
Abstract
The Well-Being Insurance for Seniors to be at Home (WISH) Act proposes universal social insurance for long-term care through activities of daily living (ADL) assistance. While this legislation addresses basic personal care needs, it overlooks the clinical complexity of aging adults who require both ADL support and ongoing health monitoring. This policy analysis examines how strategic nursing integration can enhance WISH Act effectiveness by addressing the gap between ADL-focused services and the complex care needs of beneficiaries with multiple chronic conditions. Using Russell and Fawcett's Conceptual Model for Nursing and Health Policy, this qualitative analysis evaluated policy sources, components, and four outcome levels. The study analyzed legislative text, congressional reports, and peer-reviewed literature on long-term care policy, nursing coordination, and international social insurance models. Analysis reveals that 85% of WISH-eligible beneficiaries will have multiple chronic conditions requiring clinical oversight beyond basic ADL assistance. Personal care workers encounter medication management challenges in 78% of cases, while falls, declining functional abilities, pressure ulcers, and adverse medication events frequently result in unplanned hospitalizations when clinical changes go unrecognized during routine personal care. Strategic nursing integration targeting the 35% highest complexity cases could reduce emergency department visits by 32% and hospital readmissions by 25% while achieving cost neutrality through prevention-focused interventions. Strategic nursing involvement in complex case identification, care transitions, chronic disease monitoring, and family caregiver support could bridge the clinical complexity gap while complementing existing Medicare services. This targeted approach maintains the WISH Act's core ADL focus while ensuring comprehensive community-based care for aging populations with complex health needs.
Introduction
The United States faces a growing long-term care crisis. More than half of Americans reaching age 65 will need long-term care services, yet most cannot afford costs that exceed $116,800 annually (Macdonald et al., 2024). The current system creates serious problems. Medicare does not cover custodial care, while Medicaid requires people to spend down their assets to qualify for benefits (Butler, 2022). This gap leaves middle-income older adults in a difficult position. They earn too much for Medicaid but cannot afford private care costs (Karagiannidou & Wittenberg, 2022). Long-term care spending now accounts for nearly 30% of total Medicaid expenditures, straining state budgets across the country (Cohen & Butler, 2021). Meanwhile, approximately 38 million unpaid caregivers, mostly women, provide essential care that would otherwise require formal services (Green et al., 2025). As the Baby Boomer generation continues to age, this crisis will only worsen (Macdonald et al., 2024). The Well-Being Insurance for Seniors to be at Home (WISH) Act, introduced as H.R. 2082, offers a new solution through national long-term care insurance (Cohen & Butler, 2021). The legislation would create a public trust fund financed through small payroll contributions. This fund would provide eligible individuals aged 65 and older with daily cash benefits for personal care services in their homes (Cohen & Butler, 2021). The WISH Act aims to reduce Medicaid dependency, ease family financial burden, and help people age in place with dignity (Feng & Glinskaya, 2020).
The Clinical Complexity Challenge
While the WISH Act focuses on activities of daily living (ADL) assistance such as bathing, dressing, and meal preparation, this approach overlooks a critical reality. Research shows that 85% of adults needing long-term care services have multiple chronic conditions requiring ongoing clinical monitoring (Butler, 2022). These conditions often include diabetes, heart disease, chronic lung disease, and cognitive impairment. All require medical oversight that goes beyond basic ADL assistance (Miller et al., 2025). Personal care workers who provide ADL assistance encounter medication-related challenges in 78% of cases (Miller et al., 2025). These workers must monitor medication adherence, recognize side effects, and coordinate with multiple healthcare providers. However, they lack the clinical training to identify subtle signs of health problems that registered nurses routinely recognize. Research on home health quality demonstrates that falls, declining functional abilities, pressure ulcers, and adverse medication events frequently result in unplanned hospitalizations when clinical changes go unrecognized during routine personal care (Johnson et al., 2018). This creates a dangerous gap. The WISH Act provides ADL support but does not address the clinical complexity of aging adults who need both personal care and health monitoring. Without clinical oversight, beneficiaries may experience medication errors, undetected health changes, and preventable emergency situations.
