
Abstract
Opioid misuse is a growing public health concern in the United States (U.S.). This problem continues to claim many lives and has affected the life expectancy of the U.S. population. In the past few years, the Black population has witnessed an increased rate of overdose deaths compared to their white counterparts. This review seeks to characterize recent trends in opioid prescription practices and overdose deaths among the Black population in the U.S. An integrative review was conducted with a literature search from CINHAL, MEDLINE, and PsycINFO databases. The literature search identified 11 articles for the analysis. All studies were quantitative. Six studies focused on overdose mortality and five on opioid prescription practices. The results indicate a rising trend in opioid overdose mortality among Black people due to the availability of synthetic opioids on the illegal drug market. Black people receive fewer opioid prescriptions and experience higher rates of opioid dose reduction compared to Whites. The Black population has experienced an increase in opioid overdose mortality compared to the White population within the last two decades. Opioid overdose deaths among Black people are highly associated with the proliferation of synthetic opioids, and Black men have been more affected than Black women. Black people experience lower rates of opioid prescription during E.R. visits compared to Whites. The issue of low opioid prescribing among Black people needs to be addressed since it affects their health outcomes and is a factor that contributes to the use of illicit synthetic opioids.
Introduction
The Black population in the United States (U.S.) is diverse. Members of this Black population have a varied history in the nation; while many are descendants of enslaved people, others recently arrived through various forms of immigration (Anderson, 2015). The Black population has complex ethnic and racial identities which reflect intermarriage among different races and ethnic groups. This complexity has resulted in distinct demographic and economic characteristics among the diverse Black population in the United States (Collins & Wanamaker, 2022; Lloyd et al., 2021). The Black population in the U.S. is growing steadily; in 2019, 46.8 million people in the U.S. identified as Black either as part of a multiracial or ethnic background or alone, up from the 36.2 million recorded in 2000 (U.S. Census Bureau, 2019).
The American healthcare system is challenged with inequalities that severely impact people of color and other minority groups (Gillispie-Bell, 2021; Yearby, 2018). These inequalities contribute to the gaps in health insurance coverage, unequal access to services, and poor health outcomes among certain populations (Mateo & Williams, 2021; Renna et al., 2021). However, the Black population bears most of these challenges (Gillispie-Bell, 2021). African Americans spend 20% of their annual household income on healthcare premiums and out-of-pocket costs (Kwon et al., 2018). Because African Americans tend to be poorer than other demographic groups, public insurance schemes are vital to ensure affordable healthcare and healthier outcomes (Ghosh et al., 2019). Despite the improved access to medical care under the Affordable Care Act, some stark disparities exist between the White and Black population health outcomes (Sealy-Jefferson et al., 2015). African Americans are more likely than Whites to die of pregnancy-related conditions, cardiovascular diseases, and addiction-related disorders (Mays et al., 2007). The Black population faces systemic racism in the U.S. (Lavalley & Johnson, 2022), which is detrimental to the Black population in terms of chronic stress and impacts the quality of health care they receive (Doubeni et al., 2021; King & Redwood, 2016). In this review, we use the terms African American and Black interchangeably to refer to individuals of African descent living in the U.S., recognizing the semantic and political nuances associated with each term. This acknowledges the variations in terminology used in the articles reviewed and the fact that both terms are used to describe the same population group.
