
Abstract
When a person chooses assisted dying, the impact on their family can be profound. Legislation and professional guidelines not only regulate and standardize practice, but also support the delivery of high-quality care. Within this framework, bereavement care plays a vital role by helping families prepare for the death and potentially reducing the risk of prolonged grief. This study explored how current legislation and clinical guidelines on assisted dying address the role and needs of family members, particularly regarding bereavement care. It examined the frequency of the term “family” and its synonyms, as well as the extent to which bereavement support services for relatives are described. A content analysis was conducted on legislative and guideline documents from countries where physician-administered assisted dying is legal. Documents were collected between August 2022 and June 2023, and both quantitative and qualitative analyses were used to assess references to families and descriptions of bereavement care. In total, 22 legislative frameworks and 38 clinical guidelines from nine countries were analyzed. References to family appeared far more often in guidelines (N = 1,213) than in legislation (N = 147). The frequency of these terms varied significantly, with guidelines ranging from two to 83 mentions, and legislation from zero to 18. Eight key themes related to bereavement care emerged, though specific guidance was often lacking. To improve quality care, there is a clear need to better integrate family support into assisted dying guidelines by establishing best practices for bereavement care. Future research should focus on family members’ perspectives and needs.
Background
Assisted dying also known as voluntary assisted dying (VAD) and medical assistance in dying (MAiD), is an umbrella term that includes both euthanasia (the administration of a lethal substance by a physician) and assisted suicide (the self-administration of a lethal substance) (Chambaere & Cohen, 2017; Mroz et al., 2021). This intervention has been legalized in a growing number of jurisdictions in recent years, as of October 2023 (Vissers, 2023). Although it is often perceived as an autonomous decision of the patient (Hamarat et al., 2022), assisted dying inevitably affects the personal and family network of those who choose this intervention (Roest et al., 2019; Yan et al., 2022).
While assisted dying processes have a clear technical outcome, a rapid and painless death, qualitative studies indicate that the experience can be intense and emotionally challenging for family members (Gamondi et al., 2018; Hales et al., 2019; Oczkowski et al., 2021). During the time leading up to the scheduled assisted death, family members may experience conflicting emotions (Roest et al., 2019), moral dilemmas (Gamondi et al., 2015), and exhaustion due to caregiver responsibilities (Roest et al., 2019). After the loss, some family members may begin to doubt whether they made the right decision in supporting the request (Boven et al., 2023a) or they may have negative memories of the dying process (Laperle et al., 2022). Oczkowski et al. (2021) found that family members of patients who requested assisted dying often express the need for counseling and bereavement services, as well as a desire for an organized, professional approach to the day of death. They expect healthcare providers to “choreograph” the assisted dying process and prepare them for what to expect, as many have never been present during the dying process or witnessed a dead body.
Bereavement care can encompass both support prior to and after the loss. As there is no universally accepted definition of bereavement care, the European Association for Palliative Care (EAPC) has recently developed a white paper on the subject, using the Delphi technique to identify the essential and desirable features that define bereavement care. One of these essential features of bereavement care before the loss is to prepare family members for an imminent death, whether or not through assisted means. Preparedness for death is a multifaceted construct, in which healthcare providers can facilitate by providing information and emotional and practical support (Hebert et al., 2009). Healthcare providers can play an important role, in addition to the informal network, regarding bereavement care provision (Breen et al., 2017; Guldin & Leget, 2023; LaValley, 2018). Professional bereavement care can be understood as multidimensional services provided by healthcare providers pre- and postloss to help family members prepare for and/or cope with the loss (Boven et al., 2022; Keegan et al., 2021). The EAPC (Keegan et al., 2021) and several scholars (Aoun et al., 2012; Hudson et al., 2018; Lichtenthal, 2018) have advocated for a more systematic and targeted approach, emphasizing the goodness-of-fit between needs and response, and reducing the likelihood of overlooking those who are particularly vulnerable for prolonged grief (Hudson et al., 2018; Lichtenthal, 2018).
Despite recommendations for needs-based bereavement care, it remains unclear whether and how legislation and guidelines on assisted dying consider family members and their bereavement care needs. Legislative frameworks regulate healthcare practices, while clinical guidelines help to standardize care, contributing to high-quality healthcare delivery (De Leo et al., 2023; Kruk et al., 2018). Close examination of these documents may offer valuable insights into the current provision of bereavement care to family members facing the imminent death of a relative, while also uncovering potential pathways for improvement.
Objective
We reviewed legislation and guidelines on assisted dying from various countries to elucidate the role of family members, assess professional bereavement care, and improve understanding of different practices across these different jurisdictions. The specific objectives of this study were to examine the frequency of mentioning “family” and its synonyms in legislative frameworks and guidelines, and to investigate what recommendations have been made about the provision of professional bereavement care services to family members prior to and after the loss.
Methods
Study Design
To address the research questions, we conducted a literature review that incorporated both qualitative and quantitative content analysis. This approach was chosen to provide a comprehensive summary of the legislative framework and relevant guidelines.
