
Abstract
Family caregivers provide essential unpaid care to millions of older adults and individuals with chronic illness or disability in the United States, yet federal support policies have historically been fragmented and underdeveloped. The Recognize, Assist, Include, Support, and Engage (RAISE) Family Caregivers Act of 2018 (Pub. L. 115-119) established the first national framework to coordinate federal actions, disseminate evidence-based practices, and institutionalize caregiver recognition. This study analyzed the RAISE Act using Walt and Gilson's Health Policy Triangle and Kingdon's Multiple Streams Framework to understand how its structure, political origins, and implementation mechanisms institutionalize caregiving support and create opportunities for nursing leadership. Primary data included legislative text, congressional records, and federal implementation documents; secondary data comprised policy briefs, nursing literature, and grey reports from 2016–2024. Analysis revealed that the Act reframes family caregiving as a coordinated national responsibility through recurring strategy updates, multi-sector collaboration, and public transparency, ensuring sustainability without new appropriations. The convergence of social need, feasible policy alternatives, and bipartisan support created a durable policy window (an opportune moment when conditions align for policy enactment). Nursing has substantial opportunities to shape implementation through care coordination, caregiver education, evaluation, and advocacy. The RAISE Act demonstrates how modest, consensus-based policy can generate structural impact, creating expanded opportunities for nursing to lead caregiver integration, strengthen care transitions, and advance equitable aging policy.
Introduction
Family caregiving has become one of the most pressing health and social challenges in the United States. More than 53 million Americans provide unpaid care to older adults or people living with chronic illness, disability, or functional limitations (AARP & National Alliance for Caregiving, 2020). Their work fills major gaps in the long-term care infrastructure yet often occurs without training, compensation, or recognition (Schulz & Eden, 2016). Many caregivers experience exhaustion, financial strain, and emotional distress while navigating fragmented systems of health and social support (Liu et al., 2020). In a system increasingly dependent on unpaid labor from families, effective caregiver policy is essential to quality, equity, and sustainability in care. As the population ages and life expectancy rise, the country's reliance on informal caregivers will continue to grow and can reach unsustainable levels if not addressed. Policy responses have been slow and uncoordinated, leaving caregivers with limited assistance and few opportunities to participate in care planning or decision-making (Green et al., 2024).
The Recognize, Assist, Include, Support, and Engage (RAISE) Family Caregivers Act was enacted in 2018 to address this growing healthcare crisis in the U.S. (Recognize, Assist, Include, Support and Engage [RAISE] Family Caregivers Act, 2018). The RAISE Act represents a turning point in U.S. caregiver policy because it reframes caregiving as a national responsibility rather than a private family matter. The Act marks the first time that the federal government has established a structured mechanism to recognize caregivers and to align policies across agencies responsible for aging, disability, and health programs. The Act provides the framework for developing strategies for coordinating the multiple federal and state funding networks and supporting services for family caregivers. The Advisory Council is charged with providing recommendations for support needed to improve care and coordinate federal programs to the Secretary of Health and Human Services (HHS). The Advisory Council is a group of 15 appointed members which includes diverse individuals from family member caregivers, care recipients, healthcare providers, employers, and state and local officials. The law directs the Secretary of Health and Human Services, working with this appointed Family Caregiving Advisory Council, to develop and maintain a national strategy to support family caregivers. This strategy must identify best practices, coordinate federal and state efforts, and report progress to Congress on a recurring basis. It does not create a new funding stream or entitlement program. Instead, it sets up an iterative process for coordination, evidence dissemination, and stakeholder engagement.
By emphasizing person- and family-centered care, interagency collaboration, and evidence-based strategy, the Act lays the groundwork for integrating caregivers into the broader health system. For the nursing profession, this policy is especially significant. Nurses are often the primary link between patients, families, and service systems (Kyei & Mumba, 2025). They play key roles in care coordination, education, and transitional planning, the very domains the Act seeks to strengthen (Kyei et al., 2026). Understanding how the Act structures authority, distributes responsibility, and promotes collaboration is essential to identifying where nursing leadership can contribute to implementation and long-term success (Kyei et al., 2026). Despite its importance, the RAISE Act has received limited scholarly analysis. Most public discussions have focused on its recognition of caregivers rather than its structural and operational features. Examining these features through a policy analysis lens allows a deeper understanding of how caregiver support has been established and how professional communities, including nursing, can shape outcomes. The purpose of this analysis is to explore how the RAISE Act supports family caregivers, the mechanisms it uses to coordinate federal and state actions, and the opportunities it creates for nursing leadership. The analysis aims to clarify how policy planning can drive incremental but lasting improvement in caregiver recognition and integration. By unpacking the Act's internal logic and examining its implications for the health workforce and nurses, this paper contributes to nursing policy scholarship on long-term care, care coordination, and aging services. For nursing, these lessons underscore the need for proactive participation in shaping national caregiving strategies and in translating them into practical tools that improve outcomes.
