
Abstract
Fuel2Flourish is a nurse-led initiative designed to center the voices of nurses, who are active leaders within the National Association of Hispanic Nurses (NAHN), as trusted messengers and role models in advancing the nutritional and emotional well-being of school-age children. Operating across nine local chapters in different states, this community-rooted program was built in partnership with national policy stakeholders and community leaders to respond to what children and families need most: support they can trust from people who understand their lived experiences. This study employed qualitative methods to gain feedback from chapter program leads to examine implementation processes and early perceived impacts. Through bilingual education toolkits, culturally relevant storytelling, and nurse-led workshops, nurses engaged directly with students, parents, and educators to create safe, inclusive spaces for learning and connection. Despite limited budgets and varied local conditions, Fuel2Flourish thrived by aligning clinical nursing expertise with community insight and action. This article describes the partnerships formed, and the early signs of impact seen on the ground. Fuel2Flourish shows what's possible when nurses are equipped and empowered to lead, bringing creative, locally tailored solutions to the forefront of child health promotion.
Introduction
Nursing Activism in the United States
Nursing is the largest healthcare profession in the United States, with more than 3.8 million registered nurses nationwide (American Association of Colleges of Nursing [AACN], 2023). Historically, nurses have played a central role in activism and social movements with nursing leaders such as Lavinia Dock, Lillian Wald, and Margaret Sanger using their positions to champion public health, women's rights, and health equity, as described in a recent scoping review of U.S. nursing and midwifery activism. As time passed, nurses became less directly engaged in community activism and transitioned toward advocacy through professional nursing organizations, of which approximately 10%–20% of nurses are members of more than 300 professional nursing organizations in the United States (Cline et al., 2019; Ojemeni et al., 2023). As nurses are at the forefront of care delivery, they are often seen as trusted role models within the communities they serve and have consistently been rated as the most trusted profession in the United States according to Gallup's annual Honesty and Ethics in Professions poll (Gallup, 2023).
However, Ojemeni et al. (2023) found that leadership development was almost entirely missing from the literature on U.S. nursing and midwifery activism, pointing to an important gap in how the profession prepares nurses for community involvement. At the National Association of Hispanic Nurses (NAHN), an organization that was established in 1975, members across 24 states and in over 45 chapters, strengthen their community leadership skills by engaging in nurse-led initiatives that promote the health and wellness of Latino communities and beyond (National Association of Hispanic Nurses, n.d.a, n.d.b). This article highlights the Fuel2Flourish program that was developed by NAHN in 2024. The program was designed to address the leadership development gap identified in the recent literature, where the program builds nurse leadership by integrating structured mentorship with hands-on community education for children and families.
Nursing Alignment With Federal Initiatives
In 2024, aligning with the Biden Administration's White House Challenge to End Hunger and Build Healthy Communities, NAHN announced a national commitment to providing youth education on nutrition and well-being through the Fuel2Fourish program (NAHN, n.d.a, n.d.b; The White House, 2024). This commitment was submitted in partnership with the Latinos and Hispanics in Dietetics and Nutrition (LAHIDAN), a Member Interest Group of the Academy of Nutrition and Dietetics (The Academy), the premier organization for food and nutrition professionals (Academy of Nutrition and Dietetics, 2025; Latinos and Hispanics in Dietetics and Nutrition, 2025). Nine NAHN chapters piloted the Fuel2Fourish program designed to promote healthy eating, positive mental health and careers in nursing among elementary school-aged children in Latino communities. This initiative was a White House Commitment to address the significant child health disparities in nutrition and mental health among the Latino community and to promote careers in nursing to youth (Centers for Disease Control and Prevention [CDC], 2023a, 2023b).
Inequities in U.S. Latino Child Health
Overall, child health in the United States has been on the decline, with rising rates of obesity, chronic conditions, and functional limitations (which include limitations due to chronic disease as well as developmental, neurological, and physical conditions) contributing to higher mortality rates over the past 17 years (Forrest et al., 2025). These challenges disproportionately affect Latino children, who already face higher obesity prevalence and reduced access to mental health care. The prevalence of obesity among Hispanic children aged 6–11 years is nearly twice that of non-Hispanic children of the same age (CDC, 2023a, 2023b). In addition, Latino youth are less likely than their white peers to have ever received mental health care, despite 22% exhibiting depressive symptoms (Substance Abuse and Mental Health Services Administration [SAMHSA], 2023).