Data Collection
A web search of legislative frameworks and guidelines on assisted dying was performed in two stages from August 15, 2022 to June 28, 2023. In the first stage, governmental websites were searched for publicly available legislative frameworks and guidelines. When documents could not be located, requests were made to relevant authorities. If still unavailable, we moved to the second stage, where we identified stakeholder organizations (see Appendix A). To support this process, a search strategy using specific terms (see online Appendix B) was applied in a general search engine (namely Google). This was intentional, as legislative frameworks are found on governmental websites, and guidelines generally fall within gray literature. The searches directed us to relevant stakeholder websites. Websites of the organizations were first examined for guidelines on assisted dying. When guidelines were not publicly available, the organizations were contacted by email or telephone to ascertain whether they had developed a guideline or were aware of any existing guidelines from other organizations. This strategy was required in Belgium and the Netherlands. In Belgium, we contacted LEIF, Palliatieve Zorg Vlaanderen, Recht op Waardig Sterven vzw, Fédération Bruxelloise de Soins Palliatifs, Fédération Wallonne des Soins Palliatifs, Association pour le Droit de Mourir dans la Dignité, and Liages-Solidaris, leading to the identification of one additional guideline (Solidaris). In the Netherlands, we contacted Expertisecentrum Euthanasie, Nederlandse Vereniging voor een Vrijwillig Levenseinde (NVVE), and Stichting Palliatieve Zorg Nederland (Palliaweb), who confirmed that only one guideline existed. In Canada, all relevant guidelines were readily available on the websites of professional organizations for physicians and nurses. The search strategy was developed with input from the authors and implemented by the first author (CB).
The research team included legislative frameworks and guidelines pertaining to assisted dying that adhered to the following four specified inclusion criteria. First, we only included countries where individuals can legally receive physician-assisted deaths, given the more prominent role of healthcare providers in such deaths, as emphasized by Gamondi et al. (2019). The following countries were identified between April 2002 and September 2023 based on two articles of Mroz et al. (2021, 2022): Australia, Belgium, Canada, Colombia, Luxembourg, the Netherlands, Portugal, Spain, and New Zealand. Countries that were excluded based on this criterion are: the United States, Switzerland, Germany, Italy, and Austria. It is important to note that in Canada, the legislative framework in Quebec differs from that of other provinces and territories. In Quebec, only physicians are authorized to assess eligibility for assisted dying and administer the lethal substance, whereas in other regions of Canada, both physicians and registered nurses are permitted to perform these tasks. Additionally, self-administration is not allowed in Quebec, unlike in the other jurisdictions of Canada. Second, legislative frameworks and guidelines solely focusing on nonterminal conditions were excluded, as needs may substantially differ (e.g., stigma; Helinck et al., 2024). Third, we only included the most recent legislative framework or guideline. Finally, we included legislative frameworks and guidelines that permit assisted dying, even if they have not yet been enacted, which was the case for New South Wales.
The documents were downloaded or saved as files using the NCapture feature in Chrome for easy import into NVivo software (Lumivero, 2018). Non-English or Dutch documents were translated to English using DeepL Translate to determine their appropriateness for inclusion. Translation accuracy was verified by fluent French, Spanish, and Portuguese speakers (RD and NC).
Data Analysis
A qualitative summative and quantitative content analysis was used to analyze the data (Savin-Baden & Howell Major, 2013). This analytical approach provided insights into the role of family members and professional bereavement care mechanisms provided to them both prior to and following a loss. All eligible legislative frameworks and guidelines were uploaded to NVivo 12 (QSR International) for analysis. A coding framework was developed for the quantitative content analysis (Bengtsson, 2016) of the word “family” and its associated terms, including families, relative(s), kin(sman), next of kin, carer(s), caregivers, and significant other(s) as long as these terms referred specifically to a family member. This framework was based on previous literature (Gamondi et al., 2019; Roest et al., 2019), terms used by an online dictionary and reviews (Gamondi et al., 2019; Roest et al., 2019; Variath et al., 2020), and tested on a random sample of legislative frameworks (N = 5) and guidelines (N = 5). It was refined by omitting “kin” due to frequent irrelevant hits. The Dutch terms are available from the search string mentioned in online Appendix B. These terms were quantified using NVivo's Text Search Query. Due to the differences in the number of guidelines across countries, the number of hits was divided by the respective number of guidelines per country. The documents were not read in their entirety; instead, keyword searches were used to identify relevant content. For the qualitative analysis, however, the authors engaged in close reading and in-depth interpretation of all text segments related to “family” and its synonyms.
A qualitative (summative) content analysis (Hsieh & Shannon, 2005) was conducted to identify patterns related to professional bereavement care in text sections referring to “family” or its associated terms. To address the research objective, “family” and related terms were used as the primary search terms. Bereavement care, which has varied interpretations in research and practice, was then used to verify whether it would yield additional results; no additional results were identified. Qualitative data analysis was conducted by two authors (CB and LD) using NVivo software, with CB taking the lead. Initially, CB read the paragraphs identified through keyword searches (see quantitative analysis) to become familiar with the content. During a second reading, preliminary codes were developed in discussion with LD, while retaining the original terminology as much as possible. A code tree was then developed based on these codes, and the extracts were re-examined using the code tree. Data and associated codes were discussed between CB and LD until consensus was reached. Finally, CB summarized the data into main themes and selected representative verbatims, in consultation with the other authors.
Paragraphs that were illustrative of key findings were coded in NVivo under a separate code “quotations.” The inclusion of verbatims was based on the extent to which the paragraphs conveyed, according to the authors, the central message of each theme. A balanced representation across document types (guideline or legislative framework) and countries was ensured as much as possible.
