
Abstract
Introduction
Violence toward the healthcare workforce is on the rise, impacting the quality of care provided. This study aims to assess the frequency of violence against healthcare workers (HCWs) and determine any existing disparities between private and public settings.
Methods
A cross-sectional study design was used. Data were collected from April 1, 2022, to November 30, 2022, through a structured online questionnaire, adapted from a self-reported structured questionnaire. The survey was circulated via social media platforms among HCWs in both public and private tertiary care hospitals in Pakistan. A total of 365 participants completed the survey.
Results
The frequency of violence among respondent HCWs was 38.36%. The frequency of violence was higher in public sector hospitals compared to private sector hospitals (54.03% in public vs. 30.29% in private). Incidents of physical violence were reported by 12.10% of public versus 5.39% of private sector respondents. Verbal abuse was reported by 36.29% of public vs. 21.16% of private sector respondents. Racial harassment was experienced by 12.90% of public and 9.54% of private sector respondents, while sexual harassment was reported by 11.29% of public versus 6.22% of private sector respondents.
Conclusion
A higher frequency of violence was observed in public hospitals compared to private sector hospitals, across all types of violence. These findings highlight the need for increased awareness among HCWs about existing policies on reporting workplace violence and the importance of utilizing these policies to ensure protection for all HCWs in both public and private tertiary care hospitals.
Key Messages
Workplace violence (WPV) against healthcare workers (HCWs) is a significant issue globally, particularly in low- and middle-income countries like Pakistan. Public sector hospitals are generally more vulnerable to such incidents, but comprehensive data comparing violence between public and private healthcare sectors in Pakistan remains limited.
This study reveals that WPV is more frequent in public sector tertiary care hospitals compared to private sector hospitals in Pakistan. It provides detailed insights into the types of violence (physical, verbal, racial, sexual) faced by HCWs and highlights the risk factors such as gender, profession, and age that increase vulnerability to WPV, especially in public hospitals.
The findings underscore the urgent need for policy reforms and tailored interventions in public healthcare institutions to mitigate WPV. The study may inform future research on preventive strategies, inspire policymakers to develop reporting mechanisms, and shape the implementation of comprehensive violence prevention programs in healthcare settings.
Introduction
Workplace violence (WPV) has become a critical global concern, with the healthcare sector facing the highest risk compared to other industries (Kafle et al., 2022; World Health Organization [WHO] et al., 2002). WPV not only threatens the safety of healthcare workers (HCWs) but also undermines healthcare systems, impeding the quality of care and patient outcomes (Vento et al., 2020). HCWs encompass a broad spectrum of professionals, including doctors, nurses, technicians, aides, and even domestic staff, all of whom remain vulnerable to violence within healthcare settings (Mohanty et al., 2019; O’Brien et al., 2024).
The issue has intensified in recent years, especially with the COVID-19 pandemic, which amplified existing healthcare pressures and exposed HCWs to both heightened aggression and psychological strain (Bhatti et al., 2021). A recent global review by Devi et al. highlighted how the pandemic increased aggression toward HCWs, especially in resource-limited settings, due to misinformation, fear, and overburdened systems (Devi, 2020). Global estimates from the WHO suggest that 8–38% of HCWs experience physical violence during their careers, underscoring the widespread nature of this problem (Rahama et al., 2025). While these figures highlight the widespread nature of WPV, they may not fully capture the challenges in low- and middle-income countries (LMICs) like Pakistan, where institutional resources, enforcement mechanisms, and cultural attitudes toward violence differ significantly from high-income settings.
In Pakistan, a study during the COVID-19 pandemic found 41.9% of HCWs, including doctors, paramedics, and technicians, experienced some form of violence within 2 months (Shaikh et al., 2021). However, reported figures likely underestimate the true scale due to significant underreporting, driven by the normalization of violence in healthcare and a lack of clarity among HCWs regarding what constitutes violence (McGuire et al., 2021; Spencer et al., 2023). Additionally, global definitions and prevention frameworks for WPV, such as those by the WHO and International Labor Office (ILO), may not adequately account for local factors like political instability, religiously fueled misinformation, or weak administrative enforcement in Pakistan's healthcare system (Laposa et al., 2003).
The perpetrators and nature of violence vary by context. While patients and attendants are commonly implicated, studies also highlight internal workplace dynamics as sources of violence, with incidents involving colleagues and faculty members being reported, particularly in South Asian settings (Kowalenko et al., 2005; Zubairi et al., 2019). Contributing factors include systemic issues such as overcrowding, long wait times, staff shortages, miscommunication, and the presence of psychiatric patients, all of which foster volatile environments conducive to violence (Di Prinzio et al., 2022; Gacki-Smith et al., 2009).
WPV takes a heavy toll on HCWs’ psychological well-being, contributing to stress, depression, job dissatisfaction, and, ultimately, attrition from the workforce (O’Brien et al., 2024; Zafar et al., 2013). Vulnerabilities increase under specific conditions, such as excessive work hours or when misinformation—exacerbated by low literacy levels and religiously fueled conspiracy theories—drives public mistrust toward healthcare systems, as seen in Pakistan during the pandemic (Gabarron et al., 2021; Shaikh et al., 2021; Tian et al., 2020).