The opioid crisis is a growing major public health issue in the U.S. and around the world. This problem has transformed from a problem of misuse to a crisis in the last two decades (Stoicea et al., 2019). The opioid crisis seriously threatens the U.S. population's health, economic, and social outcomes (Fuhrmann-Berger, 2018). In the U.S., the opioid crisis is one of the most disastrous public health problems that continues to claim more lives each year. This situation is worrisome as the U.S. continues to have a decreased life expectancy at least in part due to this ongoing crisis. Luo et al. (2021) and Reinhart et al. (2018) report that the hours of work lost to the opioid crisis and the burden imposed on family members who provide for their wards who have developed opioid addiction are worrying. The economic and social impact of the opioid crisis continues to affect people since the current opioid crisis shows no sign of abating (Neville & Foley, 2020). Many affected individuals usually take these opioids to manage their physical pain and escape the economic hardship and other harsh social conditions they face. The Black population in the U.S. face gaps in wages, employment, and business ownership as compared to the White population (Lang & Kahn-Lang Spitzer, 2020; Manduca, 2018) and, as a result, tend to make them poorer as compared to the Whites. This disparity sometimes subjects the Black population to economic hardships and other environmental issues. Previous studies report that socioeconomic factors, including poverty, unemployment, and poor housing conditions, are interconnected with opioid misuse (Han, Compton, et al., 2017; Han et al., 2015; Han, Jones, et al., 2017). In a related study, Dasgupta et al. (2018) identified poverty and unemployment as major pillars in the current opioid crisis facing the U.S. Considering the socioeconomic disparities between Black and White populations in the U.S. It is unsurprising that opioid overdose deaths keep soaring in the Black communities. Nevertheless, more studies are needed to understand the opioid crisis specifically in the Black community.
Over 900,000 lives have been lost to drug overdose since 1999; during this period, opioid-related overdose deaths increased more than eight times (CDC, 2021). In 2020, opioid overdose deaths accounted for nearly 75% of drug overdose deaths (Hedegaard et al., 2021). According to the Centers for Disease Control and Prevention (CDC), the United States recorded over 70,000 opioid overdose deaths between April 2020 and March 2021, and Black and Brown communities were hit hardest (DiGennaro et al., 2021). In 2020, Black Americans recorded the highest percentage rise of 48.8% in overdose deaths per 100,000 compared to 26.3% observed in White Americans (Friedman & Hansen, 2022). The statistics behind this overdose mortality demonstrate that drug overdose is gradually becoming a racial justice issue in the United States. Black Americans’ overdose deaths rate was higher than White Americans in 2020 for the first time since 1999 (Friedman & Hansen, 2022), and this shift reflects that the Black population in the U.S. has seen an increasing annual percentage of overdose deaths in recent years (Friedman & Hansen, 2022). This integrative review aims to characterize recent trends in opioid misuse and opioid overdose mortality among the Black population in the United States.
Design
An integrated literature review was conducted using established guidelines (Whittemore & Knafl, 2005). A literature search strategy was developed to enhance the extraction of data. After a careful review of eligible studies, data were extracted for analysis. The extracted data were analyzed using a content analysis method. The data were displayed in tabular and chart format to identify similarities, differences, and patterns in the data. All relevant features of texts and comments were grouped into categories and later condensed into central themes. Data from primary studies utilized in the review were examined to ensure that all analyses were grounded in the data. The review followed the 2020 PRISMA (Preferred Reporting for Systematic Reviews and Meta-Analyses) guidelines (Page et al., 2021).
Methods
A logical search was conducted using the CINAHL, PsycINFO, and MEDLINE databases. The search terms used for the search were “overdose death,” “overdose mortality,” “opioid misuse,” or “prescription opioid misuse,” “non-medical use of opioids,” “opioid dose reduction,” or “black opioid use.” The search was limited to research articles published in English since 2015. The inclusion criteria targeted studies that focused on the Black population in the United States, studies that focused on racial disparities among the U.S. population, studies published in English journals, and studies published within the last seven years (2015–2022). Citations of all selected articles were imported into the Mendeley reference manager, and all duplicates were removed. The titles and abstracts of selected articles were thoroughly reviewed, and the following studies were excluded from the review: studies that focused on opioid prescription guidelines for chronic pain, studies that focused on opioids for substance use treatment, and studies that focused on opioid use, excluding the Black population. The 11 articles were summarized logically using a data extraction technique. The extracted data were analyzed with data display matrices to code relevant features, itemize similar codes, and condense codes into central themes (Appendix A).
