
Abstract
Missed nursing care is a multifaceted patient safety issue receiving increased attention among healthcare scholars worldwide. There is limited research on missed nursing care in the Jordanian healthcare context. The current study sought to examine the perceptions of Jordanian nurses toward the amount and types of missed nursing care in medical and surgical wards. We also examined the differences in missed care items between public, private, and university hospitals in Jordan. This was a cross-sectional study using the MISSCARE Survey tool. Data collection spanned 4 months between March and July 2021. The final study sample consisted of 672 registered nurses employed in five public, three private, and two university hospitals in Jordan. Data were analyzed using descriptive statistics, Analysis of variance, and Pearson correlation coefficent test. Of the 672 registered nurses who participated, the majority were females (n = 421; 62.6%). Most participants held a bachelor's degree in nursing (n = 577; 85.9%). The three most common missed nursing activities in the participating hospitals were: ambulation, oral care, and emotional support. Nurses working in public hospitals reported the highest missed nursing care. The age and number of patients under care significantly correlated with missed nursing care. The findings could help nursing managers develop plans to reduce missed nursing care in their healthcare institutions.
Introduction
Missed nursing care (MNC) is a significant, well-documented, and multidimensional global healthcare delivery problem (Halvorsen et al., 2021; Kalánková et al., 2019; Peterson et al., 2021; Schubert et al., 2021). MNC can be defined as leaving nursing care undone, either partially or totally, or significantly delaying it (Kalisch et al., 2009; Lucero et al., 2010). It is a prevalent issue that is considered an error of omission (Jones et al., 2021; Nicholson, 2021). A systematic review of the literature found that 55%–98% of nurses miss at least one task during their shifts (Jones et al., 2015). MNC has several names in the literature including omitted care, unfinished nursing care, care left undone, unmet patient needs, and implicit rationing of nursing care (Bryant & Yoder, 2021; Gurková et al., 2021; Lucero et al., 2009; Peterson et al., 2021; Saar et al., 2021; Zhao et al., 2020). Despite its prevalence, instances of MNC are not always recognized, and they are often underestimated (Kalisch, 2009; Pereira et al., 2020). MNC represents one of the key challenges of healthcare institutions worldwide (Soares Paiv et al., 2021). MNC has a well-documented association with patient safety and nursing care quality (Peterson et al., 2021). It is also related to negative outcomes for hospitalized patients, such as patient falls (Kalisch et al., 2012), medication errors, pressure ulcers (Recio-Saucedo et al., 2018), nosocomial infections (Schubert et al., 2008), poor experience of patient care (Carthon et al., 2015), or even patient death (Ball et al., 2018). Furthermore, MNC may hurt nurses’ job satisfaction (Al-Faouri et al., 2021). Thus, the healthcare literature has recently demonstrated a substantial and enduring interest in investigating the phenomenon of MNC (Chiappinotto et al., 2021).
The influential qualitative study about MNC conducted by Kalisch (2006) found that commonly missed care items in medical and surgical wards comprise ambulation, turning, delayed or missed feeding, emotional support, and hygiene. Subsequently, several studies were conducted worldwide to examine MNC in various healthcare contexts (Blackman et al., 2018). These studies show significant consensus in the types of MNC as perceived by nurses (Kalisch et al., 2009). Evidence demonstrates that MNC was mainly related to areas of basic care, such as ambulation, turning, and mouthcare (Winsett et al., 2016). In a recent study in Italy exploring MNC in medical and surgical wards, oral care was the most frequently missed care element (Bagnasco et al., 2020). A recent study of MNC in the Malaysian context found that attending interdisciplinary conferences, teaching patients, and ambulation as the most frequently reported MNC (Nahasaram et al., 2021). Saqer and AbuAlRub (2018) and Al-Faouri et al. (2021) found that ambulation, feeding patients on time, oral care, and attending interdisciplinary conferences were among the most frequently missed care items as perceived by Jordanian nurses.
Previous research found a higher frequency of MNC in medical and surgical wards compared to other units (Bragadóttir et al., 2017). The care provided to patients in medical/surgical wards is of considerable significance to achieving positive patient healthcare results (Mizuno et al., 2005). One study found that a 10% increase in the frequency of MNC incidents in medical and surgical wards is associated with a 16% increased risk of death after surgery (Ball et al., 2018). Medical/surgical units require nurses to have extensive knowledge and skills and to deal with a vast amount of data. In addition, medical/surgical nurses deal with patients with multiple morbidities (Winsett et al., 2016).
Jordan, officially the Hashemite Kingdom of Jordan, is a country located in the Middle East with an area of 89,000 km and a population of 9,814,995 (Department of Statistics, 2015). The health care system in Jordan comprises public, private, university-affiliated, and military healthcare providers (Mrayyan et al., 2021). The public sector is the largest health care provider in Jordan (Al Maaitah et al., 2019). According to the Jordanian Ministry of Health (MOH), there were 110 public and private hospitals in Jordan with 13,731 beds in 2017. There are also two university hospitals in Jordan with 1,233 beds (Al Maaitah et al., 2019). The public sector represents the preferable place to work by Jordanian nurses due to job security (Mrayyan et al., 2021). The High Health Council (HHC) is committed to developing and endorsing national health policies and strategies. On the other hand, the MOH is mandated to oversee, observe, and endorse laws at the national level (Al Maaitah et al., 2019).