Recent studies from LMICs, such as those by Khiyani et al. (2023) in India and Chowdhury et al. (2023) in Bangladesh, have further illustrated how strained healthcare systems, misinformation, and socioeconomic disparities contribute to increased violence against HCWs in LMIC settings.
Despite growing recognition of WPV, its frequency and associated risk factors remain underexplored in Pakistan, particularly when comparing public and private tertiary care hospitals. This is significant, as patient demographics, expectations, and institutional policies often differ across these settings, potentially influencing WPV trends (Bhatti et al., 2021; Shaikh et al., 2020).
Guided by the Ecological Model, which frames violence as the product of multiple interacting factors across individual, organizational, and societal levels, this study investigates the frequency and determinants of WPV, including setting (public vs. private), age, gender, and profession. Addressing this knowledge gap is essential for developing multi-level, contextually appropriate interventions to protect HCWs and improve health system functioning in Pakistan. These findings are framed within the evolving global discourse on WPV in LMICs and are critical for informing targeted interventions that safeguard HCWs and enhance healthcare delivery quality.
Materials and Methods
Study Design and Population
A cross-sectional survey design was employed to provide a snapshot of the frequency and associated factors of WPV among HCWs in Pakistan. Cross-sectional studies are suitable for estimating the prevalence of health-related phenomena and exploring associations at a specific point in time, particularly when time and resource constraints preclude longitudinal approaches (Wang & Cheng, 2020). This design is frequently used to assess WPV in healthcare settings (Shaikh et al., 2021).
Data were collected from April 1, 2022, to November 30, 2022, using a self-reported structured questionnaire distributed to HCWs from both public and private tertiary care hospitals in Pakistan. Distribution was conducted via official emails in major cities (Karachi, Islamabad, Peshawar, and Lahore) and through social media platforms (WhatsApp, Facebook, Twitter, and Instagram) to maximize reach. The questionnaire was hosted on Google Forms to ensure accessibility and ease of data collection. Only individuals confirming their status as HCWs were included in the final analysis.
A snowball sampling strategy was utilized, whereby initial participants were encouraged to share the survey link with colleagues. This approach was chosen due to the sensitivity of the topic of WPV and the difficulty in accessing a diverse group of HCWs across both public and private sector hospitals. Snowball sampling facilitated recruitment from a wider pool of participants who might otherwise have been reluctant to respond due to fear of stigma, retaliation, or lack of institutional support. While snowball sampling enables access to hard-to-reach populations, it carries a risk of sampling bias due to peer-network homogeneity and may overrepresent certain groups (Naderifar et al., 2017).
HCWs including attending physicians, nurses, house officers, residents, interns, and clinical-year medical students who had at least 1 year of experience in at least one healthcare setting and consented to participate were included in the study. HCWs who had less than 1 year of experience or did not consent to participate were excluded from the study.
To ensure our participants fulfill our eligibility criteria, i.e., belonging to and working in a healthcare setting, Q3 of Section of Personal and Workplace Data assesses the nature of the profession of the participant. Any response stating a profession that didn’t fulfill our eligibility criteria was not recorded in our database.
The Sample Size for this study was calculated using the single proportion formula in the application Open Epi version 3.5. Assuming the frequency of violence in the health sector of Pakistan ranges between 38.4% and 40% (Shaikh et al., 2021) and using a 95% confidence interval (CI) for a two-sided normal distribution, a total of 364 participants were enrolled in this study. Design effect = 1, precision (tolerated margin of error) = 5%, significance level =5%, non-response rate = 5%.
Measurement Tools
The study questionnaire was adopted from a survey tool created by the Joint Program on Workplace Violence in the Health Sector of the ILO, the International Council of Nurses, the WHO, and the Public Services International (ILO/ICN/WHO/PSI Joint Program) (WHO et al., 2002). The questionnaire has been used in previous studies and has been previously tested and credited. The questionnaire was entered into a Google Form, and a link was generated to be circulated among social media and online messaging platforms. Versions of the questionnaire were the first pilot-tested with a sample of five healthcare professionals working at Aga Khan University Hospital (AKUH). A member of the team then asked the respondents about their understanding of the questions and whether they had any feedback or questions. The feedback was incorporated, and some changes were made to better fit the context of a Pakistani hospital setting. The final edited questionnaire was then used in this study after getting approval from the Ethics Research Committee of the AKUH.
We distinguished the responses of participants coming either from a public or a private healthcare setting by Q5, in the section of Personal and Workplace Data of our questionnaire. Public sector hospitals in Pakistan are typically government-funded and government-run hospitals. In contrast, private sector hospitals are generally run and funded through private investments or fees. This distinction was communicated clearly in the survey instructions to ensure participants could categorize their responses appropriately. Through this tool, we were able to keep track of responses received from the participants.
To prevent multiple submissions by the same individual, the online questionnaire included a unique identifier to track and limit responses, as well as collecting emails and limiting responses to one response per email. To ensure that only HCWs participated, the questionnaire included specific questions about the respondent's profession, place of work, and role within the healthcare setting. Only individuals who confirmed their employment as HCWs were included in the final analysis.