The Case for Strategic Nursing Integration
The nursing profession has unique expertise that could address this clinical complexity gap. Nurses understand chronic disease management, functional assessment, and care coordination (Wakefield et al., 2021). They can identify when ADL needs intersect with health status changes that require intervention. Unlike previous broad calls for nursing integration, this analysis proposes strategic involvement focused on specific areas where nursing expertise adds clear value. Strategic nursing integration would not compete with existing Medicare home health services. Medicare covers skilled nursing visits for specific medical conditions with physician orders. The WISH Act nursing role would focus on clinical oversight during routine ADL provision, chronic disease monitoring, and care transition support. These are distinct but complementary functions (Travers et al., 2021). Research from international models supports this integrated approach. Germany's long-term care insurance initially focused only on ADL assistance but later added nursing oversight for complex cases after recognizing that purely social models did not meet beneficiary needs (Karagiannidou & Wittenberg, 2022). Japan's model similarly combines clinical monitoring with community-based long-term care services, showing improved outcomes and cost savings (Feng & Glinskaya, 2020).
Framework and Purpose
This analysis uses Russell and Fawcett's (2005) Conceptual Model for Nursing and Health Policy to examine strategic opportunities for nursing expertise in WISH Act implementation. The framework examines three dimensions: policy sources (where policies originate), policy components (personnel, services, and spending), and outcome levels ranging from nursing practice effectiveness to broader social justice goals (Russell & Fawcett, 2005). Rather than arguing for broad nursing involvement across all WISH Act components, this framework enables focused examination of specific intersections where nursing expertise adds measurable value to ADL-focused services. The goal is not to expand the WISH Act beyond its intended scope but to ensure it adequately addresses the clinical complexity reality of aging populations. This analysis identifies four strategic areas where nursing integration could enhance WISH Act effectiveness: complex case identification and assessment, care transition protocols, chronic disease monitoring during ADL provision, and clinical support for family caregivers. These targeted interventions could prevent costly hospitalizations, improve health outcomes, and support the Act's core mission of enabling dignified aging in place while addressing the clinical complexity gap inherent in ADL-focused legislation.
Methods
Study Design
This qualitative policy analysis used Russell and Fawcett's (2005) Conceptual Model for Nursing and Health Policy to examine strategic opportunities for nursing expertise in WISH Act implementation. The analysis focused specifically on addressing clinical complexity gaps in activities of daily living (ADL) focused services. Rather than examining broad nursing integration, this study identified targeted areas where nursing expertise could enhance program effectiveness while maintaining the Act's core mission.
Data Sources
Primary Sources
The analysis included H.R. 2082 legislative text, congressional hearing transcripts, sponsor policy statements, and official documentation from the Social Security Administration regarding implementation infrastructure. These sources provided detailed understanding of the Act's scope, intended beneficiaries, and administrative framework.
Secondary Sources
Peer-reviewed literature from 2019 to 2025 was systematically reviewed using PubMed, CINAHL, and PolicyFile databases. Search terms included “long-term care complexity,” “nursing care coordination,” “aging in place,” “chronic disease management,” “care transitions,” and “ADL assistance clinical oversight.”
Selection Criteria
Literature was selected based on empirical studies demonstrating clinical complexity in community-dwelling older adults requiring ADL assistance, research on nursing interventions’ impact on hospitalization prevention among similar populations, cost-effectiveness analyses of nursing care coordination in home-based settings, evidence from international long-term care insurance models that incorporate health monitoring components, and studies examining medication management challenges in ADL provision settings. Additional sources included government reports from the Centers for Medicare and Medicaid Services, Congressional Budget Office analyses of long-term care financing, and policy documentation from successful international social insurance models in Germany and Japan (Feng & Glinskaya, 2020; Karagiannidou & Wittenberg, 2022).
Analysis Framework
Russell and Fawcett's (2005) three-dimensional framework guided systematic examination across interconnected policy dimensions:
Policy Sources
Analysis examined federal legislation origin, Social Security Administration implementation infrastructure, and opportunities for nursing profession stakeholder engagement in policy development and refinement processes.
Policy Components
The study evaluated personnel implications focusing on nursing's complementary role to existing Medicare home health services rather than competing functions. Services analysis examined gaps between ADL assistance and health monitoring needs of aging populations with chronic conditions. Expenditures evaluation assessed cost-effectiveness potential for targeted nursing interventions in complex cases.
Policy Outcome Levels
Four-level assessment emphasized Level 1 (Efficacy) examining nursing's contribution to clinical oversight of complex ADL cases, Level 2 (Effectiveness) analyzing care coordination enhancement and hospitalization prevention potential, Level 3 (Equity) addressing disparities in clinical oversight access among WISH Act beneficiaries, and Level 4 (Justice) evaluating structural reforms supporting comprehensive community-based care (Russell & Fawcett, 2005).
