
Abstract
Legally voluntary psychiatric inpatients can nonetheless experience informal coercion—pressure, leverage, or implied threats without a formal legal order—yet nursing standards and facility oversight often leave it unmeasured and unmanaged. This article synthesizes evidence on coercion mechanisms in inpatient mental health care, links them to patient outcomes, and proposes implementable safeguards. Six mechanism families commonly operate: discharge/placement leverage (delaying discharge or preferred placement unless patients comply); the “legal shadow” (invoking possible involuntary conversion); conditional privileges (phones, visitors, leave, or activities tied to participation); external contingencies (housing, custody, benefits, probation, or immigration consequences linked to hospital recommendations); procedural and documentation pressure (coercive language in plans, notes, or summaries); and interpersonal persuasion that crosses into relational coercion. Across perceived-coercion measurement studies, qualitative accounts, and therapeutic-alliance research, these mechanisms are associated with reduced trust, weaker alliance, trauma symptoms, disengagement, complaints, and higher risk of readmission or adverse events. Nurses are pivotal in privilege decisions, care planning, discharge preparation, and documentation, but often lack clear guidance for reducing coercion while maintaining safety. Policy options evaluated include routine coercion audits, patient advisory review, limits on privilege-conditionality, mandatory documentation review, and targeted training. A recommended package combines brief patient-reported coercion measures, simulation-based nursing education with competency assessment, explicit limits on privilege-based leverage, and independent documentation audits. Implementation requires alignment across hospital governance, state regulators, and professional organizations. Accountability metrics include quarterly coercion scores, privilege-policy adherence, audit findings, competency certification rates, complaint and seclusion trends, and voluntary-to-involuntary conversion ratios. Limitations include observational evidence, legal heterogeneity, and resource constraints.
Keywords
Introduction
Voluntary psychiatric admission—defined as hospitalization initiated or continued with patient consent and without a court order or involuntary commitment statute—serves as the legal basis for the majority of adult inpatient psychiatric care in the United States and comparable health systems worldwide. Data from the Substance Abuse and Mental Health Services Administration indicate that as of 2020, approximately 63% of all psychiatric hospital admissions in the United States were classified as voluntary (Substance Abuse and Mental Health Services Administration, 2022). The voluntary designation carries both legal and therapeutic significance. Legally, voluntary patients retain the right to request discharge and are not subject to the procedural protections—or restrictions—that accompany involuntary commitment. Therapeutically, voluntary admission theoretically supports patient autonomy, shared decision-making, and therapeutic alliance, which nursing ethics frameworks identify as essential to recovery-oriented care (American Psychiatric Nurses Association, 2018).
However, substantial evidence demonstrates that voluntary legal status does not guarantee the absence of coercion. Patients admitted voluntarily can experience what researchers’ term informal coercion, perceived coercion, or treatment pressures—forms of influence, leverage, or threat that operate outside formal legal orders but nonetheless constrain patient choice and autonomy (Gardner et al., 1993; Hoge et al., 1997; Katsakou & Priebe, 2006). Unlike formal coercion, which is authorized by statute and subject to judicial review, informal coercion occurs through discretionary clinical and administrative practices that lie largely outside legal and regulatory oversight. Nurses, who provide continuous bedside care, manage unit routines, make real-time decisions about privileges and safety interventions, and document patient progress, occupy critical positions in the architecture of informal coercion. Yet nursing practice standards, hospital policies, and accreditation requirements provide limited guidance on identifying, minimizing, or monitoring these practices.
Recent scholarship has strengthened the understanding of how communication deficits and power imbalances shape coercion experiences across stakeholder groups. Sugiura et al. (2020) conducted a systematic review and meta-synthesis examining perspectives of service users, informal caregivers, and professionals regarding involuntary psychiatric admission decision-making. Their analysis revealed consistent themes across all groups: lack of communication, marginalization of the service user's voice, and imbalanced authority relationships emerged as central features affecting perceived legitimacy and trust in the treatment relationship. These findings extend to voluntary admission contexts where formal legal protections are absent, but power asymmetries remain. The persistent identification of communication and voice deficits across multiple stakeholder groups—including clinicians themselves—underscores that informal coercion is not simply a patient perception issue but reflects systemic gaps in how treatment decisions are structured and negotiated in inpatient settings.
This gap has policy significance for three reasons. First, informal coercion undermines the therapeutic goals that voluntary admission is meant to support. Evidence links perceived coercion to reduced therapeutic alliance, lower treatment engagement, increased trauma symptoms, and higher rates of premature discharge against medical advice (Katsakou et al., 2010; Newton-Howes & Mullen, 2011; Sheehan & Burns, 2011). Second, informal coercion raises ethical and legal questions about the boundary between persuasion and compulsion, the validity of consent under pressure, and the transparency of the treatment relationship (Szmukler & Appelbaum, 2008). Third, addressing informal coercion may reduce reliance on formal coercion, including involuntary commitment and mechanical restraint, by building trust and cooperation rather than dependence on authority (Keski-Valkama et al., 2010).
This article offers a policy-oriented analysis of informal coercion in voluntary inpatient mental health nursing. The analysis proceeds in four steps. First, it clarifies what counts as informal coercion and distinguishes it from legitimate clinical influence. Second, it maps the mechanisms through which informal coercion operates in nursing practice and service delivery. Third, it reviews the evidence base linking these mechanisms to patient outcomes. Fourth, it evaluates policy options, recommends an implementable package of safeguards, specifies an implementation plan, and proposes accountability metrics. The article focuses on adult general psychiatric inpatient units in the United States but identifies principles that generalize to other jurisdictions with voluntary admission frameworks.
