
Abstract
Abstract
Severe fever with thrombocytopenia syndrome virus (SFTSV) is an emerging tick-borne pathogen responsible for severe and often fatal disease in East Asia; however, information from Southeast Asia remains limited. We report two fatal human SFTS cases in Thailand confirmed by quantitative reverse transcription polymerase chain reaction, in which viral RNA was detected in multiple specimen types from both patients, including plasma, cerebrospinal fluid, respiratory secretions, urine, and stool, indicating systemic infection. Rhipicephalus sanguineus ticks collected from pet dogs and from the patients’ households also tested positive for SFTSV RNA, with cycle threshold values ranging from 15.6 to 30.6. Phylogenetic analyses based on the S, M, and L segments showed that sequences obtained from human and tick samples clustered within genotype B-1 and were closely related to previously reported Thai and related Chinese strains. These findings provide molecular evidence of SFTSV in dog-associated R. sanguineus ticks and suggest a possible epidemiological association with human cases; however, their role in transmission and the direction of transmission remain uncertain. These findings expand the known geographic and ecological context of SFTSV and underscore the importance of heightened clinical awareness and integrated human–animal–vector surveillance in Southeast Asia, particularly in dengue-endemic regions where SFTS may be clinically overlooked.
Keywords
Introduction
Severe fever with thrombocytopenia syndrome virus (SFTSV; Bandavirus dabieense) is a segmented, negative-sense RNA virus of the genus Bandavirus (family Phenuiviridae) and an emerging zoonotic threat in Asia (International Committee on Taxonomy of V, 2025). Since its discovery in China in 2009 (Yu et al., 2011), SFTSV has caused severe tick-borne disease, primarily in China, South Korea, and Japan, where Haemaphysalis longicornis ticks constitute the predominant tick species in the environment and are regarded as the principal vector responsible for viral transmission (Kim et al., 2011; Chong et al., 2013). Sporadic infections have also been reported in Southeast Asia (Casel et al., 2021; Cui et al., 2024). Extensive research in East Asian countries has established SFTSV as an important emerging pathogen; however, data from regions outside East Asia, particularly Southeast Asia, including Thailand, remain limited. Previous studies in Thailand have mainly focused on serological surveys and sporadic case detections, with little molecular evidence demonstrating viral presence in clinical specimens or arthropod vectors.
In addition to tick-borne transmission, SFTSV can also be transmitted through direct contact with infected animals or humans, particularly via blood or body fluids under certain conditions (Woo et al., 2025).
Beyond the primary vector, SFTSV has been detected in several other tick species, including Rhipicephalus microplus, Amblyomma testudinarium, and Ixodes nipponensis (Yun et al., 2014; Lin et al., 2020). Previous experimental studies have suggested that Rhipicephalus sanguineus may play a role in SFTSV ecology by supporting viral infection and transovarial maintenance (Yuan et al., 2023).
R. sanguineus, the brown dog tick, is a cosmopolitan species with a worldwide distribution, including tropical and subtropical regions such as Thailand, and is closely associated with domestic dogs (Do et al., 2021; Juasook et al., 2021). It predominantly feeds on dogs but may occasionally bite humans, although such events are rarely reported; human infestation has been documented in settings of heavy tick burden and close contact with dogs (Mentz et al., 2016; Kobayashi and Iwasaki, 2017).
In addition, R. sanguineus has been reported to transmit a broad range of pathogens, including viruses such as Crimean–Congo hemorrhagic fever virus, bacteria (e.g., Bartonella henselae, Ehrlichia canis, Coxiella burnetii, and zoonotic Rickettsia spp.), and protozoa (e.g., Babesia spp. and Hepatozoon canis) (Perveen and Khan, 2022; Dantas-Torres et al., 2024). However, its role in SFTSV transmission to vertebrate hosts remains unclear and has not yet been fully established.