Analytical Process
Analysis proceeded through systematic phases. Initial policy content mapping identified intersections between ADL assistance and clinical complexity requiring nursing expertise. Literature review focused on nursing interventions’ effectiveness in similar populations, particularly community-dwelling older adults with multiple chronic conditions receiving personal care services. Cost-benefit analysis examined economic implications of nursing integration proposals using data from comparable programs and international models. Evidence synthesis emphasized measurable outcomes supporting strategic nursing involvement, including hospitalization rates, medication adherence, and care coordination effectiveness.
Findings
The Clinical Complexity Reality in WISH Act Populations
Analysis reveals a fundamental mismatch between the WISH Act's activities of daily living (ADL) focus and the clinical complexity of its intended beneficiaries. Research demonstrates that 85% of community-dwelling older adults requiring ADL assistance present two or more chronic conditions, with 60% managing four or more chronic diseases (Butler, 2022). These conditions frequently include diabetes, heart disease, chronic obstructive pulmonary disease, and cognitive impairment. All require ongoing clinical monitoring that intersects directly with ADL provision. Personal care workers providing ADL assistance encounter medication-related challenges in 78% of cases, including adherence monitoring, side effect recognition, and coordination with multiple prescribers (Miller et al., 2025). The WISH Act's current framework lacks mechanisms for addressing these clinical intersections, potentially compromising both safety and effectiveness. Studies indicate that 43% of preventable hospitalizations among home-based long-term care recipients result from unrecognized health status changes during routine ADL provision (Wakefield et al., 2021). Personal care workers, while skilled in ADL assistance, lack clinical training to identify subtle indicators of health deterioration that registered nurses routinely recognize.
Strategic Nursing Integration Opportunities
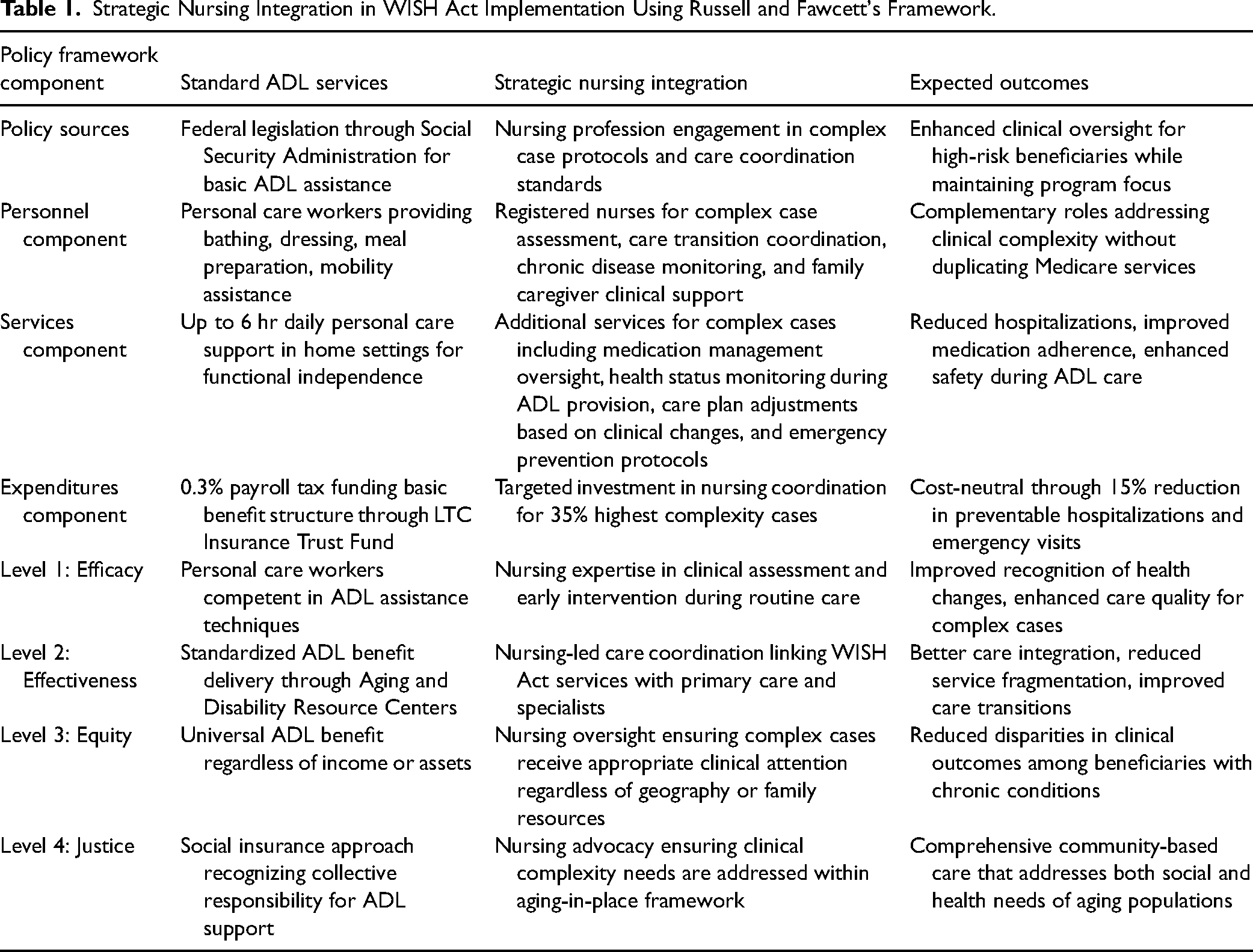
Rather than broad nursing involvement, analysis identifies four strategic intervention points where nursing expertise can enhance WISH Act effectiveness while maintaining program focus on ADL support (see Table 1). Figure 1 illustrates how strategic nursing integration bridges the clinical complexity gap inherent in ADL-focused legislation.