Methods
This analysis synthesizes evidence from peer-reviewed research, policy documents, and professional practice guidelines. Literature searches were conducted in PubMed, PsycINFO, and CINAHL databases using terms including “perceived coercion,” “informal coercion,” “voluntary psychiatric admission,” “inpatient mental health,” “therapeutic alliance,” and “nursing.” Searches covered publications from 1990 to 2025. Additional sources were identified through reference lists and consultation with subject matter experts.
The literature base on informal coercion in voluntary inpatient settings remains relatively sparse, particularly regarding nursing-specific interventions. Foundational measurement and conceptual work derive primarily from the 1990s and early 2000s, including the development of the MacArthur Perceived Coercion Scale (Gardner et al., 1993) and procedural justice frameworks (Lidz et al., 1995; Monahan et al., 1995). More recent scholarship has expanded understanding of stakeholder perspectives (Sugiura et al., 2020), human rights implications (Pértega & Holmberg, 2023, 2025), and mechanisms of influence, though systematic intervention research remains limited. This gap highlights the need for implementation science focused on reducing informal coercion in routine inpatient nursing practice.
Conceptual Clarification: Defining Informal Coercion in Voluntary Inpatient Care
Informal coercion refers to influence tactics that limit patient choice through pressure, leverage, or threat without invoking formal legal authority. The term encompasses a range of practices including explicit threats (e.g., “If you refuse this medication, we will petition the court for involuntary status”), conditional offers (e.g., “You can have phone privileges once you attend group therapy”), leverage over external contingencies (e.g., “The housing authority requires our recommendation that you are treatment-compliant”), and relational pressure (e.g., repeated persuasion that frames refusal as irrational or harmful). These practices differ from formal coercion, which operates through statutory involuntary commitment procedures, court-ordered treatment, or emergency detention laws that trigger due process protections, including legal representation, evidentiary hearings, and appeals.
The conceptual challenge lies in distinguishing informal coercion from legitimate clinical persuasion. All therapeutic relationships involve influence. Nurses educate patients, recommend treatments, express clinical concern, and structure environments to promote safety and recovery. These activities are not inherently coercive. The literature on perceived coercion, informed by procedural justice theory, identifies three features that distinguish coercive influence from acceptable persuasion: (a) outcome control, where the influencer holds unilateral power over valued outcomes such as discharge, privileges, or placement; (b) transparency deficits, where the patient does not understand the basis for decisions or believes they lack genuine choice; and (c) voice restriction, where the patient's preferences are not solicited, heard, or addressed (Lidz et al., 1995; Monahan et al., 1995). Informal coercion occurs when nurses or treatment teams leverage outcome control without transparent communication or meaningful incorporation of the patient's voice.
This definition allows for legitimate uses of authority. For example, a nurse who denies a patient's request to leave the unit unescorted because hospital policy requires supervision for suicide precautions exercises legitimate clinical authority, provided the rationale is explained, and the patient's concerns are addressed. By contrast, a nurse who tells a patient “You will not be discharged until you agree to take this antipsychotic” exercises informal coercion by tying discharge to treatment acceptance without legal authorization and without ensuring the patient understands alternatives or can meaningfully participate in the decision.
This analysis employs procedural justice theory as its primary conceptual framework. Procedural justice theory, developed in organizational and legal psychology, holds that people evaluate the fairness of processes based on three core elements: voice (opportunity to express views and preferences), transparency (clear explanation of decisions and their basis), and neutrality (freedom from bias and arbitrary decision-making) (Tyler, 2003). Applied to psychiatric care, the framework predicts that patients will experience coercion when treatment processes deny them voice in decisions, when the rationale for decisions is opaque or inconsistent, or when they perceive that staff exercise arbitrary control over valued outcomes.
Procedural justice theory explains why informal coercion occurs even in voluntary admission contexts and why it undermines therapeutic alliance and engagement. When nurses control discharge timing, privilege access, or documentation content without transparent rationale or patient input, they violate procedural justice principles. The theory also guides intervention design: safeguards that enhance voice (e.g., patient input in treatment planning), transparency (e.g., clear privilege policies with documented rationales), and neutrality (e.g., documentation audits to prevent arbitrary characterizations) should reduce perceived coercion and improve outcomes.
The framework is complemented by human rights approaches that situate patient autonomy and dignity as foundational ethical obligations rather than aspirational goals (Pértega & Holmberg, 2023). Together, these frameworks support the argument that informal coercion warrants regulatory attention comparable to formal coercion, and that reducing it requires both structural policy changes and individual competency development among nurses.
Policy and Practice Context: Why Nursing Discretion and Service Architecture Matter
Nurses hold substantial discretionary authority in inpatient psychiatric settings. They assess mental status, administer medications, manage behavioral crises, grant or deny privileges such as phone access and unit leave, participate in multidisciplinary treatment planning, prepare discharge documentation, and serve as the primary point of continuous patient contact (Delaney & Johnson, 2014). This discretion is necessary because psychiatric nursing requires real-time judgment about safety, therapeutic relationships, and individualized care. However, discretion also creates opportunities for informal coercion, particularly when institutional pressures, resource constraints, or risk-averse cultures incentivize compliance-focused practices over shared decision-making (Gilburt et al., 2008).