About 70% of Jordanians and 55% of the Kingdom's population are insured. However, there is considerable geographical variation in the proportion of the population with healthcare insurance. About 80% of insured Jordanians are insured with the public sector, while the rest are covered through private insurance, and other sources. In Jordan, direct out-of-pocket health expenditure represents about 25% of total healthcare spending, which is considered high for a middle-income country (Nazer & Tuffaha, 2017).
Despite the increasing emphasis on investigating the phenomenon of MNC worldwide (Halvorsen et al., 2021), little is known about MNC in the Jordanian healthcare context. Moreover, there is little research into the impact of the COVID-19 pandemic in Jordan. As far as we know, no studies have focused on nurses’ perceptions of MNC in medical and surgical units. Accordingly, this would appear to be an important issue to investigate, given the acute nursing shortage globally and in Jordan (Amarneh et al., 2021). In this context, it is important to mention that the high turnover rate of nurses is an ongoing issue in the Jordanian healthcare system and is regarded as the main reason for the nurse shortage (Rawashdeh & Tamimi, 2019). Meanwhile, there is also an increased demand on the healthcare system in Jordan (Al-Hamdan et al., 2017). In fact, Jordan is encountering challenges as a result of an increasing population that is anticipated to double by 2030, a surge in non-communicable diseases (NCDs), and the present human resource for health (HRH) challenges including retention and continuous training (High Health Council, 2020). According to Hayajneh et al. (2010), the main cause of inadequate staffing in Jordanian hospitals is the cost-saving approaches adopted by private hospitals and poor human resource policies adopted by public hospitals. Crucially, the assessment of MNC is essential to recognize possible areas that require improvement actions. Therefore, the results of this research could help policy makers to develop interventional programs for reducing the occurrence of MNC, therefore, improving the quality of healthcare (Blackman et al., 2018).
The aims of this cross-sectional study were to (a) describe the frequency and types of MNC in medical and surgical wards in Jordanian hospitals; (b) to examine the differences in MNC items in public, private, and university hospitals; and (c) to examine the association between professional and demographic characterstics and MNC in Jordanian hospitals. Therefore, the findings of this study should provide an important insight into MNC in the Jordanian healthcare context.
Methods
Study Design and Setting
This was a cross-sectional study carried out with registered nurses (RNs) employed at medical and surgical wards in 10 Jordanian hospitals. Performing the study in similar wards was intended to control unrelated variables in the practice environment (Winsett et al., 2016).
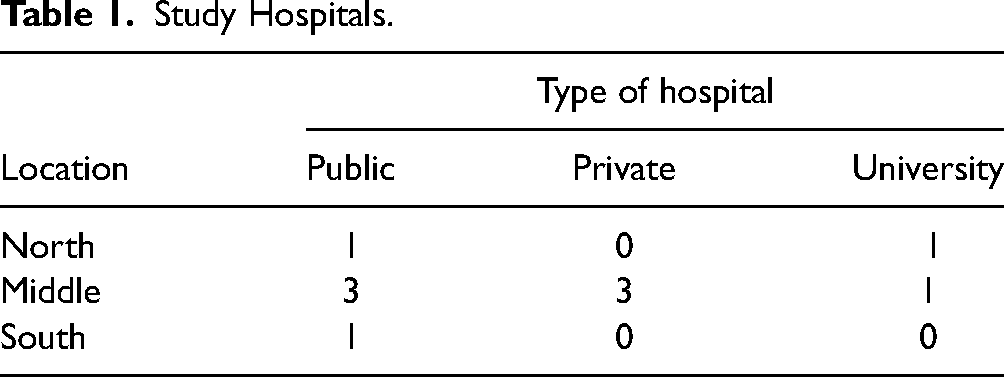
The study setting was five public hospitals, three private hospitals, and two university hospitals. A cluster random sampling technique was utilized in this study. Initially, the country was clustered into three divisions: north, middle, and south. A list of all hospitals in these three regions with beds’ capacity greater than 150 was selected. The second step comprised selecting hospitals randomly from these clusters. This resulted in a final cluster sample that consists of 10 hospitals distributed throughout the country, with two from the northern region, seven from the central region and one from the southern region. All hospitals participated voluntarily in the study (Table 1).
Study Hospitals.
Study Sample
A convenience sampling approach (Polit & Beck, 2008) was used to recruit all bedside RNs in medical and surgical wards in the selected hospitals. The study involved nurses who were available at the time of the study. The study’s inclusion criteria were an RN who is employed in the current setting for not less than a year and can read and write in English. The exclusion criteria were nurses working in a managerial position and nurses on maternal leave, annual leave, or vacation during the data collection period.