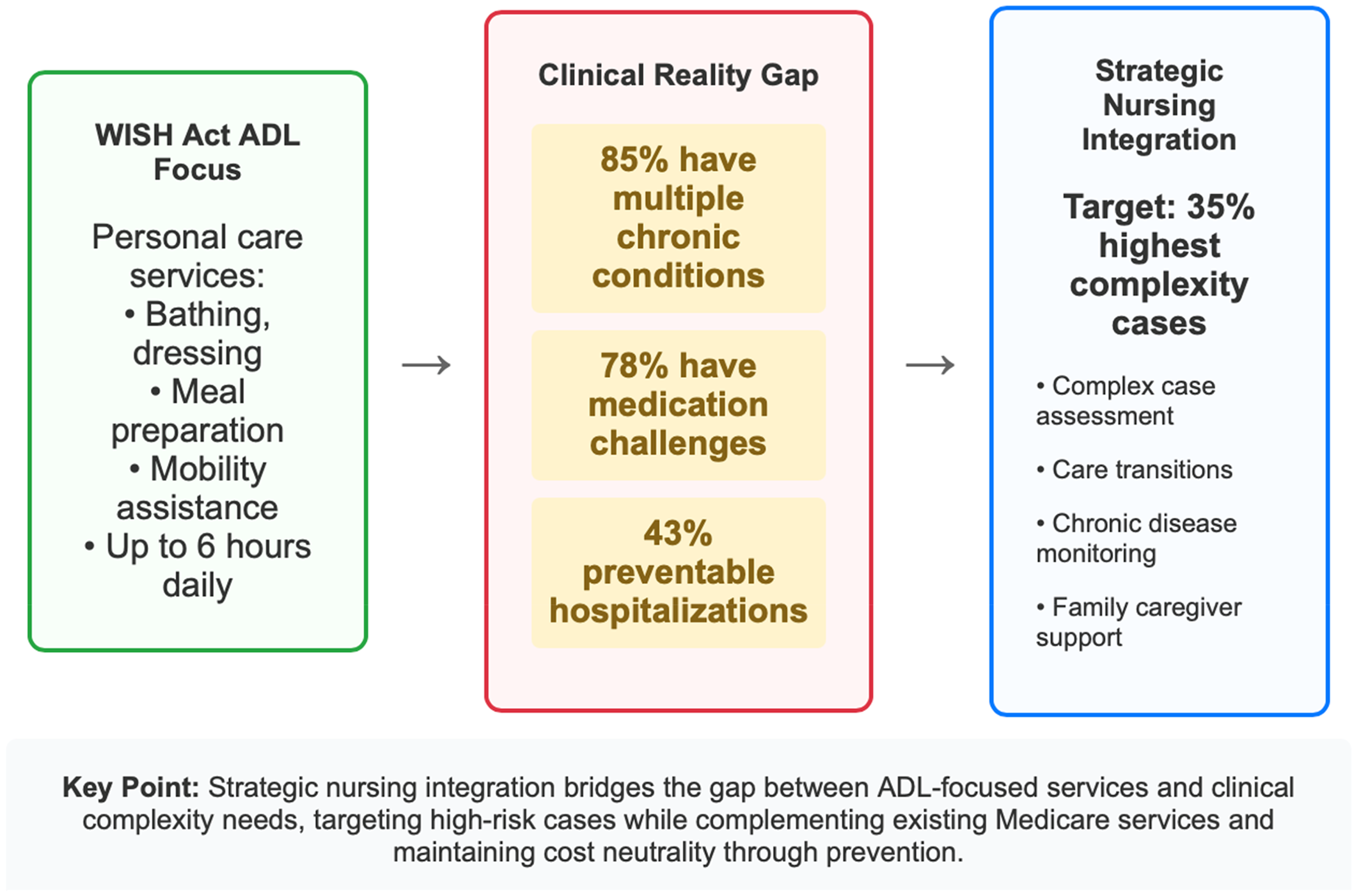
Strategic Nursing Integration Model for WISH Act Implementation.