All investigators had access to the Google Forms submissions throughout the study. The questionnaire was divided into six main sections: the personal and workplace data, sections on the different types of violence physical, verbal, and sexual harassment, and violence due to religion/ethnicity, and a final section to assess policies by the healthcare providing institute to defend HCWs. The frequency of having experienced the relevant type of violence was recorded as a “yes” or “no.” Follow-up questions were asked on whether a weapon was involved, the identity of the attacker, the time and place of the attack, and the consequences for the attacker. The questionnaire also aims to analyze the different policies present in different hospitals regarding the reporting of these incidents and a 4-point scale measures how effective HCWs find these policies (very effective, moderate, little, or not at all effective).
Another set of questions to assess long-term mental impacts asked the respondents to describe how bothered they have been since the last attack by (1) repeated, disturbing memories, thoughts, or images of the attack; (2) avoiding thinking about or talking about the attack or avoiding having feelings related to it; (3) being “super alert” or watchful and on guard, and (4) feeling like everything they did was an effort? measured on a 5-point scale (“Not at All,” “A Little Bit,” “Moderately,” “Quite a Bit,” and “Extremely”). The third section was related to psychological violence or verbal abuse, defined as “bullying, mobbing, harassment, and verbal abuse that humiliates, degrades, or otherwise indicates a lack of respect for the dignity and worth of an individual.” The primary question of interest in this section was whether, in the last 12 months, the respondent had been verbally abused in the workplace and if so, how often. Follow-up questions were related to disturbing memories, etc., like those for physical attacks, referring to the last time that the respondent was verbally abused in the workplace.
Statistical Analysis
The data collected were exported to Microsoft Excel and analyzed using Stata version 17.0 (StataCorp LP, College Station, TX, USA). Categorical variables were expressed as frequencies and percentages. Chi-square tests were performed to assess associations between categorical variables, with Fisher's exact test applied when expected cell counts were small.
To identify factors independently associated with WPV, multivariable logistic regression analyses were conducted. We employed backward stepwise logistic regression, where all candidate variables were initially included, and variables were sequentially removed based on significance levels (removal criterion p > .10) to obtain the most parsimonious model. We checked for multicollinearity among independent variables using the variance inflation factor (VIF), with all VIF values below 2, indicating no significant multicollinearity.
Adjusted odds ratios (aOR) with corresponding 95% CIs and p-values were reported to quantify the strength and precision of associations. A two-sided p-value of <0.05 was considered statistically significant. Internal consistency reliability (e.g., Cronbach's alpha) was not calculated for the study instrument, as the questionnaire was adopted from a previously validated tool developed by the ILO/ICN/WHO/PSI Joint Program on Workplace Violence in the Health Sector (WHO et al., 2002), and had already been validated in Pakistan. The tool has been applied in multiple studies within Pakistan and other LMICs with good reliability, supporting its applicability in our context.
Ethical Considerations
The study was approved for exemption from the Ethics Review Committee of AKUH, Karachi, Pakistan (ERC No: 2022-7326-21172). Informed consent was obtained from all participants after they were informed about the study's objectives, procedures, and their right to withdraw at any time.
Results
Three Hundred and Sixty- Five (365) participants answered our questionnaire and agreed to participate in the study. Two hundred and fifty-four participants were <25 years old (69.59%), whereas 127 (34.79%) were male and 238 (65.21%) were females (Table 1). Two hundred and fifteen (58.90%) participants were medical students with exposure of 1 year or more in their clinical rotations, making our study sample heavily skewed toward medical students. This reflects the ease of recruitment within this group through academic and peer networks. Most participants (82.74%) fell under the category of 1–5 years of experience, and the majority (93.42%) had direct exposure to patients. A total of 140 (38.36%) individuals experienced violence during their working hours in the last 12 months. Sixty-six percent of the participants were working in a private-sector hospital,and 33.88% were from the public sector (Table 1).
Socio-Demographic Characteristics of the Healthcare Workers (n = 365).