The research team has diverse multidisciplinary backgrounds, including educational sciences and sexology, psychology, nursing, geriatrics, psychiatry, and health policy. These disciplines share a human-centered care focus and a relational orientation, which informed the analytic process and may have influenced interpretation. The lead analyst (CB), trained in educational sciences and sexology and with a strong commitment to improving patient- and family-centered care (PFCC), may have been predisposed to emphasize the importance of the patient's surrounding network. She also has prior experience with thematic analysis and the subject matter. While we approached the policy documents with analytical rigor and engaged in interdisciplinary discussion of the findings, our positionality, shaped by prior research experience on assisted dying, may have informed the framing of key themes and interpretations.
Ethical Considerations
In accordance to the Declaration of Helsinki (World Medical Association, 2024), institutional ethical approval was not required for this study, as the examination of public websites does not fall within the domain of human subject research.
Results
Characteristics of the Included Legislative Frameworks and Guidelines
Figure 1 shows that all legislative frameworks were found on governmental websites while guidelines were primarily (N = 24, 63.2%) found on stakeholder websites (also see online Appendix A). Except for Australia and Canada, each country had one national legislative framework. In Australia, each state has an independent legislative framework.
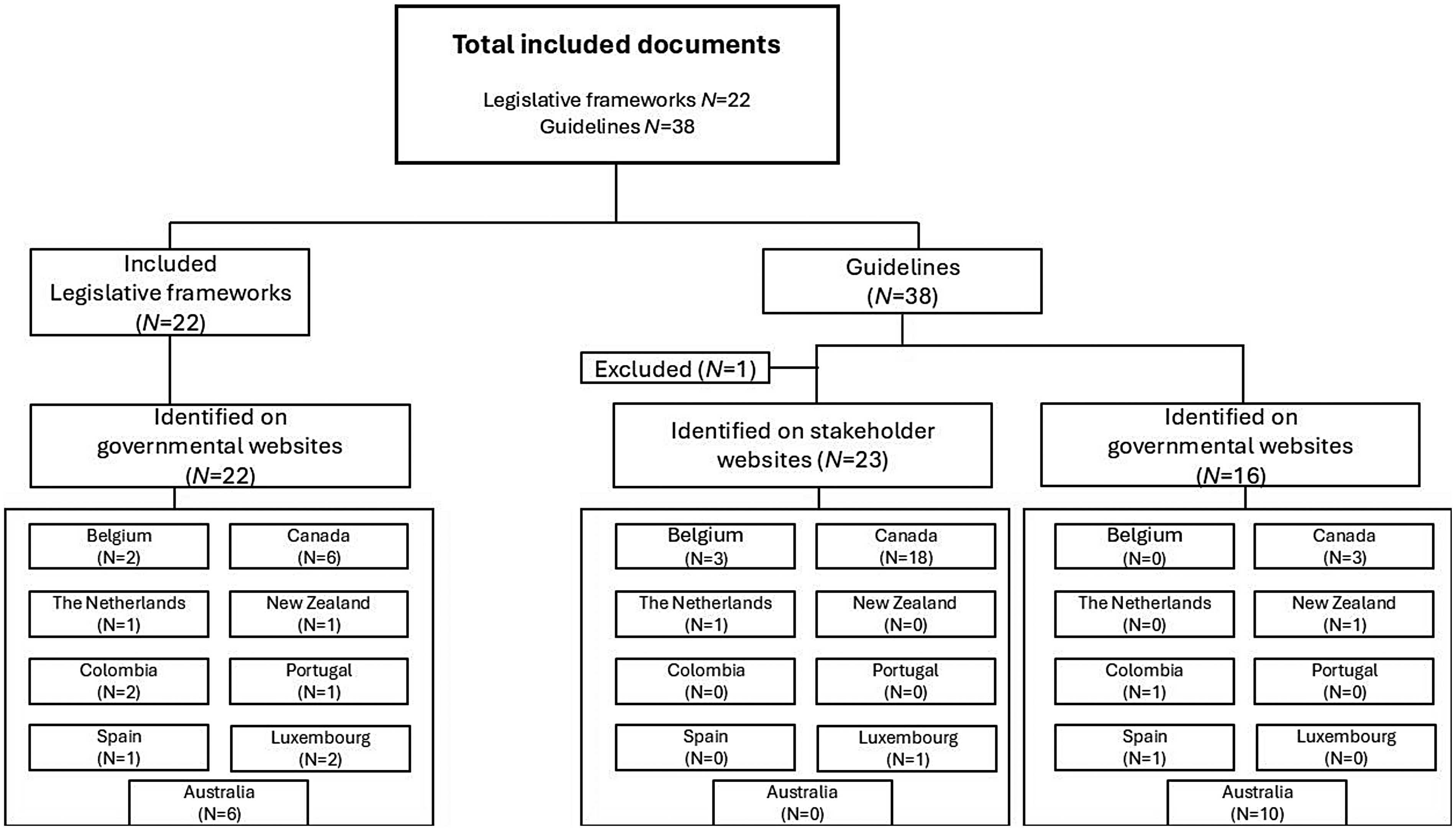
Flowchart presenting the number of documents retrieved per source, and the inclusions and exclusions.
All legislative frameworks (N = 22, 100%) and most guidelines (N = 34, 89.4%) were accessible online. However, a subset of guidelines (N = 4, 10.5%) from certain jurisdictions, Quebec and New Brunswick (Canada), Belgium, and Luxembourg, had to be requested from relevant stakeholder organizations. These included the College of Physicians of Quebec, the Nurses Association of New Brunswick, LEIF (Belgium), and Mäi Wëllen, Mäi Wee (Luxembourg). All requested guidelines were obtained, except the one from Mäi Wëllen, Mäi Wee, who declined our request.