The sample size was calculated based on the analysis of variance test (ANOVA). Using G. Power (Faul et al., 2007) software, Alpha level of 0.05, power of 0.80, and relatively small effect size of 0.13, the required sample size for comparing ten groups is 940 participants from all hospitals. Thus, the sample size in our study targeted 1,000 participants to overcome missing data.
Data Collection
Prior to commencing the study, six research assistants (RAs) who hold at least a Bachelor's degree in nursing were hired and trained on the procedures of data collection and the data collection tool. RAs explained the purposes of the study to the head nurses in the wards where data collection was conducted. Paper-based questionnaires comprising information about the purposes of the study and contact information of the principal investigator were distributed to the nurses by the head of their departments. All nurses who met the inclusion criteria were invited to participate in the study. Participants were asked to complete the questionnaires and put the completed questionnaires in the manager's office. No incentives were offered for participation in this study. The completed questionnaires were sealed in envelopes to ensure confidentiality. The envelopes were then collected by RAs and returned to the principal investigator. Of the 1,000 questionnaires that were distributed to nurses, 675 were returned, yielding an overall response rate of 68%. Three questionnaires were discarded owing to incomplete data, and 672 questionnaires were used in the final analysis.
Research Instrument
Self-report is the most common way for gaining information about care that was not provided to patients, as it can’t be found in clinical documents and other data sources (Tubbs-Cooley et al., 2019). The MISSCARE Survey was used in this study to assess MNC (Dabney et al., 2019). To date, the MISSCARE Survey is the most widely used valid instrument to assess MNC (Palese et al., 2021). The internal consistency and reliability of the original English version estimated with Cronbach's coefficient alpha ranged between 0.64 and 0.86 (Kalisch et al., 2011). In the present study, Cronbach alpha of the missed care items was 0.93.
The MISSCARE Survey consists of two sections: Section A, which evaluates the type and frequency of MNC across 25 nursing elements on a 5-point Likert scale y (1 = never, 2 = rarely, 3 = occasionally, 4 = frequently, and 5 = always). Respondents were asked to rank the relative frequency of missing each element. Section B of the survey assessed perceived reasons of MNC across 22 reasons on 4-point Likert scale (1 = not a reason, 2 = minor, 3 = moderate, and 4 = significant reason). However, this paper deals only with Section A in the MISSCARE survey. Background variables of participants included questions related to age, education, job title, professional experience, work hours, hours of overtime, days of missing work, perceived adequacy of staffing, and leaving intentions. The last element in the introductory part of the MISSCARE Survey utilizes a 5-point Likert scale which ranges from very satisfied to very dissatisfied to measure the level of nurse satisfaction with the current position, being a nurse, and the level of teamwork in the current working unit.
Permission was sought and granted from the survey authors to use the MISSCARE Survey (Dabney et al., 2019) for this study. The survey was kept in its original language (English) as English is the main language of communication in Jordanian hospitals. However, minor modifications were made to the background information section in the MISSCARE Survey to fit the Jordanian nursing context, particularly, in questions related to education degree and job titles of nurses. Questions related to age, years of experience, overtime, and days of missing work were collected as continuous data. A pilot study (n = 5 nurses) was also conducted to verify that the items and questions in the survey tool are clear and understandable. No amendments were performed to the wording of the survey after the pilot study analyses.
Ethical Considerations
Data were collected during the second wave of the COVID-19 pandemic in the period between March and July 2021. Ethical approval was obtained from the relevant university Research Ethics Committee under approval number 67/2020/4598. Permission was also obtained from the Jordanian MOH and administrations of the health facilities in which the study took place.
The introductory part of the survey provided information about the objectives and all necessary information about the study. Ethical issues raised in this study included possible embarrassment to nurses reflecting on tasks unperformed and the possibility for criticism of management in their organization. Therefore, ethical aspects including confidentiality, anonymity, and the right to withdraw from the study without punitive repercussions were highlighted. No identifiable information was obtained from the participants. Answering and submission of the questionnaire were considered as implied consent. However, one university hospital required a signed consent form by the participants prior to completing the survey. Only the research team has access to data collected for the purpose of this research.
Data Analysis
The data entry, cleaning and analysis were performed using the Statistical Packages for Software Sciences (SPSS) (version 21). Descriptive statistics (i.e., frequency, percentage) were used to describe the sociodemographic and professional characteristics of the participants and missed care items. For the purposes of analyzing the Likert scale responses for nursing perspectives toward MNC, Likert scores were collapsed into two categories. Always, frequently and occasionally were grouped as ‘MNC’, while never and rarely were collapsed into ‘absence of MNC’. This method of collapsing was used in previous research (Kalisch et al., 2009). The question related to nurses’ perceptions of staffing adequacy was recoded such that higher numbers indicates higher perception of staffing adequacy. ANOVA was used to examine differences in the evaluation of MNC by type of sector. Pearson correlation coefficient test was used to determine the relationship between professional and demographic characteristics of the nurses and MNC. P value < 0.05 was considered statistically significant.
