
Abstract
The healthcare sector is ubiquitously plagued by workforce shortages in economies around the globe. The fragility of this structural shortage becomes apparent when external shocks, such as the COVID-19 pandemic, exacerbate the lack of workers in clinical practice. In this article, we summarize current trends in healthcare workforce development across the globe, review theoretical concepts of workforce shortages, and discuss policies to address them. In practice, developed countries often address workforce shortages with targeted migration policies. However, targeted workforce migration policies only intensify workforce shortages in low-and middle-income countries. Theoretical macroeconomic models suggest that supply shortages may result from too low wages, supply lagging behind demand, and social perception. Changes in the wage rate cannot sufficiently increase the supply of health professionals as scholars find inelastic wages for physicians and nurses. Nonpecuniary factors such as working conditions, job satisfaction, and intrinsic motivation are at least equally important as financial incentives. In conclusion, increased wages can only be part of a heterogeneous policy plan to address shortages. Migration and retirement levels of health professionals can temporarily mitigate workforce shortages but rarely change the underlying systemic issues. Increasing the number of places available in medical and nursing schools while also improving, both, financial and nonfinancial incentives for employees are long-term structural policy options.
Keywords
Introduction
The recent COVID-19 crisis exacerbated already existing workforce shortages in many healthcare systems. New estimates suggest that there will be a shortage of 400,000 doctors and 2.5 million nurses across 32 Organization for Economic Cooperation and Development (OECD) countries by 2030 (Scheffler & Arnold, 2019). Countries such as the United States, Poland, Italy, Chile, Greece, or Israel will be especially hard hit, with deficiencies of more than 20% of the required workforce. In practice, we observe that almost all healthcare systems around the world claim to have a lack of health professionals (Majeed, 2017; Margaret & Irudaya Rajan; Cooper et al., 2002; Scheffler & Arnold, 2019; Zhang et al., 2020). In a market with perfect competition, economic theory suggests that the wage rate varies until it settles at the market equilibrium price where supply is equal to demand. Assuming this economic theory holds, such healthcare workforce supply shortages are only of short-term nature, given that increased prices/wages will lead to the market entry of additional suppliers. This exact phenomenon can be observed in the U.S. healthcare system. In response to the shortage of nurses during the COVID-19 crisis, New York's hospitals raised wages, leading to an increased labor supply as nurses from all over the United States and retired nurses from New York came to the rescue (Young, 2020).
However, social healthcare labor markets are generally more complex. The supply of physicians and nurses only responds to shortages with a significant time lag, due to long training periods. Further, high barriers of entry and regulations define the legal nature of the healthcare labor market—ultimately limiting the number of licensed nurses and physicians. While these factors limit the sustainable supply of working professionals, they also ensure a standardized quality in healthcare provision.
This article will therefore show that increased wages can only be part of a heterogeneous policy plan to address shortages in healthcare labor. In the short run, high-income countries can reduce shortages by importing health professionals from low-income countries. However, this will intensify shortages for the exporting countries and will not solve systemic problems of the health system in the long run. Temporary shortages may also be mitigated by increasing the retirement age of nurses and physicians. Further, the supply of health professionals could be increased by raising the number of medical and nursing graduates. Therefore, effective policies should aim to increase places available in medical and nursing schools, without reducing the quality of teaching or quality of healthcare provision. Apart from financial incentives, policies may also address nonmonetary conditions such as shifts, working environment, office conditions, etc.
First, the current state of the healthcare labor market across OECD countries is reviewed by comparing key labor metrics. Second, economic concepts explaining demand, supply, and shortages in the healthcare industry are presented. Third, these theories are then put into perspective with academic evidence analyzing the return and elasticity associated with wage rates for doctors and nurses. Finally, based on the reviewed data and literature, we draw policy implications to address shortages in the healthcare workforce.
Practice: The Healthcare Labour Market
The International Standard Industrial Classification (ISIC) categorizes health/social work as part of the service sector and defines it as “human health activities, residential care activities (including long-term care), and social work activities without accommodation” (OECD, 2019a). This section reviews the dynamics of the healthcare labor market in OECD countries.
By 2019 about 10% of the workforce was employed in the healthcare industry (OECD, 2019a). Scandinavian countries tend to employ even more health workers (ca. 15%–20%), while Turkey, Chile, and Greece lag behind (ca. 5%). Almost all countries increased their health labor share since 2000 by 2% on average. Therefore, employment growth in the health industry outperforms the overall economy (growth rate: 42% vs. 15%). The health labor market is robust to economic downturns as observed by continuing employment growth during the 2008/2009 recession (Wood, 2011). Experts predict a further surge in the future healthcare workforce (OECD, 2020). However, labor roles will have to adapt to changes in the demographic structure (e.g., long-term care) and technological advances (OECD, 2019b).
A similar and even more significant trend is observable for the number of doctors per 1,000 inhabitants (Figure 1A). On average countries employ 3.5 doctors per 1,000 inhabitants, however, this figure ranges widely from India and China with approximately 2 doctors per 1,000 inhabitants to Western European countries with approximately 4.5 doctors per 1,000 inhabitants (OECD, 2019a). Even though all countries increased the absolute head count of doctors (through migration, medical education, or other programs), some countries such as Israel experienced an even steeper population growth, ultimately resulting in a declining ratio of doctors per 1,000 inhabitants. Nevertheless, OECD countries remain concerned with their amount of doctors especially due to geographic disparities, an aging population, migration of doctors, and aging of the baby boomer doctors (Kirch & Petelle, 2017).