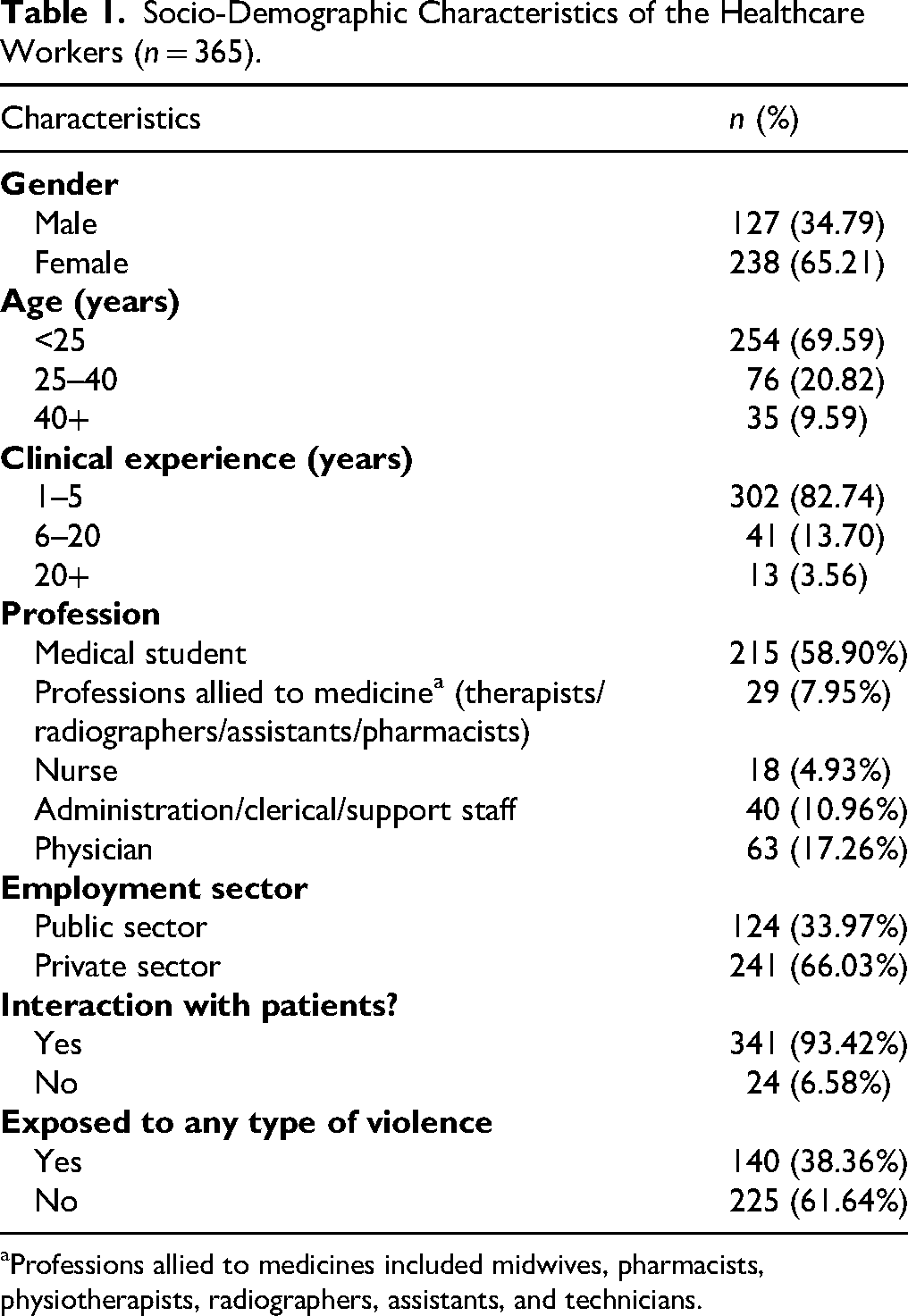
Professions allied to medicines included midwives, pharmacists, physiotherapists, radiographers, assistants, and technicians.
Among the 140 individuals who faced some sort of violence in the last 12 months, 32 had faced 2 categories of violence, 7 had faced 3 different types of violence, and 2 individuals reported facing all 4 types of violence. Hence, the total count of different types of violence faced in the last 12 months was 192. Participants from public sector hospitals showed a higher frequency of violence (72.58%) compared to private sector (42.31%), this difference was statistically significant (p = .000). Verbal abuse is the most common form of violence seen in 96 healthcare providers (private 21.16% vs. public 36.29%; p = .002). Thirty-nine respondents experienced racial harassment (private 9.54% vs. public 12.90%; p = .325). Twenty-nine suffered sexual harassment (private = 6.22%, public = 11.29%; p = .090). whereas 28 healthcare providers faced physical violence (private = 5.39%, public = 12.10%; p = .023) at their workplace (Figure 1). There was a significant association seen with the sector of the hospital and physical violence as well as verbal abuse (p < .05) (Table 2).