Service architecture shapes the context in which nursing discretion operates. Inpatient psychiatric units function within broader systems that include emergency departments, community mental health centers, criminal justice agencies, housing authorities, child welfare agencies, and managed care payers. These systems generate external contingencies that can be leveraged informally. For example, a patient may face loss of subsidized housing, termination of disability benefits, or unfavorable custody recommendations if hospital documentation characterizes them as noncompliant. Nurses, who often prepare or contribute to discharge summaries and treatment progress notes, mediate these contingencies through documentation practices. When patients perceive that refusal will result in punitive documentation, the voluntary nature of their consent becomes questionable (Canvin et al., 2002).
Contemporary environmental pressures intensify the structural conditions that facilitate informal coercion. Reduced hospital lengths of stay, driven by managed care reimbursement policies, creates time pressure that may incentivize staff to use leverage rather than sustained engagement to secure treatment decisions before discharge. The shortage of inpatient psychiatric beds nationally—estimated at a 95,000-bed deficit as of 2023—means that patients often wait days in emergency departments before admission and face rapid discharge planning to free beds for waiting patients (Treatment Advocacy Center, 2023). This bed scarcity creates institutional pressure to move patients through the system efficiently, potentially increasing the use of coercive discharge practices when patients resist recommended aftercare.
Nursing staffing challenges compound these pressures. The psychiatric nursing workforce faces critical shortages, with high turnover, burnout, and vacancy rates exceeding those in other nursing specialties (American Psychiatric Nurses Association, 2024).
Understaffed units may rely more heavily on behavioral control strategies, including privilege systems and medication leverage, when nurses lack time for therapeutic engagement and de-escalation. Inexperienced or temporary nursing staff may be less equipped to navigate the ethical complexities of persuasion versus coercion, particularly in high-acuity environments.
These system-level factors interact with the discretionary nature of nursing practice to create conditions where informal coercion becomes an expedient response to institutional demands. Policy interventions must acknowledge these realities. Reducing informal coercion requires not only nursing education and policy limits but also adequate staffing, manageable unit census, and organizational cultures that prioritize therapeutic relationships over throughput efficiency. Without attention to these structural determinants, attempts to minimize coercion through measurement and training alone may fail or create moral distress among nurses caught between professional values and institutional imperatives.
Hospital Policies Also Structure Coercion Opportunities
Many inpatient units use privilege systems that grant access to valued activities—phone calls, visitors, outdoor time, off-unit leave—based on treatment participation or behavioral compliance. While intended to promote therapeutic goals and manage safety, these systems can function as informal coercion mechanisms when nurses use them strategically to secure adherence.
Similarly, discharge practices that delay or threaten to delay discharge unless patients accept specific aftercare plans create leverage over patients who are eager to leave (Bindman et al., 2005).
State and Federal Regulatory Frameworks
Accreditation standards from The Joint Commission and the Centers for Medicare & Medicaid Services focus primarily on formal coercion—seclusion, restraint, and involuntary medication—and do not systematically address informal mechanisms. State mental health codes define involuntary commitment criteria but remain silent on informal coercion in voluntary admissions. Professional nursing standards emphasize respect for autonomy and informed consent but offer limited operational guidance on avoiding coercive leverage in complex clinical situations (American Nurses Association, 2021). This regulatory vacuum leaves informal coercion largely unmonitored and unaccountable (Table 1).