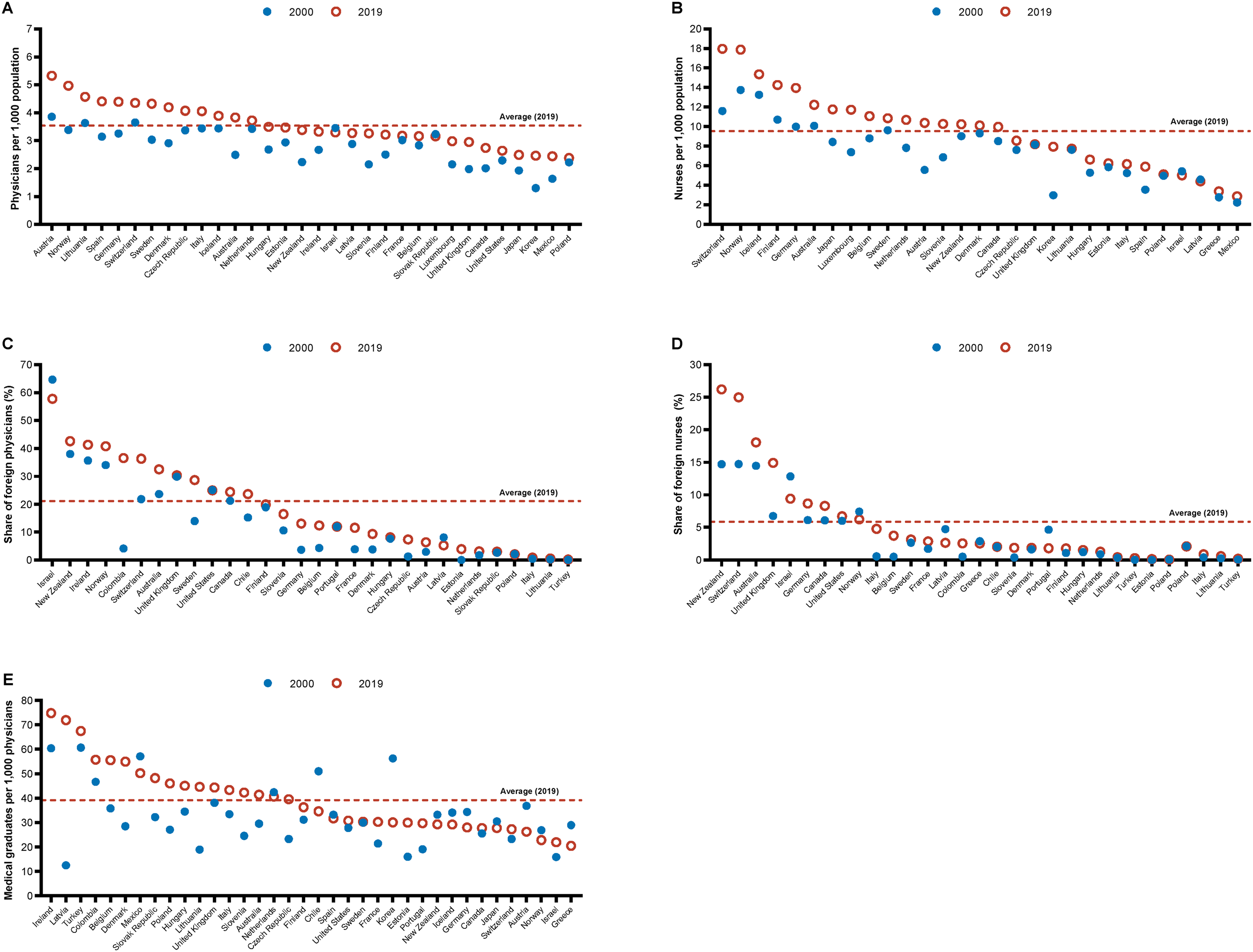
Number of (foreign) physicians, nurses, and medical graduates across OECD countries, 2000 to 2019. Graph A displays the number of physicians and graph B the number of nurses per 1,000 population across OECD countries. Graphs C and D illustrate the share of foreign trained physicians and nurses across countries. Graph E portrays the number of medical graduates per 1,000 physicians. All graphs compare 2000 to 2019 (or nearest year). Data were obtained from OECD statistics (OECD, 2019a).
Urbanization and specialization contribute to unequal geographical distribution of doctors within a country. On average urban areas have 50% more doctors than rural areas (4.3 vs. 2.8 doctors per 1,000 inhabitants) (OECD, 2019a). Health systems employ a range of measures to sustain equal geographical access to medical care. As a result, financial incentives, decentralized education, regulative quotas, and innovative healthcare delivery models are pushed forward (Kirch & Petelle, 2017; OECD, 2019b; Scheffler & Arnold, 2019).
Especially concerning is the demographic structure of doctors—on average a third of medical doctors are older than 55 years (Dellinger et al., 2017; Lee & Weston, 2012; OECD, 2019a). Western European countries, the United States, Australia, Israel, and New Zealand try to solve their shortage of health labor through immigration. In these countries, approximately a third of medical doctors are foreign (Figure 1C). While this might ease the pressure on the domestic healthcare system in the short run, such policies exacerbate shortages in foreign countries. Consequently, increased numbers of medical graduates are necessary to sustain the domestic and global labor market for healthcare professionals (Figure 1E).