Developing Nurse Leaders for Community Health
Latino nurses continue to be underrepresented in the nursing profession, making up approximately 7% of the workforce, despite a rapidly growing Latino population (18%) (AACN, 2023). Studies have shown that when Latino nurses provide care within Latino communities, enhanced language concordance and cultural alignment result in improved care delivery and increased responsiveness to patient preferences (Hayes-Bautista et al. (2016). About 78% of Latinos in the U.S. speak Spanish, with younger generations and U.S.-born Latinos being more likely to be bilingual or English-dominant (Pew Research Center, 2022). Still, increasing the number of Latino nurses alone is insufficient without intentional leadership development. Latino nurses continue to experience structural and interpersonal forms of discrimination, from overt bias to microaggressions tied to language, accent, and assumptions about social class. These dynamics fuel imposter syndrome, a heightened need to overperform to gain recognition, and limited access to mentorship (Canli & Aquino, 2024; Doede, 2017). Although the literature is limited on the impact of Latino nursing leaders on community health outcomes, leadership development programs are crucial to countering these barriers and supporting advancement (Villarruel, 2017).
Given the increasing need for bicultural tailored wellness education for American youth and families, and the intentional mentorship needed for nurses to become leaders within their communities, the Fuel2Flourish program effectively bridges the gap between community needs and access to clinical nursing leaders and experts. This article aims to highlight the impact of nurse-led national and local community collaborations in advancing federal and community health goals. Additionally, it will share lessons learned from its implementation in working with nursing leaders across nine states, promoting the value of sustained partnerships with trusted voices within diverse communities.
Methods
With funding from Direct Relief and the Coalition for Safe Food and Beverages, a call for chapter participation was released to NAHN chapters to apply for up to $10,000 in funding in August 2024. An email blast was sent to all 44 chapters for recruitment. To apply, interested chapters submitted a proposal for a chapter pilot program with a proposed budget for implementation over a one-year period, to start on October 1, 2024.
Project Participants
Chapters had to identify a target group with whom to pilot the Fuel2Flourish project within their local community. Target participants needed to include elementary school-aged children living in a predominantly Latino Community. Chapters could partner or collaborate with a variety of sites including: a school, a children sports team or league, an after-school program, a community center, a church, etc. The curriculum had to be implemented to a minimum of eight participants (children or families).
Curriculum Components
The senior author led the development of the program's minimum curriculum requirements, ensuring alignment with existing evidenced-based community programs. Chapters were given the flexibility to select the curriculum for nutrition and mental health to be delivered, but had to meet the national criteria below, which included evidenced-based materials.
Nutrition Curriculum:
The nutrition curriculum must be aligned with recommendations by the most current United States Department of Agriculture's (USDA) Dietary Guidelines for Americans (currently the 2020 edition) (U.S. Department of Agriculture, & U.S. Department of Health and Human Services [2020]).
An example of a curriculum that could be utilized was the “
If chapters chose to use a curriculum not aligned with the USDA standards, or if chapters created their own curriculum, it had to be approved by NAHN Registered Dietitians/Nutritionists serving as nutrition consultants.
Mental Health Curriculum:
The mental health curriculum should have been appropriate for the age of the target population, and it could address specific or various mental health, emotional health, and/or wellness topics.
An example of school-age mental health resources that could have been utilized included those found in the Sandy Hook Promise Learning Center Library (Sandy Hook Promise, n.d.) or the Sesame Workshop (Sesame Workshop, n.d). If chapters chose to create their own mental health curriculum or modify an existing local program, it had to be approved by a Pediatric Psychologist serving as a consultant. Nursing Careers Workshop:
Chapters were given the flexibility to create their own workshop to showcase careers in nursing.
An example of an activity could be to introduce students to the nursing profession using PowerPoint slides. NAHN provides chapters with customizable materials that outline the diverse roles of nurses, and the education pathways required to become a registered nurse. Chapters were encouraged to adapt or expand these materials to design a career workshop that reflected their local needs, partnerships, and community context.
Curriculum Length
Chapters were required to provide a minimum of three separate lessons (a nutrition component, a mental health component, and a career in nursing lesson) to the same participants. Chapters could choose the length of the lessons, and the length of time devoted to the nutrition and mental health components in each lesson. At least one lesson included a short description of careers in nursing. Chapters were required to collect baseline data, which included neighborhood characteristics, number of participants reached, age ranges of participants, and number of volunteers needed to implement the program.