Policy Package Implementation Matrix: Informal Coercion Safeguards in Voluntary Inpatient Mental Health Nursing.
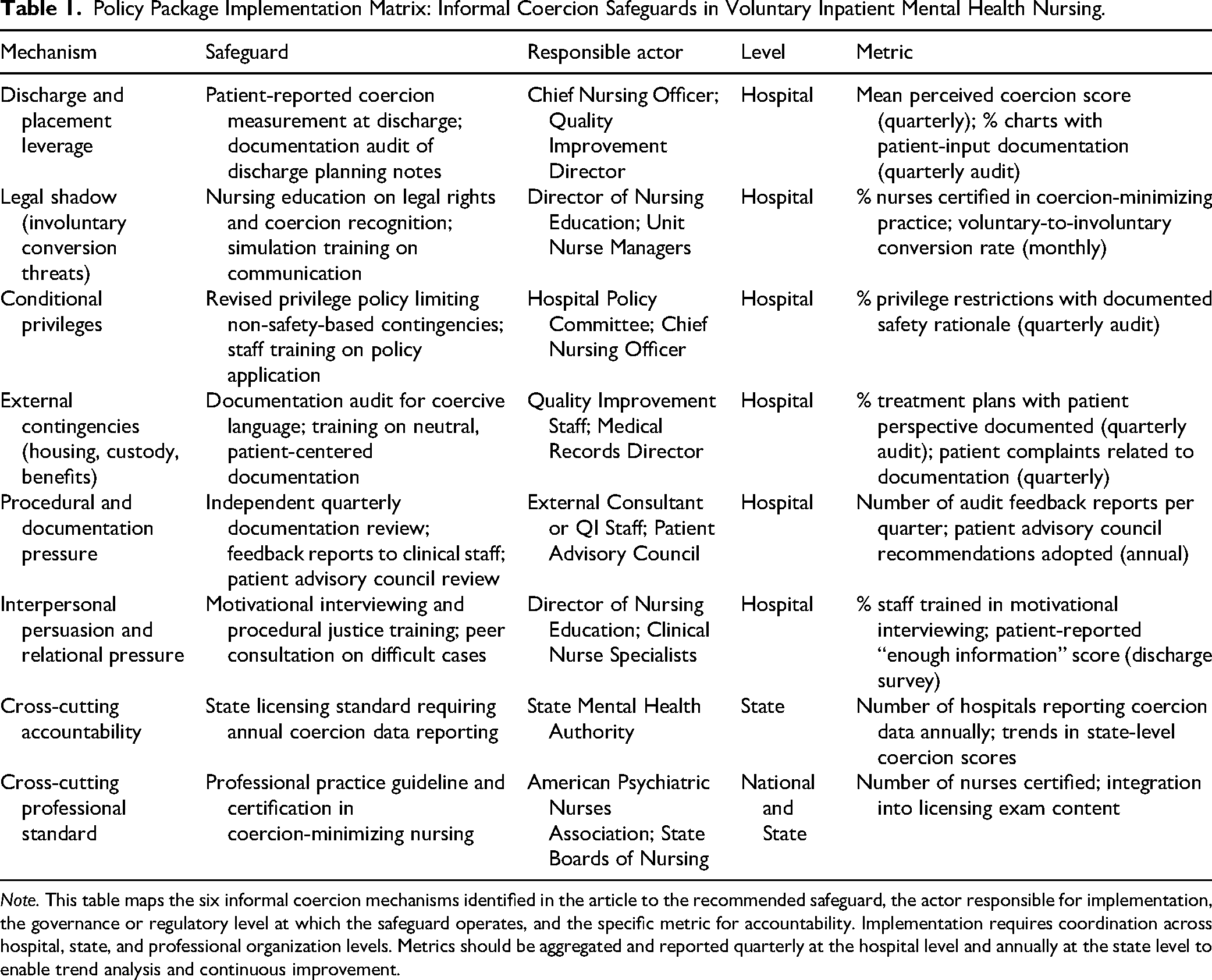
Note. This table maps the six informal coercion mechanisms identified in the article to the recommended safeguard, the actor responsible for implementation, the governance or regulatory level at which the safeguard operates, and the specific metric for accountability. Implementation requires coordination across hospital, state, and professional organization levels. Metrics should be aggregated and reported quarterly at the hospital level and annually at the state level to enable trend analysis and continuous improvement.
Mechanism Map: Categories of Informal Coercion in Nursing Practice
Six categories of informal coercion operate in voluntary inpatient mental health nursing, each linked to specific nursing roles and practice decisions. First, discharge and placement leverage involves using control over discharge timing or postdischarge placement to secure treatment compliance. Nurses participate in discharge planning and often communicate discharge readiness to physicians and social workers. When nurses signal that a patient “is not ready for discharge” because they have refused a recommended medication or declined a referral, they exercise informal coercion if that judgment is not clinically necessary for safety. This mechanism also operates when discharge is contingent on acceptance of a specific housing placement, outpatient provider, or medication regimen that the patient prefers to decline (Katsakou et al., 2011).
Second, legal shadow mechanisms involve invoking the possibility of involuntary commitment to pressure voluntary patients into compliance. Nurses may state or imply that refusal will lead to involuntary conversion, civil commitment proceedings, or emergency certification. For example, a nurse might say, “If you don’t take your medication voluntarily, we will have to commit you,” even when the patient does not meet statutory criteria for involuntary status. The threat leverages the patient's fear of losing liberty and the procedural burden of a commitment hearing (Szmukler & Appelbaum, 2008). This mechanism is particularly potent because many patients lack knowledge of their legal rights and overestimate the ease with which clinicians can initiate commitment.
Third, conditional privileges tie access to valued activities or resources to treatment adherence or compliance with unit rules. Nurses control many of these privileges through shift-to-shift decisions. Examples include requiring attendance at group therapy before allowing phone calls, restricting visitors unless the patient has “been cooperative,” or denying off-unit passes unless medication is accepted. While some privilege restrictions serve legitimate safety functions, coercion occurs when privileges unrelated to safety are used instrumentally to secure compliance with treatment that the patient has the legal right to refuse (Gilburt et al., 2008).
Fourth, external contingencies link hospital recommendations to outcomes controlled by third parties such as housing authorities, courts, child welfare agencies, or disability determination offices. Nurses contribute to the documentation that these agencies rely upon. When a patient believes that refusal will result in documentation labeling them noncompliant, uncooperative, or treatment-resistant—and that such documentation will jeopardize housing, custody, or benefits—the patient experiences informal coercion even if the nurse does not explicitly threaten to write damaging notes. The mechanism operates through the patient's reasonable perception of risk (Canvin et al., 2002).
Fifth, procedural and documentation pressure involves coercive language in treatment planning, goal setting, and progress notes. Nurses document patient behavior, participation, and treatment response. When documentation frames refusal as pathological (e.g., “Patient lacks insight and refuses recommended treatment due to paranoia”) rather than as an exercise of autonomy (e.g., “Patient declines medication, citing concerns about side effects, and requests alternative approaches”), it creates a record that can be used coercively by future providers or agencies. Similarly, when treatment plan goals are written without patient input and presented as nonnegotiable, the planning process becomes coercive (Rise et al., 2013).