Although most of the studies in this review did not state the specific theoretical framework employed, the selected studies clearly defined the various concepts employed. This limited the scope of all relevant data and focused on specific variables which were needed for the study analysis and subsequent interpretation. These specific variables help to limit generalizations and thus influence a specific phenomenon. These served as a basis for the various study hypotheses and the choice of research methods employed. The 11 studies included were cross-sectional. This type of observational study is suitable for research that delves into data surrounding a population at one specific period and enables researchers to measure multiple outcomes simultaneously. This makes the cross-sectional design more appropriate for the studies included in the review since all studies focused on specific data surrounding a particular population at a given time.
Results of the Literature Search Strategy
The literature search yielded 606 articles from the selected databases. Fifty-six studies were removed due to duplication. The remaining 550 studies were reviewed by applying the inclusion and exclusion criteria. In all, only 25 studies were identified as potentially relevant to the purpose of the review. After thoroughly reviewing the remaining 25 studies, only 11 were included in the final review process (Figure 1). All 11 studies provided a research hypothesis and relevant research questions to guide their study.
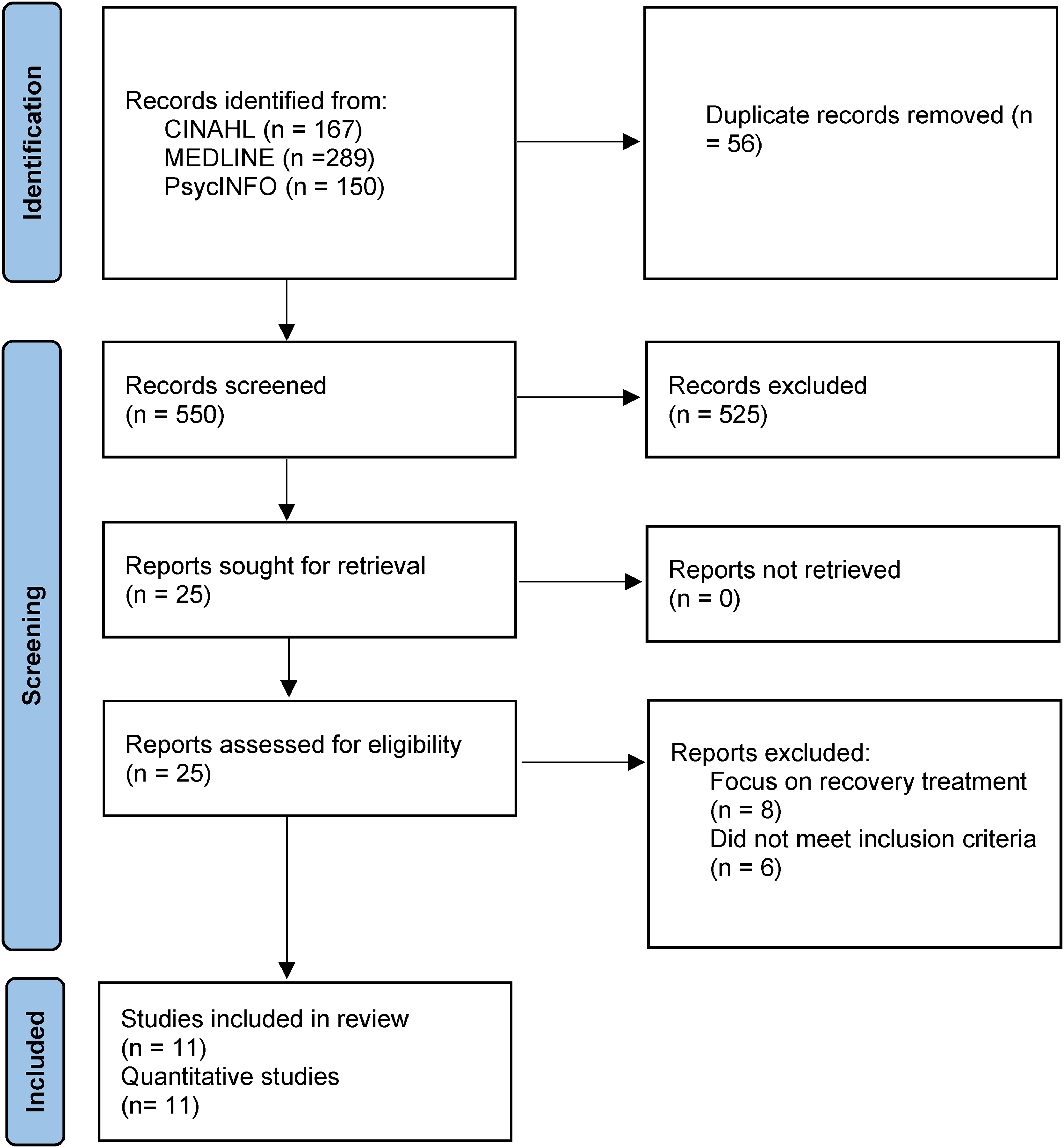
PRISMA Diagram Showing the Number of Studies Included in the Paper.