Program Lead Development for Community Programs
Each chapter identified a program lead, who received group training from the authors and ongoing mentorship to ensure understanding of program objectives and implementation strategies. During the grant period, three 1-h check-ins were scheduled where program leads discussed managing their grant budget, developing program materials, and engaging potential collaborators to build partnerships or sponsorship opportunities. Less formal one-on-one meetings were also held with chapter leads, per request, who had questions about implementing their curriculum locally or ideas for publications. Within this framework, leadership development trainings were embedded so that nurses could gain both knowledge in nutrition education and practical experience with community-based programming. Since each chapter was encouraged to submit its own manuscript, the study focused on leaders across chapters rather than collecting data from multiple members within each chapter. While additional input from other chapter members could provide complementary viewpoints, this approach emphasizes the perspective of those directly leading and accountable for the program implementation
Postprogram Evaluation Survey
Once the three required sessions were completed, the chapter's program lead filled out an evaluation survey as they were primarily responsible for the local chapter's program outcomes. The survey included questions regarding demographics that were required to submit to the funder, as well as qualitative questions to measure the nurse-led program's impact within Hispanic communities. Examples of questions included capturing the curriculum tools used for each lesson, whether new partnerships were formed, general experiences captured by the nurse lead, and plans for implementing the same or similar program in the future. See the Supplemental Materials for the full survey questionnaire collected via Microsoft Forms.
No personal or sensitive data was collected in the survey, and the data was presented at NAHN's 50th Annual Conference in Dallas, Texas in aggregate across all chapters for anonymity. Local program chapters obtained parental consent for children's participation in the community education program, including consent for photographs, if applicable to the chapter. Photographs were taken to document and demonstrate the impact of their programs in the community. These images helped to illustrate outcomes for stakeholders, support partnership development, and served as a tool for fundraising and advocacy efforts (Foster, 2024). Chapters had flexibility in how they incorporated photography to reflect their local initiatives and achievements.
The authors conducted a reflexive thematic qualitative analysis of the survey results to examine the experiences of Fuel2Flourish program leads, who were registered nurses that volunteered to lead the community program on behalf of their local chapter. Analyses followed Braun and Clarke's (2006) iterative approach, beginning with the primary author reading the participant responses repeatedly to achieve familiarization. Microsoft Copilot (using GPT-5), an AI-based writing companion, was used to generate preliminary groupings of raw text to support data management. These AI-generated groupings were treated as recommendations and not analytic findings. The primary author independently reviewed all participant responses and compared them to the AI-generated groupings to develop interpretive thematic groupings informed by lived experience as a Latina nurse leader developing and implementing prior community programs within NAHN. This positionality served as an analytic resource in contextualizing patterns and synthesizing themes, which is central to reflexive thematic analysis (Braun & Clarke, 2019). Microsoft Excel was used for manual coding and thematic grouping. After the primary author constructed the thematic groupings, the two additional co-authors reviewed the raw data and final themes to ensure coherence, clarity and alignment with participant responses. All thematic decisions remained under the control of the authors.
Results
Demographics
A total of nine chapters from nine different states applied and were accepted to participate in the Fuel2Flourish program (Figure 1). Based on applications, it was anticipated that the nine programs would reach 581 youth across the country. However, the chapters were able to exceed their goal and served 993 unique children between the ages of 1 and 12, of which 67% identified as Hispanic or Latino. Six chapters hosted their program within an elementary school setting, whereas the additional three were facilitated within the community. All programs took place within an urban or suburban setting and all chapters reported that new partnerships were formed while creating this program. To run the nine programs, 116 NAHN and community members participated. Additionally, 533 parents were reached across the nine programs.