Thus, a total of 22 legislative frameworks (see Figure 1 and online Appendix C) were included from Australia, Belgium, Canada, Colombia, Luxembourg, the Netherlands, Portugal, Spain, and New Zealand. We identified 39 guidelines, of which 38 guidelines, excluding Luxembourg's (Mäi Wëllen Mäi Wee, 2022), were included for analysis. Of the included jurisdictions, there were no guidelines found for New South Wales and Portugal. Further information on the legislative frameworks and guidelines is available in online Appendix C.
Frequency of Family-Related Terms in Legislative Frameworks and Guidelines on Assisted Dying
The word “family” and its related terms were referenced a total of 147 times in legislative frameworks and 1,110 times in guidelines, with an average of seven occurrences per legislative framework and 29 per guideline. There were substantial differences in the results between countries. The average frequency per legislation and guideline differed between countries, ranging from zero to 18 for legislative frameworks and two to 83 for guidelines. Table 1 shows that Australian legislation (N = 105, 71.4% of all legislation references) and guidelines (N = 751, 67.7% of all guideline references) had the highest frequency of the word “family” and related terms in absolute and relative numbers.
Frequencies of the Word “Family” and Related Terms in Legislative Frameworks and Guidelines By Country.
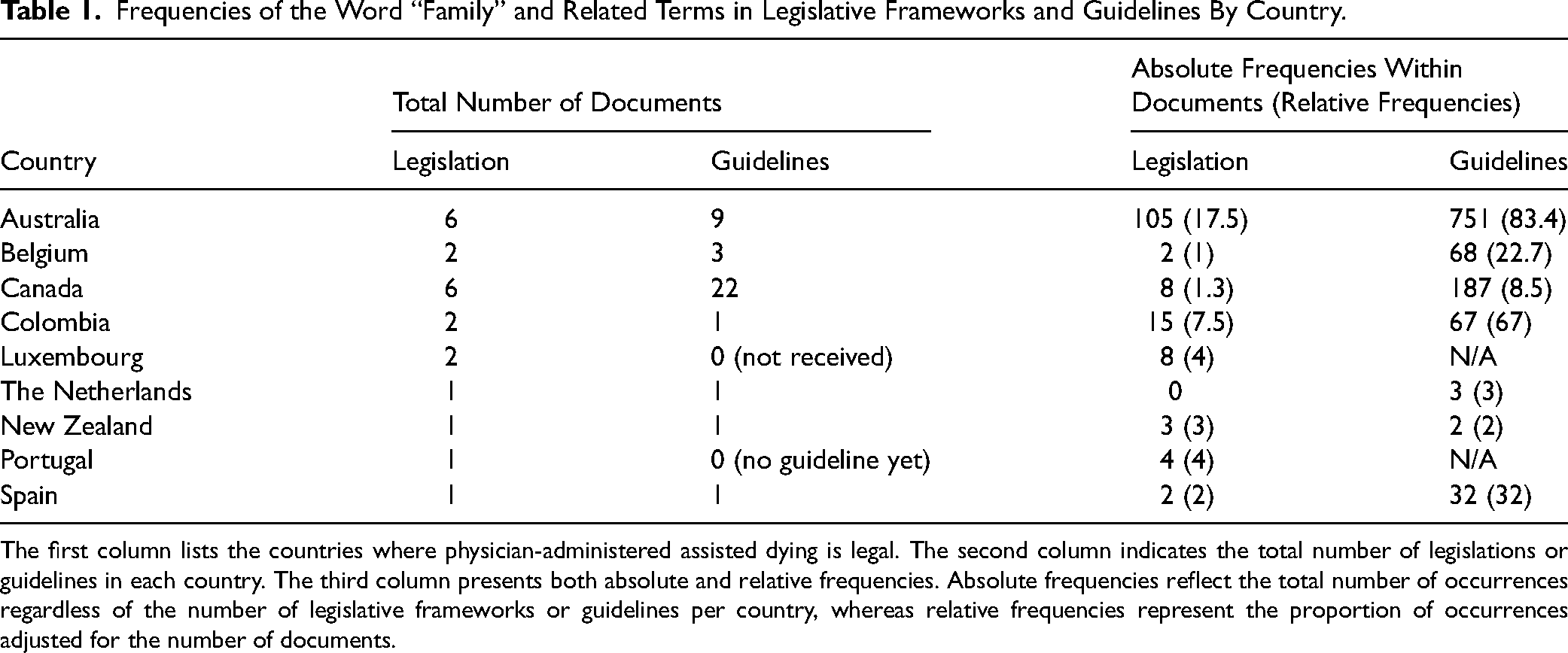
The first column lists the countries where physician-administered assisted dying is legal. The second column indicates the total number of legislations or guidelines in each country. The third column presents both absolute and relative frequencies. Absolute frequencies reflect the total number of occurrences regardless of the number of legislative frameworks or guidelines per country, whereas relative frequencies represent the proportion of occurrences adjusted for the number of documents.
The terms “family” and “families” (“familie” and “families” in Dutch) were used in the majority of legislative frameworks (N = 88, 59.9%) and in half of the guidelines (N = 600, 54.1%) worldwide.