Methods
This policy analysis used an integrative qualitative design grounded in document analysis and guided by two complementary frameworks: Walt and Gilson's Health Policy Triangle (HPT) and Kingdon's Multiple Streams Framework (MSF). The combination of these frameworks enabled a comprehensive examination of both the structural and political dimensions of the RAISE Family Caregivers Act (Public Law 115‒119). The HPT provided an analytic lens to deconstruct the Act's context, actors, content, and process (Walt & Gilson, 1994; Walt et al., 2008), while the MSF explained the agenda-setting and timing dynamics that shaped its enactment (Kingdon, 2011). Together, they supported a layered understanding of how caregiving emerged as a federal policy priority and how the law operationalizes coordination and accountability across agencies.
Data Sources
Primary data consisted of the official legislative text of the RAISE Family Caregivers Act of 2017, as published in the U.S. Government Printing Office database (RAISE Family Caregivers Act, 2018). Secondary materials included congressional reports, hearing transcripts, and legislative histories available through the Congressional Record between 2017 and 2018 (Congressional Record, 2017). Federal implementation documents produced after enactment were also analyzed, including reports and updates from the Administration for Community Living (ACL (2022), 2024), Family Caregiving Advisory Council annual reports (2021–2024), and public comment summaries posted on the U.S. Department of Health and Human Services (HHS) website (Federal Register, 2022). Grey literature from professional associations such as AARP, the National Alliance for Caregiving, and nursing organizations was reviewed to contextualize nursing relevance. Peer-reviewed literature between 2016 and 2024 addressing family caregiving policy, aging, and care coordination was used to triangulate interpretations.
Analytical Procedures
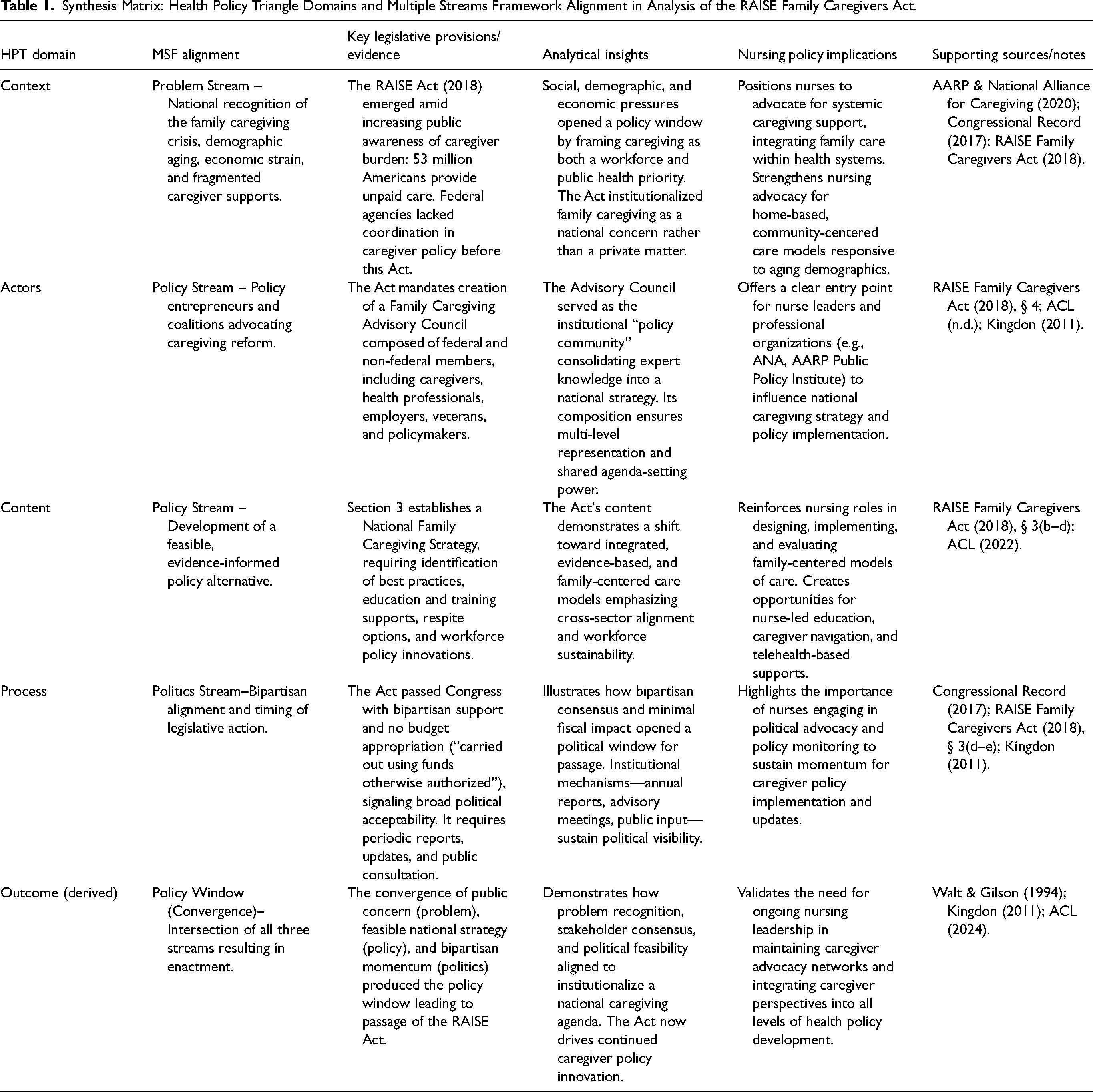