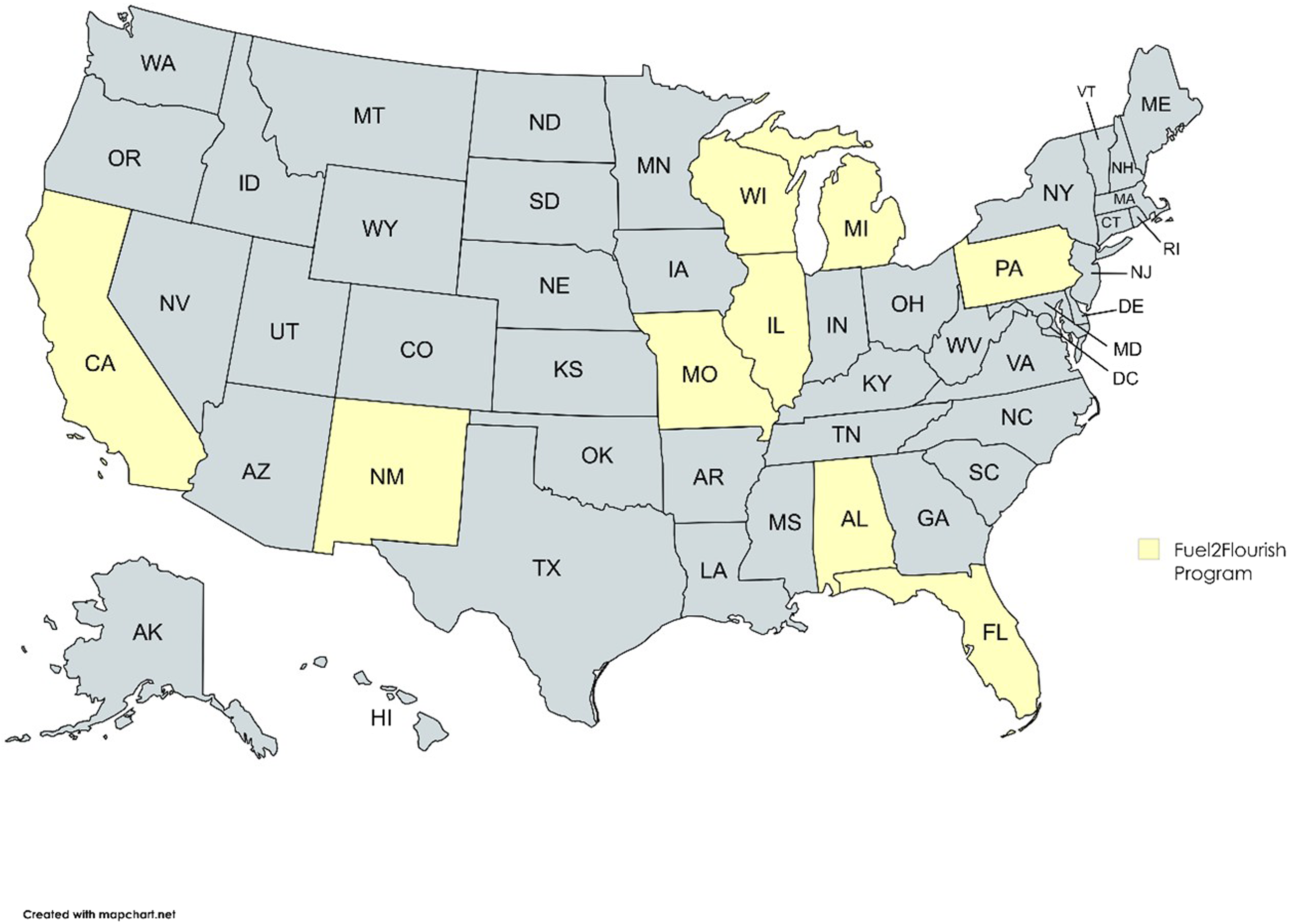
NAHN chapters located within nine states participating in the Fuel2Flourish program.
Curriculum Design
The nine chapters had the flexibility to design their programs using subject matter experts, creativity, established and new national and local partners, and using evidenced-based bilingual tools. For example, materials from the National Dairy Council (NDC) were available in English and Spanish. Figure 2 shows the type of educational tools that were used to create the nutrition and mental health workshops. The most common resource used across chapters was the NDC (n = 5 chapters) and United States Department of Agriculture (USDA) materials (n = 4 chapters), which included My Plate or Mi Plato. For the mental health lesson, the Sandy Hook Promise Learning Center was widely used. Two chapters included a Registered Dietitian to enhance the nutrition lesson curriculum, and three chapters included a licensed mental health professional to enhance the mental health curriculum. The lesson focused on careers in nursing was more fluid, and chapters reported using storytelling, role play, simulation, clinical props and a photo booth (where children dressed in nursing attire and took home a picture of themselves as nurses for the day) to interact with the youth and explore nursing as a profession.