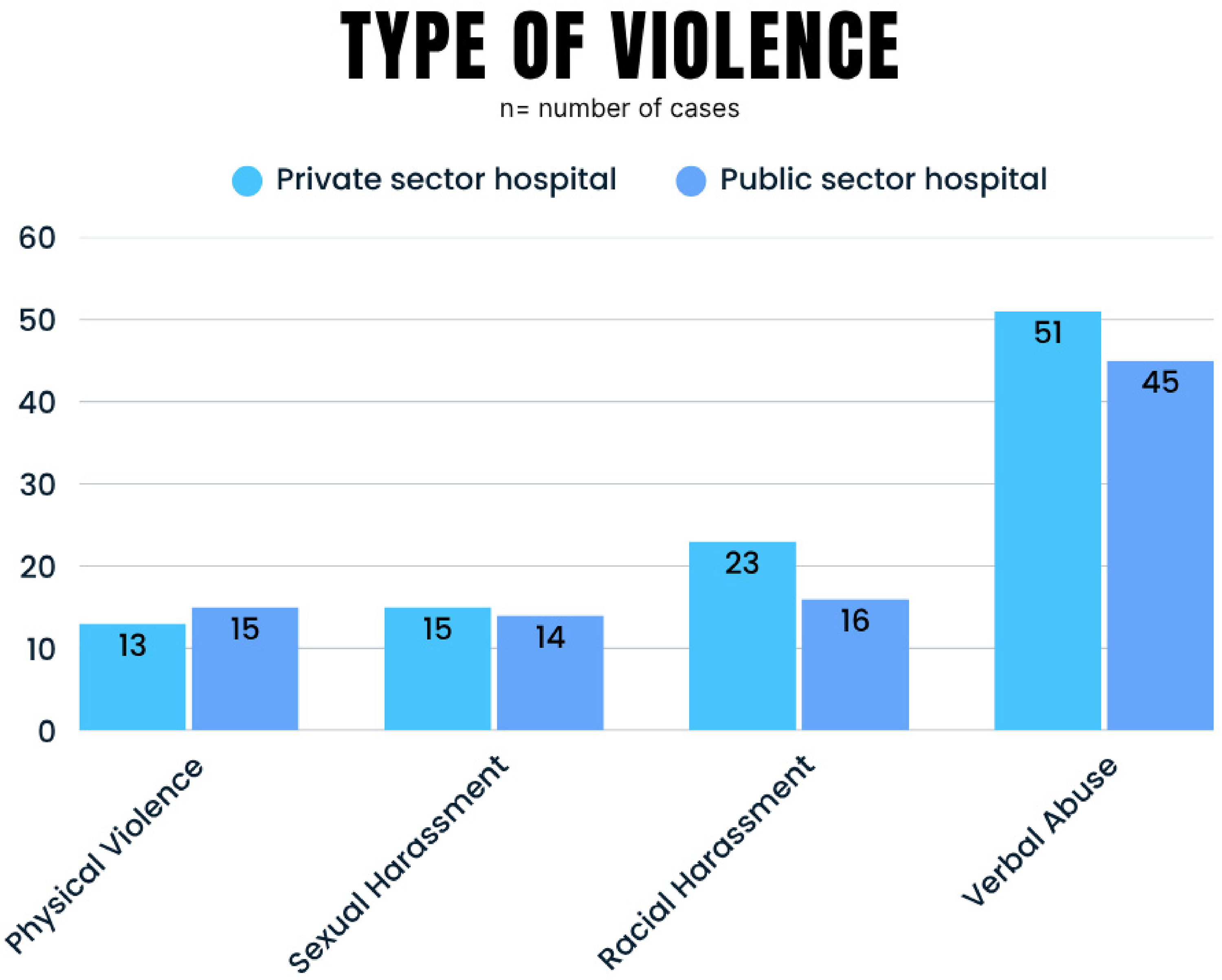
Type of violence (public vs. private hospital).
Frequency of Different Kinds of Violence Among Healthcare Workers in the Public and Private Sector Hospitals (n = 140).

In private sector hospitals, workers aged more than 40 years of age (57.14%) experienced a higher frequency of violence than those between 25 and 40 years (28.64%) and those under 25 years (25.00%), this was statistically significant (p = .005). There was a higher frequency of violence seen in males (35.71%) as compared to females (27.39%); however, this was not statistically significant (p = .180). A statistically significant association was noted between the profession of respondents and violence faced (p = .000). Medical students faced the lowest frequency of violence (20.81%) followed by administration/clerical/support staff (28.00%), whereas professions allied to medicine (56.25%), physicians (51.28%), and nurses (50.00%) had the highest frequency of violence (Table 3).
Factors Associated With Workplace Violence Among Private Sector HCWs (n = 241).
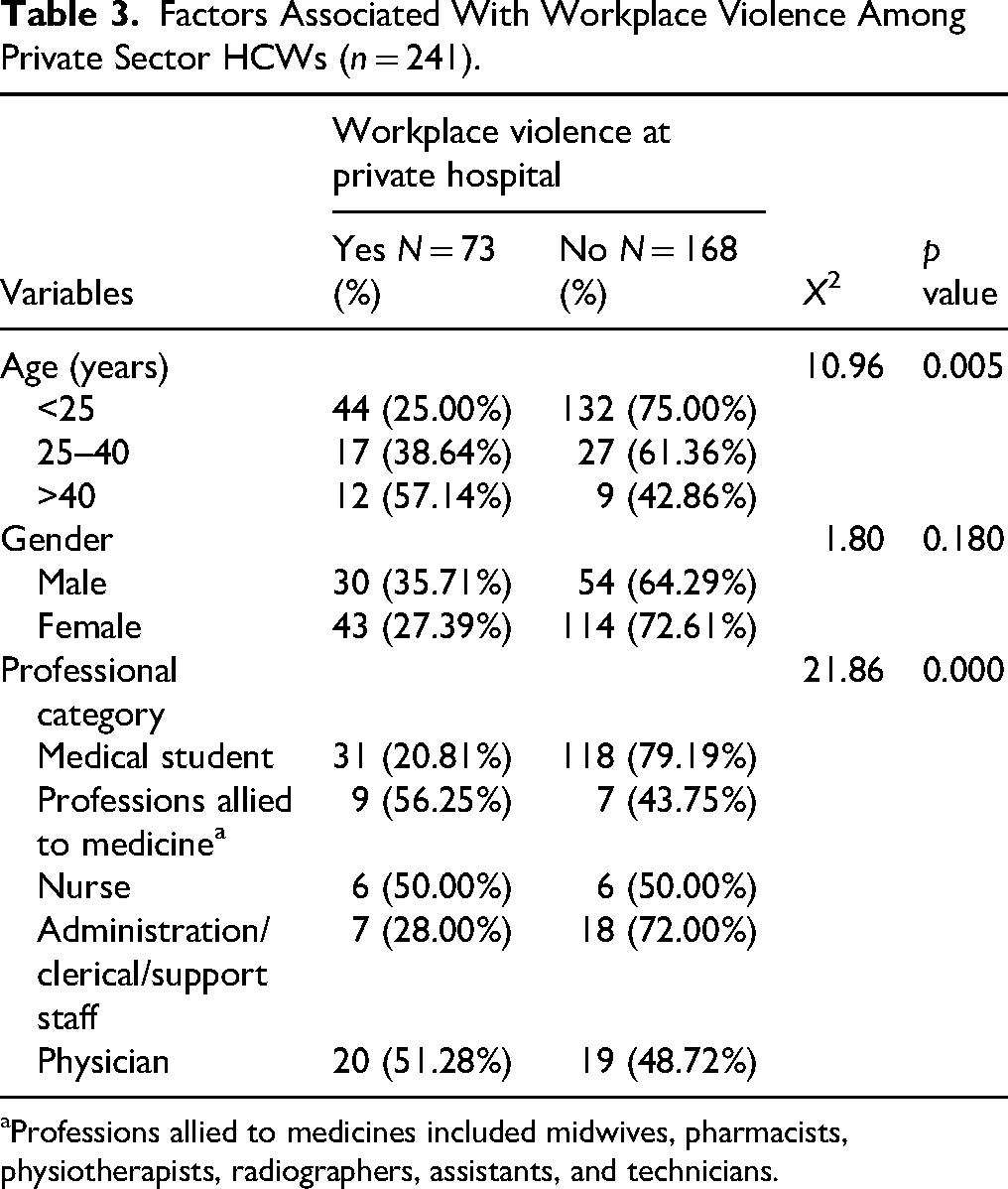
Professions allied to medicines included midwives, pharmacists, physiotherapists, radiographers, assistants, and technicians.