Wage rates for doctors vary by specialty and country. Substantial differences in wage rates across countries may further incentivize the migration of doctors to countries offering high wage rates. As expected, doctors usually earn more than the average nonmedical workforce (general practitioners: 2–4×; specialists: 2–6×) (OECD, 2019a).
While there is no internationally accepted coherent classification and definition of a nurse, most of the described trends also hold for the labor market for nursing (Figure 1B and D). On average the number of nurses per 1,000 inhabitants grew from 7.5 to 9.5. (OECD, 2019a) The spread between high- and low-income countries is even higher, ranging from 15 nurses in Western Europe to 1.5 nurses per 1,000 inhabitants in India and Brazil. Shortages in the nurse labor market are also tackled with education and immigration policies. To further ease the shortage of medical doctors, mitigate the growing supply gap, and reduce costs, new intermediary professional roles such as “nurse practitioner” or “physician assistants” were introduced (Cawley & Hooker, 2013; Dehn, 2008). These physician assistants were shown to be cost-effective compared to physicians (van den Brink et al., 2021). Coherently, a systematic review of 11 trials concluded that nurse practitioners in primary and specialized ambulatory care “have equivalent or better patient outcomes than comparators and are potentially cost-saving” (Martin-Misener et al., 2015). Nonetheless, a systematic review of 23 studies concluded that increasing the number of registered nurses in medical and surgical wards improves patient outcomes with the potential for net cost savings and, therefore, cost-effectiveness (Griffiths et al., 2023). However, the ratio between physicians and physician assistants has to be carefully balanced as data reveals a trade-off between high-quality care and faster access to healthcare services exists (Walia et al., 2022).
There are on average 2.7 nurses per doctor in OECD countries. Variations are reliant on the layout of the healthcare system and policies concerning the nurse and physician labor market. Nurses earn on average 10% more than the respective average national wage (OECD, 2019a). It remains unclear whether the wage rate sufficiently compensates nurses and addresses potential shortages. Similar to doctor migration, high wages and living conditions in wealthy countries incentivize the migration flow of nurses to the United States, Western Europe, Australia, and New Zealand (Botezat & Ramos, 2020; Saluja et al., 2020).
Theory: The Demand and Supply for Healthcare Labor and Labor Shortages
“The demand for health workers is derived from the demand for healthcare. The willingness to pay off healthcare purchasers (e.g., the government, private firms, individuals) ultimately drives the demand for the number of health workers to be employed in hospitals, clinics, and public health centres” (Scheffler & Arnold, 2019). Therefore, we will first examine conceptual frameworks to estimate the demand for health, healthcare, and ultimately healthcare workers. Thereafter, we will review models explaining shortages in the healthcare labor market.
Demand for Healthcare Labor
Grossmann postulates that health can be regarded as a good (Grossman, 1972; Grossman & Benham, 1974). On the one hand, it represents a consumption good (used to increase both an individual's utility and increase the time available for work). On the other hand, it is an investment good that deteriorates over time. Patients demand health and consume healthcare services, which are provided by healthcare professionals, to increase their health.
Furthermore, the demand for health professionals is difficult to exactly specify in the given setting, because it is largely determined by the health professional itself. Patients are usually unaware of the type, quantity, and quality they need to restore their health. Therefore, the patient (principal) contracts with a physician (agent) to detect anomalies in the patient's health and subsequentially restore them (“Principal-Agent Theory”) (Bhattacharya et al., 2013). However, the physicians (acting as an agents) also have their own personal and financial interests that are not necessarily aligned with the patient's interests (conflicting interests). Through opportunistic behavior, the physician may thereby specify the type, quantity, and quality of demanded healthcare and thereby the quantity of demanded labor himself. This may lead to phenomena such as supplier-induced demand (Evans; Yip, 1998; Gryttenn & Sørensen, 2001; Labelle et al., 1994; Wennberg et al., 1982). Considering insurance (in all sorts of variations and forms) further complicates matters by generally increasing demand for healthcare (moral hazard) and thereby distorting equilibrium conditions (Bhattacharya et al., 2013).
Moreover, as in any industry, demand also relates to the productivity of labor. Meaning that when more healthcare services are demanded, physicians are more productive. For example, during winter more people demand healthcare than during summer due to seasonal diseases (e.g., influenza) leading to more productivity on the supply side. Nevertheless, the relationship between labor and productivity—the productivity function—is hard to specify in the healthcare setting, as many unsatisfying attempts show. Therefore, the relationship between input factors (e.g., physicians, nurses, drugs, diagnostic machinery, etc.) and the output (e.g., health) is yet unknown.
To decide whether to employ an additional worker, a firm (e.g., doctor's office, hospital) will consider the resulting additional output that the worker generates (Marginal Physical Product). The relationship is influenced by the law of diminishing marginal returns. The total output of all workers in the firm is then defined as the Total Physical Product. Multiplying these production factors with the market price of the units produced gives us the marginal and total revenue curves. A firm will maximize its revenues by employing health professionals up to the point where their marginal revenue equals the marginal cost of employment. However, the marginal revenue is difficult to estimate, given that there is no general price for the output produced by a healthcare professional. Even substituting health workers does not lead to a conclusive solution, since the substitutability is difficult to estimate without a known production function. Trying to do so mostly leads to the result that the substitution of physicians with nonphysicians and other capital is inelastic (Gaynor & Town, 2011; Gunning & Sickles, 2011; Vita, 1990). In summary, estimating the demand function may fail due to an ambiguous definition of the output, the production function, the marginal revenue product (MRP), and the labor level. To complicate it even further, all of these factors are accelerated by the unobservable and unverifiable effort of health workers.