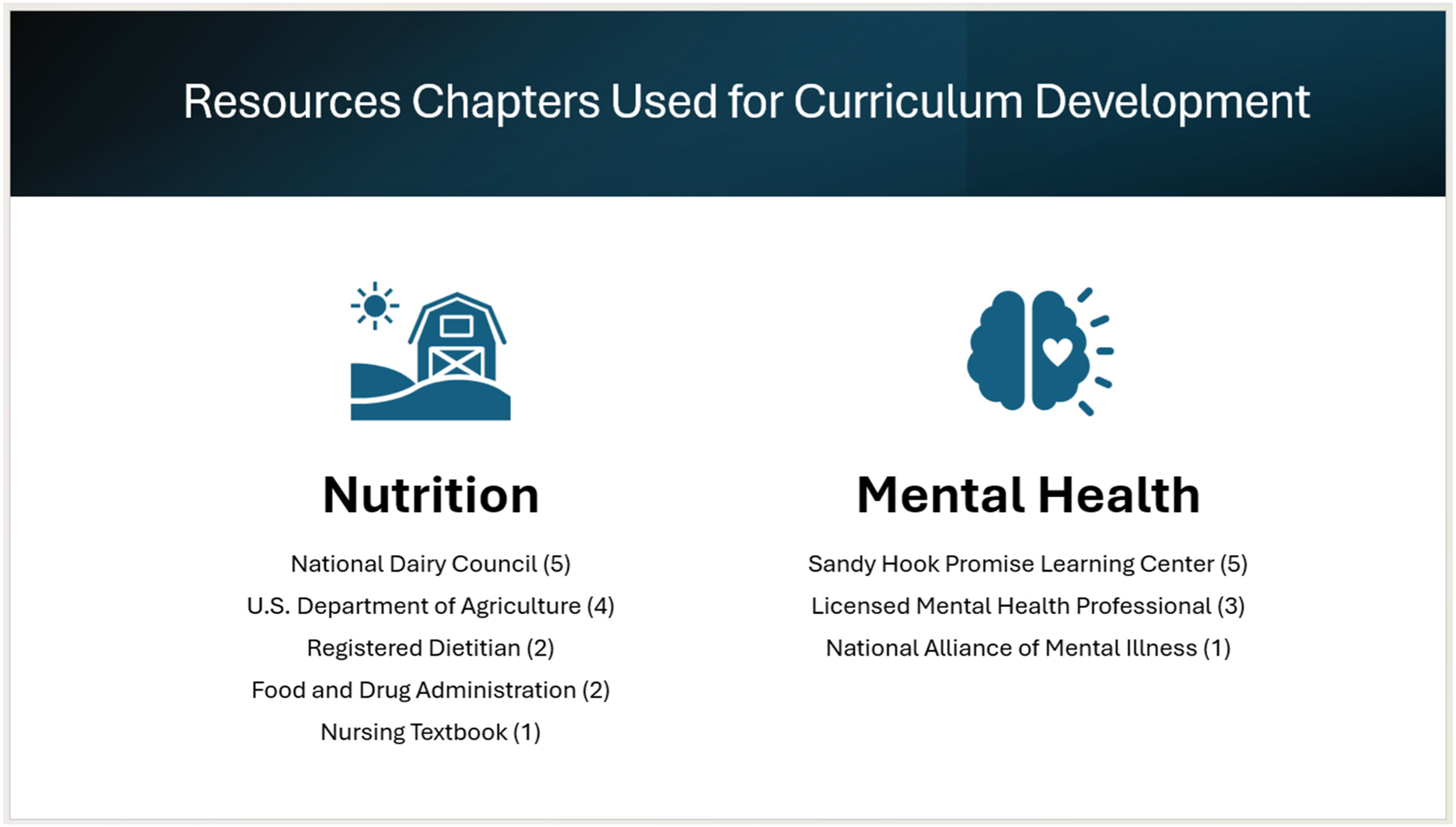
Resources chapters used for curriculum development.
All chapters responded that they felt they achieved the desired learning outcome, which was to provide education to youth about nutrition, emotional well-being and careers in nursing. While the quantitative results demonstrate the overall reach and measurable outcomes of the Fuel2Flourish program, they do not fully capture the depth of participant experiences or the nuanced ways in which the initiative shaped relationships, learning, and community engagement. To complement those metrics, qualitative data from chapter program leads were thematically analyzed to illuminate the lived realities.
Qualitative Feedback
The thematic analysis of nine-chapter reports from the Fuel2Flourish initiative surfaced three key interrelated themes: community trust and relationship building, hands-on learning and responsive adaptation, and opportunities for program improvement. The narratives were rich with moments of joy, trust-building, and tangible behavior change.
Community Trust and Relationship Building
Culturally grounded trust-building emerged as a defining feature given the visibility of Latino nurses as educators and team leads, with some sessions conducted in Spanish, fostering belonging and aspirational identity. One respondent noted, “It was powerful for our Hispanic youth to see professionals who look like them and speak their language.” Trust often surfaced in small yet profound gestures. One chapter reported that students spontaneously identified NAHN members as their “trusted adults” during a Healthy Minds activity. In another chapter, a first grader exclaimed, “¡No sabía que tú también hablabas español!”—a moment that deepened cross-cultural rapport.
Teachers, parents, and partner organizations widely affirmed the value of these programs, often requesting additional sessions or replication in other settings. One partner said the sessions were a “big success … the kids loved it.” Chapters reported new affiliations with schools, universities, clinics, and nonprofits which enhanced their credibility and impact. Extending impact into the home was a recurrent outcome. Tangible take-home items and simple recipes translated into new family habits: “I now make overnight oats for my child almost every day and I started making them for myself too,” reflected one parent.