In public sector hospitals, workers aged between 25 and 40 years (75.00%) experienced a higher frequency of violence which was comparable to those aged more than 40 years of age (71.43%). The frequency of violence in those aged less than 25 years (42.31%) was much lower than in the other two categories, this was statistically significant (p = .003). No significant association (p = .640) was noted between genders and violence faced with females (55.56%) and males (51.16%) having quite similar frequency. Physicians were seen to have faced the highest frequency of violence (83.33%), these were followed by nurses (66.67%), administration/clerical/support staff (66.67%), and professions allied to medicine (61.54%) who all had quite similar frequencies, whereas medical students reported the lowest frequency of violence (37.88%). A statistically significant association was noted between the profession of respondents and violence faced (p = .002) (Table 4).
Factors Associated With Workplace Violence Among Public Sector HCWs (n = 124).
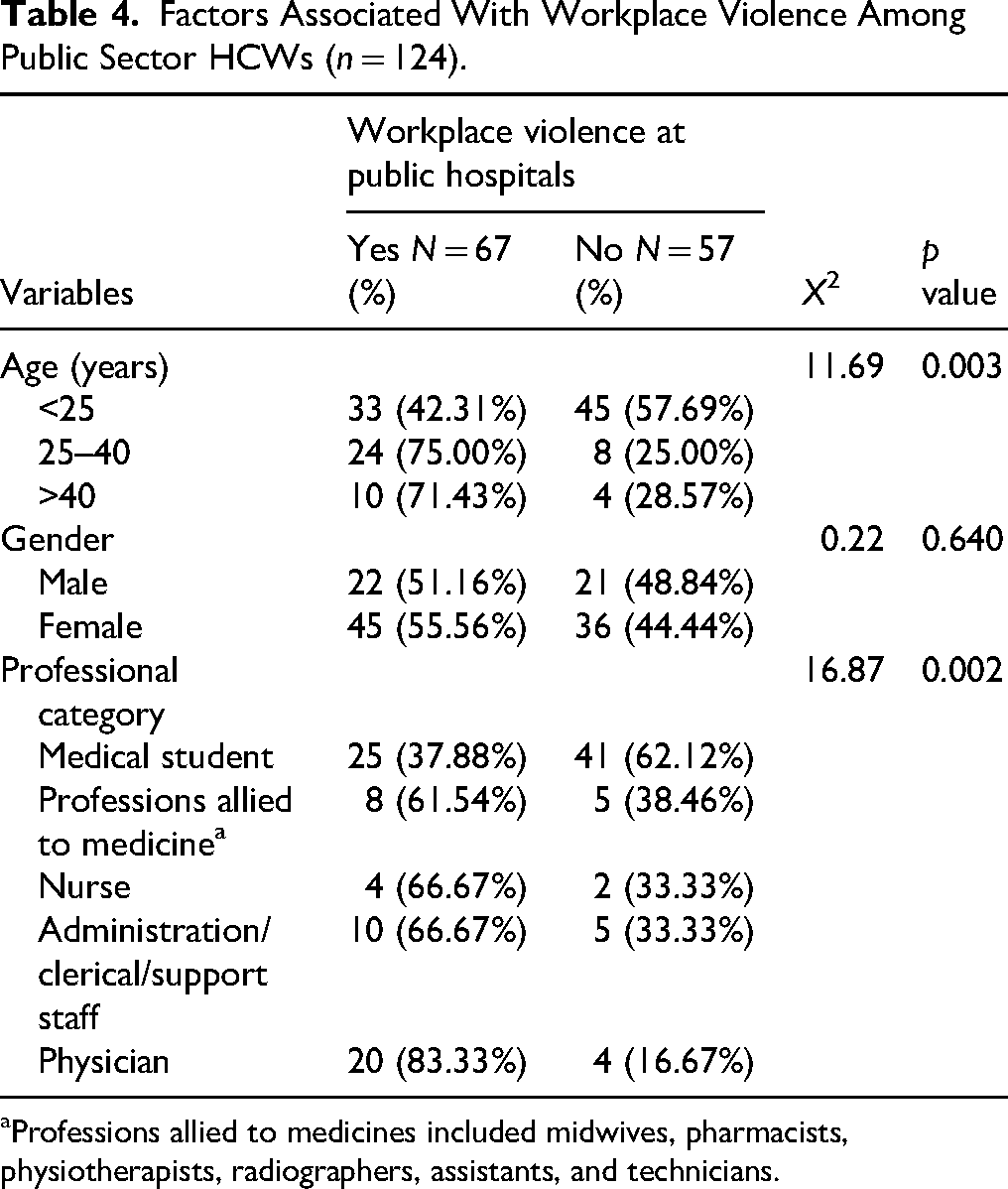
Professions allied to medicines included midwives, pharmacists, physiotherapists, radiographers, assistants, and technicians.