Results
Sample Characteristics
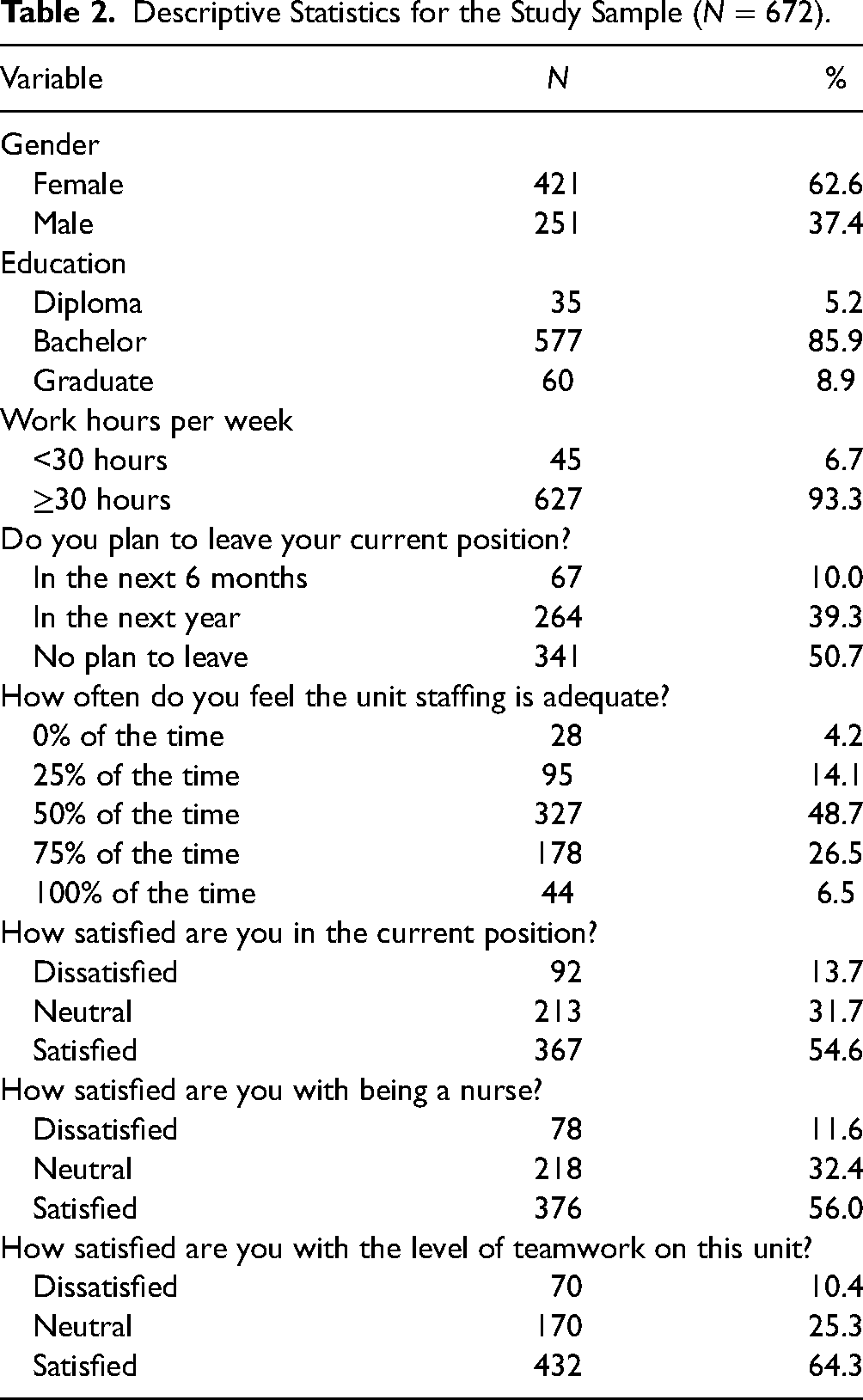
Table 2 presents the characteristics of respondents. Almost two-thirds of the nurses are females. Most participants have a bachelor’s degree in nursing (85.9%). About half of the participants are planning to leave their current position within a year. Only 7% of the participants feel that the unit staffing is adequate. Slightly more than 10% of the nurses are dissatisfied with their current position, being a nurse, and the level of teamwork on the unit.
Descriptive Statistics for the Study Sample (N = 672).
Missed Nursing Care
Table 3 shows the MNC as reported by the study participants. Ambulating or mobilizing the patients three times per day was the highest MNC (57.4%); followed by providing mouth care (56.3%), emotional support to patient and or family (52.8%), and feeding the patient when food is still warm (52.5%). The least missed elements of nursing care were: (1) bedside glucose monitoring as ordered (34.1%), (2) hand washing (35.4%), and (3) medications administered within 30 minutes before or after the scheduled time (35.9%).