The 11 studies used population-based, quantitative designs. Nine studies were identified as high quality, and the remaining two as moderate quality. The nine studies were well-performed observational studies. These classifications were based on the GRADE system of identifying the quality of evidence (Broek et al., 2009). Six studies (n = 6) focused on opioid overdose mortality, while the remaining five (n = 5) focused on opioid prescribing practices. The sample size employed for the studies ranged from 3,726 to 8,263,902. Studies focusing on opioid overdose utilized information from the CDC's Wide-ranging Online Data for Epidemiologic Research (WONDER) database, National Center for Health Statistics, and National Death Index. Other databases utilized in the other studies included National Survey on Drug Use and Health and Medical Expenditure Panel Survey. The ages of participants ranged from 0 to 65 years.
Results
Articles were examined for consistent themes. Two themes emerged from the data analysis: opioid overdose mortality from six articles and determinants of opioid misuse from the remaining five articles.
Trends in Opioid Overdose Mortality
This review indicates a rising trend in opioid overdose deaths among the Black population in the United States between 1999 and 2021. According to Althoff et al. (2020), opioid overdose mortality among non-Hispanic (N.H.) Blacks has increased by 174% compared to an 85% rise recorded among non-Hispanic (N.H.) Whites. Althoff et al. (2020) further indicated that the sharp increase was recorded among urban younger and older adults, with men experiencing the most significant increase in opioid overdose deaths. Drake et al. (2020) further reported that despite recording large numbers of overdose deaths among NH Whites from 2.8 to 19.4 per 100,000 from 1999 to 2017, N.H. Blacks experienced a similar rise in opioid overdose deaths from 3.5 to 12.9 per 100,000 in the same period. Kiang et al. (2021) assessed trends in opioid overdose mortality among N.H. Blacks and NH Whites. They reported that opioid-related mortality is increasing rapidly among the Black population in most states, with a median increase of 19.4% per year compared to 0.3% per year among the White population. Nacev et al. (2018) report that the rise in opioid overdose in Wisconsin State from 1999 to 2018 sharply increased after 2014. They further report that Black people are twice as likely to die from opioid overdose than their White counterparts in Wisconsin. Their report further indicates that this overdose mortality also varies with age and is highest among 25–34-year-old Whites and 55–64-year-old Black people. Lane et al. (2022) in a study to determine the burden of premature opioid mortality report that opioid overdose deaths account for most years of potential life lost (YPLL), and Black males suffered most of this mortality burden compared to Black females in rural counties accounting for 48% of population-adjusted YPLL.