Sixth, interpersonal persuasion and relational pressure operate through the nurse–patient relationship. Nurses build therapeutic alliances, offer reassurance, and use relational influence to encourage treatment engagement. This becomes coercive when persuasion is repetitive, dismissive of patient concerns, or framed in ways that imply the patient is irrational, ungrateful, or self-destructive for refusing. Relational coercion is subtle and difficult to monitor because it depends on tone, frequency, and the power differential inherent in the inpatient setting (Hem et al., 2018). However, qualitative studies consistently identify relational pressure—feeling that refusal will damage the relationship with trusted staff—as a significant source of perceived coercion (Katsakou & Priebe, 2006).
Evidence Base: Measurement, Prevalence, and Outcomes
Research on informal coercion in voluntary psychiatric hospitalization has employed three methodological approaches: standardized measurement of perceived coercion, qualitative exploration of patient and staff experiences, and quantitative examination of associations between coercion and clinical outcomes.
The most widely used measure of perceived coercion is the MacArthur Perceived Coercion Scale, a five-item instrument assessing the patient's sense of control, choice, and influence over the admission decision (Gardner et al., 1993). Studies using this scale demonstrate that a substantial minority of voluntary patients report high perceived coercion. A meta-analysis by Katsakou and Priebe (2006) found that across studies in the United States, United Kingdom, and Europe, between 12% and 39% of voluntary inpatients reported perceived coercion levels comparable to those of involuntary patients. Perceived coercion was associated with (a) experience of pressure from family or clinicians prior to admission, (b) perceived lack of alternatives to hospitalization, (c) insufficient explanation of admission procedures, and (d) experience of threats or negative leverage during hospitalization. Notably, perceived coercion did not correspond perfectly to legal status; some involuntary patients reported low coercion, while some voluntary patients reported high coercion.
Qualitative Research Provides Insight into Mechanisms
Interviews with voluntary inpatients in the United Kingdom conducted by Gilburt et al. (2008) identified privilege-based leverage, threatened involuntary conversion, and discharge delays as common sources of coercion. Patients described being told they would not receive leave privileges unless they accepted medication, that refusal would result in being “sectioned” (involuntary commitment under the Mental Health Act), and that discharge would be delayed indefinitely unless they agreed to aftercare plans they opposed. Similarly, a study by Canvin et al. (2002) found that patients on voluntary status feared that documentation of noncompliance would jeopardize housing placements and benefit determinations, leading them to consent to treatments they would otherwise refuse.
Outcome Studies Linkage
A longitudinal study by Katsakou et al. (2010) followed patients admitted to psychiatric wards in Europe and found that higher perceived coercion at admission predicted lower therapeutic alliance scores, reduced treatment satisfaction, and increased likelihood of disengagement from follow-up care at 3 months postdischarge. Newton-Howes and Mullen (2011) reported that patients who experienced coercion during hospitalization were more likely to discontinue outpatient treatment and to be readmitted within 6 months. Qualitative findings indicate that perceived coercion contributes to feelings of betrayal, mistrust of mental health services, and retraumatization, particularly among patients with histories of interpersonal trauma.
A study by Sheehan and Burns (2011) examined discharge against medical advice among voluntary patients and found that perceived coercion was a strong predictor of premature discharge. Patients who felt pressured or threatened were more likely to leave the hospital early, often without stabilization or follow-up arrangements. This finding suggests that informal coercion may paradoxically increase risk by undermining the voluntary patient's willingness to remain in treatment.
There is limited evidence that addresses nursing-specific practices. A qualitative study by Hem et al. (2018) explored Norwegian psychiatric nurses’ use of coercion and found that nurses not only experienced moral distress when they felt compelled to use pressure tactics to secure compliance but also believed such tactics were necessary for patient safety. Nurses reported limited training on distinguishing coercion from persuasion and expressed uncertainty about where to draw ethical boundaries. Rise et al. (2013) examined care planning practices in inpatient psychiatry and found that many treatment plans were written without meaningful patient input, reflecting procedural coercion.
Recent scholarship reinforces the urgency of addressing informal coercion while highlighting persistent gaps in intervention research. Systematic reviews demonstrate that coercive practices—both formal and informal—predict worse long-term outcomes including reduced service engagement, lower quality of life, and increased symptoms of posttraumatic stress, with effects persisting years after discharge (Luciano et al., 2014). Qualitative evidence continues to document patients’ experiences of leverage, conditional privileges, and subtle pressures that shape consent in ways not captured by legal status (Bennetts et al., 2024). Implementation science examining coercion-reduction interventions shows promise: Gooding et al. (2020) found that human rights-informed training combined with procedural changes reduced perceived coercion and improved alliance, while Steinert et al. (2021) demonstrated that systematic monitoring with feedback loops decreased use of formal coercion without compromising safety. However, these interventions focus primarily on seclusion and restraint rather than the informal mechanisms documented here. Strand et al. (2020) found that despite recognition of coercion's harms, few hospitals have implemented systematic measurement or reduction protocols, and Cusack et al. (2023) identified organizational culture and resource constraints as primary implementation barriers. This evidence-to-practice gap underscores the need for feasible, nurse-focused interventions that address informal coercion specifically within voluntary admission contexts.