Bereavement Care Provision by Healthcare Providers in Legislative Frameworks and Guidelines on Assisted Dying
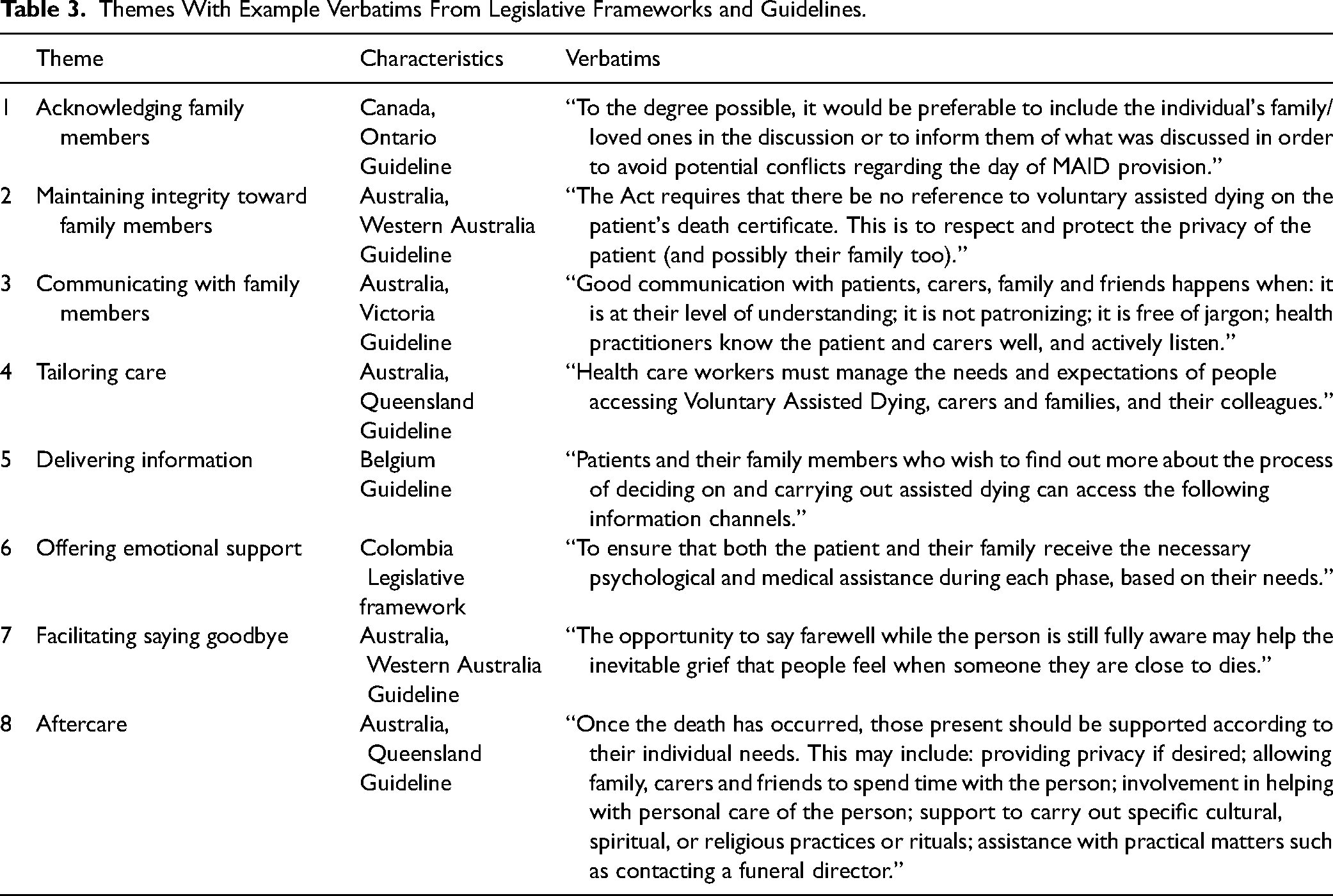
In total, bereavement care provisions to family members by healthcare providers in legislative frameworks and guidelines were mentioned 333 times. Although nonspecific support was commonly mentioned in legislative frameworks and guidelines (N = 59, 17.7%), several specific bereavement care services were also described. Eight themes related to professional bereavement care for relatives were identified: acknowledging family members, maintaining integrity toward them, communicating with them, providing tailored care, information and emotional support to them, facilitating opportunities for saying goodbye, and providing aftercare (see Table 2). In general, bereavement services were often vaguely and rather briefly described, with few concrete directions. Most bereavement services were situated in the period preceding the loss, while the focus on aftercare was less prominent.
An Overview of the Themes in the Legislative Framework and Guidelines of Each Country.