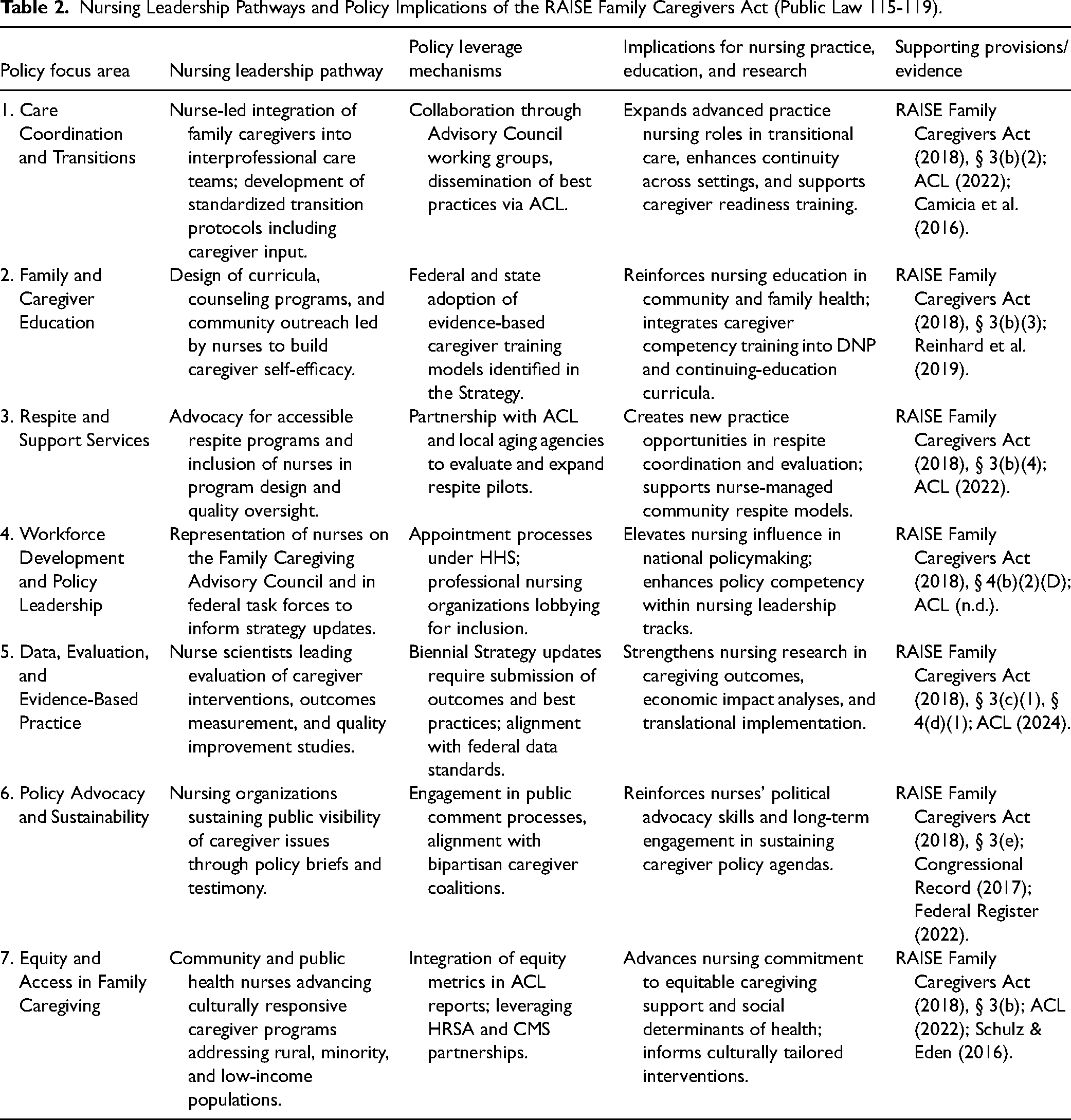
Data were imported into NVivo for systematic coding. A three-stage deductive and inductive analytic process was followed. In Stage 1, open coding was applied to the legislative text to identify recurring terms and clauses reflecting policy goals, governance structures, and accountability mechanisms. These were then categorized under the four HPT domains: context, actors, content, and process (Walt & Gilson, 1994). Each domain served as a primary code node. In Stage 2, Kingdon's MSF (2011) was used to trace how the problem, policy, and politics streams converged to produce a “policy window” for passage. This involved coding sections of congressional debates and public advocacy materials to identify expressions of problem recognition, policy proposals, and political alignment. Stage 3 involved synthesis, where patterns and interconnections between HPT domains and MSF streams were examined. This step identified how contextual conditions and actor configurations interacted with political opportunity to shape the Act's final design. A synthesis matrix (Table 1) was developed to align each HPT domain with its corresponding MSF stream, relevant statutory clauses, analytical insights, and nursing implications. This matrix enabled cross-referencing between the structural components of the Act and the political processes underpinning its development. A second matrix (Table 2) was created to extend findings toward professional translation, specifying nursing leadership pathways derived from the policy's mandates.
Synthesis Matrix: Health Policy Triangle Domains and Multiple Streams Framework Alignment in Analysis of the RAISE Family Caregivers Act.
Nursing Leadership Pathways and Policy Implications of the RAISE Family Caregivers Act (Public Law 115-119).
Rigor and Validation