Defining the production function of healthcare is further convoluted by the hierarchical and team structure of the labor force. The specialization and long training process of medical staff result in collaboration on horizontal (same hierarchy level), vertical (across different hierarchy levels), interdisciplinary (across different specialties), and interprofessional (across different professions) vectors. Defining the production function of a single nurse or physician of such teams is hence virtually impossible.
Supply of Healthcare Labor
Estimating the supply curve of healthcare labor is similarly complex. Overall, it is observed that wage rate and supply are positively correlated. No backward bending curve is observed in practice, even though theoretically it is reasonable to argue for an increased weighting of an individual's leisure time on the respective individual's utility function with higher wage rates. The supply curve is further influenced by the entries and exits of healthcare professionals, medical education, and the migration of health workers.
Market Equilibrium
The market for healthcare labor is in an economic equilibrium when the marginal supply of employees is equal to the marginal demand for employees (Figure 2A).
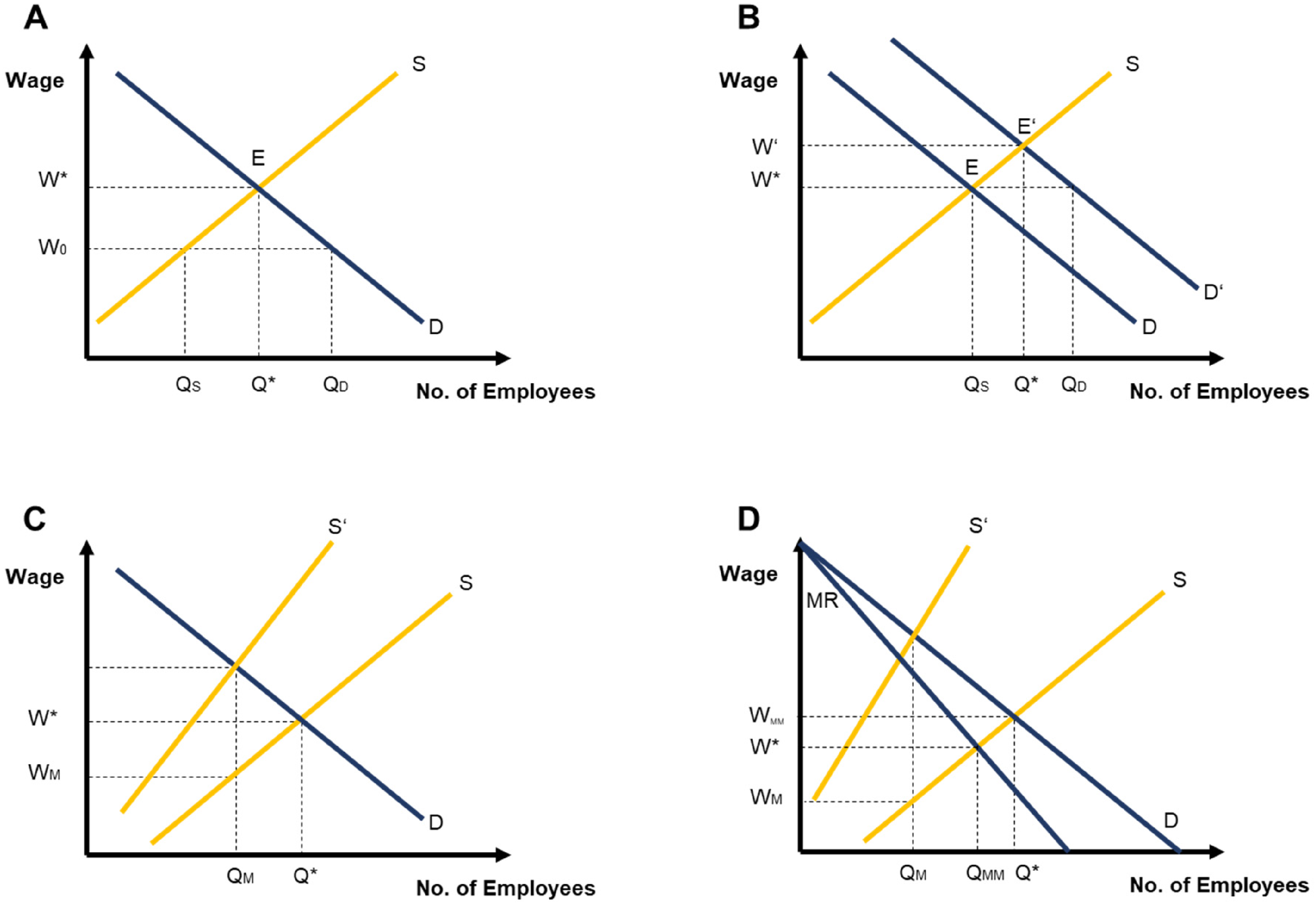
Theoretical concepts of workforce shortages in the healthcare market. Graphs display theoretical concepts of demand (blue curves marked with D) and supply (yellow curve marked with S) for healthcare workers under different market conditions. Graph A illustrates labor shortages as a result of low wages. Graph B displays shortages caused by a lag in workforce supply. Graph C portrays labor shortages under monopoly power of nurses and physicians. Graph D visualizes market dynamics with monopsony buyers, for example insurers or National Health Service in the United Kingdom, and monopoly suppliers, for example physician associations or unions.