Hands on Learning and Responsive Adaptation
Interactive, hands-on engagement drove sustained interest and knowledge retention, even across multiweek gaps. In addition to the three required lessons, chapters had the flexibility to add additional lessons. Chapters reported also providing education on handwashing, physical activity, and personal safety. Multistation nursing and health focused activities, from CPR practice to the USDA Veggie Meter®, kept students invested: “Please pick me next time, I really want to participate!” One chapter reported un-expected storm-related power outages while implementing their program. They integrated grocery vouchers alongside the planned education, which further deepened community bonds.
Responsive inclusion also reflected the capacity of chapters to adapt quickly to participants’ needs, such as restructuring sessions for a hearing-impaired student so the student could fully participate. “This made a huge difference in the [child's] ability to participate,” noted a chapter leader.
Opportunities for Program Improvement
Each chapter shared challenges and sustainability concerns around volunteer scheduling, recruitment barriers, coordination with stakeholders, and ensuring accessibility for children with physical disabilities. Chapters also highlighted the need for longer sessions, broader outreach, and consistent spaces for families to gather and learn. One chapter summarized this gap succinctly, “Our community wants opportunities … however, there are limited opportunities for these types of workshops.”
Participants recommended that NAHN continue providing funding opportunities and share findings broadly to demonstrate impact. They emphasized the importance of NAHN facilitating networking and training to build nursing leadership capacity. Continued support for culturally tailored programs and advocacy for nurse-led community initiatives was also highlighted as key to sustaining momentum. All respondents expressed strong interest in continuing the Fuel2Flourish program with additional funding, highlighting the program's positive impact and community demand for sustained culturally tailored wellness education.
Despite the challenges, together, these themes illustrate how the program functioned not just as a health education intervention, but as a culturally responsive, relationship-driven model for nursing community health leadership.
Discussion
Nurses, as clinical experts, who recognize the ethical imperative to address the social causes of poor health, have a responsibility to serve as agents of change and collaborative leaders not only within health care organizations, but also within the communities they serve (Marmot et al., 2008; Williams et al., 2016). Central to this role is the development and use of power. Power within a community builds the influence necessary to address the social determinants of health through policy engagement, collective action, and the amplification of community voice (National Academies of Science, Engineering and Medicine, 2021). This pilot demonstrated the power of nurses as change agents, whose leadership capacity developed most effectively while in action. Nurses were entrusted with the responsibility to design, implement, and adapt local community health programs in real time, working in partnership with community organizations and clinical specialists. By collaborating with educators, administrators, and community stakeholders, NAHN nurses advanced the nutritional and emotional well-being of Latino children while building community relationships and refining in real-time leadership, advocacy, and program design skills. Nursing education programs and community organizations have a clear opportunity to collaborate with professional organizations such as NAHN to create experiential pathways where these community leadership skills can flourish alongside nursing clinical expertise.
While nutrition and mental health education were a critical foundation for child health promotion in the Fuel2Flourish program, they alone cannot drive the systemic change needed for lasting improvements in community well-being. Knowledge must be reinforced by supportive environments, innovative policies, and coordinated partnerships that make healthy behaviors culturally relevant, accessible, and sustainable. Achieving this requires interdisciplinary, cross-sector collaboration among health care professionals, schools, and policymakers to address the broader determinants of health.
More recently, U.S. Secretary of Health and Human Services (HHS) Robert F. Kennedy Jr. has spotlighted the need to expand nutrition education for clinicians, arguing that future physicians and other health care professionals must be better prepared to prevent and manage diet-related chronic disease. He has urged medical schools, residency programs, licensing boards, and accrediting bodies to embed rigorous, measurable nutrition education across all stages of medical training and to modernize standards so clinicians graduate with essential skills in nutrition counseling and preventive care (Kennedy, 2025). Historically, multidisciplinary teams have played essential roles in nutrition support, yet no federal standards have required nutrition as a core course in pharmacy education, and postgraduate nutrition education for physicians and nurses has been limited (Albin et al., 2024; Cai et al., 2024; DuBois et al., 2025). Nurses receive variable formal training in nutrition, with many developing competencies through clinical experience, which may limit readiness to address diet-related health disparities early in practice (Palmer & Champion, 2025). Addressing this gap in pre-licensure curricula or in opportunities for continuing education would better prepare nurses to integrate prevention and wellness into their practice, or even within their communities (DuBois et al., 2025). As an organization, NAHN has invested in building partnerships with national stakeholders to encourage members to expand their knowledge of nutrition. NAHN recently partnered with Abbott to offer free nutrition-focused nursing continuing education credits on a variety of nutrition and mental health topics (NAHN, n.d.a, n.d.b). Additionally, NAHN's Fuel2Flourish program was supported with bilingual educational content from the National Dairy Council (NDC), with training provided for members to integrate these tools in their programs.