The evidence base has limitations. Most studies are observational and cross-sectional, limiting causal inference. Measurement relies heavily on patient self-report, which may be influenced by recall bias or mental state. Few studies disaggregate informal coercion mechanisms, making it difficult to isolate the impact of specific practices. No randomized trials have tested interventions to reduce informal coercion in inpatient settings. Despite these limitations, the consistency of findings across settings and methods supports the conclusion that informal coercion is prevalent, detectable, and associated with outcomes that matter to patients, nurses, and policymakers.
Policy Options: Evaluating Feasible Interventions
Five policy options merit evaluation as responses to informal coercion in voluntary inpatient mental health nursing.
Option 1 involves implementing standardized coercion audits using validated patient-reported measures. Hospitals would administer the MacArthur Perceived Coercion Scale or a comparable tool to all voluntary patients at discharge, aggregate results by unit and quarter, and use the data to identify high-coercion units or practices. This approach leverages existing measurement technology, aligns with patient-centered care priorities, and creates accountability through transparency. However, it requires resources for survey administration and data analysis, may face resistance from staff who perceive audits as punitive, and provides only retrospective data that cannot prevent coercion in real time. Implementation would occur at the hospital governance level, with potential mandates from state mental health authorities or accrediting bodies.
Option 2 establishes patient advisory councils with authority to review and recommend changes to privilege policies, discharge practices, and documentation standards. Councils would include current or former patients, peer support specialists, and family members, and would meet quarterly to review policies and anonymized case examples. This approach incorporates patient voice into governance, surfaces coercion mechanisms that staff may not recognize, and builds public accountability. Challenges include ensuring representative participation, protecting council members from retaliation or tokenization, and translating recommendations into enforceable policy changes. Implementation occurs at the hospital level but can be incentivized through state licensing requirements or accreditation standards.
Option 3 limits conditional privilege systems by prohibiting the use of privileges unrelated to safety as leverage for treatment compliance. Hospitals would revise policies to ensure that access to phone calls, visitors, outdoor time, and similar privileges is not contingent on medication acceptance, therapy attendance, or other treatment decisions. Privileges could still be restricted for direct safety reasons (e.g., denying off-unit leave for a patient at acute suicide risk), but not as behavior modification tools. This approach directly targets a well-documented coercion mechanism and clarifies the boundary between safety interventions and coercion. It may face resistance from staff who view privilege systems as essential to managing unit behavior and require robust alternative strategies for promoting engagement. Implementation would involve hospital policy revision, potentially guided by state regulations or professional nursing standards.
Option 4 mandates independent documentation review to identify coercive language in treatment plans, progress notes, and discharge summaries. Hospitals would establish review teams—potentially including quality improvement staff, patient advocates, or external consultants—to audit a sample of records each month and provide feedback to nursing and medical staff. Reviews would flag language that frames refusal as pathological, omits patient perspectives, or constructs narratives that disadvantage patients in external systems. This approach addresses the documentation mechanism and creates a feedback loop for professional development. It requires expertise in both clinical documentation and coercion dynamics, may be perceived as intrusive by clinicians, and does not directly prevent coercion at the point of care. Implementation occurs at the hospital level with potential oversight from state mental health authorities.
Option 5 requires direct training interventions focused on recognizing and minimizing informal coercion. Hospitals would mandate training for all psychiatric nurses covering (a) conceptual distinctions between coercion and persuasion, (b) procedural justice principles including voice, transparency, and fairness, (c) de-escalation and motivational interviewing techniques that support autonomy, and (d) simulation exercises practicing high-risk scenarios such as discharge planning and privilege decisions. Training would include competency assessment and would be integrated into annual continuing education requirements. This approach targets the knowledge and skill gaps identified in qualitative research and aligns with nursing professional development frameworks. However, training alone may be insufficient without policy changes that reduce structural incentives for coercion, and effectiveness depends on training quality and institutional culture. Implementation would involve collaboration between hospital nursing education departments, state boards of nursing, and professional nursing organizations.
Recommended Package and Justification
The most effective and feasible response to informal coercion combines four elements: (a) patient-reported coercion measurement implemented at discharge and aggregated quarterly by unit, (b) nursing education with simulation-based competency assessment integrated into annual continuing education, (c) explicit limits on conditional privilege use with revised hospital policies prohibiting nonsafety-based leverage, and (d) independent documentation audits with quarterly feedback to clinical staff.
This package addresses both structural and individual sources of informal coercion. Patient-reported measurement creates accountability and identifies problem areas. Nursing education builds competency in recognizing and avoiding coercive practices. Privilege policy limits remove a major mechanism of leverage. Documentation audits address both the procedural coercion embedded in treatment planning and the external contingencies created by hospital records.
The package is superior to single-intervention approaches because informal coercion is multidetermined. Measurement without education may identify problems without building capacity to solve them. Education without policy change may equip nurses with skills they cannot apply because institutional structures incentivize coercion. Privilege limits without measurement may reduce one mechanism while leaving others unaddressed. Documentation audits without training may correct language without changing underlying practices.
This package also balances feasibility and impact. Each element can be implemented at the hospital level without requiring statutory changes, though state-level mandates or incentives would accelerate adoption. The required resources are modest relative to hospital operating budgets: survey administration software, training curriculum development, and part-time review staff. The package aligns with existing priorities, including patient-centered care, trauma-informed practice, and quality improvement, facilitating buy-in from nursing leadership and hospital administration.