According to the CDC (CDC, 2022), fentanyl has surpassed other drugs to become the leading cause of overdose deaths in the United States. Althoff et al. (2020) report that the sharp increase in opioid overdose mortality was recorded when fentanyl was common on the drug market and further suggested that fentanyl could be the driving force behind the increased opioid overdose rates among the Black population. A report by Drake et al. (2020) indicates that overdose death due to synthetic opioids increased 90-fold among N.H. Blacks compared to a 39-fold increase observed among NH Whites from 1999 to 2017. However, heroin-related overdose death increased 8.7-fold among NH Whites and 6-fold among N.H. Blacks during the same period. A similar study by Kiang et al. (2021) indicated that synthetic opioids accounted for 76% of opioid overdose mortality in most states in the United States between 1999 and 2019. Hoopsick et al. (2021) reported that between 1999 and 2018, overdose mortality among N.H. Blacks was highly associated with synthetic opioids and heroin use, while NH Whites were highly associated with the use of natural and semisynthetic opioids such as oxycodone, hydrocodone, and hydromorphone. The report added that men had higher rates of opioid overdose mortality than women, regardless of race and ethnicity, with all forms of opioids except methadone.
Determinants of Opioid Misuse
Schuler et al. (2021) reported that from 1999 to 2018, prescription opioid misuse (POM) was higher among NH Whites than other minority groups, including N.H. Blacks. Their report further revealed a steady rise in heroin use among NH Whites from 2015 to 2018. Also, the study findings showed a significant decrease among N.H. Blacks compared to NH Whites and Asian Americans. According to Yockey et al. (2020), there is a decline in nonmedical opioid use among youth in America. However, the results of their study indicate that African American youth are more likely to engage in nonmedical opioid use than their white counterparts. The study further reported that African American youth who engage in nonmedical opioid use are likely to use it for pain relief. Also, their report further indicates that youth with a history of marijuana, alcohol, and cigarettes were more likely to engage in opioids.
Buonora et al. (2019) report that N.H. Blacks experience higher rates of opioid reduction prescription practices compared to NH Whites, and women are more likely to experience opioid dose reduction compared to men, irrespective of race. A similar study conducted among children in the United States revealed higher rates of opioid prescribing among White children compared to Black children. The study findings revealed that Black children are more likely to receive nonopioid analgesics to manage their pain (Groenewald et al., 2018). The study further revealed that racial disparities in opioid prescribing are affected by healthcare provider race and that White healthcare providers are less likely to prescribe opioids to Black patients who visit the emergency room (E.R.). Townsend et al. (2022) report that introducing and adopting the prescription drug monitoring program (PDMP), an interactive electronic database that monitors controlled substance prescriptions by all 50 states, reduced the rate of opioid high-dose receipt in the Black population but not among Whites. The report further indicates that within the first three years of PDMP implementation, the White population continued to experience opioid high-dose receipt whereas the Black population experienced an immediate reversal in high-opioid dose receipt.
Discussion
Opioid overdose mortality rates in the Black population have significantly increased in the last two decades. This trend has been observed in several studies that assessed trends in overdose mortality in the U.S. Althoff et al. (2020) reported that between 2013 and 2017, overdose mortality among Blacks increased by 174% compared to 85% observed in their White counterparts. This finding is consistent with Drake et al. (2020), who reported that Blacks experienced a sharp rise in opioid overdose deaths from 3.5 to 12.9 per 100,000 from 1999 to 2017. Although the White population continues to experience large numbers of opioid overdose deaths, the disproportionate increase in opioid overdose mortality rate among the Black population is worrying. These are all preventable deaths. This racial trend in opioid overdose mortality has been observed in most states in the U.S. Kiang et al. (2021) report that opioid overdose mortality is rapidly increasing in the Black population in most states in the U.S. with a median increase rate of 19.4% compared to 0.3% recorded among White population. This rate is 65 times higher than what was observed among White population from 1999 to 2019.