Here, we describe two fatal human cases of SFTS in Thailand, representing the first molecularly confirmed fatal infections linked to dog-associated R. sanguineus ticks collected from pet dogs and from the patients’ households. Viral RNA was detected in multiple specimen types obtained during hospitalization, indicating systemic viral dissemination prior to death. These findings provide novel insights into multisystem detection of SFTSV during acute infection and support a possible epidemiological association between domestic R. sanguineus ticks and human SFTSV cases in Thailand.
Materials and Methods
Ethics statement
This study was approved by the Institutional Review Board of Chulalongkorn University (IRB no. 710/64). The requirement for informed consent was waived, as all data were anonymized and contained no identifiable personal information.
Case description and specimen collection
In 2025, two fatal human cases of SFTS were identified in Phetchabun Province, lower northern Thailand.
Exposure histories were obtained through clinical interviews conducted by attending physicians and public health personnel as part of routine case investigation. Although no SFTS-specific standardized protocol is currently implemented in Thailand, data collection followed general infectious disease investigation practices. Information on animal contact (including contact with domestic dogs), environmental exposure, and potential arthropod exposure was collected when available and documented in the clinical history.
The first patient, an 82-year-old male farmer from Phetchabun Province, presented with a 3-day history of fever and progressive confusion. On admission, he was febrile (38.7°C), disoriented, and had leukopenia (3210 cells/µL), mild thrombocytopenia (117,000/µL), and elevated liver enzymes (AST, 375 U/L; ALT, 120 U/L). He showed altered consciousness. Meningeal signs were absent, and cerebrospinal fluid (CSF) analysis was unremarkable, with multiplex polymerase chain reaction (PCR) negative for common meningoencephalitis pathogens. His history included frequent contact with heavily tick-infested pet dogs. Despite empirical treatment with ceftriaxone and azithromycin, his condition rapidly worsened, progressing to acute respiratory and renal failure, shock, rhabdomyolysis (CPK, 17,465 U/L), and massive gastrointestinal hemorrhage. He died on day 11 of illness. SFTSV RNA was detected in plasma and CSF specimens collected during hospitalization.
The second patient was a 56-year-old man from the same subdistrict as the index case, residing about 5 km away. He had frequent contact with stray and pet dogs. He developed symptoms 13 days after the onset of illness in the first case. On admission, he had hypertension, fever, dyspnea, cough, and malaise. He developed tachycardia (148 bpm), hypotension (74/55 mm Hg), and respiratory distress with bilateral lung crepitations. Laboratory findings showed leukocytosis with neutrophilia, progressive thrombocytopenia (platelet count decreased from 203,000 cells/µL on admission to a nadir of 59,000 cells/µL over subsequent days), coagulopathy, acute kidney injury, severe transaminitis (AST, 24,567 U/L; ALT, 8708 U/L), and metabolic acidosis. Chest radiographs revealed bilateral infiltrates consistent with viral pneumonia. His condition rapidly worsened, progressing to hypoxemic respiratory failure requiring high-flow oxygen, followed by severe metabolic acidosis with elevated lactate, consistent with sepsis. Despite treatment with favipiravir, broad-spectrum antimicrobials, and intensive care, he developed recurrent massive gastrointestinal bleeding, septic shock, and fulminant hepatitis. He died on day 8 of illness. SFTSV RNA was detected in plasma, nasopharyngeal and pharyngeal swabs, urine, and stool samples collected during hospitalization.
Tick collection and identification
After confirmation of SFTSV-positive patients, ticks were collected from pet dogs in close contact with the patients and from surrounding household environments, including both indoor and outdoor areas. Dogs were identified through interviews with patients and household members, supplemented by direct on-site observation, and all accessible dogs within the household environment were included for tick collection. Ticks were collected manually from these dogs; however, no biological samples (e.g., blood or swabs) were obtained from the animals.
In the first household, four pet dogs were present, whereas five pet dogs were identified in the second household. All dogs were owned by the respective patients and had access to both indoor and outdoor environments. Several dogs were observed to be heavily infested with ticks at the time of collection. Information regarding the clinical health status of the dogs was limited, and no virological testing for SFTSV was performed. No antitick treatments were reported to have been used in the dogs in either household at the time of investigation. No specific conditions, such as dog breeding or animal rescue activities, were identified in either household.