Missed Nursing Care Sorted from Highest to Lowest (N = 672).
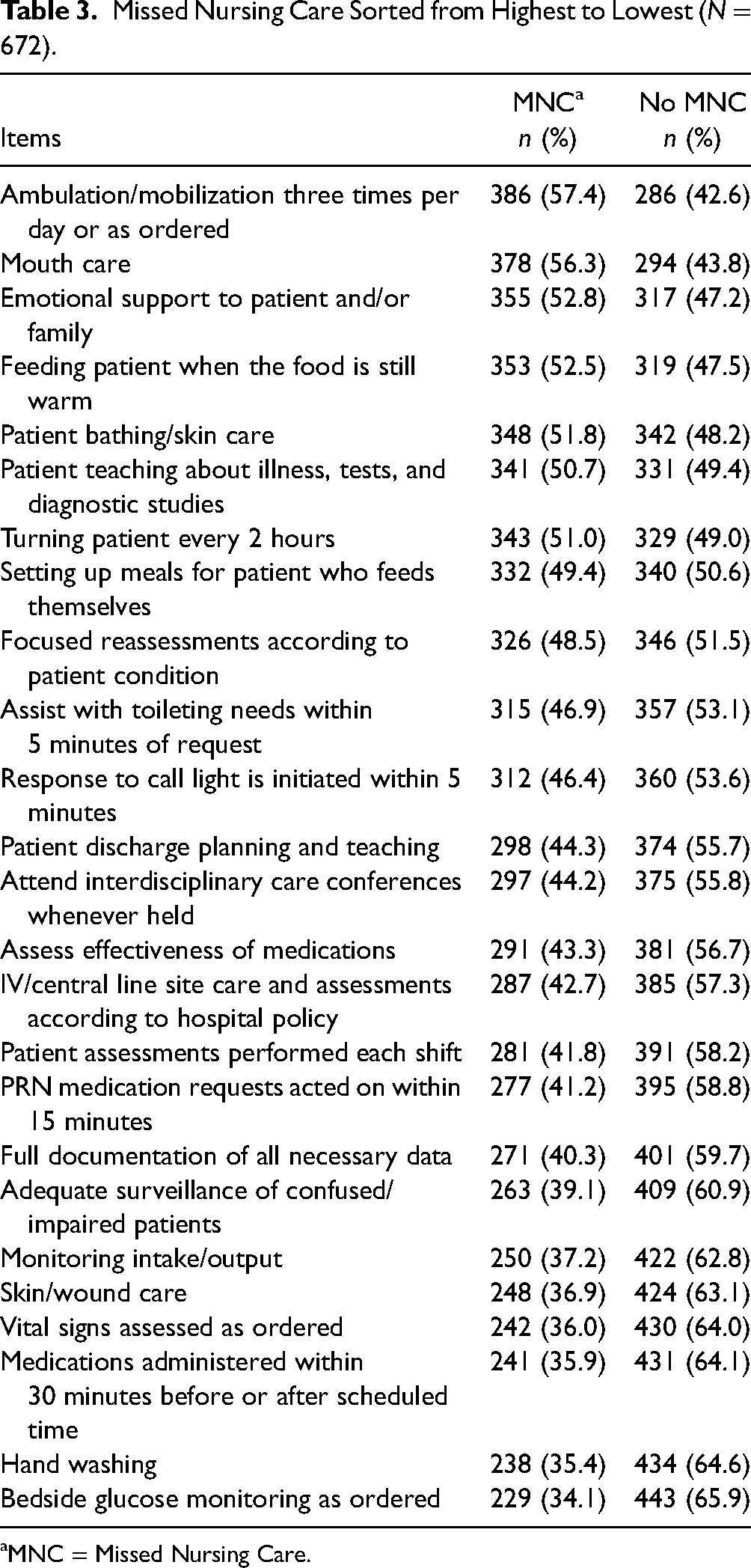
MNC = Missed Nursing Care.
MNC in Different Sectors
The MNC was the least at the private hospitals. The public hospitals have the highest MNC. The comparisons between the health sectors on the MNC are presented in Table 4.
ANOVA Test to Compare Between Health Sectors on MNC.