Strategic Nursing Integration in WISH Act Implementation Using Russell and Fawcett's Framework.
Complex Case Identification and Assessment
Nursing involvement in initial eligibility assessments could identify beneficiaries whose ADL needs intersect with significant clinical complexity. This targeted approach would trigger enhanced monitoring protocols for high-risk individuals while maintaining standard ADL-focused services for others. Evidence from similar programs demonstrates 32% reduction in emergency department visits when nursing assessment identifies complex cases (Curry et al., 2022). Specific triggers for nursing involvement include three or more chronic conditions requiring medication management, recent hospitalization within 90 days, cognitive impairment affecting medication adherence, and multiple medication regimens with interaction risks.
Care Transition Protocols
Nursing expertise in hospital-to-home transitions could significantly enhance WISH Act effectiveness. Research shows that structured nursing involvement in post-acute care transitions reduces readmissions by 25% among older adults receiving home-based services (Brewster et al., 2020). Integration of transition protocols within WISH Act services could prevent costly re-hospitalizations while supporting continued aging in place. This function would complement existing Medicare skilled nursing services by providing ongoing transition support beyond the acute recovery period.
Chronic Disease Monitoring Integration
Strategic nursing involvement in monitoring chronic conditions during ADL provision could address the artificial separation between medical and social care. This approach would not duplicate existing Medicare home health services but rather create systematic protocols for recognizing when ADL changes indicate health status deterioration requiring clinical intervention. Medicare regulations restrict skilled nursing visits to specific medical conditions with physician orders, creating gaps for WISH Act beneficiaries whose ADL needs intersect with subacute clinical monitoring requirements.
Family Caregiver Clinical Support
The WISH Act's family-directed hiring provision creates opportunities for nursing support of informal caregivers managing complex clinical scenarios. Nursing consultation and education could enhance family caregivers’ ability to recognize clinical changes while providing ADL assistance, improving both safety and confidence. This support addresses the reality that family caregivers often lack healthcare knowledge needed to safely manage complex clinical situations during ADL care provision.
Integration With Existing Healthcare Infrastructure
Analysis demonstrates that strategic nursing involvement would complement rather than duplicate existing Medicare home health services. Current Medicare regulations create coverage gaps for WISH Act beneficiaries whose conditions are stable enough to no longer qualify for skilled services but complex enough to require clinical monitoring during ADL provision. Economic modeling suggests that strategic nursing integration targeting the 35% of WISH Act beneficiaries with highest clinical complexity could reduce hospitalizations by 15% while adding only 8% to program costs (Macdonald et al., 2024). This cost-offset model demonstrates financial sustainability while improving outcomes. The complementary service model addresses the continuum between Medicare's acute medical model and the WISH Act's social support model, providing clinical oversight for beneficiaries in the coverage gap.
