protect patients and reduce staff illness and absenteeism since 1984 (CDC, 1997). Yet no consensus has been achieved, and instead, the discourse on this topic has increased. A meta-review of systematic reviews investigating interventions for improving vaccine uptake among healthcare workers found that implementing mandatory condition of service policies resulted in sustained vaccination rates up to 95%, with a small number of requests for medical and religious exemptions, terminations and voluntary resignations (Dini et al., 2018).
However, the COVID-19 vaccine mandate for work is not simple and requires ongoing discussions centered on professional, ethical, and legal responsibilities to protect the public while respecting the individual nurse's rights and choice (Dumyati et al., 2021). Strategies for improving vaccine uptake constitute changes in behavior and social-professional norms, which require time and deliberate efforts underpinned by rigorous scientific evidence. Previous studies showed that perceived self-risk and desire for self-protection and protection of family and friends were the main determinants for vaccine uptake rather than absolute disease risk or protection for patients (Rhudy et al., 2010; Vasilevska et al., 2014). These discussions have been challenging as the COVID-19 vaccine became politicized in the United States. For example, areas with a higher percentage of Republican voters had lower vaccination rates and higher COVID-19 cases and deaths per 100,000 residents (Kates et al., 2021). Thus, overcoming political division and rebuilding trust in science and each other through safe and open dialogue with those unvaccinated without shaming must be incorporated in building combined strategies of mandatory vaccine policies, educational materials and training sessions, improved access to the vaccine, organized efforts to raise awareness, and/or the use of advocacy (Corace et al., 2016; Rashid et al., 2016).
Our study also has several implications for research. Most health systems and professional organizations strongly encouraged vaccination even before federal or state mandates were in place. Nonetheless, many voiced increased concerns that the mandate would exacerbate the already severe nursing shortage due to nurses exiting their jobs and/or profession (Lopez et al., 2021). Since then, short-term employment trends have shown that some healthcare systems retained their nurses (Muoio, 2022) while others, such as skilled nursing facilities, experienced worsening of nursing staff shortage (Ochieng et al., 2022). The changes in nursing retention may not be related to the vaccine mandate, as our findings showed that the vast majority of nurses chose to be vaccinated without a mandate. However, continuing research is needed to the long-term effects of the vaccine mandate, if any, on the economic (e.g., nursing workforce recruitment and retention) and psychological (e.g., burnout) impacts.
Limitations
Our study has limitations. First, the cross-sectional nature of the data only provides a snapshot of respondents’ COVID-19 vaccination status at one point in time. The data were collected when a waiting period was required for those who tested positive for COVID-19. Thus, the interpretation of COVID-19 vaccination status warrants caution as the number of vaccinated personnel have increased since the collection of our data. Additionally, the cross-sectional nature of our study may not capture the changing dynamics of COVID-19 vaccine development and implementation. The data were collected from one state with slower COVID-19 vaccine uptake at around 55% compared to the national average of 61.1% (Ritchie et al., 2022), and we are unable to calculate a survey response rate due to listserv limitations. Thus, our findings may not be generalizable. Nurses affiliated with a state nursing organization and alumni of nursing schools in Ohio were invited, and their participation in the survey was voluntary, making it subject to selection bias. Those who were not active in state associations and/or their school alumni groups may have been omitted in the study. Lastly, we may have omitted other potentially impactful characteristics from our study, such as psychological attributes including confidence, complacency, and collective responsibility (Leung et al., 2022), knowledge of or attitudes towards the COVID-19 vaccine (Barry et al., 2021), or the degree of trust in government (Patelarou et al., 2021). We also did not collect data on socioeconomic background, which could confound a relationship between educational degree and vaccination status. Nonetheless, our findings indicate several characteristics that can identify sub-groups of nurses at risk for low vaccine uptake and potential areas of intervention to increase vaccination rates among nurses.
Conclusion
The lessons learned from vaccination during past epidemics and the current COVID-19 pandemic have taught us that vaccine uptake among nurses is a multi-factorial, complex phenomenon. The majority of nurses in our study had already received at least one dose of a COVID-19 vaccine before any COVID-19 vaccine mandate was introduced. Age, education, and the type of nursing unit were also found to be associated with nurses’ vaccination status, whereas prior COVID-19 infection was inversely associated with the vaccine status. Balancing nurses’ individual rights to bodily autonomy with professional responsibilities to protect patients is a dynamic process that requires ongoing dialog and the development of evidence-informed policies. Improving vaccine uptake requires time and deliberate efforts in behavior and social-professional norms changes. In particular, nursing education as a modifiable characteristic associated with nurses’ voluntary COVID-19 vaccination decision highlights an opportunity for further examination and potential intervention in entry-level nursing curricula to address vaccine hesitancy in the profession.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: GP is funded by the National Center for the Advancing Translational Sciences, grant number: KL2TR002547.