This increased overdose mortality rate among the Black population is not evenly distributed by sex and age. Black men have suffered more opioid overdose deaths than Black women (Althoff et al., 2020; Hoopsick et al., 2021). Men have higher opioid overdose mortality than women, regardless of race and ethnicity (Hoopsick et al., 2021). Opioid overdose mortality is highest among Black older adults (55–64 years), while in the White population, is highest among young adults (25–34 years) (Nacev et al., 2018.). These findings suggest that opioid misuse is more common among Black older adults than White older adults. This is consistent with the findings of Althoff et al. (2020), who reported increased opioid overdose mortality in older adults among the Black population. These findings reveal Black–White differences in opioid overdose mortality in the U.S., whereby Blacks experience a disproportionate burden. In a study to assess the burden of premature mortality due to opioid overdose, Lane et al. (2022) reported that the ages of males and females with fatal deaths involving opioid overdose decreased by 2.8 and 3.9 years, respectively. Lane et al. (2022) reported the most significant change of 2234% in synthetic opioid overdose deaths among Black men. These findings are not surprising since most studies report that Black men experience more opioid overdose compared to Black women and other populations.
The rising trends in opioid overdose among the Black population could be attributed to the proliferation of synthetic opioids such as fentanyl and fentanyl analogs on the drug market. Althoff et al. (2020) suggest that fentanyl could drive the increased overdose mortality among the Black population. Interestingly, these recent trends in opioid overdose mortality saw a significant increase at a time when fentanyl was common on the drug market (Kiang et al., 2021). Drake et al. (2020) report that overdose death due to synthetic opioids among the Black population increased 90-fold compared to a 39-fold increase in the White population in 2017. This finding is consistent with Kiang et al. (2021), who reported that synthetic opioid mortality accounted for 76% of overdose mortality recorded in most states in the U.S.
Hoopsick et al. (2021) further reveal that synthetic opioids and heroin are the main drugs associated with the recent opioid overdose mortality among the Black population, while mortality in the White population is associated with natural and semisynthetic opioids such as oxycodone, hydrocodone, and oxymorphone. Most studies that seek to explain this phenomenon of increased overdose death in the Black communities have postulated that the recent opioid overdose deaths are associated with the production and supply of cheap but potent opioids like fentanyl on the streets (Althoff et al., 2020; Kiang et al., 2021). This is not surprising since the results from this review imply that the Black population receives fewer opioid prescriptions to manage their pain and is more likely to experience high opioid dose reduction compared to the White population (Buonora et al., 2019). These are contributing factors among many that promote engagement of illicit opioids among the Black population. Black individuals denied adequate opioids during clinical care may pursue any avenue to obtain opioids to manage their pain. These individuals are likelier to find these synthetic opioids on the street (Althoff et al., 2020).
Although several studies report that heroin use is highly associated with the Black population, Schuler et al. (2021) report a significant steady rise in heroin use among the White population between 1999 and 2018. This finding is consistent with Drake et al. (2020), who report that heroin-related overdose deaths among the White population increased 8.7-fold compared to a 6-fold increase in the Black population between 1999 and 2017. This gradual shift needs urgent attention from stakeholders and policymakers since heroin use is a problem for both the Black and White populations. Future studies need to assess the origins behind the gradual rise in heroin use in the U.S.
Our review revealed that these disparities in opioid prescribing are also found among children of color. According to Groenewald et al. (2018), there are higher rates of opioid prescribing to NH White children than NH Black children. They further indicated that Black children are more likely to receive nonopioids to manage pain. Although they found no healthcare provider's race concordance with opioid prescribing among children, they reported that minority children received fewer opioid prescriptions from minority providers. Although this finding was reported from a study conducted among children in the U.S., stakeholders need to pay attention to this development in the adult population. Future studies need to investigate healthcare provider and patient race concordance and opioid prescribing among adults in a nationally representative sample. Opioid prescription misuse was significantly lower among the Black population compared to the White population (Schuler et al., 2021; Yockey et al., 2020). However, Yockey et al. (2020) further report that African American youth are more likely to engage in nonmedical opioid use to manage their pain.