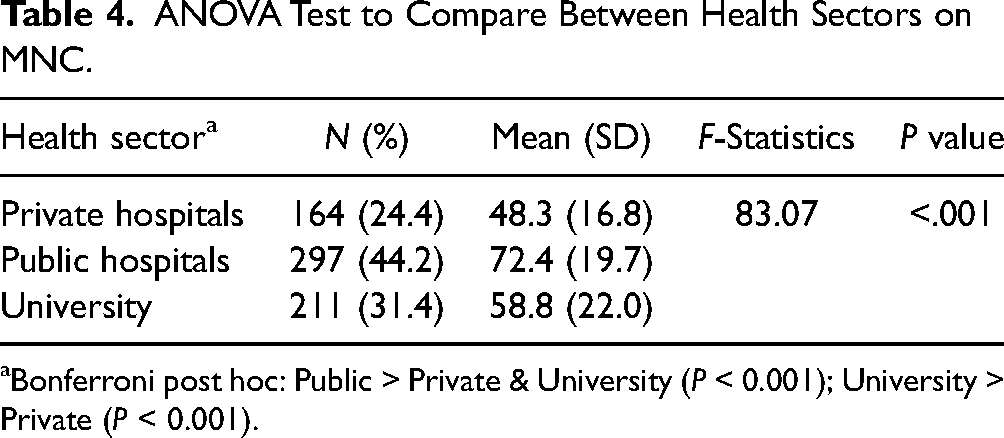
Bonferroni post hoc: Public > Private & University (P < 0.001); University > Private (P < 0.001).
MNC per Sector
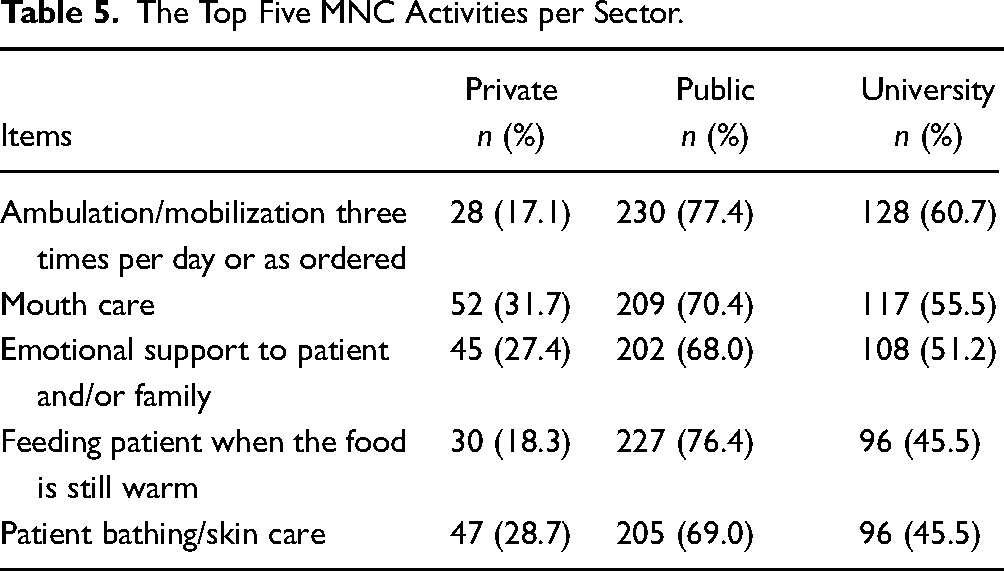
Table 5 presents the highest MNC per health sector. In the public sector, ambulating the patients (77.4%) and feeding them (76.4%) were the most common MNC. In the university hospitals sector, ambulating the patients (60.7%), and doing mouth care (55.5%) was the highest MNC. However, in the private sector, ambulating the patients was among the highest nursing care that was met (only 17.1% missed).
The Top Five MNC Activities per Sector.
The Association Between Professional and Demographic Characterstics and MNC
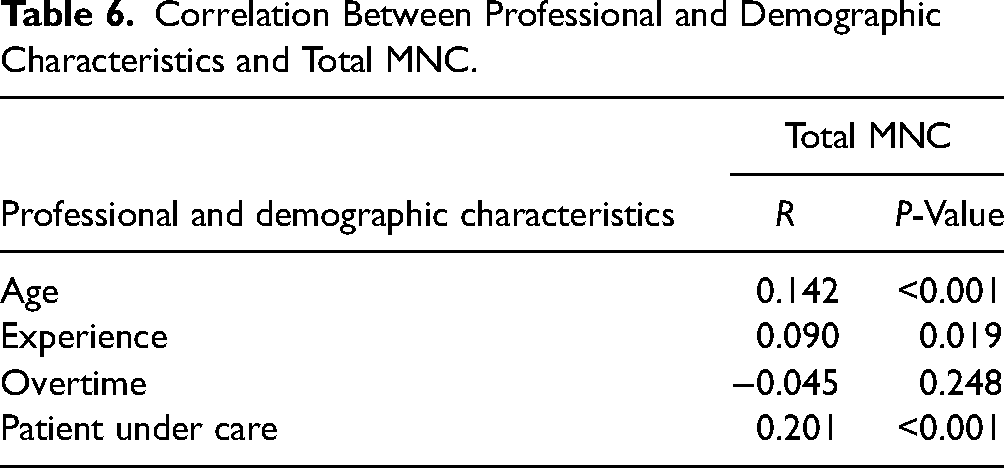
Table 6 demonstrates the findings of the Pearson correlation coefficient. The findings revealed a significant positive correlation between age and total MNC (r = 0.142, P < 0.001). A significant positive correlation was also found between number of patients under care and total MNC (r = 0.201, P <0.001).