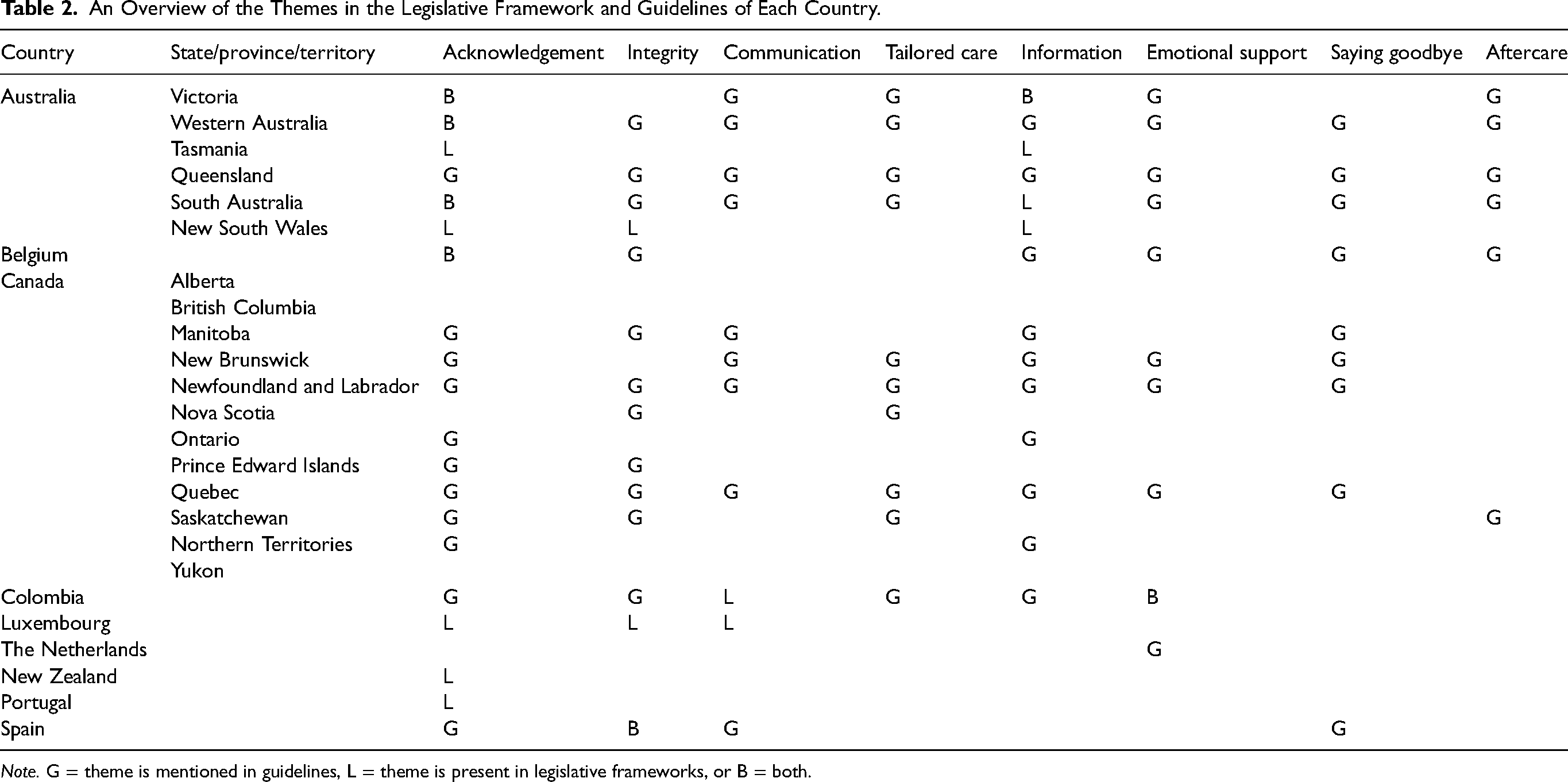
Note. G = theme is mentioned in guidelines, L = theme is present in legislative frameworks, or B = both.
Themes With Example Verbatims From Legislative Frameworks and Guidelines.
Discussion
This content analysis of legislative frameworks and guidelines on assisted dying examined both absolute frequencies (the total number of occurrences) and relative frequencies (the proportion of occurrences relative to the number of guidelines per country). The findings reveal considerable variation in the frequency of the word “family” and related terms across countries, with occurrences ranging from zero to 18 in legislation and from two to 83 in guidelines. In seven countries, “family” or related terms appear an average of five times or fewer in legislation, while only two countries mention these terms fewer than five times in their guidelines. Australian legislation (N = 105, 71.4% of all legislative references) and guidelines (N = 751, 67.7% of all guideline references) show the highest frequency of “family” and related terms. Additionally, the qualitative content analysis highlights that descriptions of professional bereavement care to family members are often brief, vague, and lacking in concrete guidance for practice. A total of eight themes related to professional bereavement care for relatives were identified: acknowledging family members, maintaining integrity toward them, communicating with them, providing tailored care, information and emotional support to them, facilitating opportunities for saying goodbye, and providing aftercare.
There is considerable variation within and between countries in the extent to which legislation and guidelines on assisted dying mention family members and good practices in bereavement care. These variations may reflect the legal recognition of family members, their bereavement care needs, and broader cultural perspectives on assisted dying. For example, the high frequencies in Australian legislation and guidelines may be partly explained by the growing emphasis on PFCC in Australia. Models of PFCC are becoming increasingly common, which is visible in the following implemented policy measures: the Australian Charter of Healthcare Rights, Australian Safety and Quality Framework for Healthcare and National Safety and Quality Health Standard (Frakking et al., 2020). The growing interest is further evidenced by the Australian Institute for Patient- and Family-Centered Care (Australian Commission on Safety and Quality in Health Care, 2011).