Equally important is recognizing that mental and emotional health are not yet consistently embedded in holistic wellness frameworks or have received national policy attention as nutrition education. Evidence from recent studies underscore the overlap between mental health and nutrition where higher intake of added sugars and ultraprocessed foods has been associated with a greater prevalence of depressive symptoms among U.S. adults; whereas higher-quality diets are linked to lower odds of depression (Du et al., 2024; Zhang et al., 2024). These findings highlight that mental health and nutrition are bidirectionally linked, reinforcing the current Fuel2Flourish core components include mental health and nutrition concepts for effective health promotion and community program interventions. National experts have noted that current health professional education often lacks comprehensive integration of mental health and the broader social determinants of health and stress the importance of preparing clinicians to recognize and address these factors across the lifespan and practice settings (National Academies of Sciences, Engineering and Medicine, 2020).
Although the United States has mental health policies and programs, large segments of the population still experience unmet mental health needs. Social support which includes family, peer, and community connections is a critical determinant of mental health outcomes, buffering against depression, stress, and loneliness (Bruss et al., 2024; CDC, 2022; Galea, 2025). Without stronger social support systems, gaps in policy translate directly into increased risk for the development and progression of mental health conditions, highlighting the need for community-level interventions alongside clinical care.
Many in the U.S. experience loneliness and its well-documented health consequences, including higher risks of depression, chronic disease, and premature mortality (Bruss et al., 2024; Stickley & Koyanagi, 2024). Public health experts stress that these challenges must be addressed proactively, starting in childhood, by fostering emotional wellness behaviors such as self-regulation, empathy, and positive relationship-building (CDC, 2023a, 2023b). Embedding these practices early on can “bend the curve” toward better lifelong well-being, reducing the social isolation that undermines both mental and physical health and learning helpful stress reducing behaviors. Qualitative feedback highlighted those strong relationships with families and community partners where nurses created a safe space for children to learn healthy behaviors, express themselves authentically, and feel proud of their culture. Meeting and coaching the same children over three sessions strengthened this rapport, with one child naming a NAHN nurse as their trusted adult, demonstrating the program's role in fostering enduring trust and support. Although the program specifically targeted Hispanic communities, it was open to all, as demonstrated by 33% of participants being non-Hispanic, showing that the program has the potential to positively impact all children.
Finally, an often-overlooked driver of impact is the power of representation, especially for the largest minority population in the United States, which reached 68 million people in 2024 and continues to experience health inequities (Piña & Martinez, 2025). Latinos remain underrepresented in nursing and, more broadly, across the U.S. health care workforce relative to their proportion of the population. Evidence across health professions demonstrates that providers from historically marginalized communities are more likely to serve in underserved communities (Marrast et al. 2014; Phillips & Malone, 2014; Xierali & Nivet, 2018). More recently, national recommendations emphasize that increasing racial and ethnic diversity within the nursing workforce and leadership is a critical strategy to advance health equity (National Academies of Science, Engineering and Medicine, 2021). Canli and Aquino (2025) found that service to others and serving as a role model were key factors that facilitated leadership development and contributed to the success of Latina nurses.
To address the health inequities that predominate within the Latino community, more Latino leaders are needed who have deep social ties with their communities. Leadership aimed at achieving health equity must be grounded in scientific and clinical knowledge, but it also requires creative social strategies, strong political commitment, and exceptional interpersonal skills (Koh & Nowinski, 2010). The program intentionally focused on cultivating these skills among participants, with the authors providing hands-on guidance, mentorship, and support throughout the experience. For many of the children engaged through Fuel2Flourish, seeing and interacting with Hispanic nurses, many of whom themselves were often the first or only Hispanic health professionals in the room, sparked a sense of possibility as many of them donned nursing gear and imagined being a “nurse for the day.” This exposure not only inspires children to envision themselves in health careers but also affirms cultural pride and belonging. For the nurses, serving as visible role models was a highlight of the program, reinforcing their own leadership identities and commitment to mentoring the next generation.
When national and state leaders intentionally engage with community partners such as nurses, they create fertile ground for innovation, aligning leadership development, culturally responsive health promotion, early wellness strategies, and authentic role modeling. The recent White House Challenge was an opportunity for cross-sector partnerships to form around a common goal, but also the flexibility to expand and address related health issues. As the new administration continues to focus on wellness and prevention (U.S. Department of Health and Human Services, n.d.), NAHN has a membership that is engaged and ready to provide leadership within their communities. Fuel2Flourish offers a framework for how such integration can accelerate progress toward community wellness while cultivating the next generation of nurse leaders.