Several strategies ensured analytic rigor. Triangulation was achieved through the integration of multiple document types, statutory texts, legislative records, implementation reports, and scholarly analyses, allowing convergence across data sources. A transparent audit trail was maintained, detailing document selection criteria, coding definitions, and framework alignment decisions. Interpretive consistency was strengthened through peer debriefing with two senior faculty experts in nursing policy and aging systems who independently reviewed the coding summaries for conceptual fidelity. All analytic decisions were revisited until consensus was reached. Framework congruence was verified by mapping analytic outputs against each framework's core constructs (O'Brien et al., 2020). For the HPT, results were checked to ensure coverage of all four domains. For the MSF, each identified policy moment was traced to evidence from legislative or agency sources demonstrating alignment with the problem, policy, and politics streams. This dual-framework cross-validation minimized bias and clarified the boundaries between policy structure and political process.
Ethical Considerations
As this study involved publicly available policy documents and did not include human participants, it did not require institutional review board approval. Nonetheless, ethical principles of academic integrity, transparency, and accurate representation of legislative intent were maintained. All primary sources were cited verbatim where relevant, and interpretations were confined to textual evidence and established policy frameworks.
Methodological Limitations
Two limitations are acknowledged. First, document analysis cannot capture informal negotiations or behind-the-scenes political influences that may have shaped the Act's passage. Second, post-enactment documents vary in detail, and some implementation outcomes are still emerging. To mitigate these constraints, cross-verification across independent federal reports and peer-reviewed analyses was performed, ensuring conclusions reflected the best available evidence at the time of writing.