Socially Perceived Shortage
The previously cited newspaper headlines in the introduction, however, may refer to the socially desired equilibrium. Therefore, the labor market may be in an economic equilibrium, but in a social disequilibrium. This means that the socially desirable quantity of doctors and nurses may be higher than the economic equilibrium suggests, leading to a socially perceived shortage.
Shortage Caused by Low Wages
A shortage may also occur when the current wage rate is below the equilibrium wage (W0 > W*). At this rate more employees are demanded than supplied, resulting in a shortage of employees equal to QD–QS (Figure 2A).
Shortage Caused by Lagging Supply
A shortage in the supply of labor may also occur due to quick/dynamic shifts in demand, whereas supply takes longer to adapt (Arrow & Capron, 1959; Blank & Stigler). For example, during the recent COVID-19 crisis many more nurses and physicians were demanded than before or available. However, strict regulations and a lengthy education and training process cause the supply of doctors and nurses only to increase in the long run (3–5 years). Meanwhile, the healthcare system experiences a shortage of labor equal to QD–QS (Figure 2B).
Shortages Under Demand Monopoly
Above we considered an efficient market, given that there are numerous employees and employers that all act independently. However, in many countries nurses and physicians are organized in associations or unions, thereby forming a monopoly. The resulting monopoly requires employers to pay equal wages for similar positions. Consequently, differential wages for an additional employee are very costly—the additional wage premium has to be paid to all employees resulting in a shift of the supply curve as the total expenditure increases. While healthcare firms want to employ Q* employees, going beyond QM employees would decrease their profits. Consequently, there is a shortage equal to Q*–QM (Figure 2C).
Shortages Under Demand Monopoly and Supply Monopsony
Furthermore, in many countries, a monopsony is responsible for the purchasing of healthcare, for example, National Health Service (NHS) in the United Kingdom. Figure 2D shows the characteristics of a market where a monopoly seller faces a monopsony buyer. In this case, the monopsony's demand curve is equal to its average cost (= MRP) and defined by the marginal revenue. At the new quantity between the monopsony and monopoly (QMM), the shortage of labor is diminished by QMM–QM. This shows monopsony buyers can be encountered with labor associations and labor bargaining. Nevertheless, a shortage of labor persists by Q*–QMM.
Evidence
Theoretic frameworks suggest that simply raising the wage rate for healthcare professionals could increase the labor supply and thereby reduce shortages if income is found to be elastic. Therefore, this section will (1) review the evidence on the personal rate of return for healthcare professions and (2) the wage elasticity for nurses and physicians. In that respect, nonfinancial incentives and intrinsic motivation are discussed as key determinants shaping labor supply.
Personal Rate of Return
Literature examining the wage rate for healthcare professionals and financial and nonfinancial incentives is mainly coherent with observed wage levels. “Wages vary with the cost of learning the business” (Adam Smith) also holds for the medical profession (Bhattacharya et al., 2013). Investigators regularly try to estimate the internal rate of return (IRR) of a professional career in medicine. The IRR calculates the discount rate at which the resulting net present value (NPV) of all future cash flows is equal to 0. If the IRR is larger than an individual's rate of return, then one should take the decision (investment) (Bhattacharya et al., 2013). An individual's overall rate of return can be split into two parts. The financial IRR values all monetary cash flows, while the nonfinancial IRR considers social (nonmonetary) benefits from practicing medicine, for example, benevolent behavior.
Table 1 provides an overview of return calculations for healthcare professionals from the United States and the United Kingdom. Even though results vary depending on the examined time frame, country, and circumstance, a few common trends arise:
There is a clear positive rate of return for medical education in the United States (14%–17%) and the United Kingdom (23%–27%). The reason for this observed country difference remains unclear. On the one hand, medical education is shorter and less expensive for british medical doctors. On the other hand, physicians tend to earn more in the United States. In contrast, the education of nurses remains disperse across countries. In the United States, nurses typically obtain a bachelor's degree. In European countries, for example, in Germany, nurses attain their license after completing a traineeship with a total duration of 3 years. Given the fragmentation and complexity of the various undergraduate, graduate, and training programs for nurses, calculating a rate of return for nursing education remains challenging (Baker et al., 2021; van Kraaij et al., 2023). Overall evidence points toward a lower rate of return for nursing education than medical school graduates. Rate of returns is higher for specialist doctors than general practitioners (Roth, 2012). This indicates additional training, effort, and specialization is valued more highly. The results are consistent with the wage difference found between specialists and general practitioners. Accordingly, higher wages are paid for specialized nurses that attained additional qualifications and certificates than general nurses, for example, those with additional qualification in wound care or those working in intensive care units. However, significant differences between subspecialities exist (Mead et al., 2020). There is a gender gap in the rate of return (Blackaby et al., 1999), as the economic wide gender pay gap persists in medicine. A systematic review of 43 studies found across almost all studies, female doctors earned significantly less than their male counterparts even after adjusting for hours worked, demographic, and work-related factors (Hoff & Lee, 2021). There appears to be a declining rate of return for medical education over time. For instance, the IRR of orthopedic surgery training has declined from 25% in 1989 to 15% in 2019 (Mody et al., 2021). The authors attribute this to the rising cost of medical education and student loan debt.