Ticks from household environments were collected through visual inspection of indoor areas and immediate outdoor surroundings, including floors, bedding, and areas where dogs were frequently present. In selected areas, cloth dragging over floor surfaces was also performed to facilitate tick collection.
Specimens were placed in sterile tubes and transported to the laboratory under controlled conditions. Ticks were morphologically identified as R. sanguineus using standard taxonomic keys. Each tick was individually processed for RNA extraction and screened for SFTSV RNA by quantitative reverse transcription polymerase chain reaction (qRT-PCR).
RNA extraction and molecular detection
Total RNA was extracted from 200 μL of each clinical specimen using an automated magLEAD 12gC instrument (Precision System Science, Chiba, Japan) according to the manufacturer’s instructions. For tick specimens, each tick homogenate was processed individually for RNA extraction using the IndiMag Pathogen Kit (Indical Bioscience, Leipzig, Germany) following the manufacturer’s protocol. Real-time qRT-PCR targeting the small (S) segment of SFTSV was performed using primers and probes described previously (Zhang et al., 2012; Rattanakomol et al., 2022). Samples with cycle threshold (Ct) values below 38 were considered positive.
Sequencing and phylogenetic analysis
For all SFTSV RNA-positive clinical specimens from both patients and representative tick samples (one from each household), a partial S segment was amplified and sequenced following a previously published protocol (Rattanakomol et al., 2023). Partial S segment amplicons were purified and sequenced using the Sanger method. Nucleotide sequences were visualized with Chromas Lite (v2.1) and analyzed using the Basic Local Alignment Search Tool (BLAST). Sequence alignment was performed using MUSCLE as implemented in MEGA12. Phylogenetic analysis of the partial S-segment sequences was conducted using the maximum-likelihood method with 1000 bootstrap replicates in MEGA12 and compared with reference SFTSV sequences retrieved from GenBank. In addition, complete coding sequences of the S, M, and L segments were obtained from plasma samples of both patients and representative tick-derived viral isolates collected from dogs in each patient household (one per household). Amplification of the complete coding regions was performed using previously described primers and PCR conditions (Rattanakomol et al., 2023). Sequencing was performed on an Illumina MiSeq platform. Raw reads were quality filtered, assembled using SPAdes, and validated by reference mapping and BLAST analysis. The resulting sequences were subsequently included in phylogenetic analyses as described above. Nucleotide sequences of the partial S segment generated in this study were deposited in GenBank under accession numbers PX309554–PX309562. Complete coding sequences of the S, M, and L segments were deposited in GenBank under the following accession numbers: PZ157784, PZ157785, PZ157787, and PZ157788 (S segment); PZ157792, PZ157793, PZ157795, and PZ157796 (M segment); and PZ157800, PZ157801, PZ157803, and PZ157804 (L segment).
Results
SFTSV detection in human clinical specimens
SFTSV RNA was detected in multiple clinical specimens from both patients (Table 1). In the first patient, viral RNA was identified in plasma (Ct = 26.29) and cerebrospinal fluid (Ct = 34.18). In the second patient, viral RNA was detected in plasma, urine, stool, nasopharyngeal, and throat swabs, with Ct values ranging from 28.6 to 32.3, confirming multisystem viral dissemination during acute infection.