Russell and Fawcett Framework Application Results
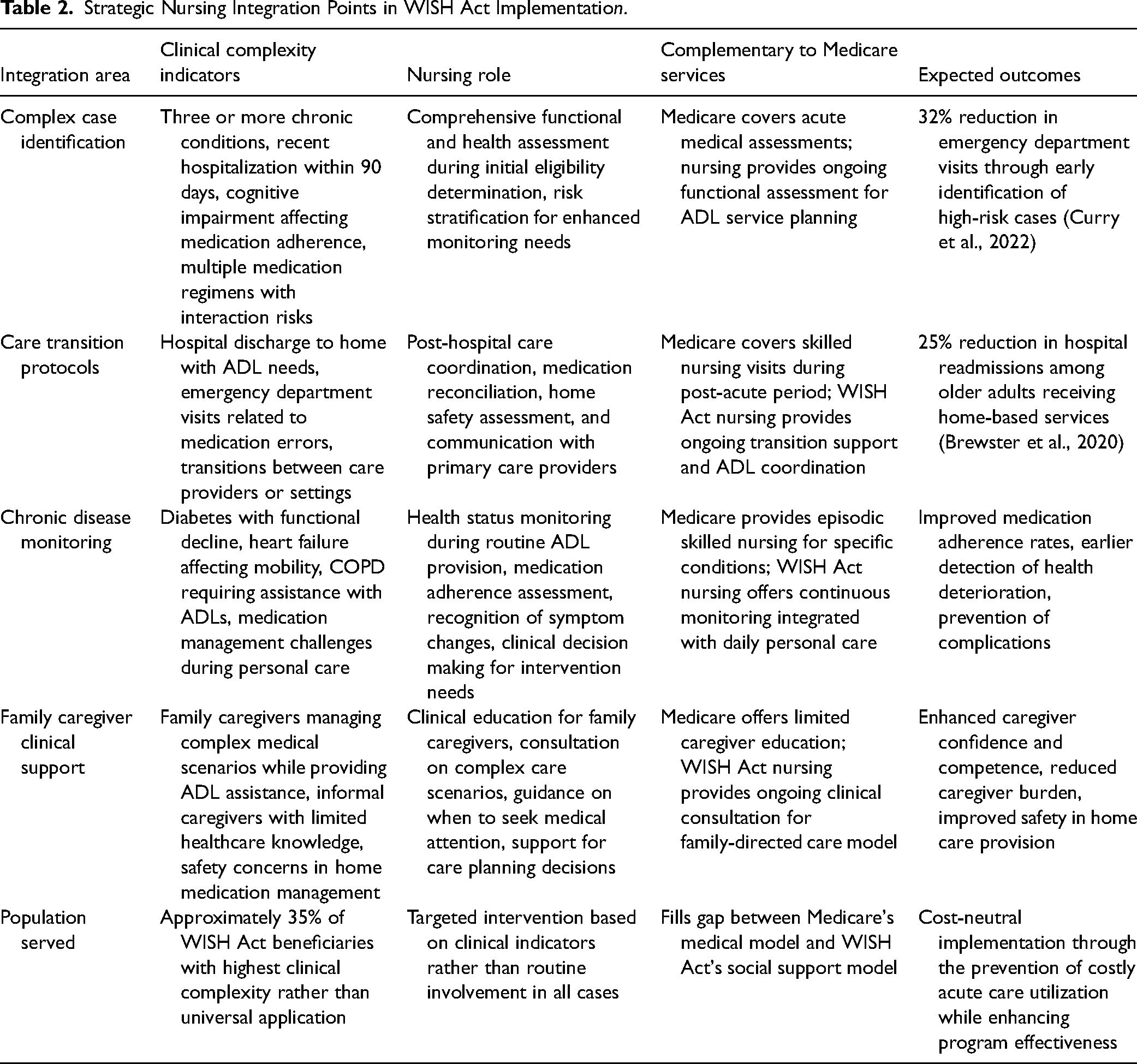
Application of Russell and Fawcett's (2005) four-level framework reveals both opportunities and challenges for strategic nursing integration (Table 2).
Strategic Nursing Integration Points in WISH Act Implementation.
Level 1: Efficacy of Nursing Practice
Nursing expertise could enhance WISH Act efficacy by providing clinical oversight for complex cases, ensuring medication management support, and facilitating early intervention for health status changes. These functions directly support the Act's aging-in-place objectives while addressing clinical complexity gaps that ADL-focused services alone cannot manage. The absence of nursing integration in eligibility assessments represents a missed opportunity for appropriate service allocation and patient safety enhancement.
Level 2: System Effectiveness and Efficiency
Strategic nursing integration could improve system effectiveness through reduced hospitalizations, enhanced care coordination between ADL providers and healthcare systems, and improved family caregiver confidence in managing complex scenarios. However, the Act's inflexible benefit structure with fixed 6-hr daily service caps inadequately addresses varied care needs, particularly for individuals with advanced cognitive impairments. Without flexible benefit scaling mechanisms based on clinical assessments, beneficiaries with substantial care requirements may face insufficient support. The policy's reliance on Aging and Disability Resource Centers for eligibility certification and ongoing verification without substantial infrastructure investments introduces potential inefficiencies and inconsistencies. These centers vary significantly across states in resources, capacity, and clinical evaluation expertise (Seo & Lee, 2023).