Discussion
This study investigates the frequency and risk factors of WPV faced by HCWs in public versus private tertiary care hospitals in Pakistan. While WPV has been documented globally, comparative data from LMICs like Pakistan, especially between healthcare sectors, remain limited. Our study addresses this gap by providing insights into violence patterns and determinants in both public and private healthcare settings. Although medical students formed the majority of our respondents, their experiences provide an important lens into the vulnerabilities of trainees who represent the future healthcare workforce. Addressing WPV at the level of students is critical, as early exposure may normalize violence and contribute to workforce attrition in LMICs.
Our findings reveal that violence toward HCWs is significantly more prevalent in public than private tertiary care hospitals, across all forms of violence examined (Figure 1). Of the 140 respondents, 38.36% reported experiencing some form of violence in the past 12 months. Although this figure is slightly lower than the 41.9% reported during the height of the COVID-19 pandemic in Pakistan (Shaikh et al., 2021), it remains concerning and reflects the persistent risks HCWs face, even beyond the pandemic's peak.
A key finding is the significantly higher rates of physical violence (12.10% in public vs. 5.39% in private hospitals) and verbal abuse (36.29% in public vs. 21.16% in private hospitals). These patterns align with existing literature suggesting that public hospitals, which often serve larger, lower-income, and more critically ill patient populations, face unique challenges that exacerbate tensions and violence (Khan et al., 2021; Toska et al., 2023). Overcrowding, limited resources, long waiting times, and patient dissatisfaction are more pronounced in public sector facilities, creating an environment conducive to aggression (Di Prinzio et al., 2022; Gacki-Smith et al., 2009; Khan et al., 2021).
Moreover, differences in security infrastructure and administrative responsiveness between sectors may partly explain the disparity. Private hospitals often have stricter visitor controls, better-trained security personnel, and clearer reporting pathways, making violent incidents less likely or more swiftly addressed (Akinleye et al., 2019; Basu et al., 2012). In contrast, bureaucratic challenges, underfunding, and higher patient volumes limit public hospitals’ ability to implement and enforce safety protocols effectively.
Beyond institutional differences, our analysis also reveals demographic and professional risk factors for WPV. HCWs aged over 25, particularly physicians, nurses, and allied health professionals, are significantly more likely to experience violence compared to younger individuals or medical students. This pattern can be attributed to increased patient-facing responsibilities among these groups. Physicians and nurses, in particular, engage directly with patients and families during high-stakes moments, including emergency care, diagnosis delivery, and critical procedures, making them more vulnerable to aggression (Ahmer et al., 2008; (ICRC) ICOTRC, 2021).
Healthcare hierarchies also exacerbate interprofessional tensions that contribute to WPV (Lee & Lee, 2024). In South Asian hospitals, steep authority gradients mean that junior doctors and nurses often absorb pressures from both directions—patients and their families on one side, and senior physicians or administrators on the other (Khiyani et al., 2023). This “dual vulnerability” places them at heightened risk of mistreatment, bullying, or scapegoating during adverse outcomes or resource shortages ((ICRC) ICOTRC, 2021; Kowalenko et al., 2005; Zubairi et al., 2019). Thus, WPV reflects both external aggression and internal organizational culture issues. Moreover, hierarchical cultures may discourage reporting, as younger or lower-ranked staff fear retaliation or lack confidence in institutional redress mechanisms (Lee & Lee, 2024). These internal structural drivers highlight that WPV is not merely episodic but embedded in the organizational culture of healthcare systems in LMICs.
To compound this issue, in LMIC contexts, WPV cannot be separated from broader gendered hierarchies within healthcare (Rahama et al., 2025). Female nurses, who form the majority of Pakistan's nursing workforce, face a dual burden: as frontline providers, they are disproportionately exposed to aggression from patients and attendants, while within hospitals, they navigate entrenched power imbalances that marginalize their voices, limit decision-making authority, and normalize disrespectful or abusive behaviors from senior colleagues. These intersecting professional and gendered hierarchies place nurses at heightened risk of verbal, psychological, and even sexual harassment (Abdulwehab & Kedir, 2025; Kafle et al., 2022; Spencer et al., 2023). Consistent with global literature, our study also identified nurses as a particularly vulnerable group, reflecting structural and cultural dynamics in LMICs where nurses often serve as the first point of contact for patients, manage frontline care delivery, and work within rigid hierarchies that expose them simultaneously to patient-driven aggression and internal workplace abuse (Lee & Lee, 2024; Melnyk et al., 2020).