Rate of Returns for Medical Professions.
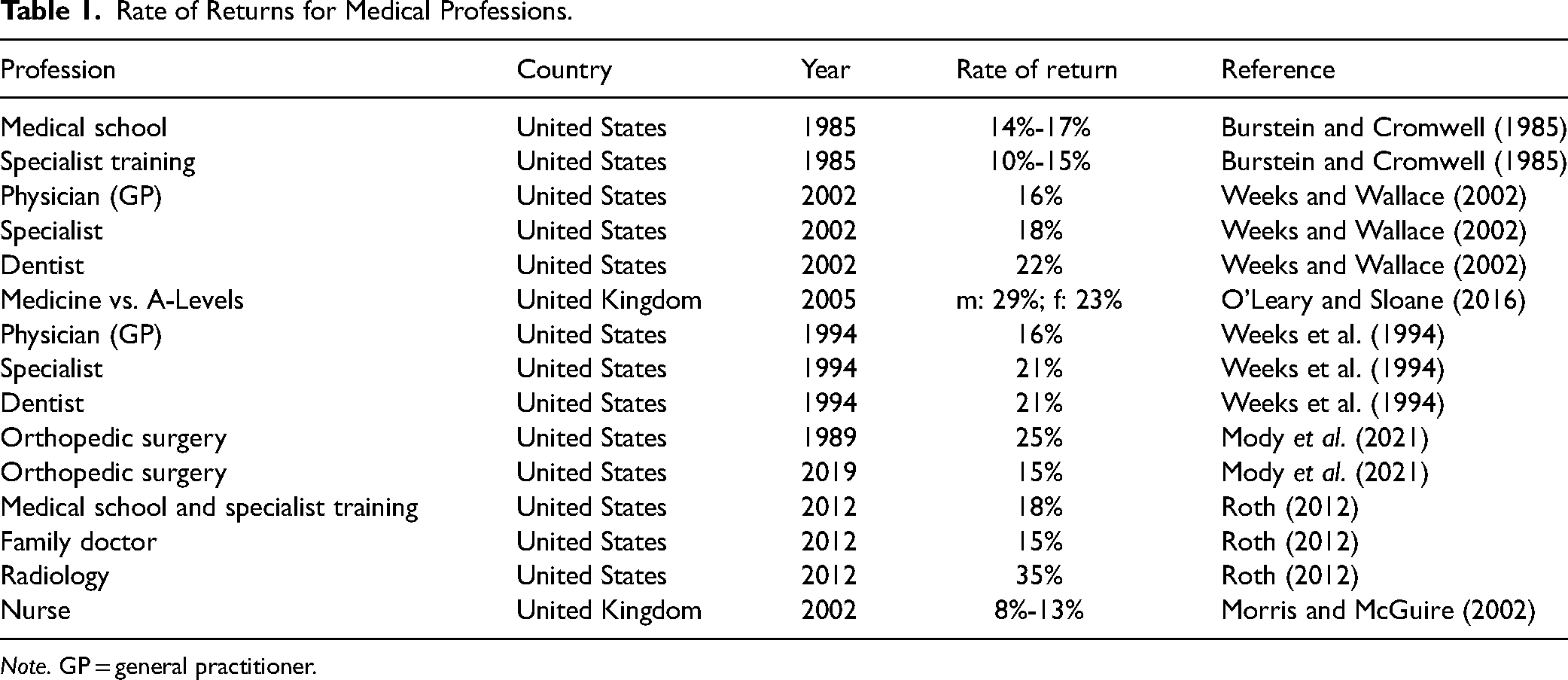
Note. GP = general practitioner.
Nevertheless, limitations exist in the provided evidence. Variables such as economic, social, and demographic factors may have been omitted and bias the results. It is especially necessary to control for factors such as worked hours, retirement differences, and differences in skill. Bhattacharya controlled for these factors and found that they only account for approximately 50% of the IRR (Bhattacharya, 2005). The remaining variation must therefore be explained by barriers of entry to becoming a physician and subsequently a specialist doctor (Bhattacharya et al., 2013). Many countries such as the United States, the United Kingdom or Germany require doctors and nurses to obtain licenses in order to practice (Michaeli et al., 2022b). Given that these licenses can only be obtained through medical/nursing school, limited enrollment is a key hurdle shaping the long-term supply of medical professionals. This main barrier of entry presumably explains the remaining variation of the excess IRR. Furthermore, migration is limited by differences in educational standards and licensing examinations. While medical and nursing licenses are similar and acknowledged by most Western European countries, the United Kingdom requires most foreign physicians and nurses to pass their national licensing exams. Similarly, nurses must pass a certification exam and obtain a state license to register and work in the United States. Although these requirements safeguard the quality of healthcare provision, that may be regarded as an entry barrier limiting supply of healthcare workers.
Income Elasticity
If we assume that labor shortages in the healthcare market are caused by inadequate wages (as previously explained), theory consequently suggests an effective policy would increase wages to stimulate the supply of labor. However, this hypothesis only holds if the labor supply curve is elastic to wage increases. Elasticity measures the percentage change in the quantity supplied for a one percentage change in the wage rate. In this case the elasticity (wage response) consists of the substitution effect (leisure substitutes worked hours) and the income effect. Only if doctors and nurses value the additional wage rate more than their leisure time, an increased wage rate results in a higher supply. This section examines the academic evidence of wage elasticity for doctors and nurses.