Specimens Positive for SFTSV, Thailand, 2025
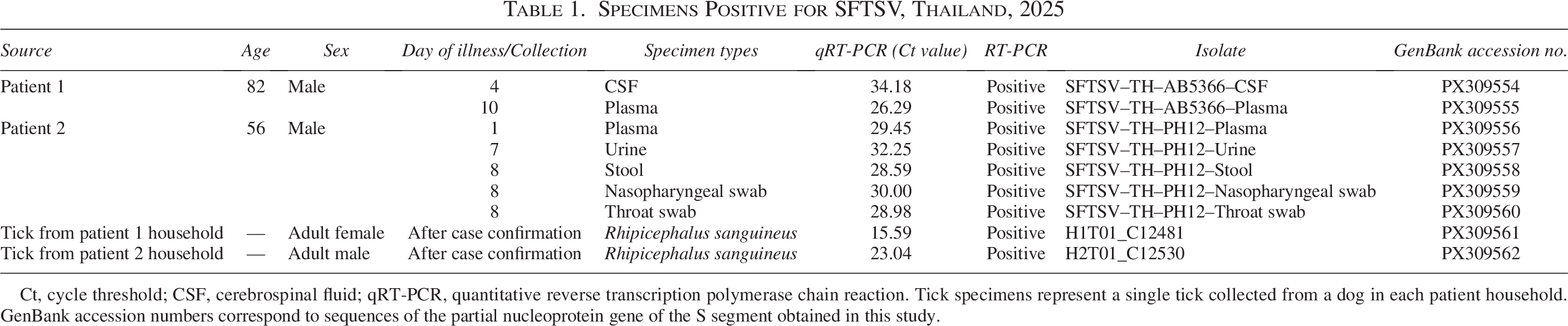
Ct, cycle threshold; CSF, cerebrospinal fluid; qRT-PCR, quantitative reverse transcription polymerase chain reaction. Tick specimens represent a single tick collected from a dog in each patient household. GenBank accession numbers correspond to sequences of the partial nucleoprotein gene of the S segment obtained in this study.
SFTSV detection in ticks from household dogs and environments
In the first household, a total of 44 R. sanguineus ticks were collected from four pet dogs and the surrounding household environment. Among these, SFTSV RNA was detected in three ticks (6.8%). Two SFTSV-positive ticks were free-living adults collected from indoor locations: one from an indoor doormat (Ct = 27.07) and another from a doormat near the bathroom (Ct = 21.19). The third positive tick, an adult female, was collected from one of the pet dogs and showed the highest viral load (Ct = 15.59).
In the second household, 44 R. sanguineus ticks were collected from five pet dogs belonging to the second patient. Of these, 13 ticks (29.5%) tested positive for SFTSV RNA by qRT-PCR, with Ct values ranging from 21.3 to 30.6. Positive ticks were obtained from four dogs and included seven adult females and six adult males.
Collectively, these findings demonstrate the presence of SFTSV RNA in R. sanguineus ticks collected from both dogs and domestic environments, supporting a possible epidemiological association with the human cases. However, nontick transmission routes cannot be excluded.
Sequencing and phylogenetic analysis
Partial S segment sequences (476 bp) were successfully amplified from all SFTSV RNA-positive clinical specimens of both patients and from representative tick samples (one from each household) collected from pet dogs. Sequences obtained from human and tick samples were identical, showing 100% nucleotide identity, indicating close genetic relatedness. Phylogenetic analysis revealed that all sequences formed a monophyletic cluster within genotype B-1 and shared 99.7–100% identity with previously reported Thai strains and >99% identity with related Chinese strains from 2012 to 2024 (Fig. 1).