Synthesis
Analysis of the RAISE Family Caregivers Act using the integrated Health Policy Triangle and Kingdon's Multiple Streams Framework reveals a concise, consensus-oriented policy that reframes family caregiving as a coordinated federal responsibility (Figure 1). The Act's structure demonstrates coherence across context, actors, content, and process, translating social recognition of caregiver burden into a recurring national strategy rather than a one-time program.
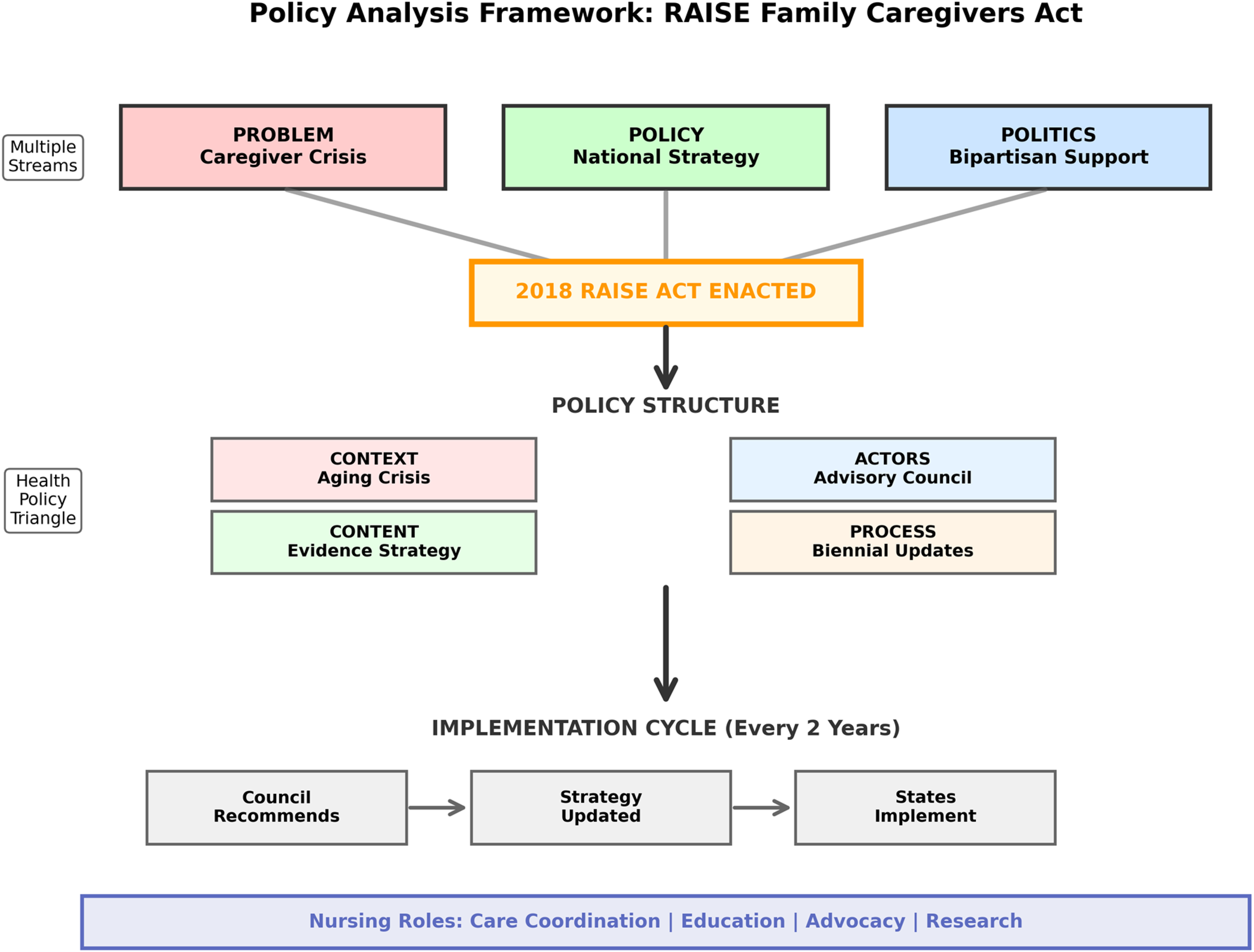
Policy analysis of the RAISE Family Caregivers Act using integrated frameworks. Top: Kingdon's Multiple Streams Framework showing convergence of problem, policy, and politics streams leading to 2018 enactment. Middle: Walt and Gilson's Health Policy Triangle domains structuring the Act's design. Bottom: Linear implementation sequence with biennial updates, showing Advisory Council recommendations informing strategy updates that guide state-level implementation.