Correlation Between Professional and Demographic Characteristics and Total MNC.
Discussion
Investigating MNC is essential to align with healthcare institutions’ current patient safety initiatives (Lee & Kalisch, 2021). This paper examined missed care items in medical and surgical wards in ten Jordanian hospitals. It also investigates differences in missed care items in different healthcare sectors. Overall, ambulation, oral care, and emotional support to the patient and/or family were the top three missed care elements. Bedside glucose monitoring as ordered, hand washing, and medications administered within 30 minutes of the scheduled time were the three least missed elements of care.
The findings of this study indicate that ambulation was the most frequently missed care item in the participating hospitals. This is consistent with previous literature (Zeleníková et al., 2019). Doherty-King and Bowers (2013) found that nursing staff regarded ambulation as being a responsibility for other personnel. Also, nurses do not recognize the importance of ambulation for better health outcomes and do not prioritize this care item (Kalisch et al., 2011). Furthermore, ambulation of patients is not documented in the patient records on a routine basis. Thus, there is less likelihood that this care would be recognized as left undone by nurses (Kalisch et al., 2011). This finding may relate to a lack of time and equipment during the COVID-19 pandemic (Bergman et al., 2021). However, it may also relate to patients’ dependence on relatives in the provision of some elements of care, such as ambulation, which has been less available during pandemic related lockdowns (Al-Faouri et al., 2021). In this context, existing documentation systems may need to be refocused (Kalisch et al., 2011). Importantly we found that ambulation was less frequently missed in private hospitals compared with public and university hospitals. This could be related to reduced nursing workload and availability of equipment in the private sector compared with other sectors. It should be stated that the MISSCARE Survey was not designed to explore in-depth the reasons for missing ambulation, in particular by nurses. The point above could be an area for future research.
Consistent with the previous literature (Saqer & AbuAlRub, 2018), the results of this study revealed that nurses perceived the provision of oral care for hospitalized patients as one of the prominent missed care items. Despite being an essential element in nursing care, nursing staff frequently neglect oral care as they do not appreciate its importance for patients (Blackman et al., 2018). If this care is not provided, especially for dependent patients, it can lead to mucositis for patients receiving oxygen therapy which can aggravate their breathing problems (Carpenito, 2021). One study found that nurses during COVID-19 do not have time to perform proactive interventions such as mouth care (Bergman et al., 2021). A recent mixed methods study uncovered that workload, lack of appropriate resources, and lack of knowledge and skills to perform oral care were among the reasons that hamper prioritizing oral care provision by nurses (van Noort et al., 2020). Hence, resources to carry out oral examination and oral hygiene should be available in the work environment (van Noort et al., 2020).
Emotional support was also found to be one of the most frequently missed care items in the study setting. This finding was congruent with a prior studies by Al-Kandari and Thomas (2009) and Albsoul et al. (2019). It is important to highlight the significance of psychosocial care by nursing staff in this context. In fact, psychosocial care has a significant impact on patients’ quality of life. However, nurses often consider psychosocial care as not integral to their practice or less important to the patients (Legg, 2011). The reason for the missing provision of psychosocial support to patients could be related to the dominance of the functional nursing model in the public sector in Jordan; therefore, minimizing the provision of patient-centered care (Shuriquie et al., 2008). In this regard, it is important to emphasize that nursing programs in universities should aim for preparing student nurses’ knowledge and skills in holistic care provision to patients (Safadi et al., 2011). Lack of management support could also explain this important finding (Jangland et al., 2017). Missing psychosocial support to patients could also be related to medical dominance over the nursing profession and interprofessional conflicts that have a detrimental impact on the provision of patient-centered care in healthcare organizations (Belrhiti et al., 2021). Another possible justification for missing emotional support would be changes in the work environment, namely, the formation of new care teams, lack of resources, and heavy workload during the COVID-19 pandemic (Safdari et al., 2022).
Consistent with other studies (Papastavrou et al., 2016), medication administration was one of the least missed care activities perceived by nurses. The reason for this finding could be attributed to the fact that nurses are medically oriented. Thus, they focus on the medical aspects of care and underestimate the role of psychosocial support in promoting health. Additionally, during the pandemic, nurses tend to prioritize activities related to the administration of antibiotics and antiviral drugs over other tasks related to communication and interaction with patients (Danielis & Mattiussi, 2020).
Handwashing was perceived by the nurses as one of the least frequently missed care items. This is in line with previous research (Dutra et al., 2019). This finding was not surprising, given that this research was conducted during the second wave of the COVID-19 pandemic. During the pandemic, a recent Jordanian study found that 96% of nurses in acute care settings washed their hands before/after handling patients (Alhwamdih et al., 2021). Handwashing is also protective for nurses and patients. However, this practice demonstrates that nurses are aware of this protective measure and appreciate this in their daily practice.