Nonetheless, the low POM among the Black population could be attributed to the low opioid prescription rate among the Black population in the U.S. compared to their White counterparts (Buonora et al., 2019; Townsend et al., 2022). The White population has not experienced the same significant high-dose reduction as the Black population (Townsend et al., 2022). This confirms why natural and semisynthetic opioids versus synthetic opioids and heroin remain the leading causes of opioid overdose mortality among White and Black populations.
Conclusion
The opioid overdose mortality rate has increased significantly among the Black population in the United States since 2013. Black men are more affected by this mortality rise than Black women or Whites. Black older adults are most vulnerable to this recent mortality rise. This significant mortality increase has been largely attributed to the proliferation of synthetic opioids on the drug market. This confirms that synthetic opioids are gradually permeating the drug supply that previously mainly involved heroin. The Black population is less likely to engage in POM and nonmedical use of opioids because of less access to prescription opioids. This is reflected in the lower rates of overdose mortality due to natural and semisynthetic opioids observed in the Black population compared to Whites. However, this observed trend, related to lower opioid prescribing by Black patients during emergency room visits, can potentially affect health outcomes in this population, especially among those seeking pain treatment.
Policy changes in recent years to control opioid prescribing practices have contributed to the increased use of synthetic opioids among the Black population. Some of these disparities push Black individuals to engage in synthetic opioid use to manage their pain. This phenomenon could partly explain the recent rise in overdose mortality due to synthetic opioids among the Black population. Unfortunately, Black children also share the same fate and are less likely to receive opioids during E.R. visits (Groenewald et al., 2018). This could result in the undertreatment of pain in these children. Additionally, the Black population continues to experience high opioid dose reduction compared to their White counterparts, and women are more likely to experience high opioid dose reduction irrespective of race. This development can result in discriminatory and insufficient pain treatment among the Black population and women. Further studies are needed to explore the reasons behind this unfortunate trend in opioid dose reduction and assess its impact on pain treatment.
The introduction of PDMP, which resulted in opioid dose reduction among Black individuals, also presents another set of disparities in opioid prescribing in the U.S. Unfortunately, the Black population continues to suffer such disparities, which have serious consequences on their health outcomes. The CDC opioid prescription guidelines for chronic noncancer pain effectively manage pain among the Black population and others (Dowell et al., 2016). If this guideline is equally applied across diverse groups, it will significantly improve pain management in affected populations. It is expected that the CDC continues to review these guidelines with current evidence and recommendations from stakeholders and policymakers to address its unintended consequences. Clinicians require further training on racial biases and implicit biases that perpetuate health disparities in the Black community. Clinical decisions need to be based on clinical factors and evidence-based treatment protocols to prevent bias toward particular groups of patients.
It is recommended for future studies focus on why the implementation of the PDMP resulted in an immediate decline in high opioid dose receipt, primarily among the Black population. Also, the issue of healthcare provider race and opioid prescribing should be explored in older adults among a nationally representative sample. The findings of these studies could clarify the disparities in opioid prescribing among the diverse population in the United States.
Policy Implications
The findings of this study have important policy implications for addressing the opioid epidemic in the Black population in the U.S. Policy interventions should prioritize the availability of overdose-reversal medications such as naloxone in areas where the Black populations have high rates of overdose mortality. Policymakers should also work toward increasing access to addiction treatment services to combat the opioid epidemic in the Black communities. Efforts should be made to address the disparity in opioid prescription practices between Blacks and Whites and to ensure that Black patients are not undertreated for pain. Healthcare providers and policymakers must collaborate to develop and implement strategies to improve chronic pain management among Black patients.
Additionally, there is a need for further research to identify the root causes of the disparities in opioid prescription practices and overdose mortality rates between Black and White populations. The findings of this study provide a foundation for policymakers and healthcare providers to address the opioid epidemic in the Black population and develop effective, equitable, and culturally sensitive interventions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Appendix A
Data Extraction and Coding Table.