Two meaningful tradeoffs require attention. First, privilege policy limits may increase staff concerns about managing unit safety and behavioral challenges without leverage tools. Mitigation involves simultaneously investing in alternative engagement strategies such as motivational interviewing, peer support, and individualized safety planning and providing staff with consultation support during the transition. Second, documentation audits may create tension or defensiveness among clinicians who perceive review as punitive. Mitigation involves framing audits as quality improvement rather than compliance enforcement, ensuring feedback is constructive and educational, and involving frontline nurses in developing audit criteria and improvement plans.
While formal cost-effectiveness analysis was beyond the scope of this policy review, preliminary evidence suggests that reducing informal coercion may generate cost savings through reduced readmissions, decreased length of stay associated with improved alliance, and reduced litigation and complaint resolution costs. Future research should conduct an economic evaluation comparing implementation costs to downstream savings.
Implementation Plan: Actors, Levels, and Timeline
Implementation of the recommended package requires coordinated action across three levels: hospital governance, state regulatory agencies, and professional nursing organizations.
At the hospital governance level, the chief nursing officer and quality improvement director lead implementation. In the first quarter, the hospital establishes a task force including nursing leadership, patient advocates, and quality staff to develop implementation protocols. The task force (a) selects a patient-reported coercion measure and integrates it into discharge workflows, (b) contracts with nursing education specialists to develop a training curriculum with simulation modules, (c) convenes a policy review committee to draft revised privilege policies, and (d) assigns documentation review responsibilities to quality improvement staff or external consultants. In the second and third quarters, the hospital pilots the revised privilege policies on one unit, trains nursing staff in cohorts, and conducts initial documentation audits. In the fourth quarter, the hospital expands the privilege policy and training hospital-wide, begins quarterly reporting of coercion measurement data to the board and staff, and establishes a regular audit feedback cycle.
At the state regulatory level, the state mental health authority incorporates informal coercion monitoring into hospital licensing and oversight. Within the first year, the authority issues guidance to licensed psychiatric hospitals recommending adoption of the four-element package and offering technical assistance for implementation. The authority revises hospital licensing standards to require (a) annual reporting of patient-reported coercion data, (b) documentation of nursing education on coercion minimization, and (c) written policies governing privilege use.
The authority conducts site visits that include interviews with patients and review of privilege and documentation policies. This level of action provides statewide consistency, creates regulatory accountability, and supports underresourced hospitals with implementation tools.
At the professional organization level, the American Psychiatric Nurses Association and state boards of nursing integrate informal coercion content into continuing education requirements and practice standards. Within 2 years, the association publishes a position statement and practice guideline on minimizing informal coercion in inpatient care, develops a certification program for competency in coercion-minimizing practice, and incorporates coercion content into the psychiatric-mental health nursing certification examination. State boards of nursing adopt the guideline as a reference for practice standards and include coercion-related scenarios in disciplinary case reviews. This level of action ensures that informal coercion is recognized as a professional competency issue and integrated into nursing education and credentialing.
Minimal resources required include (a) survey software and data management capacity, (b) training curriculum development and trainer fees, (c) part-time documentation review staff or consultant contracts, and (d) policy development time for nursing and quality leadership. For a 50-bed inpatient psychiatric unit, estimated annual costs are approximately $75,000 for the first year (including curriculum development and initial training) and $40,000 per year for ongoing implementation (surveys, audits, and annual training). These costs are small relative to typical inpatient psychiatric unit budgets, which range from $5 million to $15 million annually, depending on region and payer mix.
Barriers include staff resistance, particularly if nurses perceive the package as increasing workload or scrutinizing their clinical judgment. Mitigation involves engaging frontline nurses in design and pilot testing, framing the package as a professional development opportunity rather than a compliance burden, and ensuring that implementation timelines allow adequate preparation. Resource constraints in public and safety-net hospitals may limit adoption.
Mitigation involves state technical assistance, phased implementation that prioritizes high-impact elements, and potential funding support through Medicaid quality incentive programs or mental health block grants. Variation in state legal frameworks governing voluntary admission and patient rights may require adaptation of privilege policies and documentation standards. Mitigation involves state-level guidance that interprets the package in light of local statutes and case law.
Accountability Metrics: Measuring Progress and Impact
Ten metrics provide accountability for the implementation and impact of the recommended package.
Metrics are organized into patient-reported, process, and outcome categories.
Patient-reported metrics include (a) mean perceived coercion score on the MacArthur Perceived Coercion Scale or equivalent, aggregated quarterly by unit and reported as a trend line with a target of year-over-year reduction, and (b) percentage of voluntary patients reporting they had enough information to make decisions about treatment, measured via a two-item survey question at discharge with a target of 85% or higher. These metrics directly capture patient experience and create accountability for coercion reduction.
Process metrics include (a) percentage of eligible nursing staff who have completed coercion minimization training and demonstrated competency via simulation assessment, with a target of 100% within 18 months, (b) percentage of patient charts with privilege restrictions documented with explicit safety rationale, measured via quarterly audit with a target of 95% or higher, (c) percentage of treatment plans that include documented patient input and preferences, measured via quarterly audit with a target of 90% or higher, and (d) number of documentation audit feedback reports provided to nursing and medical staff per quarter, with a target of at least one report per quarter per unit. These metrics ensure that the structural and educational components of the package are implemented as intended.