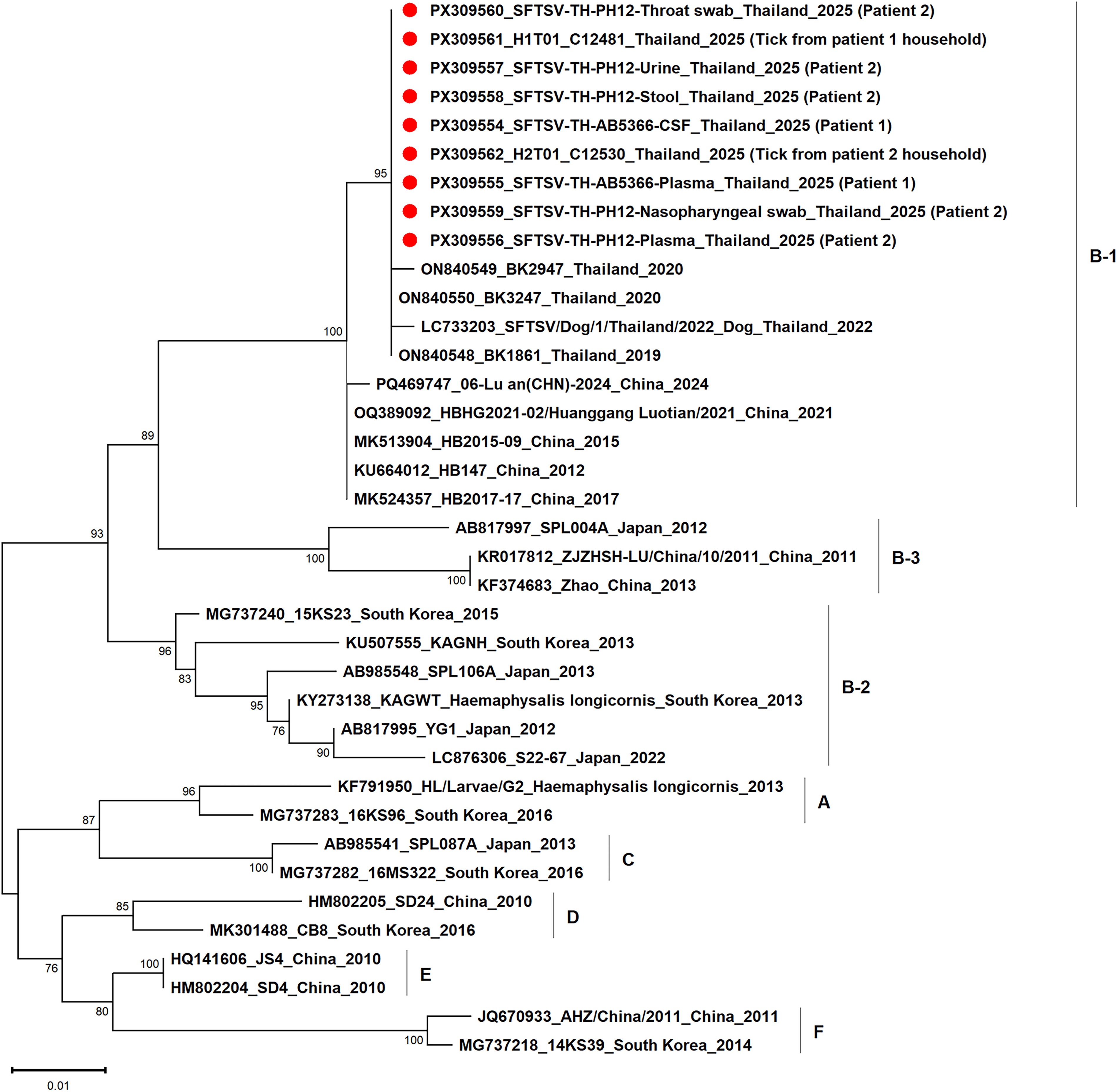
Maximum likelihood phylogenetic tree of SFTSV based on the partial S segment nucleotide sequences. The tree was constructed in MEGA12 using the Kimura 2-parameter model with a gamma distribution (K2 + G) to account for rate variation among sites. Bootstrap values were calculated with 1000 replicates, and values ≥80% are shown at the corresponding nodes. Red closed circles indicate SFTSV strains identified in this study. The scale bar indicates the number of nucleotide substitutions per site. SFTSV, severe fever with thrombocytopenia syndrome virus.
Consistent clustering patterns were observed in phylogenetic analyses based on the complete coding sequences of the S, M, and L segments, in which sequences obtained from human specimens and representative tick samples collected from pet dogs (one from each household) also grouped within genotype B-1 (Fig. 2). These findings support the circulation of closely related SFTSV strains in the local setting. However, they do not establish direct transmission among humans, dogs, and ticks.