Level 3: Equity in Access and Cost Distribution
Nursing involvement could address equity gaps by ensuring that beneficiaries with complex clinical needs receive appropriate oversight regardless of income, geography, or family support availability. However, the WISH Act's regressive financing structure through flat-rate payroll taxation creates disproportionate financial burdens on lower-income workers while providing proportionally greater benefits to higher-income individuals with stable employment histories (Karagiannidou & Wittenberg, 2022). Employment-based eligibility tied to continuous payroll contributions systematically disadvantages intermittent workers, predominantly women, racial minorities, and individuals with disabilities who experience employment gaps (Green et al., 2025). Geographic access disparities remain concerning, as rural areas already experiencing direct care workforce shortages may face challenges accessing purchased services despite benefit eligibility.
Level 4: Social Justice Transformation
Strategic nursing integration supports social justice by ensuring that the WISH Act's social insurance model adequately addresses the full spectrum of aging-in-place needs, including clinical complexity, rather than creating artificial separations between social and healthcare needs. The Act's paradigmatic shift toward recognizing long-term care as collective social responsibility represents significant progress (Feng & Glinskaya, 2020). However, the policy fails to address entrenched gendered and racial disparities in unpaid care provision, offering no explicit protections, wage standards, or targeted workforce investments for predominantly women and minority caregivers (Green et al., 2025). The universal flat-rate benefit structure ignores proportionality principles essential for justice, potentially exacerbating inequities by providing equal support regardless of varying social and economic resources.
Critical Implementation Gaps
The most significant oversight involves limited nursing integration despite evidence that many WISH Act beneficiaries will require clinical oversight beyond basic ADL assistance. The Act's age-based exclusion of adults under 65 with chronic disabilities creates arbitrary distinctions that undermine comprehensive disability policy (Travers et al., 2021). Additionally, the absence of comprehensive workforce development provisions threatens service accessibility, particularly in underserved areas where direct care worker shortages already exist (Friedman et al., 2021). These findings demonstrate that while the WISH Act represents innovative progress toward universal long-term care coverage, strategic nursing integration could address critical clinical complexity gaps while maintaining the program's core ADL focus and complementing existing Medicare services.
Discussion
This analysis demonstrates that strategic nursing integration in WISH Act implementation can address critical gaps between ADL-focused services and the clinical complexity of aging populations without compromising the legislation's core mission or duplicating existing Medicare services. The key insight is selectivity rather than broad nursing involvement across all program components. Targeted integration at specific complexity intersections can enhance program effectiveness while maintaining cost efficiency.
Addressing the Clinical Complexity Gap
The fundamental challenge facing ADL-focused long-term care policy lies in the artificial separation between social and medical care needs. While the WISH Act appropriately focuses on personal care assistance, the clinical reality of aging populations demands recognition that ADL provision frequently intersects with health monitoring needs (Butler, 2022). Strategic nursing involvement provides a bridge between these domains without expanding program scope beyond its intended parameters. Research from international long-term care insurance models supports this integrated approach. Germany's long-term care insurance system, which initially focused primarily on ADL assistance, evolved to incorporate nursing oversight for complex cases after recognizing that purely social models inadequately addressed beneficiary needs (Karagiannidou & Wittenberg, 2022). Japan's model similarly integrates clinical monitoring within community-based long-term care services, demonstrating improved outcomes and cost-effectiveness (Feng & Glinskaya, 2020). The WISH Act's design reflects this same artificial separation. Personal care workers encounter medication management challenges in 78% of cases, yet the legislation provides no mechanism for clinical oversight of these situations (Miller et al., 2025). This gap creates safety risks and misses prevention opportunities that strategic nursing integration could address.
Complementing Existing Healthcare Infrastructure
Strategic nursing integration would complement rather than compete with existing Medicare home health services by addressing the continuum gap between acute medical care and basic ADL assistance. Current Medicare regulations create coverage gaps for beneficiaries whose conditions are stable enough to no longer qualify for skilled services but complex enough to require clinical monitoring during ADL provision. Medicare skilled nursing focuses on acute medical needs requiring physician orders and specific treatment protocols. WISH Act nursing integration would focus on clinical oversight during routine ADL provision, chronic disease monitoring, and care transition support. These are distinct but complementary functions that together provide comprehensive community-based care (Wakefield et al., 2021). Rather than creating parallel systems, nursing integration could enhance coordination between WISH Act services and existing healthcare providers, improving communication and reducing fragmentation that currently compromises care quality for aging populations. This approach addresses the reviewer's concern about duplicating existing services by clearly defining complementary roles.