The implications of WPV toward nurses extend beyond individual harm; they contribute to workforce attrition, burnout, and reduced care quality, ultimately exacerbating healthcare system weaknesses in LMICs like Pakistan (Shaikh et al., 2020; Shaikh et al., 2021). Given the critical role nurses play in care continuity and patient outcomes, targeted interventions to protect and empower them are essential. Policies should include robust enforcement of anti-violence protocols, accessible reporting mechanisms, legal protections against harassment, and workplace culture reforms that promote dignity and equity. These findings resonate with broader challenges faced by the Global South, where resource constraints, sociopolitical instability, and fragile health systems intensify risks for HCWs, particularly nurses. Our study contributes to the global discourse by providing context-specific evidence from Pakistan, underscoring the urgency for tailored, multi-level strategies to safeguard HCWs.
Patient expectations and societal mistrust toward healthcare systems also play a critical role. In LMICs like Pakistan, lower health literacy, economic disparities, and misinformation—often amplified by religious or political narratives—fuel unrealistic patient expectations and frustration with perceived system failures (Gabarron et al., 2021; Gillespie et al., 2010; Tian et al., 2020; Zafar et al., 2013). Public sector patients, who often lack alternative care options, may express dissatisfaction more aggressively, particularly when outcomes do not meet expectations.
Our study underscores the need for tailored, multi-level interventions to address WPV. Public sector hospitals, in particular, require enhanced security measures, clear reporting pathways, and administrative accountability. Additionally, training HCWs in de-escalation techniques, communication skills, and stress management is essential, especially for those in high-risk roles like physicians and nurses.
Furthermore, systemic factors must be addressed. Improving resource allocation, reducing staff shortages, and fostering a more supportive organizational culture can mitigate triggers for violence. Interventions must also account for sociopolitical factors, including combating misinformation and enhancing public trust in healthcare.
This study has notable strengths, including sectoral comparison and a diverse sample from multiple provinces. However, limitations exist. Our sample was disproportionately composed of medical students, which may limit representativeness of frontline HCWs such as nurses and paramedics who are often more directly exposed to WPV. While medical students bring valuable insights, particularly regarding violence during clinical rotations, their experiences may differ from those of full-time frontline HCWs. Second, the use of snowball sampling, while practical for reaching HCWs on a sensitive issue such as WPV, introduces the possibility of sampling bias. Findings may be influenced by peer-network homogeneity, potentially limiting representativeness and generalizability to the wider healthcare workforce. Similarly, self-reported data introduces potential recall or social desirability biases.
Moreover, rural HCWs were underrepresented, which limits the generalizability of our findings to predominantly urban tertiary care settings. This gap is important given that rural HCWs may face different patterns and drivers of WPV due to limited resources, weaker security infrastructure, and sociocultural differences. Future studies should purposively recruit rural HCWs to capture these unique experiences and allow for more comprehensive, nationally representative comparisons. Lastly, the cross-sectional design restricts the ability to infer causality between risk factors and violence exposure, as associations observed in this study cannot establish temporal or causal relationships. Therefore, our findings should be interpreted as correlational rather than causal. Future longitudinal or mixed-methods studies are needed to better examine causal pathways and underlying mechanisms. Despite these limitations, our findings provide a foundation for future research and policy action to protect HCWs and strengthen healthcare delivery in Pakistan.
Conclusion
Our study revealed a higher frequency of WPV in public hospitals compared to private sector hospitals in Pakistan, with significant associations between violence and factors such as HCW's age, profession, and employment sector. Physicians, nurses, and allied health professionals, particularly males over 25 in public hospitals, are at increased risk.
These findings contribute to the broader understanding of WPV in healthcare settings, particularly in LMICs like Pakistan, and underscore the need for urgent, tailored interventions. Our study also challenges assumptions about the uniformity of WPV across different healthcare settings, indicating the need for differentiated strategies tailored to each sector's unique challenges. This underscores the urgency for comprehensive WPV prevention programs that include clear reporting mechanisms, enforcement of security protocols, and ongoing training for HCWs.
Future research should focus on longitudinal analyses to assess intervention impacts and explore other risk factors, such as the long-term effects of the COVID-19 pandemic on WPV in healthcare. This study provides a foundation for such research and offers essential insights for informing policy and practice to safeguard HCWs and improve healthcare delivery in Pakistan.
Footnotes
Acknowledgments
Not applicable.
Author Contributions
Conceptualization, SMA, FS; methodology, AI and AJ; validation, FS and SS.; formal analysis, SMA, MH, LH, and AR.; data curation, MJ, BY, HR, and ARR; writing—original draft preparation, SMA, HEA, UR, and AI; writing—review and editing, FS and SMA; visualization, HT and LH; supervision, FS, SMA; project administration, FS and SS.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author. The raw data supporting the conclusions of this article will be made available by the authors on request.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved for waiver by the Ethical Review Committee of Aga Khan University (2022-7326-21172 and 30/3/2022).