Many Western countries historically place a greater emphasis on individualism and self-determination, consistent with a cultural focus on autonomy (Fontalis et al., 2018). This focus is evident in end-of-life decision-making policies and practices, which tend to affirm the autonomy of the individual (Wilson et al., 2014). The focus on autonomy is also reflected in legislation and some guidelines on assisted dying. The legislation on assisted dying has traditionally assumed a “colloque singulier” between doctors and patients, with limited attention to the needs of family members. However, emerging evidence indicates that relatives are typically involved in all stages of assisted dying (Roest et al., 2019; Thangarasa et al., 2022; Yan et al., 2022), highlighting the importance of acknowledging the triadic relationship among patients, relatives, and healthcare providers (Roest et al., 2019). This shift reflects a growing recognition that autonomy does not exist in isolation but is embedded within social networks (Gómez-Vírseda et al., 2020). Accordingly, relatives are increasing acknowledged in the context of assisted dying, making it the most frequently mentioned main theme in our analysis (yet limited). This shift is clearly illustrated in the position papers of the Dutch Royal Medical Association. In 1984, assisted dying was framed solely within the physician–patient relationship, with no mention of relatives. Subsequent papers in 1995 and 2003 noted that, although euthanasia and assisted dying remains primarily a matter between an individual patient and physician, relatives are often closely involved. The most recent paper (2021) further clarifies that physicians may take the opinions of relatives into account in their decision-making process (Renckens et al., 2024). Although relatives are increasingly acknowledged in research and clinical practice, this recognition is still limited in guidelines and legislative frameworks.
Relatives often experience euthanasia as emotionally challenging (Gamondi et al., 2018; Hales et al., 2019; Oczkowski et al., 2021), however, our study shows that emotional support needs are rarely addressed in existing legislation and guidelines. This gap may partially result from an overreliance on quantitative evidence, which to date suggests that grief following assisted dying is not more intense or complex than grief after unassisted deaths (Laperle et al., 2022; Swarte et al., 2003). Nevertheless, emotional support may be necessary not only at the moment of the assisted dying decision but also throughout the period leading up to death and during bereavement. This need is likely to be particularly urgent in cases of psychiatric patients. In Belgium and the Netherlands, where euthanasia for psychiatric patients has been legal since 2002, relatives often report emotional hardship, stigma, taboo, social isolation, and complications regarding reconciling with the person's request (Helinck et al., 2024). With Canada's upcoming expansion of euthanasia legislation in March 2027 to include individuals with psychiatric conditions (Government of Canada, 2024), there is a critical opportunity to explicitly integrate relatives’ emotional support needs and concrete directions into guidelines. Anticipating and addressing these needs will not only be important in the Canadian context but may also provide valuable guidance for other countries that consider similar legislative developments in the future. Another main theme that was rarely mentioned is aftercare, which is not surprising, as recent research shows that relatives have limited expectations regarding it (Boven et al., 2024). This may be partly explained by relatives’ recognition that healthcare providers are often overburdened and have limited resources (Walker & Deacon, 2016), which could lower their expectations. Further research is needed to explore relatives’ expectations of professional aftercare in the context of assisted dying globally. Finally, the theme “facilitating goodbye” was also infrequently mentioned despite relatives struggling with uncertainty, limited familiarity with dying, and desire to support their loved one's wish for a “good death” (Sallnow et al., 2022). The Greek term “euthanasia” literally means “a good death” (van Hooff, 2004), reflecting the desire to achieve a dignified end to life through medical means. This growing reliance on healthcare providers may inadvertently fuel family member's erosion of language, knowledge, and confidence to manage the dying process (Sallnow et al., 2022), indicating a profound gap in guidelines on assisted dying. Rather than replacing relatives’ role with professionals, we advocate strengthening family members’ capacities to navigate issues around death and dying and to facilitate saying goodbye appropriately. Accordingly, both healthcare providers and family members would benefit from the inclusion of grief literacy and compassionate communities initiatives in guidelines on assisted dying.
Despite calls for structured, needs-based bereavement care (Aoun et al., 2012; Keegan et al., 2021), evidence shows that healthcare providers often rely on intuition and personal experience when offering support during assisted dying, resulting in ad hoc and inconsistent provision (Boven et al., 2023b). This reveals a significant gap in which bereavement care must be developed from the bottom up, leading to variation both within and between countries and potentially creating uncertainty for early-career healthcare providers. To improve future nursing practice, it would be beneficial to incorporate reflective moments and opportunities for peer learning, and to develop evidence-based guidelines describing good practices. The limited descriptions of bereavement care services likely reflect the paucity of research on family members’ needs in the context of assisted dying (Brown et al., 2022; Hales et al., 2019; Smolej et al., 2022). Future research should investigate the need for professional bereavement support from the perspective of family members and identify effective practices. In particular, culturally sensitive research is essential, as neglecting this dimension may exacerbate inequalities among Indigenous populations and ethnic minorities. Inequalities to care may also arise from financial arrangements. In Belgium and the Netherlands (Expertisecentrum Euthanasie, 2025), for example, the costs of euthanasia procedures are covered by health insurance, which helps safeguard more equal access. By contrast, the United States illustrates how the absence of such coverage may reinforce inequality, as most government-run health insurance programs and private insurance policies do not reimburse assisted dying, which is particularly impactful on individuals with limited resources and high symptom burdens (Kozlov et al., 2022). Not only do insufficient policies and guidelines play a role (Ward et al., 2021), inadequate education and training (Sandham et al., 2022) are likely responsible too for the lack of a systematic provision. This underscores the need to reform pre- and postgraduate curricula across healthcare disciplines to better prepare providers for supporting families in the context of assisted dying. While some countries, such as the Netherlands and Belgium, have established training programs, Australia is currently the only jurisdiction mandating compulsory training for practitioners before participating in assisted dying, in contrast to Colombia, where all doctors are considered competent to receive a euthanasia request (Del Villar et al., 2025).