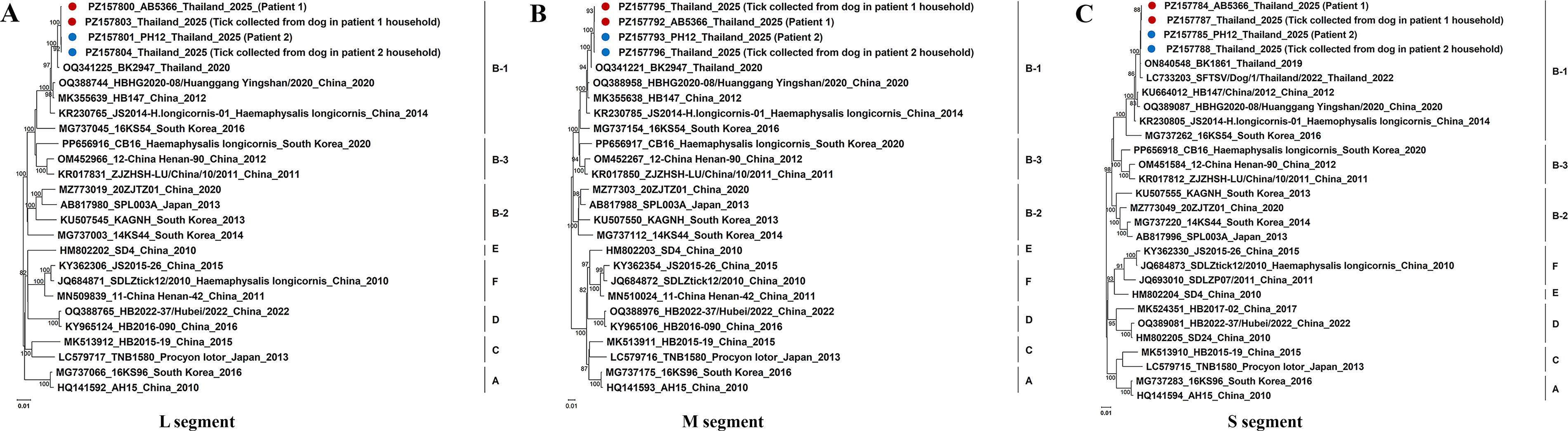
Maximum likelihood phylogenetic trees of SFTSV based on complete coding sequences of the L
Discussion
This study provides molecular evidence of SFTSV RNA detection in R. sanguineus ticks collected from pet dogs in Thailand, with sequences showing high genetic similarity to those detected in fatal human infections. The concurrent detection of viral RNA in multiple clinical specimen types from both patients further demonstrates systemic viral dissemination during acute disease. These findings extend the known ecological range of SFTSV beyond East Asia into Southeast Asia. Evidence for local transmission is supported by the absence of travel history in both patients and the occurrence of cases in a nonborder province. Previous studies in Thailand have detected SFTSV in rodents, dogs, and chigger mites, with high seroprevalence in dogs (Ishijima et al., 2023; Linsuwanon et al., 2024); however, the role of specific tick species as vectors has remained unresolved, as one prior study did not detect SFTSV RNA in ticks (Saba Villarroel et al., 2024). The present findings contribute to this knowledge by demonstrating the presence of SFTSV RNA in dog-associated R. sanguineus ticks in Thailand. These findings support a possible epidemiological association between domestic R. sanguineus ticks and SFTSV circulation in Thailand. The epidemiological link to human infection is further supported by phylogenetic clustering and close genetic relatedness between sequences obtained from ticks and patients within genotype B-1, suggesting a possible epidemiological association.