The findings of this study indicate that the amount of MNC is higher in public hospitals than in private and university hospitals. It can be suggested that this can be due to differences in the nurse–patient ratio between public and private hospitals in Jordan. One study found that nurse:patient ratio in medical and surgical wards is 1:6 in private hospitals compared to 1:12 in public hospitals (Al-Hamdan et al., 2017). The evidence demonstrated that if the nurse/patient ratio increased by one patient (over the ratio 1:6), the risk of patient death increased by 7% (Aiken et al., 2014).
Furthermore, public hospitals in Jordan are characterized by an increasing nursing shortage compared to other sectors (Mrayyan, 2005). Nurses in the private sector in Jordan do not have job security compared with nurses in the public sector. Hence, they could be more apprehensive about the consequences if reported events of MNC during their practice (Al-Faouri et al., 2021). It can also be argued that MNC is lower in university hospitals than in public hospitals as these hospitals require nurses to operate based on higher standards of care (Mrayyan et al., 2021).
When comparing MNC in private and university hospitals, our findings demonstrate that MNC is higher in university hospitals than in private hospitals. Similarly, Al-Faouri et al. (2021) found that level of MNC was the lowest in the private sector compared to public and teaching hospitals. Apart from the fact that private hospitals are the least crowded sector in the Jordanian healthcare sector (Mrayyan et al., 2021), the explanation for this finding might be related to the increased workload on nurses in university hospitals as nurses are required to mentor students in their training (Krichbaum et al., 2011). In addition, the teaching hospitals are recognized for relocating nurses to other units that have reduced staffing levels (Amarneh, 2017), which may lead to more unmet nursing care in these settings.
In the present study, we found that the age and number of patients cared for were significantly correlated with MNC. This finding is similar to previous research (Chegini et al., 2020). Professional attentiveness and precision may diminish in aging nurses, which ultimately reduces the capability to identify omitted care (Palese et al., 2015). Increased number of patients under care may increase nursing workload; therefore, increasing the potential for MNC. Nursing administrators need to have an efficient and sufficient nursing staff to meet patients’ care needs in order to improve nursing care in hospitals (Diab & Ebrahim, 2019).
The implications of these findings for public policy and health service management are difficult to evaluate. Further analysis is required as to how the particular culture and systems in Jordan influence these findings and allow the application of lessons from other jurisdictions to be applied. The evidence demonstrated the impact of perceived MNC on resourcing levels, which in turn relates to overall system resourcing, which faces major financial and workforce challenges. On the other hand, some operational initiatives such as mandating error reporting systems in private hospitals, which emphasize the privacy and anonymity of the reporter and the training of staff on error reporting, are more achievable (Lederman et al., 2013).
Limitations
The present study has several limitations that should be considered when interpreting the findings. Firstly, the cross-sectional design gives only a snapshot of the real situation of MNC in the involved hospitals. Therefore, the results of this study may be different if the study was performed at another time. Secondly, the use of convenience sampling technique to recruit RNs from the study setting. Therefore, the findings may not be generalizable to all RNs in Jordan. However, the risk of sampling bias for the participating hospitals would be reduced in this study, given that the majority of the population lives in northern and middle regions in Jordan (Department of Jordanian Statistics, 2018). Thirdly, measurement of MNC in this study relied on nurses perceptions of missed care through self-reported surveys, which are subject to bias as participants may report what is socially acceptable (social desirability bias) (Chung & Monroe, 2003). As such, direct observational methods or review of existing documentation (Tesoro et al., 2018) to characterize actual missed care incidences should be considered in future research. Fourthly, the surveys were distributed to the participants through their managers. This technique could pressure participants to fill out the survey in a specific manner (Day, 2005). Fifthly, despite the inclusion of most healthcare sectors in Jordan: public, private, and university, the inclusion of military hospitals is needed in future research. Sixthly, the timing of the data collection during the COVID-19 pandemic could impact the study's findings. Lastly, while the association between MNC and patient and organizational outcomes was not the purpose of this study, it would be important to investigate such association in future studies.
Conclusion
A study of Jordanian RNs conducted during the COVID-19 in medical and surgical wards found that many nursing activities, notably ambulation, oral care, and psychosocial support, were perceived to be missed more frequently by nursing staff. Nurses working in public hospitals were more likely to miss care than those working in private and university hospitals. However, differences in reasons of MNC in various health care sectors require further investigation. Alterations in the practice environment and staffing are tactics to reduce care compromise. Nurse managers should examine work settings in order to recognize weaknesses (Lake et al., 2020); therefore, reducing the potential for MNC in the hospital setting.
Footnotes
Acknowledgment
The authors thank all the nurses who participated in this study for their invaluable time and information.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research of this article: Deanship of Academic Research, University of Jordan (grant number 67/2020/4598). The authors disclosed receipt of the following financial support for the research of this article: Deanship of Academic Research, University of Jordan (grant number 67/2020/4598).
Correction (May 2023):
This article has been updated with the city ‘Amman’ for the corresponding author since its original publication.