Physicians
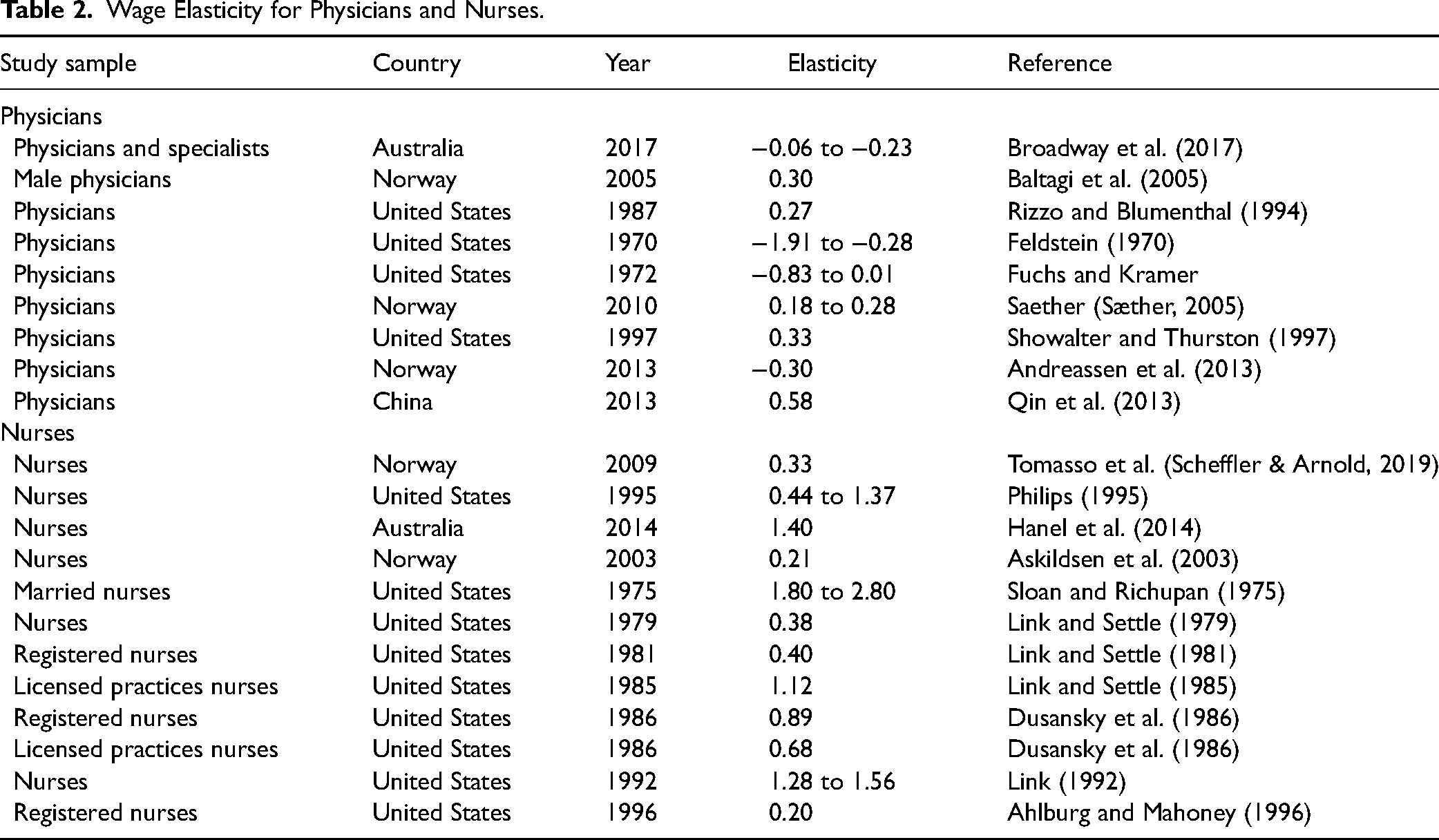
Evidence in Table 2 demonstrates that doctors are comparatively unresponsive to changes in the wage rate. The substitution effect is minor in magnitude (0.3) and the income effect is almost negligible (−0.18). Sather (2010) and Showalter & Thurston (1997) found that the substitution effect is larger for self-employed physicians in the United States and Norway, while hospital physicians seem to be less responsive to wage changes (Sæther, 2005; Showalter & Thurston, 1997). In summary, changes in the wage rate cannot sufficiently increase the supply of physician labor. The working environment and conditions are suggested to have a larger effect on physician satisfaction and, henceforth, the supply of labor (Michaeli et al., 2022c; Michaeli et al., 2022a; Perez-Dominguez et al., 2021; Scott et al., 2011) However, generalizable and policy shaping evidence is difficult to establish in that regard.
Wage Elasticity for Physicians and Nurses.
Nurses
Even though there is extensive literature on wage elasticity for the nursing profession, no coherent conclusion arises. Elasticity values range from 0.2 (inelastic) to 2.8 (highly elastic) depending on the studied nurse characteristics, study design, country, and time period. Studies that found elasticities greater than 1 examined married nurses or had an unusual study design/year (Askildsen et al., 2003; Link 1992; Phillips, 1995). Considering the remaining evidence, it is therefore reasonable to conclude that nurses’ wages are inelastic (0.5) but greater than physicians’ wage elasticity.