The policy context was defined by escalating caregiver demands, demographic aging, and fragmentation among federal and state programs. Over 50 million Americans were providing unpaid care with minimal systemic support (AARP & National Alliance for Caregiving, 2020). The Act emerged when public and political attention to this crisis converged, forming Kingdon's (2011) “problem stream” (the recognition that a significant social issue requires policy attention). Legislators intentionally designed a framework that recognized caregiving as a national concern without creating new entitlement spending. By embedding coordination duties within existing federal structures (Administration for Community Living, Centers for Medicare and Medicaid Services, Social Security Administration, Department of Veterans Affairs), the Act lowered fiscal resistance while signaling federal commitment (RAISE Family Caregivers Act, 2018). The context thus reflects strategic pragmatism: an enabling rather than directive approach that legitimized caregiving as infrastructure vital to health and long-term care delivery. Non-preemption clauses (provisions preventing federal law from overriding state authority) and rule-of-construction clauses (interpretive guidelines preserving existing legal frameworks) reinforced this cooperative stance, preserving state flexibility while inviting alignment.
The actor configuration embodies the plural governance model typical of modern U.S. social policy. The Family Caregiving Advisory Council institutionalizes multi-sector representation, combining federal agencies, such as the Centers for Medicare and Medicaid Services, the Administration for Community Living, and the Department of Veterans Affairs, with up to fifteen appointed members representing caregivers, providers, employers, and advocates (ACL, n.d.). Federal members are non-voting, ensuring interagency coordination without dominance. This configuration, as reflected in Table 1, operationalizes the HPT actor dimension (Walt & Gilson, 1994) by embedding stakeholder collaboration within the statute. In Kingdon's (2011) terms, the council functions as a sustained “policy community” (a network of specialists who share expertise and influence policy development) that converts professional and experiential expertise into feasible strategy proposals. Through quarterly public meetings and annual reports, it maintains issue visibility and generates the documentation guiding updates to the national strategy. The open design decentralizes policy development, replacing individual lobbying with an institutional feedback system.
The policy's content emphasizes coordination, education, and sustainability. Section 3 directs the Secretary of Health and Human Services, in consultation with the Advisory Council, to develop and update a National Family Caregiving Strategy identifying best and promising practices, education and training supports, respite options, and mechanisms to eliminate redundancies (RAISE Family Caregivers Act, 2018). This content advances a unified theory of change: strengthening caregiver capability and integrating caregivers into care teams improves quality and reduces system fragmentation. Technical assistance provisions extend this learning to states and localities, but the Act explicitly prohibits mandates to adopt identified best practices. This voluntary design favors diffusion through collaboration rather than compliance, allowing adaptable implementation across diverse health and social care systems. The content also institutionalizes evaluation through the required collection and publication of evidence on caregiver support models.
The policy process transforms the Act from a legislative event into an iterative governance mechanism. The Secretary must develop the initial strategy within 18 months and update it every two years based on council recommendations and public input (RAISE Family Caregivers Act, 2018). These statutory timelines anchor a predictable cycle of assessment and revision. The council's annual reports inventory federally funded caregiver programs, identify gaps, and evaluate impacts on Medicare, Medicaid, and related services. Each component reinforces the others: the council provides data and recommendations; the Secretary synthesizes them into a public strategy (ACL (2022)); and the public consultation process renews accountability (Federal Register, 2022). The result is a self-correcting policy system that converts stakeholder feedback into successive strategy iterations. Within Kingdon's (2011) framework, this process sustains the convergence of problem, policy, and politics streams by periodically reopening the policy window through scheduled review.