Outcome metrics include (a) rate of voluntary patients requesting discharge against medical advice, reported monthly with a target of year-over-year reduction, (b) rate of voluntary-to involuntary status conversions, reported monthly as a ratio of conversions to voluntary admissions with a target of year-over-year reduction, (c) rate of patient complaints or grievances related to coercion, pressure, or lack of information, reported quarterly with a target of year-over-year reduction, and (d) rate of seclusion or restraint events among voluntary patients, reported monthly with a target of year-over-year reduction. These metrics capture downstream effects of coercion on patient behavior and safety events.
Metrics should be reported to hospital leadership, nursing staff, patient advisory councils, and state mental health authorities. Public reporting at the facility level, with appropriate privacy protections, enhances accountability and allows patients and families to make informed decisions about treatment settings. Risk adjustment for patient acuity and unit characteristics may be necessary to ensure fair comparison across units and over time.
Limitations
This policy analysis has four primary limitations. First, it relies on observational evidence linking informal coercion mechanisms to patient outcomes. Causal inference is limited by confounding, selection bias, and measurement error. The recommended package represents a theoretically grounded and evidence-informed synthesis, but its effectiveness requires empirical testing. Randomized trials comparing hospitals implementing the package to control sites would provide stronger evidence, though such trials face logistical and ethical challenges.
Second, the analysis focuses on the U.S. legal and regulatory context, particularly state-level mental health codes and federal accreditation frameworks. While the conceptual framework and many recommendations generalize to other jurisdictions with voluntary admission systems, implementation details will vary. Countries with different mental health acts, nursing scope-of-practice regulations, or patient rights frameworks will require adapted approaches.
Third, the recommended package does not address root causes of coercion that lie outside hospital control, including housing shortages, gaps in community mental health services, and criminal justice involvement that create external contingencies. Informal coercion in inpatient settings reflects broader system failures. The package can reduce nursing-mediated coercion, but comprehensive solutions require investments in housing, outpatient services, and alternatives to hospitalization.
Fourth, implementation feasibility varies substantially across hospital types. Well-resourced academic medical centers have greater capacity for training, audit systems, and policy development than underresourced public hospitals or rural facilities. The implementation plan acknowledges this variation and recommends state-level support, but resource disparities may limit equitable adoption. Targeted funding and technical assistance are necessary to avoid widening quality gaps.
Implications for Nursing Practice, Research, and Policy
For nursing practice, this analysis identifies informal coercion as a core professional competency issue. Psychiatric-mental health nurses require explicit education on recognizing coercion, applying procedural justice principles, and using therapeutic communication techniques that respect autonomy under pressure. Nursing leaders should integrate coercion minimization into orientation programs, annual competency assessments, and peer consultation processes. Documentation practices, privilege decisions, and discharge planning should be approached with awareness of coercion risk and commitment to transparency and voice.
For nursing research, priorities include (a) intervention studies testing the effectiveness of training, policy changes, and audit systems in reducing perceived coercion, (b) measurement development to create brief, valid tools suitable for routine clinical use, (c) qualitative research exploring nursing decision-making in high-coercion scenarios to inform simulation training, and (d) longitudinal studies examining the relationship between informal coercion and long-term recovery, trauma symptoms, and service engagement. Research should attend to variation by patient characteristics, including race, gender, trauma history, and prior involvement with coercive systems, to identify equity concerns.
For policy, this analysis supports three actions. First, state mental health authorities should revise hospital licensing standards to require monitoring and reduction of informal coercion in voluntary admissions, using the metrics and package outlined here as a model. Second, accrediting bodies such as The Joint Commission should incorporate informal coercion into patient rights and quality-of-care standards, moving beyond exclusive focus on formal coercion. Third, federal agencies, including the Substance Abuse and Mental Health Services Administration and the Centers for Medicare & Medicaid Services, should provide guidance, technical assistance, and potentially financial incentives for hospitals implementing coercion reduction programs, leveraging quality incentive payment structures in Medicaid and Medicare.
State boards of nursing and professional organizations should recognize coercion minimization as a professional standard, integrate it into practice guidelines, and ensure that disciplinary processes address coercive practices when they rise to the level of ethical or professional violations. Nursing education programs should incorporate content on informal coercion, procedural justice, and shared decision-making in mental health into both undergraduate and graduate curricula.
Finally, patient advocacy organizations and peer-run programs have a critical role in monitoring implementation, ensuring patient voice in policy development, and holding hospitals accountable through public reporting and advocacy. The recommended package includes patient advisory councils as a governance mechanism; these councils should have access to coercion measurement data and the authority to review and influence hospital policies.
Conclusion
Informal coercion in voluntary inpatient mental health nursing is prevalent, measurable, and amenable to policy intervention. Six mechanisms—discharge leverage, legal shadow threats, conditional privileges, external contingencies, procedural pressure, and relational coercion—operate through nursing discretion and service architecture. Evidence links these mechanisms to reduced therapeutic alliance, treatment disengagement, and adverse outcomes. A policy package combining patient-reported measurement, nursing education, privilege policy limits, and documentation audits offers a feasible and effective response. Implementation requires coordinated action by hospital governance, state regulators, and professional nursing organizations. Accountability metrics spanning patient experience, process adherence, and clinical outcomes enable monitoring and continuous improvement. Addressing informal coercion strengthens the ethical foundation of voluntary psychiatric care, supports recovery-oriented practice, and advances nursing's commitment to patient autonomy and dignity.
Footnotes
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.