Inelastic income suggests that nonfinancial factors are strongly weighed by nurses. Job satisfaction gained through promotion and education is found to be valued more by nurses than income alone (Shields & Ward, 2001). “Relations with colleagues, degree of autonomy, or intrinsic rewards” (Hanel et al., 2014) are further nonfinancial determinants that nurses consider (Clark, 2001). For example, a study of intensive care unit nurses found higher satisfaction rates among nurses that reported higher levels of nurse–physician collaboration, for example, nurses that were closely integrated in care decision-making processes with physicians (Baggs & Ryan, 1990). Precisely positive relationships with colleagues, the degree of autonomy/span of control, and organizational support, for example, support by supervisors and colleagues, we repeatedly identified as the key determinants of nurse satisfaction (Lee & Cummings, 2008; Utriainen & Kyngäs, 2009). Further, improvements in nurses’ work environment are not only a key factor to reduce the burnout and turnover rate among nurses’ but also to increase patient satisfaction and outcome (Vahey et al., 2004). Labor supply could be increased by raising the quality of such nonpecuniary factors. Several investigators found shift work to be a distinguishing (often negatively perceived) characteristic of the nurse profession (Askildsen et al., 2003; Di Tommaso et al., 2009; Hanel et al., 2014; Lagarde & Blaauw, 2009; Lagarde & Blaauw, 2014). Furthermore, it has been proven in several instances that intrinsic motivation can be harmed by financial incentives (also known as “motivation crowding out”) (Frey & Jegen, 2001; Frey & Oberholzer-Gee, 1997; Titmuss, 1970). Heyes delivered evidence for this hypothesis to hold in the nursing labor market as well (Heyes, 2005). He found the current wage structure to be inefficient and noted: “increasing wages might attract the ‘wrong sort’ of people into the profession” (Heyes, 2005).
Discussion: Ways Forward
We argued that the demand for health labor can be estimated through the demand for health services which in turn can be calculated using the demand for health. Health insurance, the principal-agent relationship and supplier-induced demand further complicate the market for healthcare workforce. Estimating the demand and supply curve is also multifaceted due to an unknown production function, unknown productivity, measurement errors, intrinsic motivation (effort), and the hierarchical specialized team structure present in hospitals. Theoretical models are therefore built on a fragile basis. According to simple macroeconomic equilibrium models, supply shortages may be a result of too low wages, supply lagging behind demand and social perception. In theory, monopsony buyers (e.g., NHS) exacerbate these shortages but can be faced with monopsony sellers (e.g., labor associations). Henceforth, we require more sophisticated economic theories and models capturing international workers to describe the market for healthcare workforce.
Literature analyzing the rate of return associated with medical and nursing education shows four main results: (1) there is a consistent positive return to medical education; (2) the rate of return is lower for nursing education than for medical school graduates; (3) the rate of return is higher for specialist doctors than for general practitioners; and (4) the gender wage gap persists in medicine. Bhattacharya argues that the excess IRR can be in half explained by omitted variables such as worked hours, differences in skill, and retirement and in half by barriers of entry. While medical licenses ensure a standardized high quality in the provision of healthcare, it also limits labor supply. Therefore, scholars theorized that wages could be lowered by increasing labor supply through a higher number of medical school graduates.
In contrast, if we assume that wage rates are the major cause of labor shortages in the healthcare market, an effective labor policy that increases wage rates would result in a growing supply of labor. However, this hypothesis only holds if the labor supply curve is elastic to wage increases. Evidence shows that physicians are comparatively unresponsive to changes in the wage rate (substitution effect: 0.3 and income effect: −0.18). Wage elasticity for nurses is greater but also inelastic (0.5). In summary, changes in the wage rate cannot sufficiently increase the supply of health professionals. Nonpecuniary factors such as working conditions, job satisfaction, and intrinsic motivation are at least equally important as the financial incentive. Healthcare employers must recognize improving nonpecuniary labor aspects, for example, shift work, social recognition, holidays, working hours, labor benefits, training options, and career development programs, are key components of modern healthcare workforce employment and retention. Employers should further aim to advance the “social” factors valued by the modern medical workforce (particularly nurses), for example, autonomy, quality of interactions with colleagues, and flat vertical hierarchy in the organization that honors and values the entire team.
Conclusion
In conclusion, increased wages can only be part of a heterogeneous policy plan to address shortages. Migration and retirement levels of health professionals can temporarily mitigate labor shortages but rarely change the underlying systemic issues. Increasing the amount of places available in medical and nursing schools while also improving, both, financial and nonfinancial incentives for employees are structural policies worth exploring.
Footnotes
Acknowledgement
The authors are grateful for comments and suggestions received by the editor of the journal and the anonymous referees. None of the additional contributors received any compensation.
Author Contributions
DTM was involved in concept and design, drafting of the manuscript, administrative, technical, or material support, and study supervision. All authors contributed to critical revision of the manuscript for important intellectual content.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Sharing Statement
All data used in this study were in the public domain. All data relevant to the study are included in the article or uploaded as supplementary information.
Funding
The authors received financial support for the research, authorship, and/or publication of this article. Outside of this work T.M. was supported by the German Cancer Research Center (DKFZ) Clinician Scientist Program and D.T.M. was supported by the Federal Ministry of Education and Research (BMBF) Young Scientist Award and the German Cancer Society's (DKG) Young Talent Award.