The Act's political design reflects fiscal realism (pragmatic policymaking constrained by budget limitations), requiring implementation within existing agency resources without new appropriations. A sunset clause (a provision that terminates legislation after a specified period) initially limited the Act to three years at enactment. These fiscal constraints ensured bipartisan passage (Congressional Record, 2017) and preserved political viability across diverse legislative priorities. The legislation depends on interagency collaboration and voluntary state adoption rather than federal mandates or enforcement authority. Despite this limited fiscal scope, the Act employs soft power (influence through persuasion, transparency, and reputational incentives rather than legal enforcement) to drive alignment. Mandatory reporting requirements and technical assistance create normative pressure by elevating programs that achieve measurable outcomes and disseminating effective models through federal channels. The Act substitutes transparency and evidence dissemination for regulatory compulsion, allowing reputational incentives and performance visibility to motivate adoption. Across HPT domains, contextual urgency generated political will; diverse actors supplied legitimacy; content provided coherence and evidence orientation; and the process guaranteed continuous learning. These dimensions collectively transform caregiving from episodic concern to permanent policy agenda. The legislation functions as governance infrastructure through which caregiver policy evolves, achieving institutional durability rather than resource expansion. Across HPT domains, the synthesis shows that the Act's primary achievement is institutional durability rather than resource expansion. Contextual urgency generated political will; diverse actors supplied legitimacy; content provided coherence and evidence orientation; and the process guaranteed continuous learning. These dimensions collectively transform caregiving from episodic concern to permanent policy agenda. The legislation thus functions less as a finite program and more as a governance infrastructure through which caregiver policy evolves.
Implementation logic (the structured, step-by-step reasoning for translating policy mandates into operational practice) follows a clear sequence. The Advisory Council consolidates stakeholder knowledge; the Secretary formulates and publishes the strategy; agencies coordinate existing efforts and provide technical assistance; and states and community partners adapt practices suited to local conditions (ACL, 2024). Nursing engagement is embedded at multiple points in this chain, particularly in care coordination, caregiver training, and outcomes evaluation, as outlined in Table 2. The structure invites professional leadership to translate strategy into operational standards within care settings and educational curricula. Because implementation relies on voluntary cooperation, professional expertise becomes the main channel through which policy intent materializes. The Act's design also produces predictable systemic effects. The first is sustained attention: mandated updates and public reporting ensure that caregiving remains on the federal agenda, preventing policy drift. The second is gradual standardization: dissemination of effective models and comparative data creates implicit benchmarks without regulatory enforcement. The third is diffusion through professional networks: by including providers and accreditation bodies among its members, the council facilitates the spread of practices through existing professional and institutional channels. These mechanisms leverage reputation and evidence rather than authority, allowing continuous improvement within resource constraints.
Risks within this model are primarily those of uneven implementation and dependence on existing funding streams. Yet the Act's transparency and feedback mechanisms mitigate them by rewarding performance and documenting gaps for future congressional action. Its non-preemption language limits federal overreach, preserving legitimacy while sustaining collaboration. The balance between constraint and coordination is the Act's defining feature: it manages to institutionalize caregiving policy without provoking the fiscal or jurisdictional conflicts that have derailed similar efforts. The synthesis therefore depicts the RAISE Act as a structurally modest but conceptually sophisticated policy. Its success lies in transforming diffuse caregiving pressures into a national learning system supported by recurrent evaluation and stakeholder participation. Through the convergence of Kingdon's (2011) streams, the policy achieved enactment; through the HPT's interacting domains (Walt & Gilson, 1994), it sustains momentum. The design promotes incremental progress through collaboration, evidence use, and professional engagement. Nursing's role within this framework is not ancillary but central, anchoring implementation through care coordination expertise, caregiver education, data generation, and policy advocacy as summarized in Table 2 (Camicia et al., 2016). By embedding iterative evaluation and multi-actor governance, the Act establishes caregiving as a continuous policy enterprise, ensuring that family caregivers remain visible within national health and social policy long after initial enactment.
Discussion
This analysis shows that the RAISE Family Caregivers Act is a structurally modest policy that can still shift practice in meaningful ways. Its strength is not new spending but a durable mechanism for coordination, transparency, and learning. For older adults and their caregivers, these features matter. Care transitions remain fragmented across hospitals, primary care, home health, and long-term services (Naylor et al., 2018). The Act's strategy requirement and reporting cadence can tighten these interfaces if professional actors, especially nurses, translate policy into operational standards. Three implications for care coordination follow from the results. First, the Act's recurring strategy updates create a policy clock that can drive clinical standardization. Health systems should align discharge and handoff protocols to the national caregiving strategy and use the Council's reports as a reference point (ACL, 2024). Nurses are well positioned to lead this alignment through unit-level checklists, EMR prompts that capture caregiver capacity and preferences, and community referrals documented at discharge (Camicia et al., 2016). Second, the Act legitimizes caregivers as partners in the team. Nursing practice can leverage this by building structured “caregiver readiness” assessments into care plans and by using brief, teach-to-goal education with return demonstration for complex tasks like medication management or wound care (Hirschman et al., 2015). Third, since the law relies on soft power, measurement becomes the currency. Nurse scientists should define a parsimonious (carefully selected and minimal) set of caregiver-sensitive outcomes and test them in real settings so that future strategy updates prioritize what works.