Our findings highlight the urgent need for clinical awareness of SFTS in Thailand and throughout Southeast Asia. In this region, where clinical manifestations overlap with several otherendemic infections, including dengue, leptospirosis, scrub typhus, and chikungunya, SFTS may be easily misdiagnosed. Clinicians should include SFTS in the differential diagnosis of patients presenting with acute febrile illness, thrombocytopenia, and rapid progression to multiorgan failure. Timely recognition is essential for appropriate management and an effective public health response. Strengthening integrated surveillance involving humans, animals, and vectors will be important to clarify transmission dynamics and prevent further fatalities. This is especially important in dengue-endemic regions, where SFTS may be mistaken for more common febrile illnesses and therefore missed. Incorporating epidemiological exposure history, including contact with domestic animals and potential vector exposure, into case definitions and clinical assessment may improve early detection and clinical suspicion of SFTS, particularly in dengue-endemic settings.
SFTSV RNA was detected in R. sanguineus ticks collected directly from pet dogs as well as from household environments in two independent households. This repeated detection, including multiple positive ticks with relatively low Ct values, supports a possible epidemiological association between dog-associated ticks and the human cases. However, these findings do not establish vector competence or the direction of transmission. Compared with Haemaphysalis longicornis, the primary vector of SFTSV in East Asia, R. sanguineus is primarily associated with dogs and is well adapted to domestic and peridomestic environments, whereas H. longicornis parasitizes a broad range of host species, including livestock, wildlife, and occasionally dogs, reflecting differences in ecological niches and transmission contexts (Zhao et al., 2020; Dantas-Torres and Otranto, 2022). Although R. sanguineus has been reported to bite humans, it is generally considered to do so infrequently; therefore, tick-to-human transmission in these cases should be interpreted with caution.
Alternative transmission routes should also be considered. SFTSV has been reported to be transmitted through direct contact with infected animals or humans, particularly via blood or body fluids, and close contact with dogs may represent a potential exposure pathway (Jung et al., 2019; Fang et al., 2021; Wu et al., 2022; Kim et al., 2025; Li et al., 2026). In addition, virological testing of the dogs was not performed; therefore, the infection status of the animals remains unknown. In addition, infection via other tick species cannot be excluded. Although SFTSV RNA was detected in ticks, this finding does not confirm the presence of infectious virus or demonstrate vector competence. While experimental studies have demonstrated vector competence for certain tick species (Yuan et al., 2023), the role of R. sanguineus in natural transmission remains uncertain, particularly in the context of Thailand. Tick collection was performed after confirmation of human infection; therefore, the temporal relationship between infected ticks and human cases cannot be determined. While it is possible that ticks acquired viral RNA after the onset of human infection, this possibility should be interpreted with caution. Accordingly, while our results support an epidemiological association, the direction of transmission remains uncertain.
Future investigations incorporating concurrent sampling of humans, animals, and ticks, together with genomic and phylogenetic analyses, would be valuable to better resolve transmission pathways and clarify the direction of transmission.
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article.
Disclaimer
The material has been reviewed by the Walter Reed Army Institute of Research. There is no objection to its presentation and/or publication. The opinions or assertions contained herein are the private views of the author and should not to be construed as official, or as reflecting true views of the Department of the Army or the Department of Defense. The investigators have adhered to the policies for the protection of human subjects as prescribed in AR 70-25.
Footnotes
Acknowledgments
The authors thank all staff members of the Center of Excellence in Clinical Virology for their technical and administrative assistance. Support for S.K. and W.C. was provided by the Second Century Fund (C2F) of Chulalongkorn University. Investigation, disease control activities, and specimen collection were done by the Department of Disease Control, Ministry of Public Health, Thailand; the Office of Disease Prevention and Control 2, Phitsanulok, Thailand; Vector Borne Disease Control 2.2, Phetchabun, Thailand; the Phetchabun Provincial Public Health Office; the Wang Pong District Livestock Office; the Phetchabun Provincial Livestock Office; the Mueang Phetchabun District Livestock Office; the Lom Sak District Livestock Office; the Phetchabun Animal Quarantine Station; Wang Pong Hospital; Wang Kradaeng Ngoen Subdistrict Health Promotion Hospital; and Bangkok Hospital Phitsanulok. The assistance provided by the Department of Entomology, WRAIR-AFRIMS, for this work was supported by the Global Emerging Infections Surveillance Program.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by the