In our opinion, guidelines could benefit from a more contextual approach. We do not extend our recommendation for a more contextual approach to assisted dying legislation itself. In countries like Belgium, the Netherlands, and Canada, such legislation primarily aims to remove criminal liability by outlining eligibility criteria and procedural safeguards. It establishes the conditions under which assisted dying is permitted, while best practices for bereavement care for families are considered complementary to the legal framework. The situation is different in Switzerland, where the penal code has since 1942 stipulated that assisting in suicide is not a crime provided there are no selfish or covetous motives. Assisted dying is therefore not regulated by specific legislation, instead, since the 1980s, right-to-die organizations have interpreted this legal permission as authorization to support individuals seeking assisted suicide (Mroz et al., 2021). The proposed contextual approach does not imply that relatives need to be treated as codecision makers (they should not have to provide consent for a request or have the authority to block it), but rather that their perspective (thoughts, feelings, concerns) and bereavement care needs should be acknowledged. We suggest that future research reviews legislation and guidelines in countries limited to self-administration of lethal medication, and investigate potential differences in expectations of professional bereavement care.
Strengths and Limitations of the Study
This review is the first to analyze the role of family and professional bereavement care mechanisms, both before and after a loss. A previous review of regulatory documents was exclusively conducted in the Canadian context, and does not specifically address bereavement care (Pesut et al., 2019).
This study also has several limitations. We could only include legal frameworks and guidelines that are available online, provided by the government or identified stakeholders (see online Appendix A). The challenge with guidelines is that they cannot be systematically searched for in research search engines, unlike systematic reviews. We believe that we have identified most guidelines; however, it cannot be guaranteed that all relevant guidelines have been identified. We recommend that future research studies also search for policies in care settings (e.g., hospitals). In addition, we searched for keywords related to family rather than bereavement care, as there is a lack of consistent interpretation of the latter term in research and practice. Some keywords (such as caregiver and carer) may extend beyond familial relationships, however, we aimed to ensure that all keywords potentially related to family were included.
Conclusion
Our study finds that “family” and related terms are used with varying frequencies in legislation and guidelines on assisted dying. On average, “family” is mentioned more in guidelines than in legislative frameworks. While professional bereavement care for family members is acknowledged in some of these documents, the descriptions tend to be brief and lack concrete directions for practice. The high frequency of references in Australian legislation and guidelines likely reflects the country's legal recognition of family and its strong emphasis on PFCC, supported by relevant policy measures. Family member's perspectives are often underrepresented in legislation and guidelines on assisted dying. It appears that advocacy is needed for the increased visibility of family members in assisted dying guidelines. This implies a more contextual approach, in which relatives are not treated as codecision makers, but that their perspective and bereavement care needs are acknowledged. This could contribute to relatives being adequately supported before, during, and after the assisted dying process. Our findings also suggest the need for further qualitative research on relatives’ needs and expectations regarding professional bereavement care, such as emotional support, aftercare and opportunities to say goodbye, to enhance its provision in the context of assisted dying.
Supplemental Material
sj-docx-1-ppn-10.1177_15271544251408789 - Supplemental material for What About the Family? A Content Analysis of International Legislative Frameworks and Guidelines on Assisted Dying
Supplemental material, sj-docx-1-ppn-10.1177_15271544251408789 for What About the Family? A Content Analysis of International Legislative Frameworks and Guidelines on Assisted Dying by Charlotte Boven, MSc, PhD, Gilla K. Shapiro, MPP, MPA, PhD, Liesbeth Van Humbeeck, RN, MSc, PhD, Let Dillen, MA, PhD, Nele Van Den Noortgate, MD, PhD and Gary Rodin, MD, FRCPC, PhD in Policy, Politics, & Nursing Practice
Footnotes
Acknowledgments
We want to express our gratitude to the native speakers, Ramon Duran-Romaña and Nuno Chicória, who checked the accuracy of translations.
Author Contributions
Charlotte Boven: conceptualization, formal analysis, funding acquisition, investigation, methodology, visualization, writing—original draft and review and editing. Gilla K. Shapiro: conceptualization, methodology, supervision, writing—original draft and review and editing. Liesbeth Van Humbeeck: conceptualization, funding acquisition, methodology, and writing—original draft. Let Dillen: conceptualization, methodology, supervision, and writing—original draft and review and editing. Nele Van Den Noortgate: conceptualization, funding acquisition, methodology, supervision, and writing—original draft and review and editing. Gary Rodin: conceptualization, methodology, supervision, and writing—original draft and review and editing.
Data Availability
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
Not applicable. In accordance to the Declaration of Helsinki, institutional ethical approval was not required for this study, as the examination of public websites does not fall within the domain of human subject research.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. The research stay of CB at the Princess Margaret Cancer Centre was funded by the Research Foundation–Flanders (FWO) (K221322N). The funding source had no involvement in the research conduct nor in the preparation of the manuscript.
Writing Assistance
During the preparation of this work, the authors used ChatGPT to improve language and readability. After using this tool/service, the authors reviewed and edited the content as needed and take(s) full responsibility for the content of the publication.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.