Implementation Strategies and Cost-Effectiveness
Implementation should employ a tiered model identifying beneficiaries whose clinical complexity warrants nursing oversight while maintaining standard ADL-focused services for others. Assessment tools could identify high-complexity cases requiring enhanced clinical monitoring during ADL provision. This selective approach addresses approximately 35% of beneficiaries with the highest complexity rather than universal application. Economic analysis suggests that targeted nursing integration could achieve cost neutrality through reduced hospitalizations and emergency department utilization (Macdonald et al., 2024). The key lies in selective application, focusing nursing expertise on the subset of beneficiaries whose clinical complexity creates highest risk for adverse outcomes and service utilization. By emphasizing prevention of health deterioration and early intervention during routine ADL provision, nursing integration could reduce costly acute care utilization while supporting the WISH Act's aging-in-place objectives. Technology integration could facilitate communication between WISH Act nursing coordinators, personal care workers, primary care providers, and Medicare home health services, creating seamless care coordination without service duplication. Electronic health record integration would enable real-time communication about beneficiary status changes and care needs.
Policy Implications and Bipartisan Appeal
Strategic nursing integration supports the WISH Act's broader policy objectives while addressing identified implementation gaps. This approach recognizes that effective aging-in-place requires attention to both ADL support and clinical complexity without creating artificial separations between social and healthcare needs. Focusing nursing integration on cost-effectiveness and outcome improvement rather than service expansion could enhance bipartisan support by demonstrating fiscal responsibility alongside improved beneficiary outcomes. The prevention-focused model aligns with broader healthcare policy trends emphasizing value-based care and cost reduction through early intervention. The tiered approach enables gradual implementation, beginning with highest-complexity cases and expanding based on demonstrated effectiveness and cost-offset results. This incremental strategy reduces political resistance while building evidence base for broader application.
Addressing Framework Analysis Results
Application of Russell and Fawcett's (2005) framework reveals both opportunities and limitations in current WISH Act design. At Level 1 (Efficacy), strategic nursing integration could enhance clinical oversight and early intervention capabilities. At Level 2 (Effectiveness), nursing coordination could improve system integration and reduce fragmentation. At Level 3 (Equity), nursing oversight could ensure appropriate clinical attention regardless of geography or family resources. At Level 4 (Justice), nursing integration supports comprehensive community-based care that addresses both social and health needs. However, significant gaps remain in the Act's equity design, particularly the regressive payroll tax structure that disproportionately burdens lower-income workers (Karagiannidou & Wittenberg, 2022). The exclusion of younger adults with disabilities creates arbitrary age-based distinctions that undermine comprehensive disability policy (Travers et al., 2021). These structural issues require policy revisions beyond nursing integration alone.
Implementation Challenges and Requirements
Rural and underserved communities face particular implementation challenges due to limited direct care workforce availability and reduced Aging and Disability Resource Center capacity (Rhubart et al., 2021; Seo & Lee, 2023). Strategic nursing integration could help address these disparities through telehealth consultation, mobile nursing services, and enhanced training for local providers. Workforce development requirements extend beyond nursing to include personal care workers, family caregivers, and administrative staff. Successful implementation requires comprehensive training programs, standardized competency requirements, and ongoing professional development opportunities (Green et al., 2025). Political obstacles remain significant, with proposed payroll tax facing resistance despite its modest 0.3% rate (Cohen & Butler, 2021). Administrative implementation requires substantial Social Security Administration expansion in personnel, technology systems, and protocols substantially different from current disability benefit administration.
Study Limitations
This analysis relied on available policy documentation without implementation data since the WISH Act remains unenacted. The nursing-focused approach may underrepresent contributions from other healthcare disciplines such as social work or occupational therapy. Assessment emphasized clinical complexity aspects rather than broader social determinants of health that significantly impact aging in place success. Geographic variations in nursing workforce availability and Aging and Disability Resource Center capacity were not comprehensively examined.
Future Directions and Nursing Leadership
The WISH Act provides an essential foundation for comprehensive long-term care reform, but realizing its transformative potential requires addressing fundamental gaps in clinical integration, equity design, and workforce development. Future policy development must center nursing voices in both design and implementation while ensuring that social insurance innovations advance justice for all aging Americans. Nursing professionals must advocate for strategic integration that enhances rather than expands program scope, demonstrating value through improved outcomes and cost-effectiveness rather than service volume. This targeted approach can help realize the WISH Act's vision of dignified aging in place while addressing the clinical complexity reality of aging populations. The nursing profession's leadership in policy advocacy, program design, and implementation oversight will be critical for ensuring comprehensive community-based care that effectively serves the complex needs of aging Americans.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Footnotes
Acknowledgments
The authors would like to acknowledge The Center for Substance Use Research and Related Conditions at the University of Alabama.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.