Limitations
Although the evaluation achieved a 100% response rate among participating chapters (nine of nine), recruitment was sent to more than 40 chapters nationwide. The limited number of responding chapters suggests that the findings may not fully represent the broader NAHN membership. In this evaluation, we achieved nine interviews, which are generally considered sufficient to identify core themes (Wutich et al., 2024). However, because only nine chapters participated out of more than 40, it is not possible to determine whether the themes identified would fully saturate across the broader NAHN chapter network. Additional chapter participation may have revealed new themes or nuances, especially among chapters with different levels of infrastructure, readiness, or experience in program development. It is likely that chapters that responded had stronger internal infrastructure, more engaged leadership, or nurses who already had interest or experience in program development and implementation.
Additionally, the requirement that program leads independently develop the proposal and budget—without support from NAHN National—may have narrowed the applicant pool to nurses with prior experience in grant writing, budgeting, or program planning. Chapters without these skills or resources may have been less willing or able to apply, further constraining representativeness. This introduces a selection bias that limits generalizability.
Despite these limitations, participating chapters demonstrated strong initiative and adaptability. The program's flexible design enabled chapters to tailor activities to their available resources while still benefiting from structured mentorship, resulting in meaningful growth in leadership capacity and community engagement skills. Future program cycles should consider providing centralized support, such as proposal development workshops, budget templates, or technical assistance, to ensure broader accessibility across chapters of varying capacity levels. Expanding support during the application phase may help reduce barriers to participation, improve representativeness, and strengthen overall program impact.
Conclusion
Fuel2Flourish demonstrates the power of nurse-led, culturally responsive programming to strengthen the nutritional and emotional well-being of Latino children across diverse U.S. communities. By positioning NAHN nurses as trusted messengers and visible role models, this initiative bridged the gap between evidenced-based public health guidance and the lived realities of families, fostering trust, engagement, and meaningful behavior change. Partnerships with schools, community organizations, and families were central to its success, enabling bilingual, hands-on education that reflected local priorities. Early outcomes suggest that when nurses are equipped with the resources, autonomy, and community connections to lead, they can catalyze improvements in child health and inspire the next generation to envision themselves in health careers. Sustained investment in such models has the potential to expand their reach, deepen their impact, and advance child health and well-being well beyond the initial nine chapters.
Disclosure Statement
The views expressed in this manuscript are solely those of the authors and do not necessarily reflect the positions of any affiliated institutions or organizations. The authors declare no conflicts of interest related to this work. Microsoft Copilot was utilized as described in the Methods section, including support for refining phrasing and enhancing clarity, as needed. The data to support the findings of this study are not publicly available. These findings were presented in July 2025 at NAHN's 50th Annual Conference in Dallas, Texas, United States.
Supplemental Material
sj-docx-1-ppn-10.1177_15271544261463203 - Supplemental material for Fuel2Flourish: Nurses as Trusted Voices Promoting Latino Child Well-Being Across Nine U.S. States
Supplemental material, sj-docx-1-ppn-10.1177_15271544261463203 for Fuel2Flourish: Nurses as Trusted Voices Promoting Latino Child Well-Being Across Nine U.S. States by Adrianna Nava, Kate Filipiak and Aida Miles in Policy, Politics, & Nursing Practice
Footnotes
Acknowledgments
We gratefully acknowledge Direct Relief and the Coalition for Safe Food and Beverages for funding the Fuel2Flourish chapter programs. We also thank our partners—Latinos and Hispanics in Dietetics and Nutrition (LAHIDAN) and Lana Balvin Frantzen, PhD, MS, National Dairy Council (NDC) for their invaluable insights and support of this program. Thank you to Abbott for their support in sharing nutrition and mental health education resources for NAHN members. A special thank you to the dedicated chapter leads, members and volunteers from Michigan, Kansas City (El Corazón), Greater Milwaukee, New Mexico, Central Florida, Alabama, Illinois, Sacramento, and Western Pennsylvania/Pittsburgh for their leadership, creativity, and commitment in bringing Fuel2Flourish to life in their communities. You can see highlights of their local chapter program in the NAHN Fuel2Flourish YouTube playlist.
Funding
The authors disclosed receipt of the following financial support for the community project, authorship, and/or publication of this article: This work was supported by the Coalition for Safe Food and Beverages and Direct Relief.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the community project, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.