The nursing workforce is central to this translation. Table 2 outlines clear leadership pathways. The short-term priority is competency development. Organizations should embed caregiver engagement skills into orientation and continuing education across inpatient, primary care, and home-based services. Content should cover assessment of caregiver strain (Liu et al., 2020), communication under stress, navigation of long-term services and supports (LTSS), and referral pathways for respite and financial counseling. Graduate programs should integrate policy literacy on federal aging and caregiving statutes, since the Act's open processes allow direct input from the profession. A second priority is role design. Advanced practice nurses can anchor complex care clinics that include structured caregiver coaching and telehealth follow-ups in the first 30 days post-discharge (Naylor et al., 2014). These clinics can serve as demonstration sites that feed data to the federal reporting cycle, accelerating diffusion. Equity considerations are critical to successful implementation. Because the Act relies on voluntary adoption rather than mandates, health systems with greater resources may more readily implement evidence-based caregiver practices, while under-resourced safety-net settings may struggle to participate. This could inadvertently widen existing disparities in caregiver support. Nursing leaders should therefore pair adoption with equity safeguards. Practical steps include proactive identification of caregivers with limited English proficiency, standardized social risk screening for financial strain and housing instability, and dedicated partnerships with Area Agencies on Aging and community organizations in rural and minority communities (Schulz & Eden, 2016). The national strategy can support this by highlighting models that close disparities (ACL (2022)), but local nursing leadership must operationalize equity checks in everyday care.
The Act's political design has trade-offs that nursing can mitigate. Absence of new funding constrains scale. Yet transparency and technical assistance can still produce change if professional networks carry the signal. Nursing organizations should coordinate submissions during public comment periods (Federal Register, 2022), propose uniform measures, and request that successful models be packaged as implementation toolkits. At the system level, chief nursing officers can designate a “RAISE liaison” who tracks Council outputs, aligns internal policies with federal guidance, and reports outcomes tied to the strategy domains. These moves convert a light federal touch into concrete local action. There are risks. Implementation may be uneven. Reporting may devolve into compliance rather than improvement. Caregiver education efforts can be shallow if not linked to follow-up and reinforcement. To counter these risks, the profession should emphasize rigorous evaluation designs and simple feedback loops. For example, a two-measure bundle such as 30-day unplanned utilization and a validated caregiver strain score (del-Pino-Casado et al., 2021) can anchor small tests of change. Publishing these results in accessible venues and routing them to the Advisory Council will help the most practical models rise in the national strategy.
Future research should focus on three areas. First, dosage and timing of caregiver training during episodes of acute care and at home. Second, the marginal impact of nurse-led coordination versus usual practice on caregiver health, not only patient outcomes (Legault et al., 2021). Third, the economic case for caregiver integration across Medicare and Medicaid, including effects on skilled nursing admissions and length of stay. Studies should prioritize pragmatic designs and multi-site collaboratives to accelerate uptake. Policy refinement is also feasible within the current statute. The Council could endorse a core caregiver assessment template for use at admission and discharge, with optional fields for specialty populations. It could also identify a short list of quality indicators that systems can adopt without heavy IT build. Finally, it could highlight contracting and payment arrangements that reward caregiver engagement, such as modest add-on payments for documented education and coordination activities in post-acute episodes. These steps do not require new appropriations yet would clarify expectations and reduce variation. Overall, the Act gives nursing a national platform to solve longstanding coordination problems for older adults and their families (Reinhard et al., 2019). Its governance design matches nursing's comparative advantages: systems thinking, team leadership, and practical measurement. If nurses bring clear standards, simple metrics, and tested models to the biennial strategy cycle, the policy will produce cumulative gains even without large new funding. The opportunity now is to move from a national learning agenda to local routines that make caregiving visible in every plan of care and in every care transition.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.